
Pro-Inflammatory Diets Are Associated with Frailty in an Urban Middle-Aged African American and White Cohort

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. HANDLS Study
2.2. Study Participants
2.3. Participant Characteristics
2.4. Dietary Collection Method
2.5. Dietary Inflammatory Index (DII)
2.6. Frailty
2.7. Statistical Analyses
3. Results
3.1. Sample Characteristics
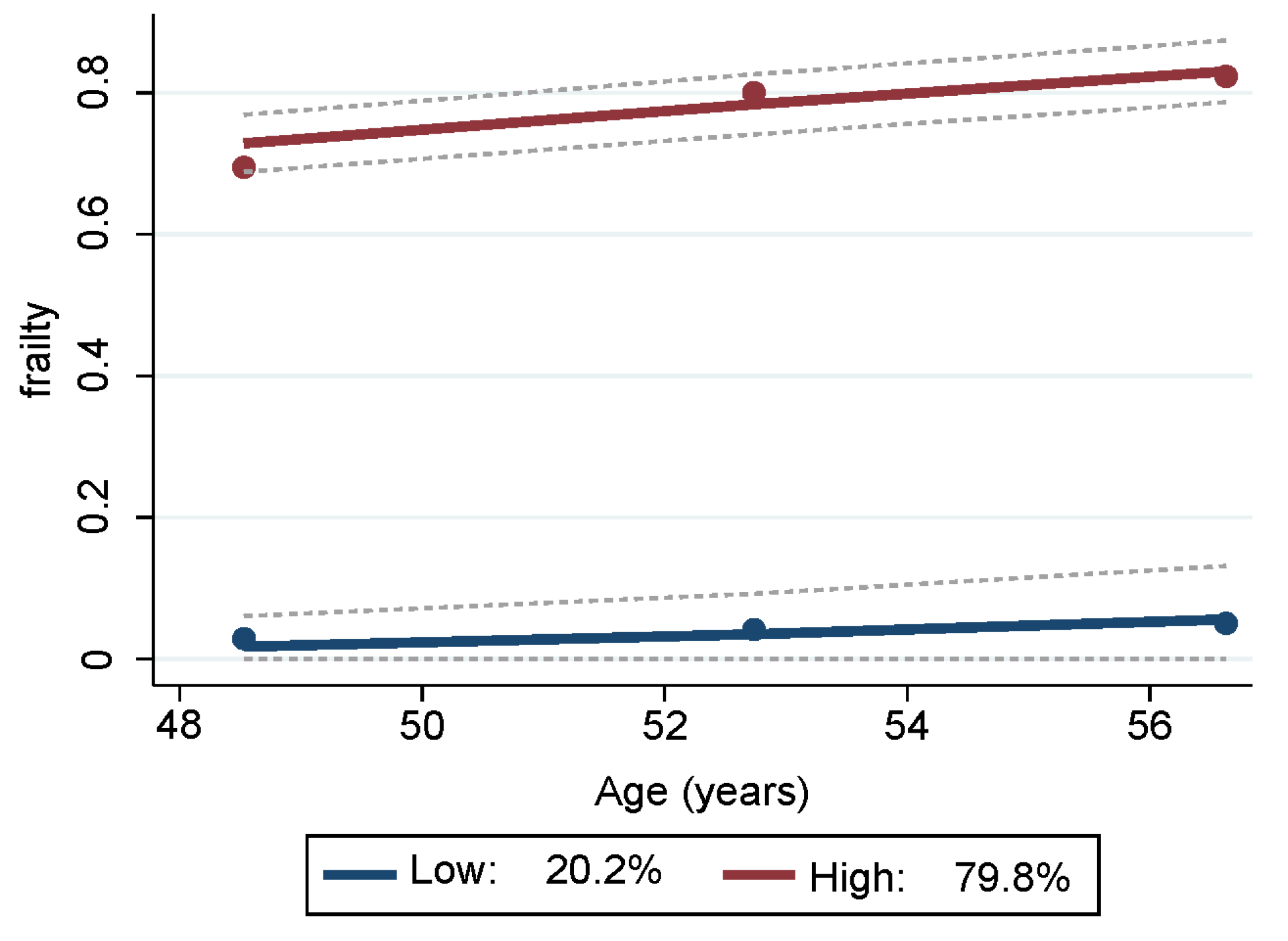
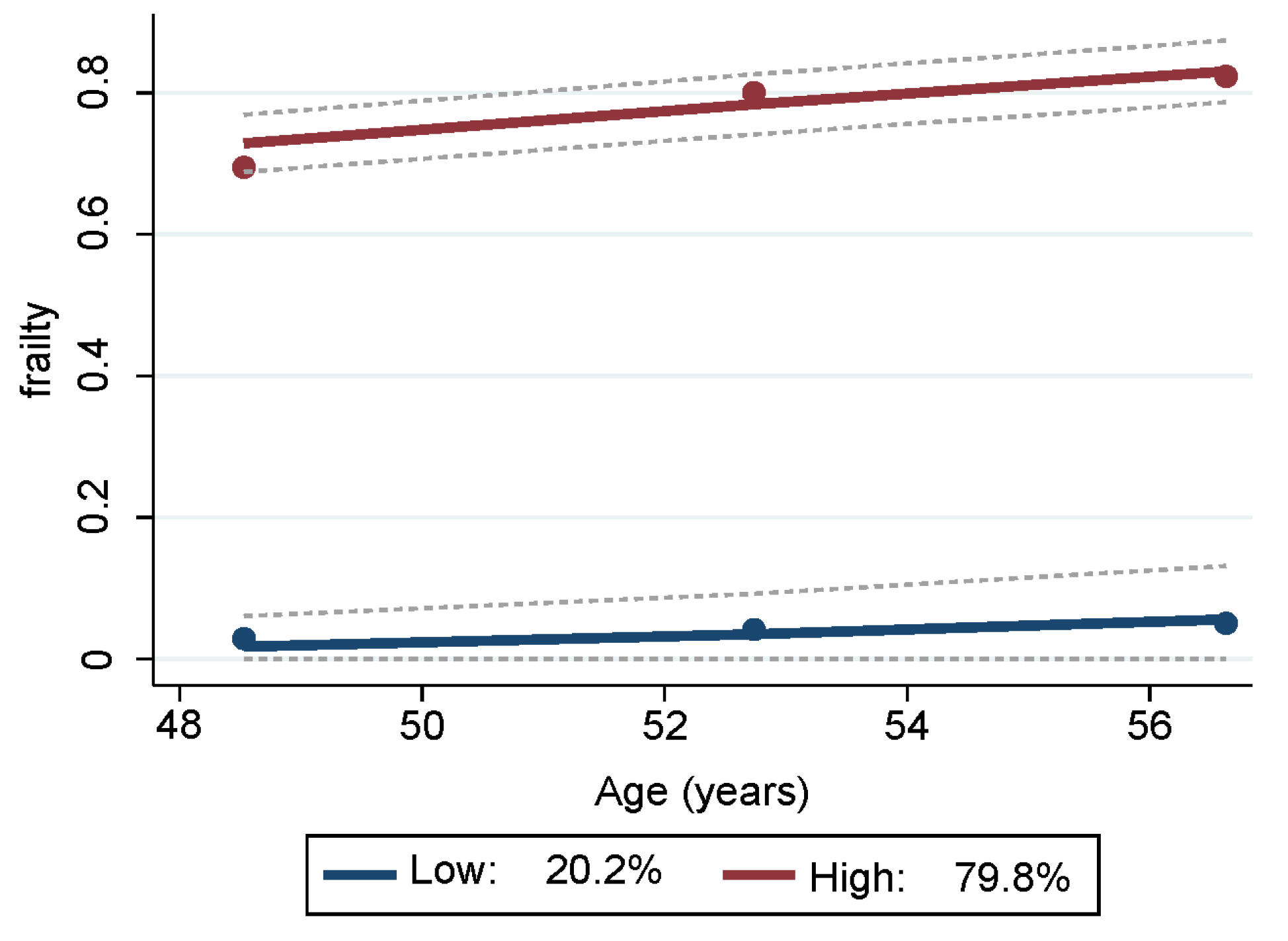
3.2. Frailty Categories and Group Trajectories
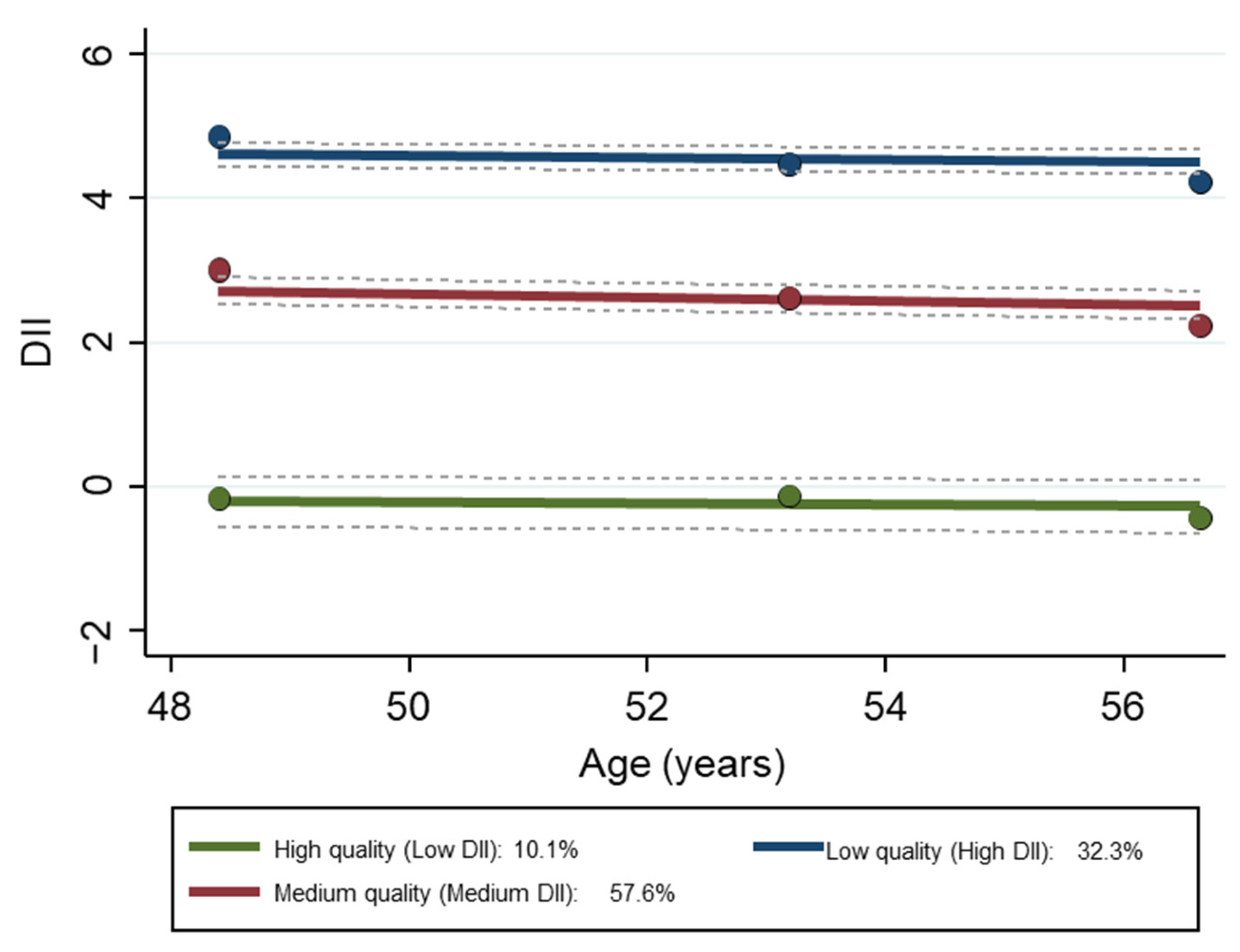
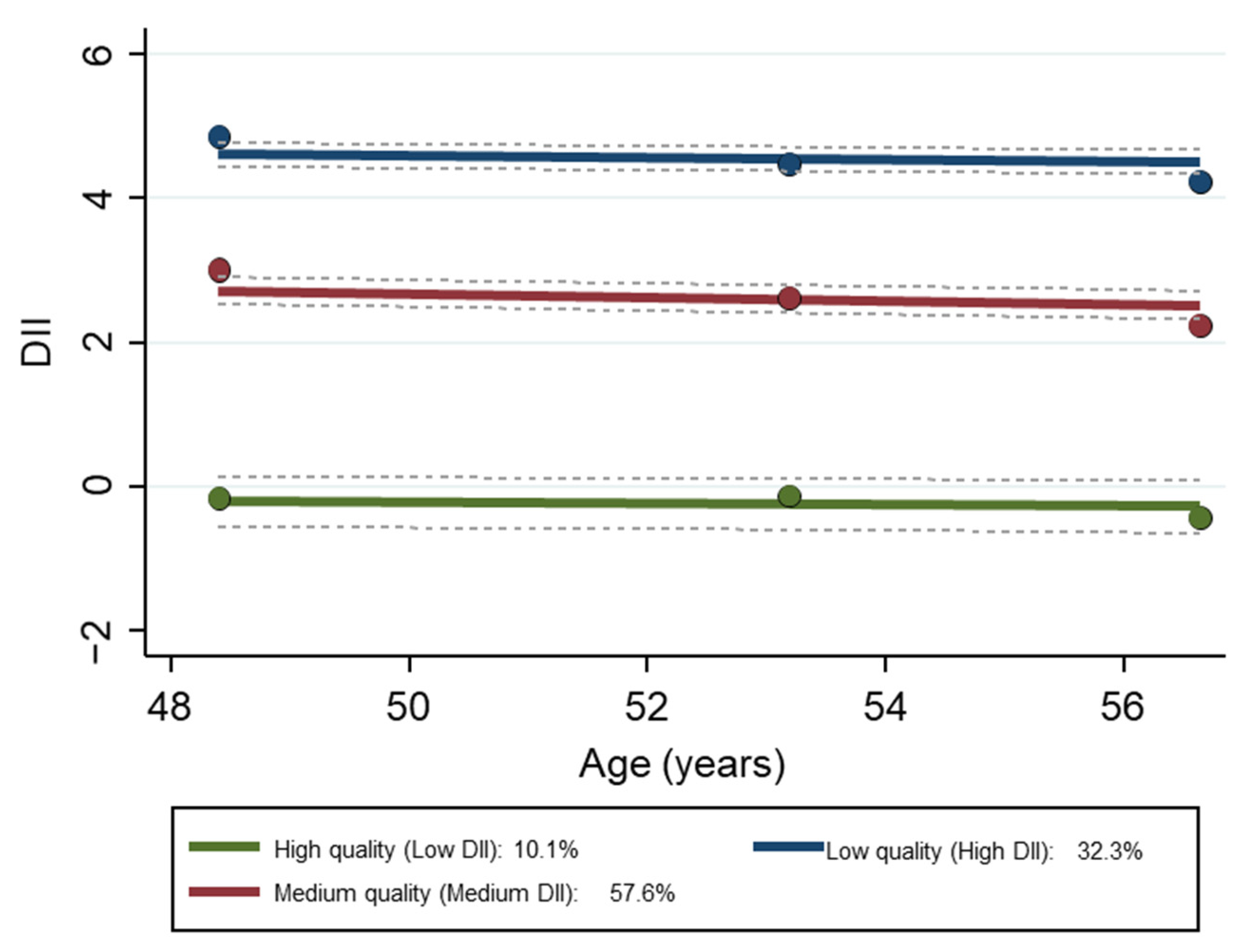
3.3. Dietary Quality Group Trajectories
3.4. Findings Based on Multiple Logistic Regression with Remaining Non-Frail as Outcome
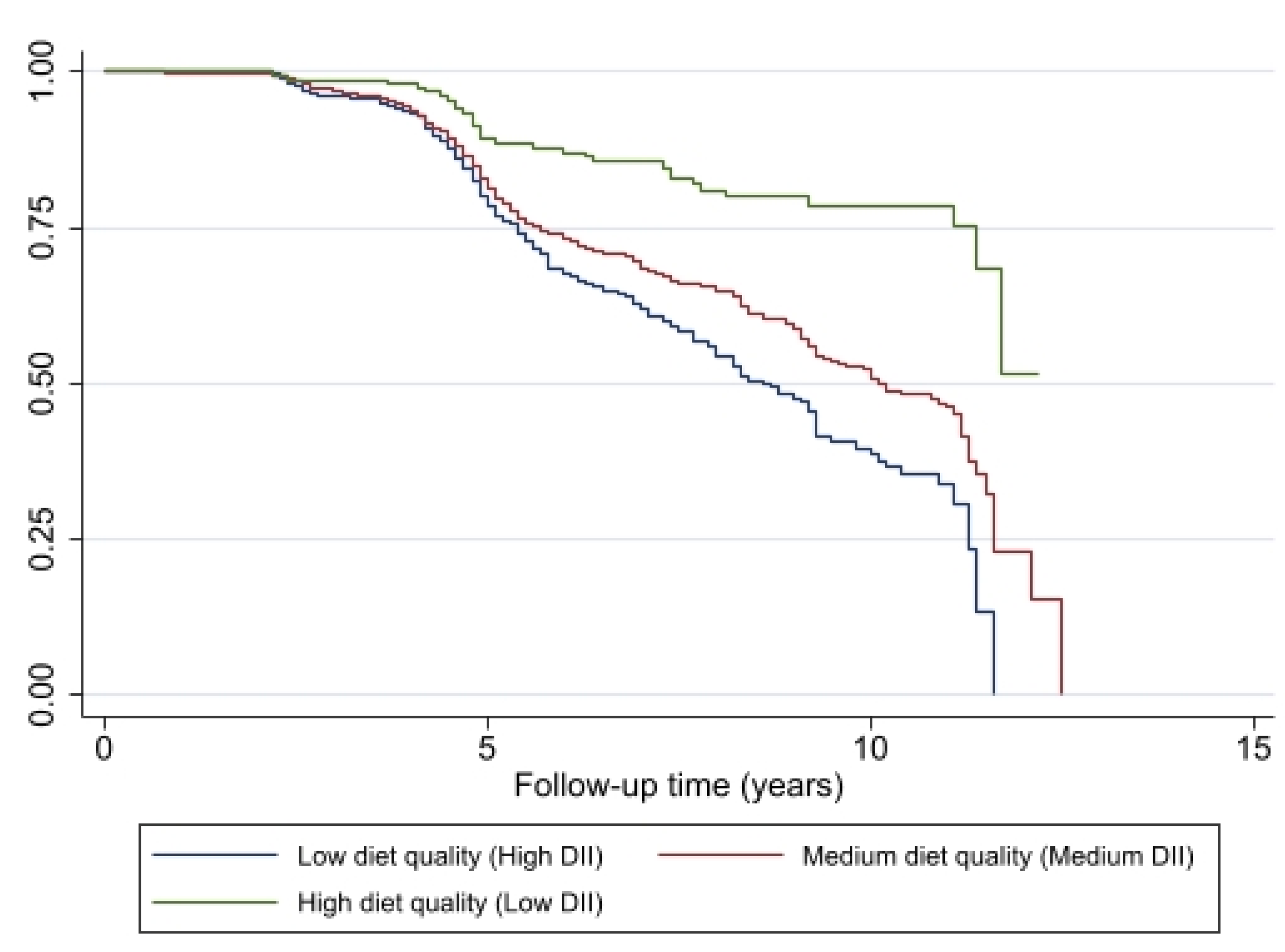
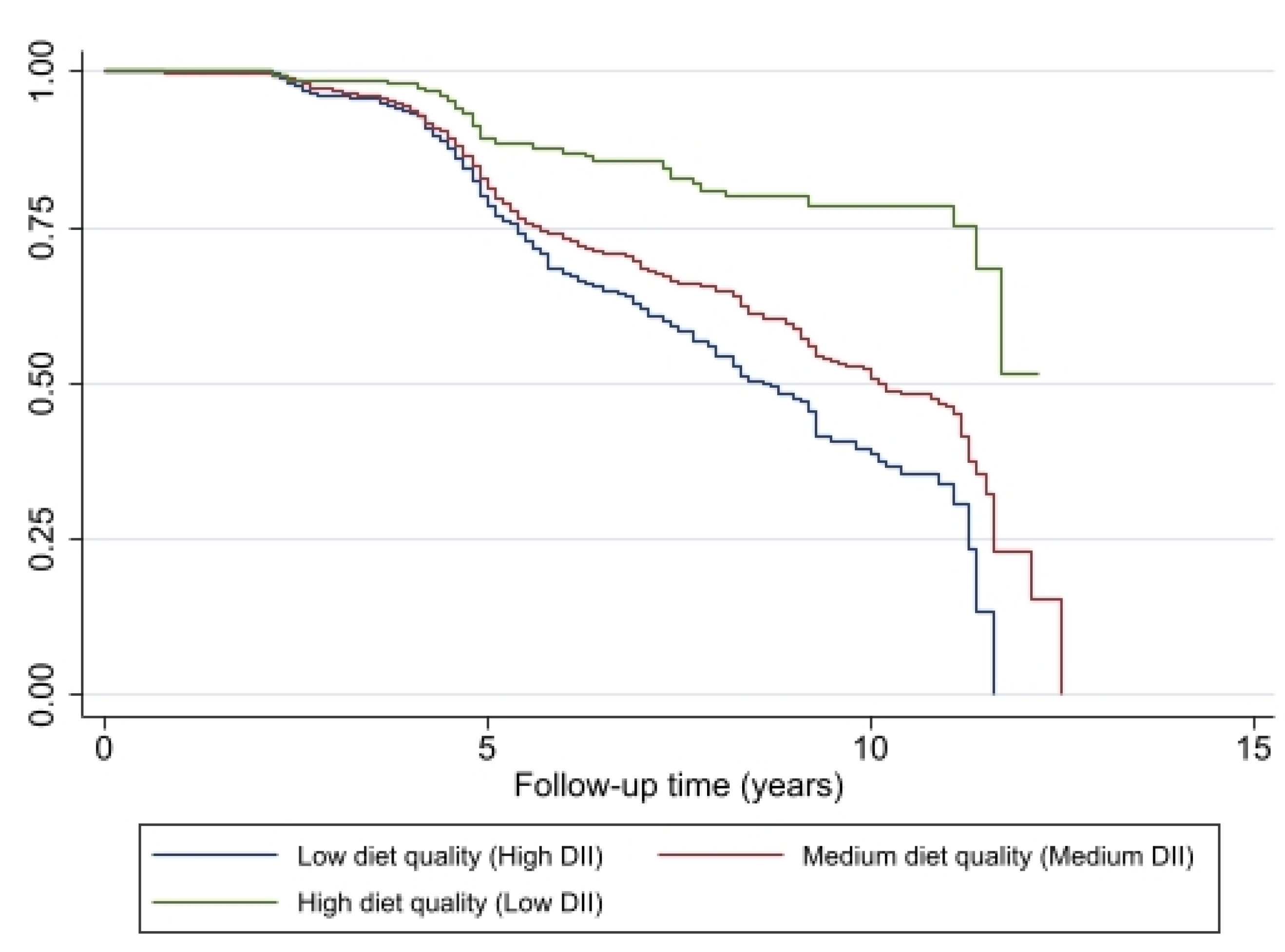
3.5. Findings Based on Proportional Hazards Regression with Time to Frailty as Outcome
3.6. Findings Based on Mixed-Effects Regression with DII Scores as Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gimeno-Mallench, L.; Sanchez-Morate, E.; Parejo-Pedrajas, S.; Mas-Bargues, C.; Inglés, M.; Sanz-Ros, J.; Román-Domínguez, A.; Olaso, G.; Stromsnes, K.; Gambini, J. The Relationship between Diet and Frailty in Aging. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 1373–1382. [Google Scholar] [CrossRef]
- Jang, I.-Y.; Jung, H.-W.; Lee, H.Y.; Park, H.; Lee, E.; Kim, D.H. Evaluation of Clinically Meaningful Changes in Measures of Frailty. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- Howlett, S.E.; Rutenberg, A.D.; Rockwood, K. The degree of frailty as a translational measure of health in aging. Nat. Aging 2021, 1, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Stow, D.; Matthews, F.E.; Hanratty, B. Frailty trajectories to identify end of life: A longitudinal population-based study. BMC Med. 2018, 16, 171. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.Q.; Theou, O.; Tucker, G.R.; Adams, R.J.; Visvanathan, R. Recurrent Measurement of Frailty Is Important for Mortality Prediction: Findings from the North West Adelaide Health Study. J. Am. Geriatr Soc. 2019, 67, 2311–2317. [Google Scholar] [CrossRef]
- Ni Lochlainn, M.; Cox, N.J.; Wilson, T.; Hayhoe, R.P.G.; Ramsay, S.E.; Granic, A.; Isanejad, M.; Roberts, H.C.; Wilson, D.; Welch, C.; et al. Nutrition and Frailty: Opportunities for Prevention and Treatment. Nutrients 2021, 13, 2349. [Google Scholar] [CrossRef] [PubMed]
- Capurso, C.; Bellanti, F.; Lo Buglio, A.; Vendemiale, G. The Mediterranean Diet Slows Down the Progression of Aging and Helps to Prevent the Onset of Frailty: A Narrative Review. Nutrients 2019, 12, 35. [Google Scholar] [CrossRef]
- Feart, C. Nutrition and frailty: Current knowledge. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 95, 109703. [Google Scholar] [CrossRef]
- Parsons, T.J.; Papachristou, E.; Atkins, J.L.; Papacosta, O.; Ash, S.; Lennon, L.T.; Whincup, P.H.; Ramsay, S.E.; Wannamethee, S.G. Physical frailty in older men: Prospective associations with diet quality and patterns. Age Ageing 2019, 48, 355–360. [Google Scholar] [CrossRef]
- Struijk, E.A.; Hagan, K.A.; Fung, T.T.; Hu, F.B.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Diet quality and risk of frailty among older women in the Nurses’ Health Study. Am. J. Clin. Nutr. 2020, 111, 877–883. [Google Scholar] [CrossRef]
- Ward, R.E.; Orkaby, A.R.; Chen, J.; Hshieh, T.T.; Driver, J.A.; Gaziano, J.M.; Djousse, L. Association between Diet Quality and Frailty Prevalence in the Physicians’ Health Study. J. Am. Geriatr. Soc. 2020, 68, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Jayanama, K.; Theou, O.; Godin, J.; Cahill, L.; Shivappa, N.; Hébert, J.R.; Wirth, M.D.; Park, Y.-M.; Fung, T.T.; Rockwood, K. Relationship between diet quality scores and the risk of frailty and mortality in adults across a wide age spectrum. BMC Med. 2021, 19, 64. [Google Scholar] [CrossRef]
- Hengeveld, L.M.; Wijnhoven, H.A.H.; Olthof, M.R.; Brouwer, I.A.; Simonsick, E.M.; Kritchevsky, S.B.; Houston, D.K.; Newman, A.B.; Visser, M. Prospective Associations of Diet Quality with Incident Frailty in Older Adults: The Health, Aging, and Body Composition Study. J. Am. Geriatr. Soc. 2019, 67, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, D.; Kurotani, K.; Yoshida, T.; Nanri, H.; Watanabe, Y.; Date, H.; Itoi, A.; Goto, C.; Ishikawa-Takata, K.; Kimura, M.; et al. Diet quality and physical or comprehensive frailty among older adults. Eur. J. Nutr. 2022, 61, 2451–2462. [Google Scholar] [CrossRef] [PubMed]
- Rashidi Pour Fard, N.; Amirabdollahian, F.; Haghighatdoost, F. Dietary patterns and frailty: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 498–513. [Google Scholar] [CrossRef]
- Fung, T.T.; Struijk, E.A.; Rodriguez-Artalejo, F.; Willett, W.C.; Lopez-Garcia, E. Fruit and vegetable intake and risk of frailty in women 60 years old or older. Am. J. Clin. Nutr. 2020, 112, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Bandeen-Roche, K.; Seplaki, C.L.; Huang, J.; Buta, B.; Kalyani, R.R.; Varadhan, R.; Xue, Q.-L.; Walston, J.D.; Kasper, J.D. Frailty in Older Adults: A Nationally Representative Profile in the United States. J. Gerontol. Ser. A 2015, 70, 1427–1434. [Google Scholar] [CrossRef]
- Griffin, F.R.; Mode, N.A.; Ejiogu, N.; Zonderman, A.B.; Evans, M.K. Frailty in a racially and socioeconomically diverse sample of middle-aged Americans in Baltimore. PLoS ONE 2018, 13, e0195637. [Google Scholar] [CrossRef]
- Fanelli Kuczmarski, M.; Cotugna, N.; Pohlig, R.T.; Beydoun, M.A.; Adams, E.L.; Evans, M.K.; Zonderman, A.B. Snacking and Diet Quality Are Associated With the Coping Strategies Used By a Socioeconomically Diverse Urban Cohort of African-American and White Adults. J. Acad. Nutr. Diet 2017, 117, 1355–1365. [Google Scholar] [CrossRef] [PubMed]
- Fanelli Kuczmarski, M.; Sebastian, R.S.; Goldman, J.D.; Murayi, T.; Steinfeldt, L.C.; Eosso, J.R.; Moshfegh, A.J.; Zonderman, A.B.; Evans, M.K. Dietary Flavonoid Intakes Are Associated with Race but Not Income in an Urban Population. Nutrients 2018, 10, 1749. [Google Scholar] [CrossRef]
- Fanelli Kuczmarski, M.; Bodt, B.A.; Stave Shupe, E.; Zonderman, A.B.; Evans, M.K. Dietary Patterns Associated with Lower 10-Year Atherosclerotic Cardiovascular Disease Risk among Urban African-American and White Adults Consuming Western Diets. Nutrients 2018, 10, 158. [Google Scholar] [CrossRef]
- Fanelli Kuczmarski, M.; Pohlig, R.T.; Stave Shupe, E.; Zonderman, A.B.; Evans, M.K. Dietary Protein Intake and Overall Diet Quality Are Associated with Handgrip Strength in African American and White Adults. J. Nutr. Health Aging 2018, 22, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Nagin, D.S. Group-based trajectory modeling: An overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- National Institutes of Health; National Institute on Aging; Intramural Research Program. Healthy Aging in Neighborhoods of Diversity across the Life Span. Available online: https://handls.nih.gov/02Protocol.htm (accessed on 20 January 2023).
- US Department of Health and Human Services. The 2004 HHS Poverty Guidelines. Available online: https://aspe.hhs.gov/2004-hhs-poverty-guidelines (accessed on 20 January 2023).
- Beydoun, M.A.; Noren Hooten, N.; Maldonado, A.I.; Beydoun, H.A.; Weiss, J.; Evans, M.K.; Zonderman, A.B. Body mass index and allostatic load are directly associated with longitudinal increase in plasma neurofilament light among urban middle-aged adults. J. Nutr. 2022, 152, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Lafortune, L.; Martin, S.; Kelly, S.; Kuhn, I.; Remes, O.; Cowan, A.; Brayne, C. Behavioural Risk Factors in Mid-Life Associated with Successful Ageing, Disability, Dementia and Frailty in Later Life: A Rapid Systematic Review. PLoS ONE 2016, 11, e0144405. [Google Scholar] [CrossRef]
- Stenholm, S.; Strandberg, T.E.; Pitkala, K.; Sainio, P.; Heliovaara, M.; Koskinen, S. Midlife obesity and risk of frailty in old age during a 22-year follow-up in men and women: The Mini-Finland Follow-up Survey. J. Gerontol A Biol. Sci. Med. Sci. 2014, 69, 73–78. [Google Scholar] [CrossRef]
- Steinfeldt, L.; Anand, J.; Murayi, T. Food reporting patterns in the USDA Automated Multiple-Pass Method. Procedia Food Sci. 2013, 2, 145–156. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. Food and Nutrient Database for Dietary Studies. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-download-databases/ (accessed on 6 June 2023).
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D Scale:A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D. A Stata Plugin for Estimating Group-Based Trajectory Models. Sociol. Methods Res. 2013, 42, 608–613. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. Advances in group-based trajectory modeling and an SAS procedure for estimating them. Sociol. Methods Res. 2007, 35, 542–571. [Google Scholar] [CrossRef]
- Shivappa, N.; Stubbs, B.; Hebert, J.R.; Cesari, M.; Schofield, P.; Soysal, P.; Maggi, S.; Veronese, N. The Relationship Between the Dietary Inflammatory Index and Incident Frailty: A Longitudinal Cohort Study. J. Am. Med. Dir. Assoc. 2018, 19, 77–82. [Google Scholar] [CrossRef]
- Millar, C.L.; Dufour, A.B.; Shivappa, N.; Habtemariam, D.; Murabito, J.M.; Benjamin, E.J.; Hebert, J.R.; Kiel, D.P.; Hannan, M.T.; Sahni, S. A proinflammatory diet is associated with increased odds of frailty after 12-year follow-up in a cohort of adults. Am. J. Clin. Nutr. 2022, 115, 334–343. [Google Scholar] [CrossRef]
- Resciniti, N.V.; Lohman, M.C.; Wirth, M.D.; Shivappa, N.; Hebert, J.R. Dietary Inflammatory Index, Pre-Frailty and Frailty among Older US Adults: Evidence from the National Health and Nutrition Examination Survey, 2007–2014. J. Nutr. Health Aging 2019, 23, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Laclaustra, M.; Rodriguez-Artalejo, F.; Guallar-Castillon, P.; Banegas, J.R.; Graciani, A.; Garcia-Esquinas, E.; Lopez-Garcia, E. The inflammatory potential of diet is related to incident frailty and slow walking in older adults. Clin. Nutr. 2020, 39, 185–191. [Google Scholar] [CrossRef]
- Satia, J.A. Diet-related disparities: Understanding the problem and accelerating solutions. J. Am. Diet Assoc. 2009, 109, 610–615. [Google Scholar] [CrossRef]
- Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Bandinelli, S.; Ferrucci, L. Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults. Nutrients 2021, 13, 1129. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Final Determination Regarding Partially Hydrogenated Oils (Removing Trans Fat). Available online: https://www.fda.gov/food/food-additives-petitions/final-determination-regarding-partially-hydrogenated-oils-removing-trans-fat (accessed on 23 October 2023).

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | Sex | Race | ||||
|---|---|---|---|---|---|---|---|
| Males | Females | p a | African American | White | p | ||
| N = 2901 | N = 1261 | N = 1640 | N = 1724 | N = 1177 | |||
| Age, v 1, X ± SE | 48.5 ± 0.2 | 48.4 ± 0.3 | 48.5 ± 0.2 | 0.573 | 48.3 ± 0.2 | 48.7 ± 0.3 | 0.312 |
| Sex, % Males | 43.5 | - | - | 43.3 | 43.8 | 0.796 | |
| Race, % African American | 59.4 | 59.2 | 59.6 | 0.796 | - | - | |
| % below poverty status b | 41.2 | 37.6 | 44.0 | 0.001 | 47.7 | 31.7 | <0.001 |
| Education, <HS, % | 6.5 | 7.3 | 5.9 | 0.248 | 4.8 | 9.0 | <0.001 |
| Education, HS, % | 60.2 | 60.9 | 59.6 | reference | 64.4 | 53.9 | reference |
| Education, >HS, % | 33.3 | 31.8 | 34.5 | 0.214 | 30.8 | 37.1 | <0.001 |
| Current smokers, % | 48.8 | 54.9 | 44.1 | <0.001 | 51.0 | 45.5 | 0.010 |
| Current drug users, % | 18.2 | 23.9 | 13.9 | <0.001 | 21.8 | 13.1 | <0.001 |
| Allostatic load, X ± SE | 1.94 ± 0.03 | 1.91 ± 0.05 | 1.96 ± 0.04 | 0.466 | 1.90 ± 0.04 | 1.99 ± 0.04 | 0.146 |
| Frailty | Overall | Sex | Race | ||||
|---|---|---|---|---|---|---|---|
| Males | Females | β ± SE | African Americans | White | β ± SE | ||
| N = 2901 | N = 1261 | N = 1640 | N = 1724 | N = 1177 | |||
| Visit 1 | |||||||
| Non-frail | 54.1 ± 1.0 | 62.1 ± 1.4 | 48.0 ± 1.3 | Referent group | 54.2 ± 1.3 | 53.9 ± 1.5 | Referent group |
| Pre-frail | 35.9 ± 0.9 | 31.1 ± 1.4 | 39.6 ± 1.3 | −0.50 ± 0.08 *** | 36.5 ± 1.2 | 35.1 ± 1.4 | 0.03 ± 0.08 |
| Frail | 10.0 ± 0.6 | 6.7 ± 0.7 | 12.4 ± 0.8 | −0.87 ± 0.14 *** | 9.2 ± 0.7 | 11.0 ± 0.9 | −0.18 ± 0.13 |
| Visit 2 | |||||||
| Non-frail | 49.1 ± 1.2 | 56.4 ± 1.8 | 43.8 ± 1.5 | Referent group | 49.6 ± 1.5 | 48.4 ± 1.8 | Referent group |
| Pre-frail | 38.2 ± 1.1 | 36.3 ± 1.7 | 39.6 ± 1.5 | −0.34 ± 0.10 ** | 38.3 ± 1.5 | 38.1 ± 1.7 | −0.02 ± 0.10 |
| Frail | 12.7 ± 0.8 | 7.3 ± 0.9 | 16.6 ± 1.1 | −1.07 ± 0.17 *** | 12.1 ± 1.0 | 13.5 ± 1.2 | −0.14 ± 0.15 |
| Visit 3 | |||||||
| Non-frail | 48.6 ± 1.1 | 55.8 ± 1.7 | 43.6 ± 1.4 | Referent group | 49.7 ± 1.4 | 47.0 ± 1.7 | Referent group |
| Pre-frail/Frail | 39.7 ± 1.1 | 33.0 ± 1.6 | 39.2 ± 1.4 | −0.42 ± 0.10 *** | 36.5 ± 1.4 | 36.8 ± 1.7 | −0.06 ± 0.10 |
| Frail | 14.7 ± 0.8 | 11.2 ± 1.1 | 17.2 ± 1.1 | −67.4 ± 0.14 *** | 13.8 ± 1.0 | 16.2 ± 1.3 | −0.21 ± 0.13 |
| N = 2901 | Loge (OR) | SE | p |
|---|---|---|---|
| Model 1 | |||
| Pre-frail or frail | Base outcome a | ||
| Remaining non-frail trajectory = main outcome | |||
| DII trajectory | Referent: Group 1 | ||
| Medium vs. High DII | 0.662 | 0.116 | <0.001 |
| Low vs. High DII | 1.569 | 0.171 | <0.001 |
| Age v 1 | 0.009 | 0.005 | 0.076 |
| Sex, Male | 0.130 | 0.095 | 0.171 |
| Race, African American | 0.282 | 0.099 | 0.004 |
| Poverty, <125% poverty | −0.886 | 0.106 | <0.001 |
| Model 2 | |||
| Pre-frail or frail | Base outcome | ||
| Remaining non-frail trajectory = main outcome | |||
| DII trajectory | Referent: Group 1 | ||
| Medium vs. High DII | 0.570 | 0.120 | <0.001 |
| Low vs. High DII | 1.291 | 0.181 | <0.001 |
| Age v 1 | 0.010 | 0.006 | 0.062 |
| Sex, Male | 0.265 | 0.100 | 0.008 |
| Race, African American | 0.317 | 0.103 | 0.002 |
| Poverty, <125% poverty | −0.741 | 0.111 | <0.001 |
| Education | Referent: <High School | ||
| High School | 0.267 | 0.252 | 0.289 |
| >High School | 0.405 | 0.256 | 0.118 |
| Current smoker v 1 | −0.561 | 0.128 | <0.001 |
| Drug User v 1 | −0.429 | 0.161 | 0.010 |
| Allostatic load | −0.209 | 0.050 | <0.001 |
| N = 2065 | Coefficient | SE | p | HR | LCL | UCL |
|---|---|---|---|---|---|---|
| DII trajectory | ||||||
| Medium vs. High DII | −0.215 | 0.098 | 0.028 | 0.806541 | 0.665591 | 0.977341 |
| Low vs. High DII | −1.042 | 0.207 | <0.001 | 0.352748 | 0.235106 | 0.529258 |
| Age v 1 | 0.014 | 0.005 | 0.004 | 1.014098 | 1.004209 | 1.024085 |
| Sex | −0.286 | 0.089 | 0.013 | 0.751263 | 0.631006 | 0.894438 |
| Race | −0.286 | 0.091 | 0.002 | 0.751263 | 0.628537 | 0.897951 |
| Poverty status | 0.139 | 0.094 | 0.141 | 1.149124 | 0.955768 | 1.381597 |
| Education | ||||||
| High School | 0.050 | 0.197 | 0.800 | 1.051271 | 0.714537 | 1.546694 |
| >High School | −0.064 | 0.209 | 0.760 | 0.938005 | 0.622731 | 1.412894 |
| Current smoker v 1 | 0.329 | 0.100 | 0.001 | 1.389578 | 1.14225 | 1.690459 |
| Drug User v 1 | 0.222 | 0.116 | 0.057 | 1.248571 | 0.994654 | 1.567309 |
| Allostatic load | 0.102 | 0.040 | 0.014 | 1.107383 | 1.023881 | 1.197696 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuczmarski, M.F.; Beydoun, M.A.; Georgescu, M.F.; Noren Hooten, N.; Mode, N.A.; Evans, M.K.; Zonderman, A.B. Pro-Inflammatory Diets Are Associated with Frailty in an Urban Middle-Aged African American and White Cohort. Nutrients 2023, 15, 4598. https://doi.org/10.3390/nu15214598
Kuczmarski MF, Beydoun MA, Georgescu MF, Noren Hooten N, Mode NA, Evans MK, Zonderman AB. Pro-Inflammatory Diets Are Associated with Frailty in an Urban Middle-Aged African American and White Cohort. Nutrients. 2023; 15(21):4598. https://doi.org/10.3390/nu15214598
Chicago/Turabian StyleKuczmarski, Marie Fanelli, May A. Beydoun, Michael F. Georgescu, Nicole Noren Hooten, Nicolle A. Mode, Michele K. Evans, and Alan B. Zonderman. 2023. "Pro-Inflammatory Diets Are Associated with Frailty in an Urban Middle-Aged African American and White Cohort" Nutrients 15, no. 21: 4598. https://doi.org/10.3390/nu15214598
APA StyleKuczmarski, M. F., Beydoun, M. A., Georgescu, M. F., Noren Hooten, N., Mode, N. A., Evans, M. K., & Zonderman, A. B. (2023). Pro-Inflammatory Diets Are Associated with Frailty in an Urban Middle-Aged African American and White Cohort. Nutrients, 15(21), 4598. https://doi.org/10.3390/nu15214598