

Parenteral Nutrition: Current Use, Complications, and Nutrition Delivery in Critically Ill Patients

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Data Collection and Study Endpoints
2.3. Statistical Analysis
3. Results
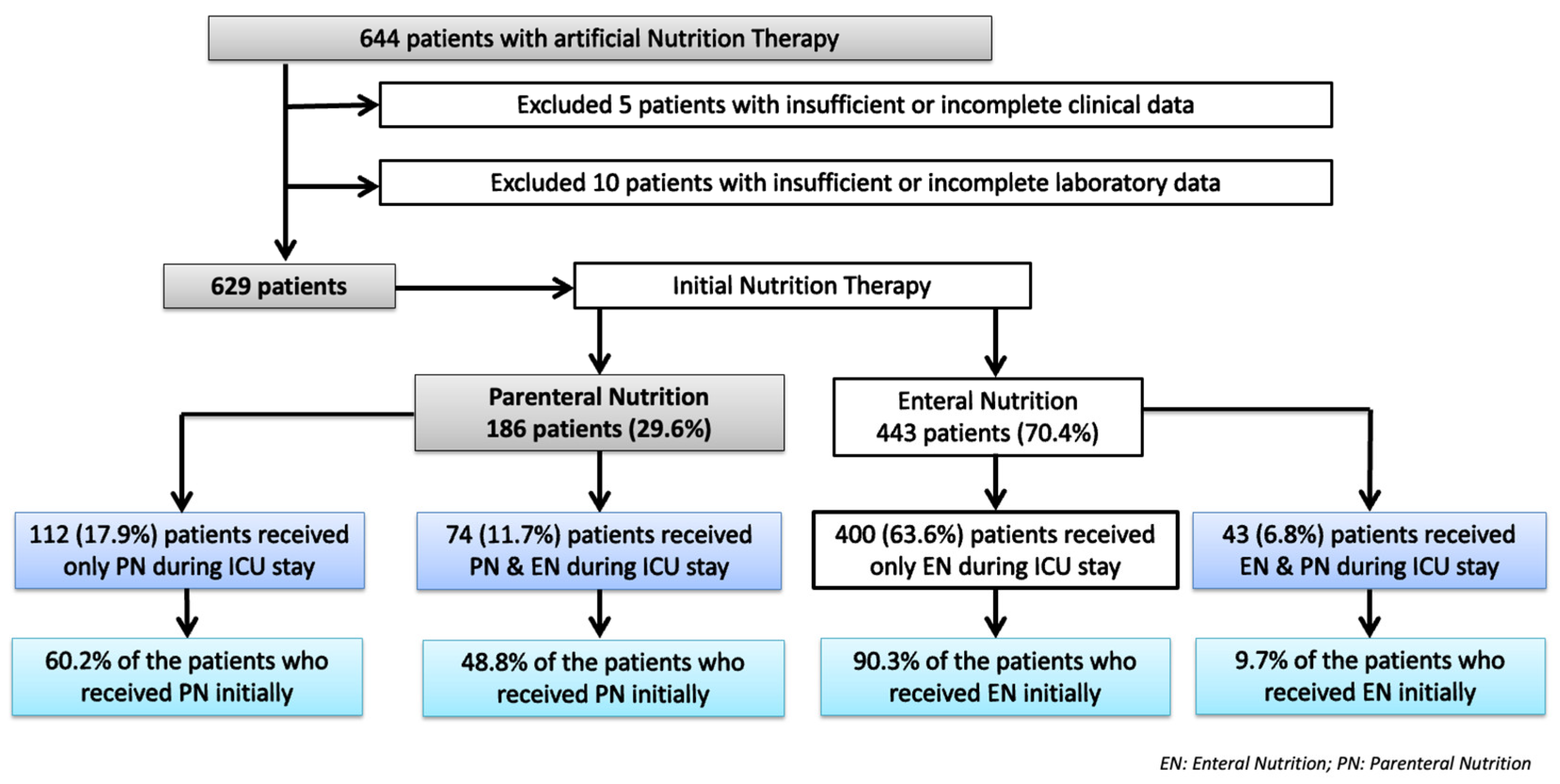
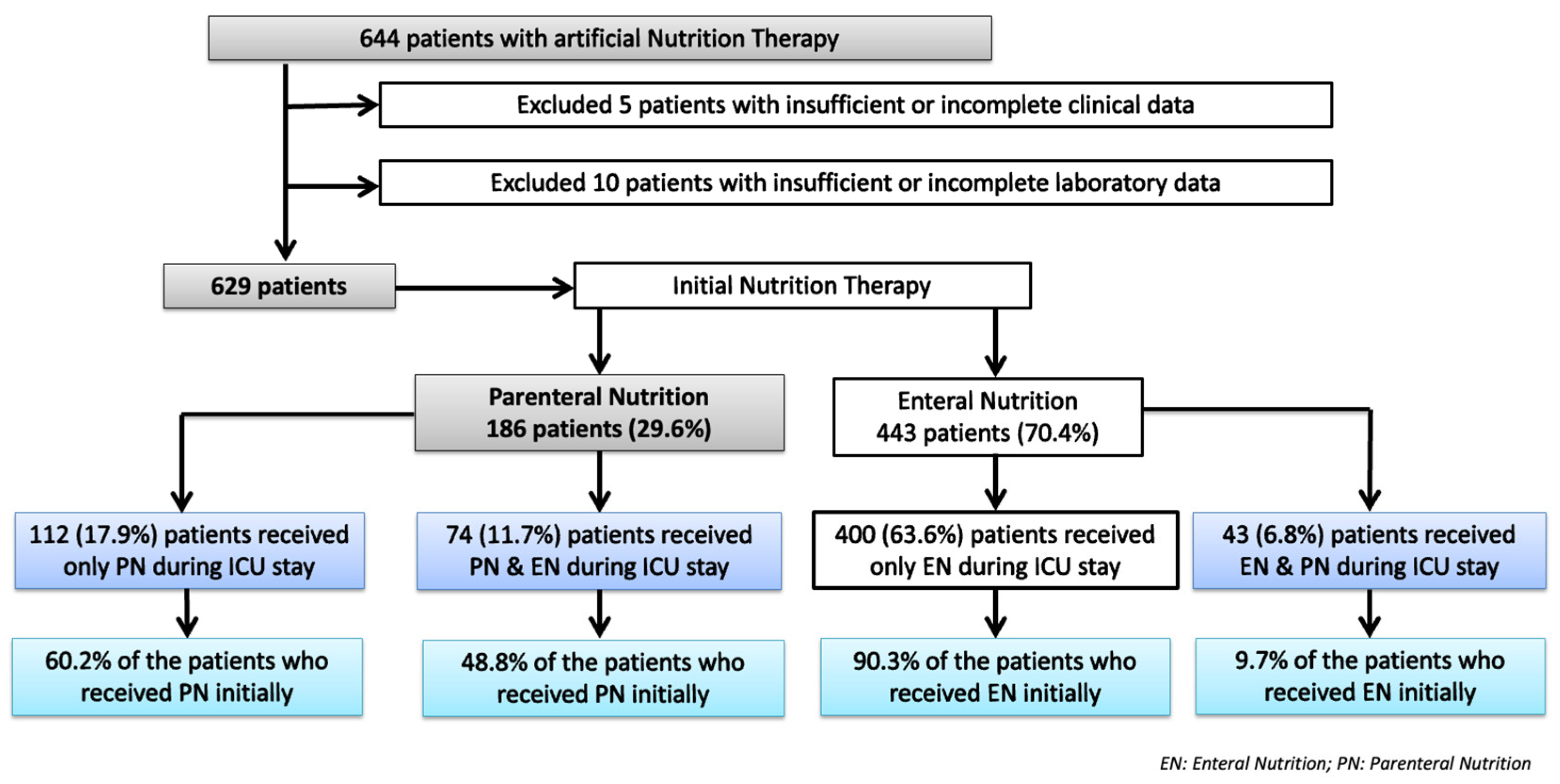
3.1. Population Included in the Study
3.2. Current Use and Complications Associated with PN
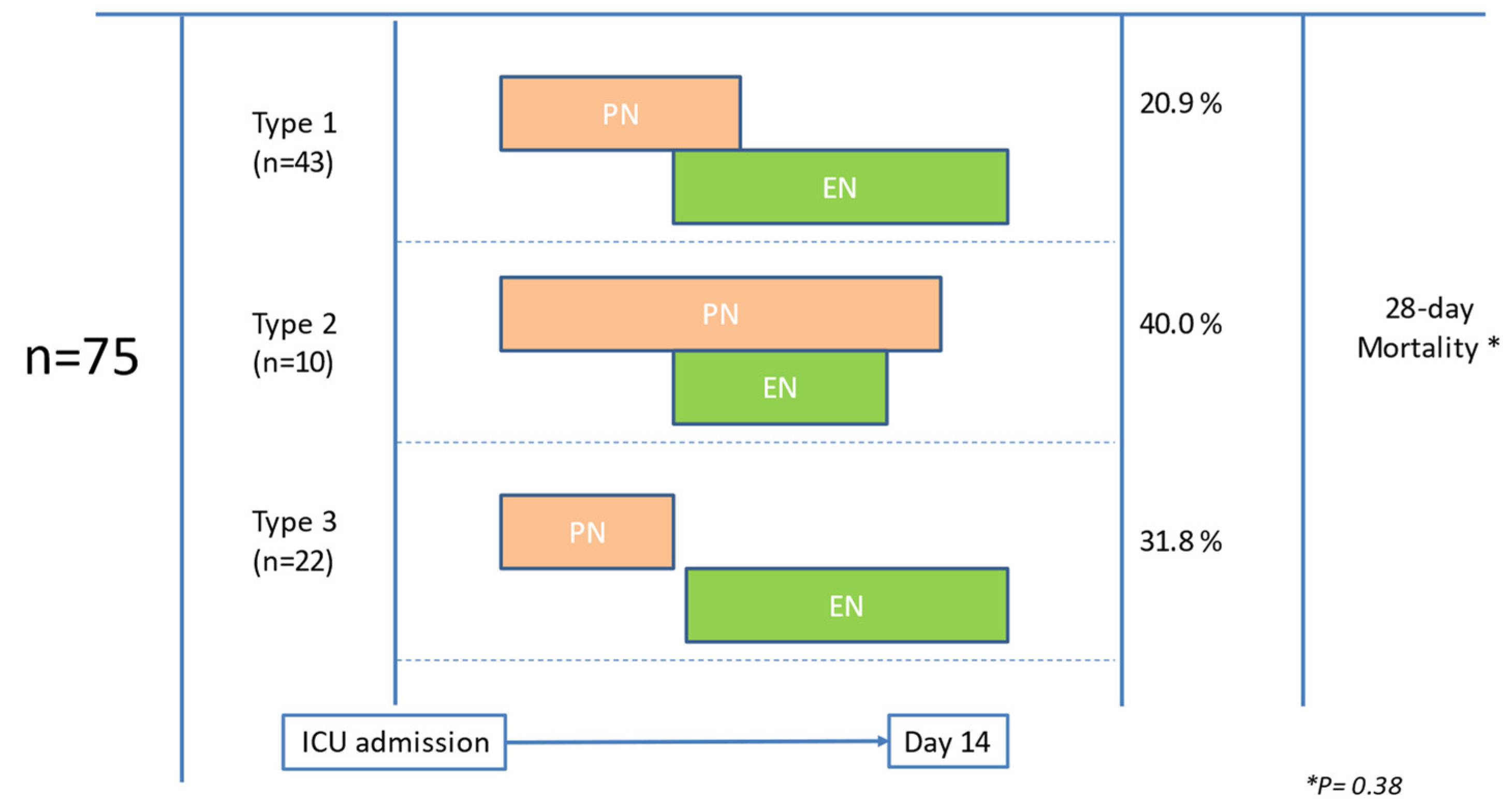
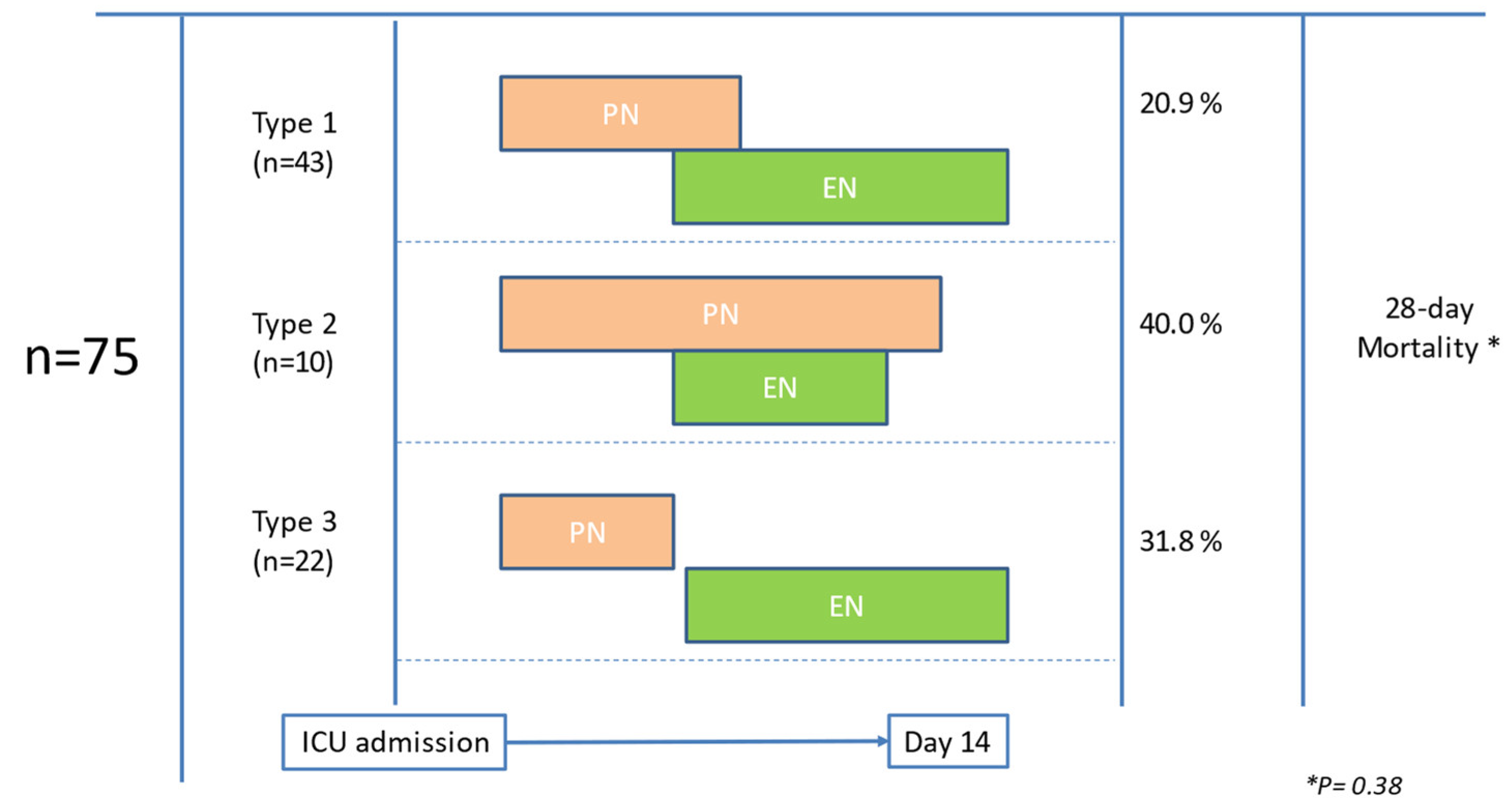
3.3. Assessment of Nutrition Delivery
3.4. Differences between the PN and PN-EN Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Lew, C.C.H.; Yandell, R.; Fraser, R.J.L.; Chua, A.P.; Chong, M.F.F.; Miller, M. Association Between Malnutrition and Clinical Outcomes in the Intensive Care Unit: A Systematic Review. JPEN J. Parenter. Enter. Nutr. 2017, 41, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Herrero Meseguer, J.I.; Lopez-Delgado, J.C.; Martínez García, M.P. Recommendations for specialized nutritional-metabolic management of the critical patient: Indications, timing and access routes. Metabolism and Nutrition Working Group of the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC). Med. Intensiva (Engl. Ed.) 2020, 44 (Suppl. S1), 33–38. [Google Scholar] [CrossRef] [PubMed]
- Vaquerizo Alonso, C.; Bordejé Laguna, L.; Fernández-Ortega, J.F. Recommendations for specialized nutritional-metabolic management of the critical patient: Introduction, methodology and list of recommendations. Metabolism and Nutrition Working Group of the Spanish Society of Intensive and Critical Care Medicine and Coronary Units (SEMICYUC). Med. Intensiva 2020, 44 (Suppl. S1), 1–14. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Bingham, A.L.; McCall, M.; Patel, J.; Rice, T.W.; Braunschweig, C.; McKeever, L. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The American Society for Parenteral and Enteral Nutrition. JPEN J. Parenter. Enter. Nutr. 2022, 46, 12–41. [Google Scholar] [CrossRef] [PubMed]
- Serviá Goixart, L.; López Delgado, J.C.; Grau Carmona, T. Evaluation of the degree of adherence to the nutritional recommendations of the critical care patient. Nutr. Hosp. 2019, 36, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Quenot, J.P.; Plantefeve, G.; Baudel, J.L.; Camilatto, I.; Bertholet, E.; Cailliod, R.; Reignier, J.; Rigaud, J.P. Bedside adherence to clinical practice guidelines for enteral nutrition in critically ill patients receiving mechanical ventilation: A prospective, multi-centre, observational study. Crit. Care 2010, 14, R37. [Google Scholar] [CrossRef]
- Gungabissoon, U.; Hacquoil, K.; Bains, C.; Irizarry, M.; Dukes, G.; Williamson, R.; Deane, A.M.; Heyland, D.K. Prevalence, risk factors, clinical consequences, and treatment of enteral feed intolerance during critical illness. JPEN J. Parenter. Enter. Nutr. 2015, 39, 441–448. [Google Scholar] [CrossRef]
- Elke, G.; van Zanten, A.R.; Lemieux, M.; McCall, M.; Jeejeebhoy, K.N.; Kott, M.; Jiang, X.; Day, A.G.; Heyland, D.K. Enteral versus parenteral nutrition in critically ill patients: An updated systematic review and meta-analysis of randomized controlled trials. Crit. Care 2016, 20, 117. [Google Scholar] [CrossRef]
- Harvey, S.E.; Parrott, F.; Harrison, D.A.; Bear, D.E.; Segaran, E.; Beale, R.; Bellingan, G.; Leonard, R.; Mythen, M.G.; Rowan, K.M. Trial of the route of early nutritional support in critically ill adults. N. Engl. J. Med. 2014, 371, 1673–1684. [Google Scholar] [CrossRef]
- Servia-Goixart, L.; Lopez-Delgado, J.C.; Grau-Carmona, T.; Trujillano-Cabello, J.; Bordeje-Laguna, M.L.; Mor-Marco, E.; Portugal-Rodriguez, E.; Lorencio-Cardenas, C.; Montejo-Gonzalez, J.C.; Vera-Artazcoz, P.; et al. Evaluation of Nutritional Practices in the Critical Care patient (The ENPIC study): Does nutrition really affect ICU mortality? Clin. Nutr. ESPEN 2022, 47, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Grau, T.; Bonet, A.; Rubio, M.; Mateo, D.; Farré, M.; Acosta, J.A.; Blesa, A.; Montejo, J.C.; de Lorenzo, A.G.; Mesejo, A.; et al. Liver dysfunction associated with artificial nutrition in critically ill patients. Crit. Care 2007, 11, R10. [Google Scholar] [CrossRef] [PubMed]
- Lederer, D.J.; Bell, S.C.; Branson, R.D.; Chalmers, J.D.; Marshall, R.; Maslove, D.M.; Ost, D.E.; Punjabi, N.M.; Schatz, M.; Smyth, A.R.; et al. Control of Confounding and Reporting of Results in Causal Inference Studies. Guidance for Authors from Editors of Respiratory, Sleep, and Critical Care Journals. Ann. Am. Thorac. Soc. 2019, 16, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Pichard, C. Parenteral nutrition in the ICU: Lessons learned over the past few years. Nutrition 2019, 59, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Jeejeebhoy, K.N. Parenteral nutrition in the intensive care unit. Nutr. Rev. 2012, 70, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Grecu, I. How to choose the route. World. Rev. Nutr. Diet 2013, 105, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Hiesmayr, M.; Pichard, C. Parenteral nutrition in the ICU setting: Need for a shift in utilization. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Bielawska, B.; Allard, J.P. Parenteral nutrition and intestinal failure. Nutrients 2017, 9, 466. [Google Scholar] [CrossRef]
- Reintam Blaser, A.; Poeze, M.; Malbrain, M.L.; Björck, M.; Oudemans-van Straaten, H.M.; Starkopf, J.; Gastro-Intestinal Failure Trial Group. Gastrointestinal symptoms during the first week of intensive care are associated with poor outcome: A prospective multicentre study. Intensive Care Med. 2013, 39, 899–909. [Google Scholar] [CrossRef]
- Casaer, M.P.; Mesotten, D.; Hermans, G.; Wouters, P.J.; Schetz, M.; Meyfroidt, G.; Van Cromphaut, S.; Ingels, C.; Meersseman, P.; Muller, J.; et al. Early versus late parenteral nutrition in critically ill adults. N. Engl. J. Med. 2011, 365, 506–517. [Google Scholar] [CrossRef]
- Singer, P.; Anbar, R.; Cohen, J.; Shapiro, H.; Shalita-Chesner, M.; Lev, S.; Grozovski, E.; Theilla, M.; Frishman, S.; Madar, Z. The tight calorie control study (TICACOS): A prospective, randomized, controlled pilot study of nutritional support in critically ill patients. Intensive Care Med. 2011, 37, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Sweetman, E.A.; Finfer, S.R.; Cooper, D.J.; Heighes, P.T.; Davies, A.R.; O’Leary, M.; Solano, T.; Peake, S. Early parenteral nutrition in critically ill patients with short-term relative contraindications to early enteral nutrition: A randomized controlled trial. JAMA 2013, 309, 2130–2138. [Google Scholar] [CrossRef]
- Reignier, J.; Boisramé-Helms, J.; Brisard, L.; Lascarrou, J.B.; Hssain, A.A.; Anguel, N.; Argaud, L.; Asehnoune, K.; Asfar, P.; Bellec, F.; et al. Enteral versus parenteral early nutrition in ventilated adults with shock: A randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2). Lancet 2018, 391, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Matejovic, M.; Huet, O.; Dams, K.; Elke, G.; Vaquerizo Alonso, C.; Csomos, A.; Krzych, Ł.J.; Tetamo, R.; Puthucheary, Z.; Rooyackers, O.; et al. Medical nutrition therapy and clinical outcomes in critically ill adults: A European multinational, prospective observational cohort study (EuroPN). Crit. Care 2022, 26, 143. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Cordón, L.; Yébenes, J.C.; Martínez de Lagrán, I.; Campins, L. Transition from total parenteral nutrition to enteral nutrition in critically ill patients in Spain: A national survey. Med. Intensiva 2022, 46, 475–477. [Google Scholar] [CrossRef] [PubMed]
- Veldsman, L.; Richards, G.A.; Blaauw, R. The dilemma of protein delivery in the intensive care unit. Nutrition 2016, 32, 985–988. [Google Scholar] [CrossRef]
- Lopez-Delgado, J.C.; Servia-Goixart, L.; Grau-Carmona, T.; Bordeje-Laguna, L.; Portugal-Rodriguez, E.; Lorencio-Cardenas, C.; Vera-Artazcoz, P.; Macaya-Redin, L.; Martinez-Carmona, J.F.; Marin Corral, J.; et al. Factors associated with the need of parenteral nutrition in critically ill patients after the initiation of enteral nutrition therapy. Front Nutr. 2023, 10, 1250305. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All Patients n = 186 | Only PN n = 112 | PN-EN n = 74 | p-Value | ||
|---|---|---|---|---|---|
| Baseline characteristics and comorbidities | |||||
| Age, years, mean ± SD | 64.32 ± 13.90 | 63.8 ± 14.53 | 65.09 ± 12.95 | 0.53 | |
| Sex, male patients, n (%) | 124 (66.7) | 68 (60.7) | 56 (75.7) | 0.05 | |
| Body mass index, kg/m2, mean (range) | 26.8 (14.7–41.1) | 27.3 (14.7–40.2) | 26.3 (17.3–41.2) | 0.24 | |
| Hypertension, n (%) | 89 (47.8) | 53 (47.3) | 36 (48.6) | 0.88 | |
| Diabetes mellitus, n (%) | 47 (25.3) | 27 (24.1) | 20 (27.0) | 0.73 | |
| Chronic obstructive pulmonary disease, n (%) | 27 (14.5) | 14 (12.5) | 13 (17.6) | 0.39 | |
| Acute myocardial infarction, n (%) | 26 (14.0) | 17 (15.2) | 9 (12.2) | 0.66 | |
| Chronic liver disease, n (%) | 10 (5.4) | 22 (19.6) | 16 (21.6) | 0.89 | |
| Chronic renal failure, n (%) | 22 (11.8) | 13 (11.6) | 9 (12.2) | 0.95 | |
| Immunosuppression, n (%) | 23 (12.4) | 13 (11.6) | 10 (13.5) | 0.81 | |
| Neoplasia, n (%) | 65 (35.0) | 43 (38.4) | 22 (29.7) | 0.27 | |
| Type of patient | Medical, n (%) | 79 (42.3) | 43 (39.4) | 36 (48.6) | 0.02 |
| Trauma, n (%) | 8 (4.3) | 2 (1.8) | 6 (8.1) | ||
| Surgery, n (%) | 99 (53.2) | 67 (59.8) | 32 (43.2) | ||
| APACHE II, mean ± SD | 19.78 ± 7.47 | 18.95 ± 6.98 | 21.05 ± 8.03 | 0.06 | |
| SAPS II, mean ± SD | 49.80 ± 18.59 | 48.02 ± 19.38 | 52.44 ± 17.15 | 0.13 | |
| SOFA at ICU admission, mean ± SD | 6.81 ± 4.04 | 6.14 ± 4.04 | 7.81 ± 3.85 | 0.005 | |
| Patient with malnutrition (based on SGA), n (%) | 110 (59.1) | 65 (58.0) | 45 (60.8) | 0.76 | |
| mNUTRIC score, mean ± SD | 4.55 ± 1.94 | 4.39 ± 1.98 | 4.78 ± 1.85 | 0.18 | |
| Patient at risk based on mNUTRIC score, n (%) | 90 (48.4) | 52 (46.4) | 38 (51.3) | 0.76 | |
| Nutritional support | |||||
| Time of PN initiation, h, mean ± SD | 38.34 ± 35.19 | 41.62 ± 38.5 | 33.36 ± 29.04 | 0.12 | |
| Early PN, <48 h, n (%) | 140 (75.3) | 82 (73.2) | 58 (78.4) | 0.49 | |
| Kcal/kg/day *, mean ± SD | 19.94 ± 6.72 | 19.27 ± 7.24 | 20.96 ± 5.74 | 0.09 | |
| Protein, g/kg/day *, mean ± SD | 1.01 ± 0.41 | 0.95 ± 0.43 | 1.17 ± 0.36 | 0.03 | |
| Outcomes | |||||
| Mechanical ventilation, n (%) | 144 (77.4) | 76 (67.9) | 68 (91.9) | 0.001 | |
| Mechanical ventilation, days, mean ± SD | 12.23 ± 17.48 | 7.33 ± 11.24 | 17.71 ± 21.29 | <0.001 | |
| Vasoactive drug support, n (%) | 140 (75.3) | 72 (64.3) | 68 (91.9) | <0.001 | |
| Renal replacement therapy, n (%) | 37 (19.9) | 21 (18.7) | 16 (21.62) | 0.71 | |
| Respiratory tract infection, n (%) | 56 (30.1) | 35 (31.2) | 21 (28.4) | 0.74 | |
| Catheter-related infections, n (%) | 15 (8.1) | 12 (10.7) | 3 (4.0) | 0.08 | |
| ICU stay, days, mean ± SD | 18.56 ± 12.61 | 11.51 ± 10.46 | 24.34 ± 24.63 | <0.001 | |
| Hospital stay, days, mean ± SD | 39.49 ± 31.36 | 32.56 ± 21.7 | 50.03 ± 45.78 | <0.001 | |
| 28-day mortality, n (%) | 46 (24.7) | 27 (24.1) | 19 (25.7) | 0.86 | |
| Only PN n = 112 | Only EN n = 400 | EN-PN n = 43 | p-Value ** | ||
|---|---|---|---|---|---|
| Baseline characteristics and comorbidities | |||||
| Age, years, mean ± SD | 63.8 ± 14.53 | 60.72 ± 15.45 | 60.23 ± 13.56 | 0.33 | |
| Sex, male patients, n (%) | 68 (60.7) | 267 (66.7%) | 31 (72.1) | 0.39 | |
| Body mass index, kg/m2, mean (range) | 27.3 (14.7–40.2) | 28.17 ± 6.32 | 27.12 ± 4.92 | 0.17 | |
| Hypertension, n (%) | 53 (47.3) | 170 (42.5) | 17 (39.5) | 0.24 | |
| Diabetes mellitus, n (%) | 27 (24.1) | 103 (25.7) | 13 (30.2) | 0.91 | |
| Chronic obstructive pulmonary disease, n (%) | 14 (12.5) | 72 (18.0) | 9 (20.9) | 0.55 | |
| Acute myocardial infarction, n (%) | 17 (15.2) | 59 (14.7) | 7 (16.3) | 0.89 | |
| Chronic liver disease, n (%) | 22 (19.6) | 22(5.5) | 0 | 0.13 | |
| Chronic renal failure, n (%) | 13 (11.6) | 42 (10.5) | 3 (7.0) | 0.88 | |
| Immunosuppression, n (%) | 13 (11.6) | 42 (10.5) | 6 (13.9) | 0.86 | |
| Neoplasia, n (%) | 43 (38.4) | 61 (15.2) | 8 (18.6) | 0.01 | |
| Type of patient | Medical, n (%) | 43 (39.4) | 285 (71.2) | 31 (72.1) | 0.001 |
| Trauma, n (%) | 2 (1.8) | 59 (14.7) | 4 (9.3) | ||
| Surgery, n (%) | 67 (59.8) | 56 (14.0) | 8 (18.6) | ||
| APACHE II, mean ± SD | 18.95 ± 6.98 | 20.04 ± 7.85 | 22.49 ± 8.03 | 0.16 | |
| SAPS II, mean ± SD | 48.02 ± 19.38 | 48.37 ± 17.41 | 51.03 ± 15.94 | 0.43 | |
| SOFA at ICU admission, mean ± SD | 6.14 ± 4.04 | 7.09 ± 3.17 | 8.65 ± 3.54 | 0.04 | |
| Patient with malnutrition (based on SGA), n (%) | 65 (58.0) | 138 (34.5) | 16 (37.2) | 0.16 | |
| mNUTRIC score, mean ± SD | 4.39 ± 1.98 | 3.96 ± 2.17 | 4.81 ± 2.17 | 0.18 | |
| Patient at risk based on mNUTRIC score, n (%) | 52 (46.4) | 165 (41.2) | 27 (62.8) | 0.76 | |
| Nutritional support | |||||
| Time of nutrition initiation, h, mean ± SD | 41.62 ± 38.5 | 36.40 ± 31.31 | 44.15 ± 25.49 | 0.02 | |
| Early nutrition therapy, <48 h, n (%) | 82 (73.2) | 308 (77.0) | 26 (60.5) | 0.69 | |
| Kcal/kg/day *, mean ± SD | 19.27 ± 7.24 | 14.50 ± 5.60 | 15.46 ± 5.31 | <0.001 | |
| Protein, g/kg/day *, mean ± SD | 0.95 ± 0.43 | 0.76 ± 0.34 | 0.83 ± 0.28 | 0.03 | |
| Outcomes | |||||
| Mechanical ventilation, n (%) | 76 (67.9) | 391 (97.7) | 40 (93) | 0.007 | |
| Mechanical ventilation, days, mean ± SD | 7.33 ± 11.24 | 13.23 ± 13.94 | 21.50 ± 18.35 | 0.03 | |
| Vasoactive drug support, n (%) | 72 (64.3) | 296 (74.0) | 32 (74.4) | 0.01 | |
| Renal replacement therapy, n (%) | 21 (18.7) | 41 (10.2) | 17 (39.5) | 0.31 | |
| Respiratory tract infection, n (%) | 35 (31.2) | 102 (25.5) | 8 (18.6) | 0.64 | |
| Catheter-related infections, n (%) | 12 (10.7) | 26 (6.5) | 2 (4.6) | 0.08 | |
| ICU stay, days, mean ± SD | 11.51 ± 10.46 | 18.58 ± 16.23 | 23.88 ± 19.50 | <0.001 | |
| Hospital stay, days, mean ± SD | 32.56 ± 21.7 | 34.60 ± 29.80 | 39.20 ± 28.15 | 0.001 | |
| 28-day mortality, n (%) | 27 (24.1) | 99 (24.7) | 16 (37.2) | 0.86 | |
| Day | Kcal/kg/Day | Protein g/kg/Day | ||||
|---|---|---|---|---|---|---|
| Only PN n = 112 | Only EN n = 400 | p-Value | Only PN n = 112 | Only EN n = 400 | p-Value | |
| 1 | 14.71 ± 8.58 | 6.86 ± 4.73 | <0.001 | 0.73 ± 0.51 | 0.36 ± 0.27 | <0.001 |
| 2 | 19.93 ± 8.37 | 12.97 ± 6.81 | <0.001 | 0.99 ± 0.60 | 0.68 ± 0.38 | 0.001 |
| 3 | 20.05 ± 7.70 | 15.56 ± 7.36 | 0.001 | 1.00 ± 0.46 | 0.81 ± 0.43 | 0.07 |
| 4 | 20.18 ± 7.34 | 16.54 ± 7.38 | 0.004 | 1.03 ± 0.47 | 0.88 ± 0.42 | 0.13 |
| 5 | 20.27 ± 7.37 | 17.11 ± 7.40 | 0.08 | 1.03 ± 0.47 | 0.90 ± 0.42 | 0.17 |
| 6 | 20.10 ± 8.85 | 17.61 ± 7.45 | 0.09 | 1.03 ± 0.47 | 0.95 ± 0.43 | 0.25 |
| 7 | 20.16 ± 9.64 | 17.72 ± 7.71 | 0.08 | 1.04 ± 0.51 | 0.95 ± 0.42 | 0.24 |
| Mean 1st week | 13.62 ± 4.89 | 10.11 ± 4.37 | 0.001 | 0.94 ± 0.42 | 0.72 ± 0.33 | 0.04 |
| 8 | 21.02 ±10.10 | 18.13 ± 7.33 | 0.01 | 1.06 ± 0.49 | 0.96 ± 0.43 | 0.28 |
| 9 | 23.73 ± 8.04 | 18.20 ± 7.24 | 0.001 | 1.08 ± 0.54 | 0.98 ± 0.43 | 0.44 |
| 10 | 22.93 ± 9.48 | 18.44 ± 7.56 | 0.05 | 1.08 ± 0.60 | 0.98 ± 0.43 | 0.36 |
| 11 | 25.03 ± 8.22 | 19.36 ± 7.07 | 0.001 | 1.16 ± 0.60 | 1.04 ± 0.40 | 0.13 |
| 12 | 24.79 ± 8.94 | 19.53 ± 7.25 | 0.001 | 1.26 ± 0.53 | 1.04 ± 0.43 | 0.07 |
| 13 | 25.61 ± 6.90 | 19.75 ± 6.76 | 0.001 | 1.27 ± 0.50 | 1.03 ± 0.44 | 0.10 |
| 14 | 21.98 ± 7.92 | 20.50 ± 6.67 | 0.88 | 1.09 ± 0.54 | 1.05 ± 0.43 | 0.51 |
| Mean 2nd week | 19.27 ± 7.24 | 14.50 ± 5.60 | 0.01 | 0.95 ± 0.43 | 0.76 ± 0.34 | 0.06 |
| Day | Kcal/kg/Day | Protein g/kg/Day | ||||||
|---|---|---|---|---|---|---|---|---|
| All Patients n = 186 | Only PN n = 112 | PN-EN n = 74 | p-Value | All Patients n = 186 | Only PN n = 112 | PN-EN n = 74 | p-Value | |
| 1 | 14.46 ± 8.37 | 14.71 ± 8.58 | 14.07 ± 8.07 | 0.60 | 0.72 ± 0.46 | 0.73 ± 0.51 | 0.72 ± 0.39 | 0.88 |
| 2 | 19.92 ± 8.09 | 19.93 ± 8.37 | 19.91 ± 7.71 | 0.98 | 0.99 ± 0.52 | 0.99 ± 0.60 | 0.99 ± 0.40 | 0.94 |
| 3 | 20.82 ± 7.58 | 20.05 ± 7.70 | 21.93 ± 7.32 | 0.10 | 1.04 ± 0.45 | 1.00 ± 0.46 | 1.11 ± 0.43 | 0.11 |
| 4 | 21.18 ± 7.76 | 20.18 ± 7.34 | 22.42 ± 8.14 | 0.06 | 1.08 ± 0.48 | 1.03 ± 0.47 | 1.14 ± 0.49 | 0.13 |
| 5 | 21.19 ± 7.99 | 20.27 ± 7.37 | 22.14 ± 8.54 | 0.15 | 1.10 ± 0.51 | 1.03 ± 0.47 | 1.17 ± 0.54 | 0.07 |
| 6 | 21.41 ± 8.69 | 20.10 ± 8.85 | 22.56 ± 8.45 | 0.10 | 1.12 ± 0.49 | 1.03 ± 0.47 | 1.20 ± 0.50 | 0.05 |
| 7 | 21.99 ± 8.97 | 20.16 ± 9.64 | 23.42 ± 8.19 | 0.05 | 1.15 ± 0.52 | 1.04 ± 0.51 | 1.23 ± 0.52 | 0.04 |
| Mean 1st week | 15.56 ± 6.57 | 13.62 ± 4.89 | 16.84 ± 7.21 | 0.001 | 0.99 ± 0.40 | 0.94 ± 0.42 | 1.07 ± 0.37 | 0.04 |
| 8 | 22.37 ± 9.04 | 21.02 ±10.10 | 23.14 ± 8.37 | 0.26 | 1.12 ± 0.52 | 1.06 ± 0.49 | 1.15 ± 0.54 | 0.38 |
| 9 | 23.31 ± 7.83 | 23.73 ± 8.04 | 23.10 ± 7.80 | 0.73 | 1.14 ± 0.51 | 1.08 ± 0.54 | 1.17 ± 0.50 | 0.44 |
| 10 | 23.26 ± 9.42 | 22.93 ± 9.48 | 23.42 ± 9.49 | 0.83 | 1.15 ± 0.54 | 1.08 ± 0.60 | 1.19 ± 0.50 | 0.38 |
| 11 | 21.48 ± 8.55 | 25.03 ± 8.22 | 19.99 ± 8.32 | 0.030 | 1.06 ± 0.52 | 1.16 ± 0.60 | 1.02 ± 0.48 | 0.33 |
| 12 | 23.40 ± 9.04 | 24.79 ± 8.94 | 22.76 ± 9.13 | 0.44 | 1.18 ± 0.51 | 1.26 ± 0.53 | 1.14 ± 0.50 | 0.44 |
| 13 | 23.91 ± 7.93 | 25.61 ± 6.90 | 23.20 ± 8.31 | 0.32 | 1.18 ± 0.50 | 1.27 ± 0.50 | 1.14 ± 0.50 | 0.40 |
| 14 | 23.36 ± 10.26 | 21.98 ± 7.92 | 23.97 ± 11.23 | 0.58 | 1.14 ± 0.60 | 1.09 ± 0.54 | 1.16 ± 0.63 | 0.71 |
| Mean 2nd week | 19.94 ± 6.72 | 19.27 ± 7.24 | 20.96 ± 5.74 | 0.09 | 1.01 ± 0.41 | 0.95 ± 0.43 | 1.08 ± 0.36 | 0.03 |
| Variables | Hazard Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Mean g of protein/kg/day | 0.29 (0.18–0.47) | 0.001 |
| Mechanical ventilation | 0.51 (0.26–1.29) | 0.15 |
| Days on mechanical ventilation | 0.85 (0.81–0.89) | 0.001 |
| Vasoactive drug support | 0.90 (0.89–1.87) | 0.35 |
| Mean length of ICU stay | 0.96 (0.92–0.99) | 0.008 |
| Catheter-relation infections | 3.91 (0.84–8.83) | 0.115 |
| All Patients (n = 186) | PN Only (n = 112) | PN-EN (n = 74) | p-Value | ||
|---|---|---|---|---|---|
| Lipid profile | |||||
| Cholesterol, mean ± SD (mg/dL) | Day 1 | 99 ± 47 | 102 ± 49 | 96 ± 43 | 0.53 |
| Day 3 | 99 ± 38 | 99 ± 35 | 99 ± 44 | 0.97 | |
| Day 7 | 113 ± 42 | 107 ± 31 | 118 ± 48 | 0.26 | |
| ICU discharge | 123 ± 48 | 119 ± 38 | 130 ± 61 | 0.28 | |
| High cholesterol levels (>200 mg/dL), n (%) | 8 (4.3) | 1 (0.9) | 7 (9.5) | 0.32 | |
| Triglycerides, mean ± SD (mg/dL) | Day 1 | 148 ± 114 | 134 ± 100 | 168 ± 129 | 0.14 |
| Day 3 | 186 ± 110 | 173 ± 97 | 203 ± 126 | 0.20 | |
| Day 7 | 187 ± 87 | 178 ± 79 | 194 ± 94 | 0.44 | |
| ICU discharge | 185 ± 101 | 190 ± 86 | 176 ± 124 | 0.54 | |
| Hypertriglyceridemia (>350 mg/dL), n (%) | 16 (8.6) | 6 (5.4) | 10 (13.5) | 0.24 | |
| Liver parameters | |||||
| Bilirubin, mean ± SD (mg/dL) | Day 1 | 2.47 ± 1.55 | 1.31 ± 1.25 | 3.62 ± 1.92 | 0.11 |
| Day 3 | 2.46 ± 1.36 | 1.54 ± 1.20 | 3.42 ± 1.59 | 0.32 | |
| Day 7 | 2.23 ± 1.36 | 2.74 ± 1.32 | 1.64 ± 1.39 | 0.87 | |
| ICU discharge | 2.51 ± 1.22 | 2.67 ± 1.16 | 2.25 ± 1.31 | 0.72 | |
| High bilirubin levels (>1.23 mg/dL), n (%) | 77 (41.4) | 46 (41.1) | 31 (41.9) | 0.70 | |
| High transaminases (AST or ALT > 40 IU/L), n (%) | 108 (58.1) | 58 (51.8) | 50 (67.6) | 0.68 | |
| High ALP levels (>129 UI/L), n (%) | 91 (48.9) | 51 (45.5) | 40 (54.0) | 0.05 | |
| High GGT levels (>67 IU/L), n (%) | 132 (71.0) | 75 (67.0) | 57 (77.0) | 0.80 | |
| Liver dysfunction, n (%) | 75 (40.3) | 48 (42.9) | 27 (36.5) | 0.41 | |
| Blood proteins and C-reactive protein | |||||
| Prealbumin, mean ± SD (mg/L) | Day 1 | 117.5 ± 70.7 | 115.9 ± 72.9 | 119.9 ± 68.1 | 0.80 |
| Day 3 | 108.4 ± 64.5 | 106.1 ± 68.7 | 112.9 ± 55.9 | 0.64 | |
| Day 7 | 144.7 ± 68.7 | 149.1 ± 69.8 | 140.9 ± 68.8 | 0.65 | |
| ICU discharge | 164.9 ± 77.8 | 171.8 ± 81.2 | 150.7 ± 69.8 | 0.27 | |
| Low prealbumin levels, <200 mg/L, n (%) | 117 (62.9) | 72 (64.3) | 45 (60.8) | 0.43 | |
| Albumin, ± SD (g/L) | Day 1 | 2.54 ± 0.65 | 2.51 ± 0.62 | 2.58 ± 0.71 | 0.50 |
| Day 3 | 2.39 ± 0.52 | 2.40 ± 0.52 | 2.37 ± 0.51 | 0.74 | |
| Day 7 | 2.42 ± 0.57 | 2.45 ± 0.55 | 2.39 ± 0.59 | 0.62 | |
| ICU discharge | 2.53 ± 0.63 | 2.52 ± 0.64 | 2.54 ± 0.62 | 0.87 | |
| Low albumin levels, <30 g/L, n (%) | 175 (94.1) | 107 (95.5) | 68 (91.9) | 0.89 | |
| C-reactive protein, mean ± SD (mg/L) | Day 1 | 173.6 ± 144.2 | 171.2 ± 133.5 | 177.3 ± 160.1 | 0.79 |
| Day 3 | 152.8 ± 128.6 | 168.8 ± 135.6 | 128.09 ± 113.9 | 0.07 | |
| Day 7 | 144.7 ± 90.6 | 120.5 ± 97.8 | 129.62 ± 81.3 | 0.10 | |
| ICU discharge | 104.2 ± 109.9 | 119.4 ± 123.7 | 76.07 ± 71.2 | 0.03 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Delgado, J.C.; Grau-Carmona, T.; Mor-Marco, E.; Bordeje-Laguna, M.L.; Portugal-Rodriguez, E.; Lorencio-Cardenas, C.; Vera-Artazcoz, P.; Macaya-Redin, L.; Llorente-Ruiz, B.; Iglesias-Rodriguez, R.; et al. Parenteral Nutrition: Current Use, Complications, and Nutrition Delivery in Critically Ill Patients. Nutrients 2023, 15, 4665. https://doi.org/10.3390/nu15214665
Lopez-Delgado JC, Grau-Carmona T, Mor-Marco E, Bordeje-Laguna ML, Portugal-Rodriguez E, Lorencio-Cardenas C, Vera-Artazcoz P, Macaya-Redin L, Llorente-Ruiz B, Iglesias-Rodriguez R, et al. Parenteral Nutrition: Current Use, Complications, and Nutrition Delivery in Critically Ill Patients. Nutrients. 2023; 15(21):4665. https://doi.org/10.3390/nu15214665
Chicago/Turabian StyleLopez-Delgado, Juan Carlos, Teodoro Grau-Carmona, Esther Mor-Marco, Maria Luisa Bordeje-Laguna, Esther Portugal-Rodriguez, Carol Lorencio-Cardenas, Paula Vera-Artazcoz, Laura Macaya-Redin, Beatriz Llorente-Ruiz, Rayden Iglesias-Rodriguez, and et al. 2023. "Parenteral Nutrition: Current Use, Complications, and Nutrition Delivery in Critically Ill Patients" Nutrients 15, no. 21: 4665. https://doi.org/10.3390/nu15214665
APA StyleLopez-Delgado, J. C., Grau-Carmona, T., Mor-Marco, E., Bordeje-Laguna, M. L., Portugal-Rodriguez, E., Lorencio-Cardenas, C., Vera-Artazcoz, P., Macaya-Redin, L., Llorente-Ruiz, B., Iglesias-Rodriguez, R., Monge-Donaire, D., Martinez-Carmona, J. F., Sanchez-Ales, L., Sanchez-Miralles, A., Crespo-Gomez, M., Leon-Cinto, C., Flordelis-Lasierra, J. L., Servia-Goixart, L., & on behalf of the ENPIC Study Group. (2023). Parenteral Nutrition: Current Use, Complications, and Nutrition Delivery in Critically Ill Patients. Nutrients, 15(21), 4665. https://doi.org/10.3390/nu15214665