
Association between Dietary Acid Load and Hypertension in Chinese Adults: Analysis of the China Health and Nutrition Survey (2009)



Abstract
:1. Introduction
2. Materials and Methods
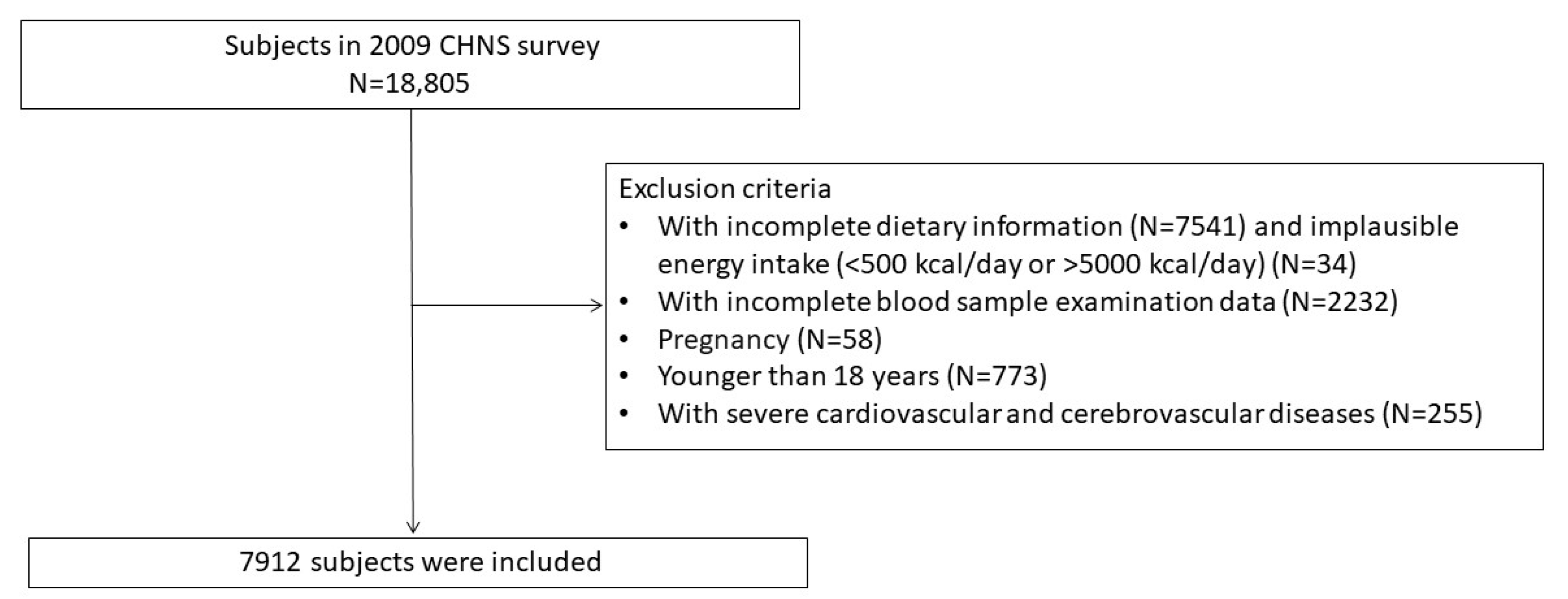
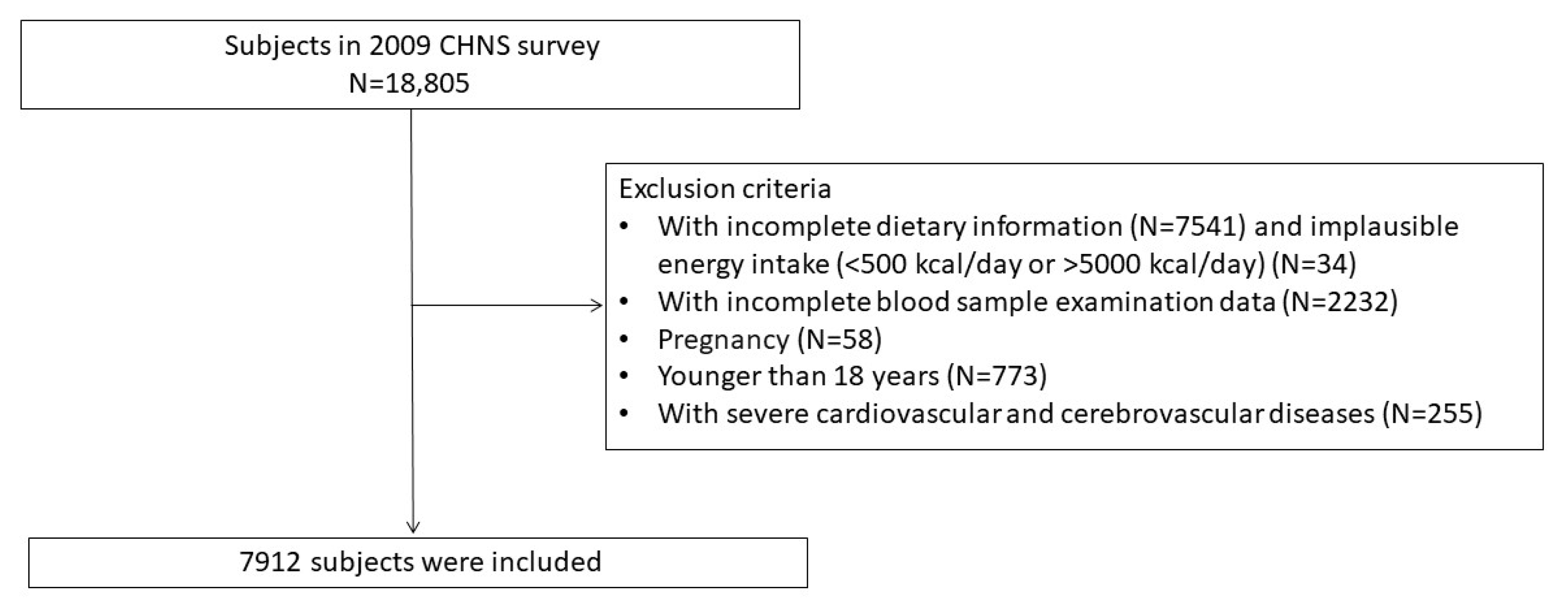
2.1. Data Sources and Study Population
2.2. Evaluation of Diet, PRAL and NEAP
2.3. Definition of Hypertension
2.4. Other Variables
2.5. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. The Correlation between DAL and Hypertension
3.2.1. PRAL and Hypertension
3.2.2. NEAP and Hyperuricemia
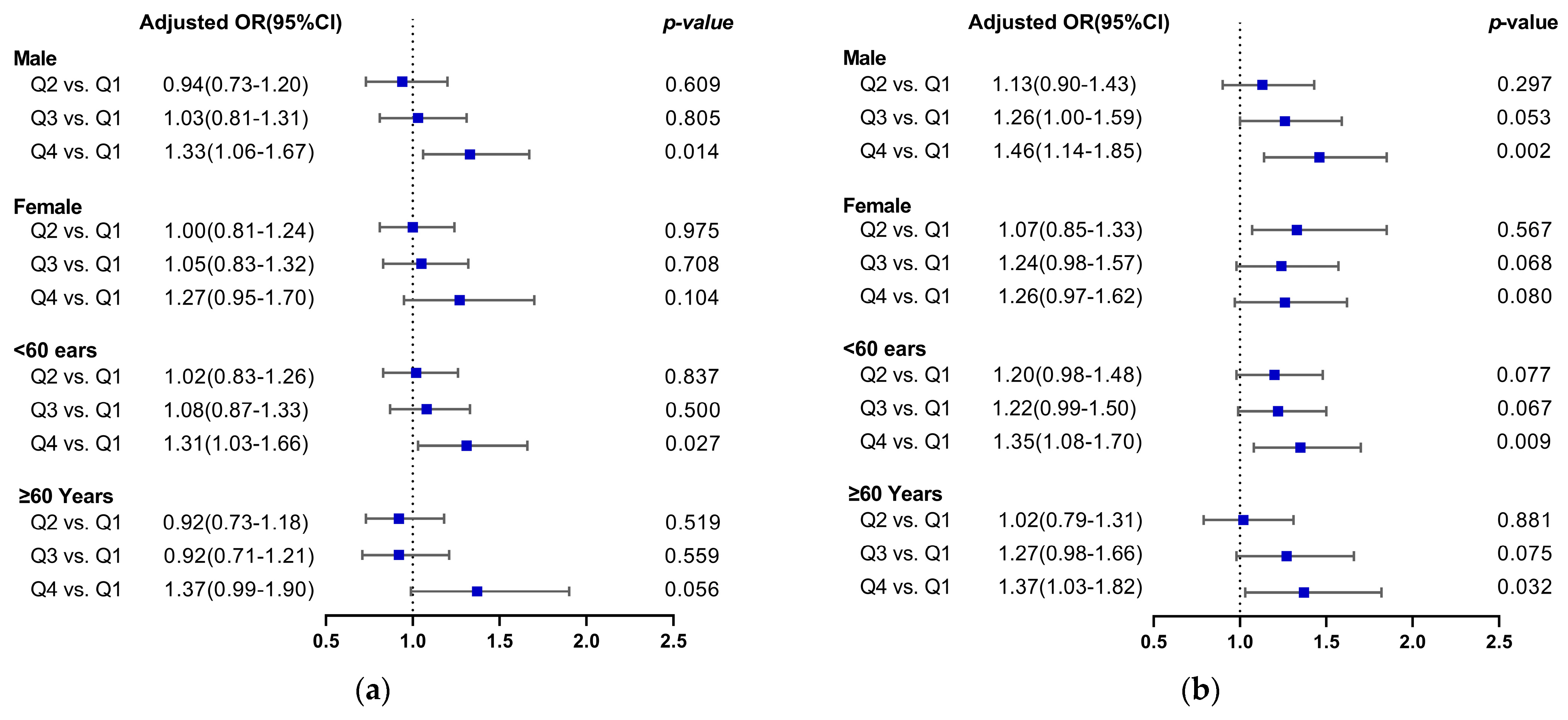
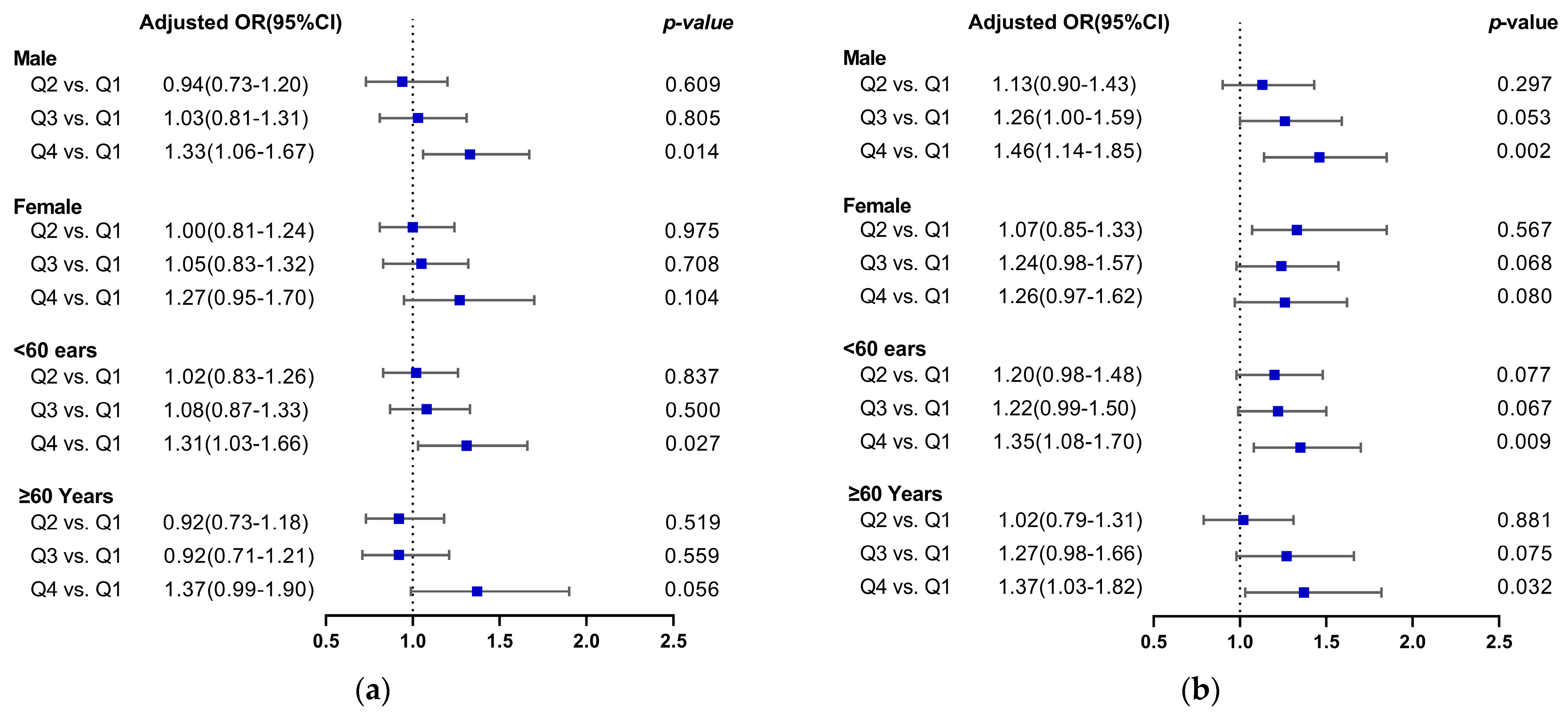
3.2.3. Stratification Analysis Based on Gender and Age
3.3. Sensitivity Analysis
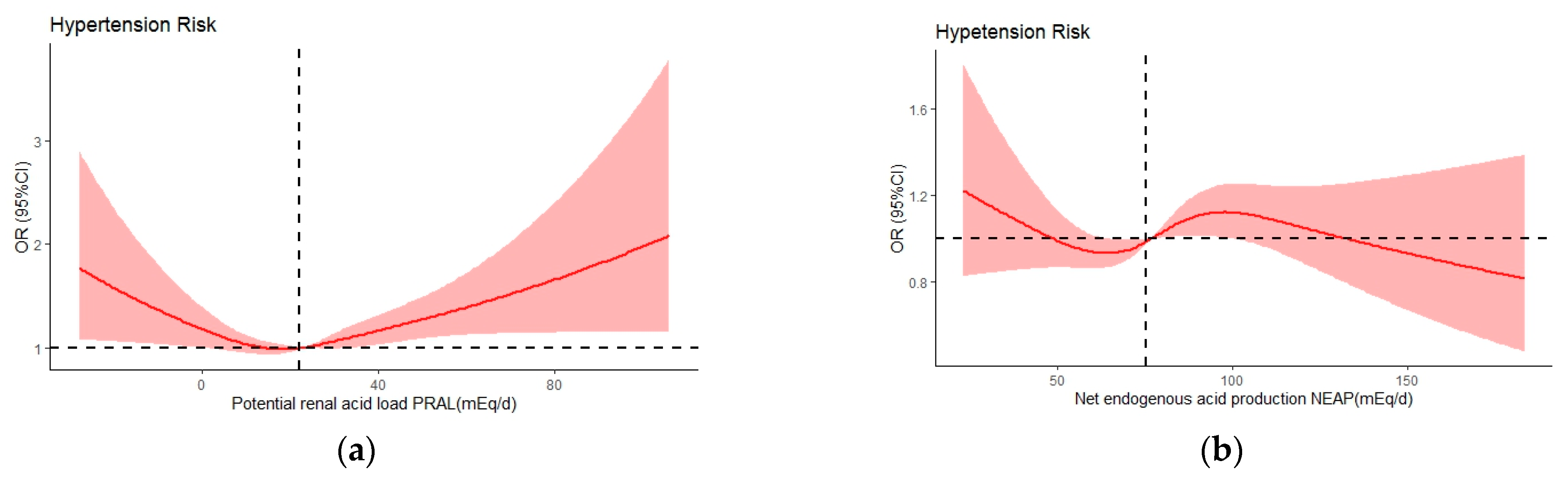
3.4. DAL and Hypertension Risk Based on Restricted Cubic Spline Analysis (RCS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moick, S.; Sommer, I.; Gartlehner, G. WHO Guideline for the Pharmacological Treatment of Hypertension in Adults. Gesundheitswesen Bundesverb. Arzte Offentlichen Gesundheitsdienstes 2023, 85, 139–142. [Google Scholar] [CrossRef]
- Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [CrossRef]
- Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [CrossRef]
- Valenzuela, P.L.; Carrera-Bastos, P.; Gálvez, B.G.; Ruiz-Hurtado, G.; Ordovas, J.M.; Ruilope, L.M.; Lucia, A. Lifestyle interventions for the prevention and treatment of hypertension. Nat. Rev. Cardiol. 2021, 18, 251–275. [Google Scholar] [CrossRef]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Filippou, C.; Tatakis, F.; Polyzos, D.; Manta, E.; Thomopoulos, C.; Nihoyannopoulos, P.; Tousoulis, D.; Tsioufis, K. Overview of salt restriction in the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean diet for blood pressure reduction. Rev. Cardiovasc. Med. 2022, 23, 36. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; O’Keefe, J. Low-grade metabolic acidosis as a driver of chronic disease: A 21st century public health crisis. Open Heart 2021, 8, e001730. [Google Scholar] [CrossRef] [PubMed]
- Frassetto, L.A.; Todd, K.M.; Morris, R.C., Jr.; Sebastian, A. Estimation of net endogenous noncarbonic acid production in humans from diet potassium and protein contents. Am. J. Clin. Nutr. 1998, 68, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.M.; Sergi, D.; Colombari, S.; Capatti, E.; Situlin, R.; Biolo, G.; Di Girolamo, F.G.; Lazzer, S.; Šimunič, B.; Pišot, R.; et al. Dietary Acid Load but Not Mediterranean Diet Adherence Score Is Associated with Metabolic and Cardiovascular Health State: A Population Observational Study From Northern Italy. Front. Nutr. 2022, 9, 828587. [Google Scholar] [CrossRef] [PubMed]
- Incollingo Rodriguez, A.C.; Epel, E.S.; White, M.L.; Standen, E.C.; Seckl, J.R.; Tomiyama, A.J. Hypothalamic-pituitary-adrenal axis dysregulation and cortisol activity in obesity: A systematic review. Psychoneuroendocrinology 2015, 62, 301–318. [Google Scholar] [CrossRef]
- Remer, T.; Dimitriou, T.; Manz, F. Dietary potential renal acid load and renal net acid excretion in healthy, free-living children and adolescents. Am. J. Clin. Nutr. 2003, 77, 1255–1260. [Google Scholar] [CrossRef]
- Osuna-Padilla, I.A.; Leal-Escobar, G.; Garza-García, C.A.; Rodríguez-Castellanos, F.E. Dietary acid load: Mechanisms and evidence of its health repercussions. Nefrologia 2019, 39, 343–354. [Google Scholar] [CrossRef]
- Remer, T.; Manz, F. Potential renal acid load of foods and its influence on urine pH. J. Am. Diet. Assoc. 1995, 95, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Adeva, M.M.; Souto, G. Diet-induced metabolic acidosis. Clin. Nutr. 2011, 30, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Quade, B.N.; Parker, M.D.; Occhipinti, R. The therapeutic importance of acid-base balance. Biochem. Pharmacol. 2021, 183, 114278. [Google Scholar] [CrossRef]
- Krupp, D.; Esche, J.; Mensink, G.B.M.; Klenow, S.; Thamm, M.; Remer, T. Dietary Acid Load and Potassium Intake Associate with Blood Pressure and Hypertension Prevalence in a Representative Sample of the German Adult Population. Nutrients 2018, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Engberink, M.F.; Bakker, S.J.; Brink, E.J.; van Baak, M.A.; van Rooij, F.J.; Hofman, A.; Witteman, J.C.; Geleijnse, J.M. Dietary acid load and risk of hypertension: The Rotterdam Study. Am. J. Clin. Nutr. 2012, 95, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.W.; Ji, G.Y.; Jiang, Q.; Wang, P.; Huang, R.; Ma, W.J.; Chen, Z.H.; Peng, J.W. Association between dietary acid load and the risk of hypertension among adults from South China: Result from nutrition and health survey (2015–2017). BMC Public Health 2019, 19, 1599. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989-2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Su, C.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B. Secular Trends in Energy and Macronutrient Intakes and Distribution among Adult Females (1991-2015): Results from the China Health and Nutrition Survey. Nutrients 2018, 10, 115. [Google Scholar] [CrossRef]
- Du, S.; Batis, C.; Wang, H.; Zhang, B.; Zhang, J.; Popkin, B.M. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am. J. Clin. Nutr. 2014, 99, 334–343. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.; Adams, R.; Carnethon, M.; De Simone, G.; Ferguson, T.B.; Flegal, K.; Ford, E.; Furie, K.; Go, A.; Greenlund, K.; et al. Heart disease and stroke statistics—2009 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2009, 119, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Zou, Q.; Wang, H.; Su, C.; Du, W.; Ouyang, Y.; Jia, X.; Wang, Z.; Ding, G.; Zhang, B. Longitudinal association between physical activity and blood pressure, risk of hypertension among Chinese adults: China Health and Nutrition Survey 1991–2015. Eur. J. Clin. Nutr. 2021, 75, 274–282. [Google Scholar] [CrossRef]
- Bardin, T.; Richette, P. Definition of hyperuricemia and gouty conditions. Curr. Opin. Rheumatol. 2014, 26, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Chinese expert consensus on the treatment of hyperuricemia and gout. China Endocrinol. Metab. 2013, 29, 913–920. [CrossRef]
- Diagnosis and classification of diabetes mellitus. Diabetes Care 2013, 36 (Suppl. S1), S67–S74. [CrossRef] [PubMed]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2014, 63, 713–735. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B.E.; Okubo, H.; Sasaki, S. Higher dietary acid load is weakly associated with higher adiposity measures and blood pressure in Japanese adults: The National Health and Nutrition Survey. Nutr. Res. 2017, 44, 67–75. [Google Scholar] [CrossRef]
- Chen, S.W.; Chen, Z.H.; Liang, Y.H.; Wang, P.; Peng, J.W. Elevated hypertension risk associated with higher dietary acid load: A systematic review and meta-analysis. Clin. Nutr. ESPEN 2019, 33, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Curhan, G.C.; Forman, J.P. Diet-dependent net acid load and risk of incident hypertension in United States women. Hypertension 2009, 54, 751–755. [Google Scholar] [CrossRef]
- Di Giosia, P.; Giorgini, P.; Stamerra, C.A.; Petrarca, M.; Ferri, C.; Sahebkar, A. Gender Differences in Epidemiology, Pathophysiology, and Treatment of Hypertension. Curr. Atheroscler. Rep. 2018, 20, 13. [Google Scholar] [CrossRef]
- Luis, D.; Huang, X.; Riserus, U.; Sjögren, P.; Lindholm, B.; Arnlöv, J.; Cederholm, T.; Carrero, J.J. Estimated dietary acid load is not associated with blood pressure or hypertension incidence in men who are approximately 70 years old. J. Nutr. 2015, 145, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Scialla, J.J.; Anderson, C.A. Dietary acid load: A novel nutritional target in chronic kidney disease? Adv. Chronic Kidney Dis. 2013, 20, 141–149. [Google Scholar] [CrossRef]
- Fernández-Llama, P.; Ayasreh, N.; Calero, F. Hypertension in the elderly: What we need to know. Hipertens. Y Riesgo Vasc. 2021, 38, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Rylander, R.; Tallheden, T.; Vormann, J. Acid-base conditions regulate calcium and magnesium homeostasis. Magnes. Res. 2009, 22, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Stroup, B.M.; Sawin, E.A.; Murali, S.G.; Binkley, N.; Hansen, K.E.; Ney, D.M. Amino Acid Medical Foods Provide a High Dietary Acid Load and Increase Urinary Excretion of Renal Net Acid, Calcium, and Magnesium Compared with Glycomacropeptide Medical Foods in Phenylketonuria. J. Nutr. Metab. 2017, 2017, 1909101. [Google Scholar] [CrossRef] [PubMed]
- Kesteloot, H.; Tzoulaki, I.; Brown, I.J.; Chan, Q.; Wijeyesekera, A.; Ueshima, H.; Zhao, L.; Dyer, A.R.; Unwin, R.J.; Stamler, J.; et al. Relation of urinary calcium and magnesium excretion to blood pressure: The International Study Of Macro- And Micro-nutrients And Blood Pressure and The International Cooperative Study On Salt, Other Factors, And Blood Pressure. Am. J. Epidemiol. 2011, 174, 44–51. [Google Scholar] [CrossRef]
- Rodrigues Neto Angéloco, L.; Arces de Souza, G.C.; Almeida Romão, E.; Garcia Chiarello, P. Alkaline Diet and Metabolic Acidosis: Practical Approaches to the Nutritional Management of Chronic Kidney Disease. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2018, 28, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Behers, B.J.; Melchor, J.; Behers, B.M.; Meng, Z.; Swanson, P.J.; Paterson, H.I.; Mendez Araque, S.J.; Davis, J.L.; Gerhold, C.J.; Shah, R.S.; et al. Vitamins and Minerals for Blood Pressure Reduction in the General, Normotensive Population: A Systematic Review and Meta-Analysis of Six Supplements. Nutrients 2023, 15, 4223. [Google Scholar] [CrossRef]
- Beam, A.; Clinger, E.; Hao, L. Effect of Diet and Dietary Components on the Composition of the Gut Microbiota. Nutrients 2021, 13, 2795. [Google Scholar] [CrossRef]
- Li, J.; Yang, X.; Zhou, X.; Cai, J. The Role and Mechanism of Intestinal Flora in Blood Pressure Regulation and Hypertension Development. Antioxid. Redox Signal. 2021, 34, 811–830. [Google Scholar] [CrossRef]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N.R.C.; Li, Q.; Lackland, D.T.; Leung, A.A.; Anderson, C.A.M.; et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: Systematic review and meta-analysis of randomised trials. BMJ 2020, 368, m315. [Google Scholar] [CrossRef]
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.C.; He, F.J.; Tan, M.; Cappuccio, F.P.; Neal, B.; Woodward, M.; Cogswell, M.E.; McLean, R.; Arcand, J.; MacGregor, G.; et al. The International Consortium for Quality Research on Dietary Sodium/Salt (TRUE) position statement on the use of 24-hour, spot, and short duration (<24 hours) timed urine collections to assess dietary sodium intake. J. Clin. Hypertens. 2019, 21, 700–709. [Google Scholar] [CrossRef]
- Park, Y.; Dodd, K.W.; Kipnis, V.; Thompson, F.E.; Potischman, N.; Schoeller, D.A.; Baer, D.J.; Midthune, D.; Troiano, R.P.; Bowles, H.; et al. Comparison of self-reported dietary intakes from the Automated Self-Administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. Am. J. Clin. Nutr. 2018, 107, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Covas, M.I.; Marrugat, J.; Vila, J.; Pena, A.; Alcántara, M.; Masiá, R. Use of a three-day estimated food record, a 72-hour recall and a food-frequency questionnaire for dietary assessment in a Mediterranean Spanish population. Clin. Nutr. 2001, 20, 429–437. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.; Cameron, C.; Butcher, E.; Cook, N.R.; Woodward, M.; Campbell, N.R.C. Comparison of 24-hour urine and 24-hour diet recall for estimating dietary sodium intake in populations: A systematic review and meta-analysis. J. Clin. Hypertens. 2019, 21, 1753–1762. [Google Scholar] [CrossRef]
- Chmielewski, J.; Carmody, J.B. Dietary sodium, dietary potassium, and systolic blood pressure in US adolescents. J. Clin. Hypertens. 2017, 19, 904–909. [Google Scholar] [CrossRef]
- Wang, Y.J.; Yeh, T.L.; Shih, M.C.; Tu, Y.K.; Chien, K.L. Dietary Sodium Intake and Risk of Cardiovascular Disease: A Systematic Review and Dose-Response Meta-Analysis. Nutrients 2020, 12, 2934. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; Eguchi, M.; Kurotani, K.; Kochi, T.; Pham, N.M.; Ito, R.; Kuwahara, K.; Tsuruoka, H.; Mizoue, T.; Kabe, I.; et al. High dietary acid load is associated with increased prevalence of hypertension: The Furukawa Nutrition and Health Study. Nutrition 2015, 31, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, I.; Maher, T.; Hulter, H.N.; Schambelan, M.; Sebastian, A. Effect of diet on plasma acid-base composition in normal humans. Kidney Int. 1983, 24, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Angeloco, L.R.N.; Arces de Souza, G.C.; Romão, E.A.; Frassetto, L.; Chiarello, P.G. Association of dietary acid load with serum bicarbonate in chronic kidney disease (CKD) patients. Eur. J. Clin. Nutr. 2020, 74, 69–75. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 7412) | Hypertension (n = 2133) | Non-Hypertension (n = 5779) | p-Value |
|---|---|---|---|---|
| Age (years) | 50.2 (14.9) | 58.7 (12.9) | 47.1 (14.3) | <0.0001 |
| Gender | ||||
| Male | 3725 (47.1%) | 1058 (49.6%) | 2667 (46.1%) | <0.01 |
| Female | 4187 (52.9%) | 1075 (50.4%) | 3112 (53.9%) | |
| PRAL 1 group | 24.7 (17.3) | 24.9 (18.1) | 24.6 (16.9) | 0.532 |
| NEAP 2 group | 76.6 (22.9) | 77.4 (23.1) | 76.4 (22.8) | 0.085 |
| Marital status | ||||
| Single | 489 (6.2%) | 38 (1.8%) | 451 (7.8%) | <0.0001 |
| Married | 6677 (84.4%) | 1770 (83%) | 4907 (84.9%) | |
| Other | 746 (9.4%) | 325 (15.2%) | 421 (7.3%) | |
| Region | ||||
| Urban | 2416 (30.5%) | 660 (30.9%) | 1756 (30.4%) | 0.633 |
| Rural | 5496 (69.5%) | 1473 (69.1%) | 4023 (69.6%) | |
| Education level | ||||
| Low | 3460 (43.7%) | 1192 (55.9%) | 2268 (39.2%) | <0.0001 |
| Middle | 4088 (51.7%) | 888 (41.6%) | 3200 (55.4%) | |
| High | 364 (4.6%) | 53 (2.5%) | 311 (5.4%) | |
| Smoking status | ||||
| No | 5462 (69.0%) | 1426 (66.9%) | 4036 (69.8%) | <0.05 |
| Yes | 2450 (31.0%) | 707 (33.1%) | 1743 (30.2%) | |
| Alcohol intake | ||||
| No | 6234 (78.8%) | 1621 (76%) | 4613 (79.8%) | <0.0001 |
| Yes | 1678 (21.2%) | 512 (24%) | 1166 (20.2%) | |
| Physical activity 3 (MET·hours/week) | 131.00 (70.63–239.43) | 123.83 (53.33–227.33) | 133.08 (73.67–243.92) | <0.0001 |
| Hyperuricemia | ||||
| Yes | 1195 (15.1%) | 477 (22.4%) | 718 (12.4%) | <0.0001 |
| No | 6717 (84.9%) | 1656 (77.6%) | 5061 (87.6%) | |
| Diabetes | ||||
| Yes | 827 (10.5%) | 401 (18.8%) | 426 (7.4%) | <0.0001 |
| No | 7085 (89.5%) | 1732 (81.2%) | 5353 (92.6%) | |
| TC 4 (mmol/L) | 4.86 (1.00) | 5.10 (1.02) | 4.76 (0.98) | <0.0001 |
| TG 5 (mmol/L) | 1.65 (1.44) | 1.93 (1.57) | 1.55 (1.38) | <0.0001 |
| LDL-C 6 (mmol/L) | 2.97 (0.98) | 3.16 (1.03) | 2.90 (0.96) | <0.0001 |
| HDL_C 7 (mmol/L) | 1.44 (0.50) | 1.42 (0.62) | 1.45 (0.45) | 0.065 |
| eGFR 8 (mL/min/1.73m2) | 79.6 (16.7) | 72.7 (16.4) | 82.2 (16.1) | <0.0001 |
| BMI 9 (kg/m2) | 23.3 (3.4) | 24.6 (3.7) | 22.8 (3.2) | <0.0001 |
| Sleep duration (hours) | ||||
| 6–9 | 5367 (67.8%) | 1371 (64.3%) | 3996 (69.2%) | <0.0001 |
| ≤6 | 756 (9.6%) | 276 (12.9%) | 480 (8.3%) | |
| ≥9 | 1789 (22.6%) | 486 (22.8%) | 1303 (22.5%) |
| Nutrients | Hypertension | Non-Hypertension | p-Value |
|---|---|---|---|
| Energy (Kcal) | 1836.29 (1450.32–2300.57) | 1897.18 (1521.66–2335.36) | <0.0001 |
| Carbohydrate (g/1000 kcal) | 164.84 (143.12–187.41) | 166.23 (145.15–188.09) | 0.179 |
| Protein (g/1000 kcal) | 39.22 (33.79–47.32) | 38.42 (33.05–46.21) | <0.005 |
| Animal protein (g/1000 kcal) | 13.98 (6.53–24.28) | 14.35 (6.73–23.95) | 0.615 |
| Plant protein (g/1000 kcal) | 22.92 (18.77–27.80) | 22.23 (18.37–27.09) | <0.005 |
| Fat (g/1000 kcal) | 22.26 (14.02–30.10) | 22.10 (14.11–29.66) | 0.539 |
| Cholesterol (mg/1000 kcal) | 172.31 (82.71–283.74) | 167.66 (86.42–266.41) | 0.41 |
| Dietary fiber (g/1000 kcal) | 5.83 (4.34–7.78) | 5.66 (4.31–7.54) | 0.112 |
| Calcium (mg/1000 kcal) | 220.49 (164.43–298.55) | 206.77 (156.41–277.70) | <0.0001 |
| Phosphorous (mg/1000 kcal) | 570.27 (502.62–651.95) | 558.27 (492.14–636.08) | <0.0001 |
| Potassium (mg/1000 kcal) | 996.53 (831.31–1219.34) | 996.24 (831.93–1210.87) | 0.744 |
| Magnesium (mg/1000 kcal) | 162.34 (140.08–189.20) | 160.96 (138.85–186.66) | 0.09 |
| Sodium (mg/1000 kcal) | 368.13 (212.67–591.92) | 333.92 (201.38–591.92) | <0.005 |
| PRAL | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Q1 | 1 (ref) | 1 (ref) | 1 (ref) | |||
| Q2 | 0.92 (0.81–1.07) | 0.283 | 0.95 (0.81–1.11) | 0.481 | 0.97 (0.83–1.14) | 0.725 |
| Q3 | 0.88 (0.76–1.01) | 0.072 | 0.99 (0.84–1.15) | 0.849 | 1.03 (0.87–1.22) | 0.727 |
| Q4 | 1.03 (0.90–1.19) | 0.646 | 1.24 (1.06–1.46) | <0.01 | 1.34 (1.10–1.62) | <0.01 |
| NEAP | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Q1 | 1 (ref) | 0.001 | 1 (ref) | 1 (ref) | ||
| Q2 | 0.92 (0.81–1.07) | 0.283 | 1.07 (0.91–1.25) | 0.423 | 1.09 (0.93–1.28) | 0.303 |
| Q3 | 0.88 (0.76–1.01) | 0.072 | 1.17 (1.00–1.37) | 0.051 | 1.12 (1.03–1.43) | <0.05 |
| Q4 | 1.03 (0.90–1.19) | 0.646 | 1.23 (1.05–1.44) | <0.05 | 1.29 (1.09–1.53) | <0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, F.; Zhang, M.; Wang, R.; Sun, M.; Zhang, Z.; Qiao, Y.; Zhang, Z. Association between Dietary Acid Load and Hypertension in Chinese Adults: Analysis of the China Health and Nutrition Survey (2009). Nutrients 2023, 15, 4664. https://doi.org/10.3390/nu15214664
Lin F, Zhang M, Wang R, Sun M, Zhang Z, Qiao Y, Zhang Z. Association between Dietary Acid Load and Hypertension in Chinese Adults: Analysis of the China Health and Nutrition Survey (2009). Nutrients. 2023; 15(21):4664. https://doi.org/10.3390/nu15214664
Chicago/Turabian StyleLin, Feng, Min Zhang, Ruoyu Wang, Meng Sun, Zongfeng Zhang, Yanjiang Qiao, and Zhaofeng Zhang. 2023. "Association between Dietary Acid Load and Hypertension in Chinese Adults: Analysis of the China Health and Nutrition Survey (2009)" Nutrients 15, no. 21: 4664. https://doi.org/10.3390/nu15214664
APA StyleLin, F., Zhang, M., Wang, R., Sun, M., Zhang, Z., Qiao, Y., & Zhang, Z. (2023). Association between Dietary Acid Load and Hypertension in Chinese Adults: Analysis of the China Health and Nutrition Survey (2009). Nutrients, 15(21), 4664. https://doi.org/10.3390/nu15214664