
Modulatory Properties of Vitamin D in Type 2 Diabetic Patients: A Focus on Inflammation and Dyslipidemia


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Registration
2.2. Adapted Search Strategy and Information Sources
2.3. Study Selection Procedure
2.4. Data Extraction, Quality, and Certainty of Evidence Assessment
2.5. Subgroup, Sensitivity Analysis, and Publication Bias
2.6. Data Synthesis and Statistical Analysis
3. Results
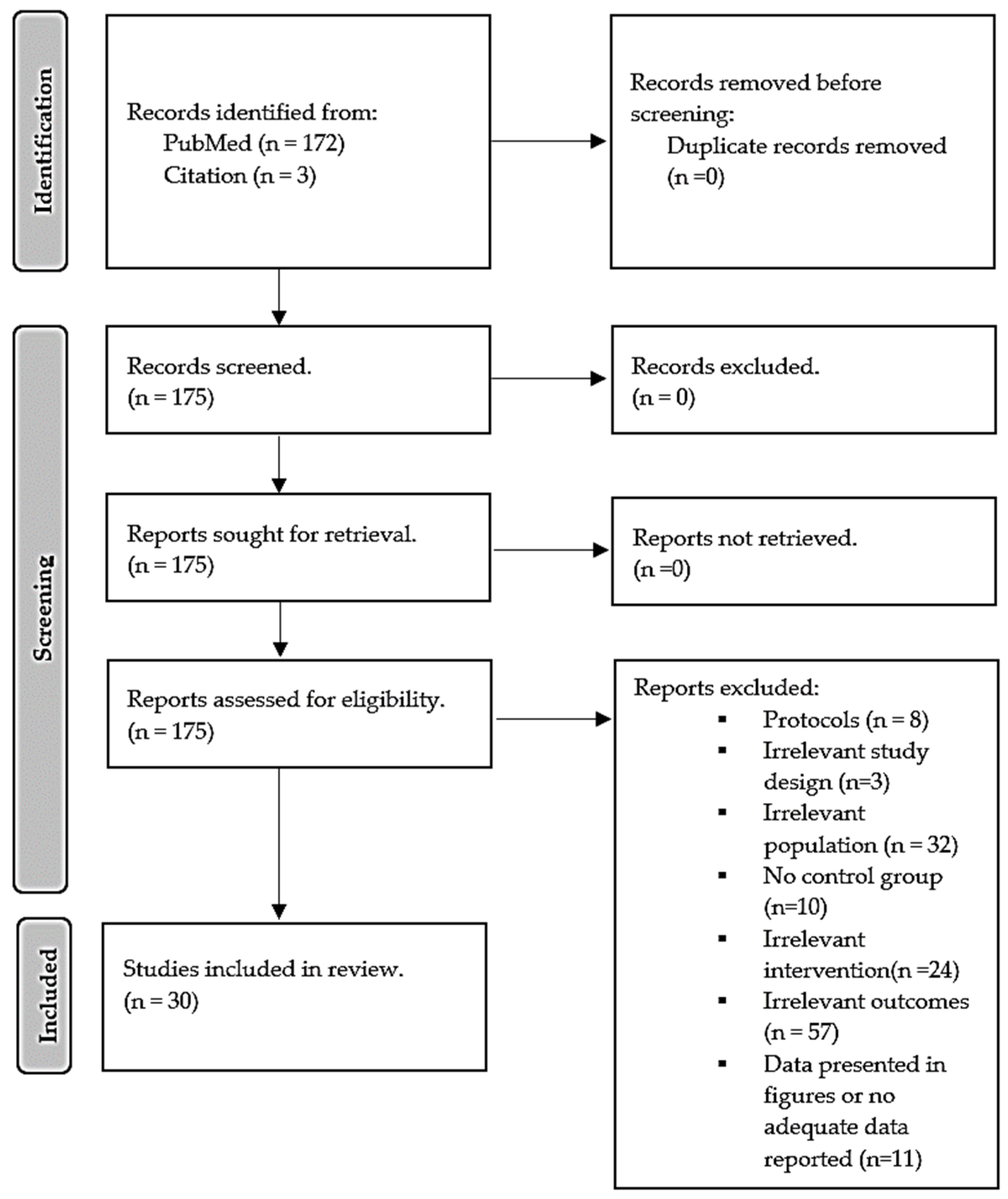
3.1. Comprehensive Search and Information Sources
3.2. General Characteristics of Included Randomized Controlled Trials

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design, Country | Population and Sample Size | Intervention Group, n. Male, n (%) | Mean Age of Intervention Group (Years) | Vitamin D, Dosage, and Duration of Intervention | Effect on Lipids and Inflammatory Markers |
|---|---|---|---|---|---|---|
| Hu et al., 2022 [68] | Randomized controlled trial (RCT); China | T2D patients, 220 | 115; 32 (27.8) | 66.05 ± 9.35 | Oral dose of 800 IU (two capsules) of vitamin D3 for 30 months. | Vitamin D supplementation significantly decreased total cholesterol (TC) and CRP. |
| Hoseini et al., 2022 [57] | Randomized, single-blinded, placebo-controlled clinical trial; Iran | T2D patients, 20 | 10; 10 (100) | 49.10 ± 1.23 | 50,000 IU of Vitamin D capsules per week for eight weeks. | Vitamin D supplementation significantly reduced tumor necrosis factor-alpha (TNF-α) and CRP. |
| Limonte et al., 2021 [58] | Randomized double-blinded placebo-controlled trial; USA | T2D patients, 1312 | 703; 376 (53.5) | 67.4 ± 7.0 | 2000 IU vitamin D3 per day for five years. | Vitamin D supplementation showed no significant changes in interleukin (IL)-6 and CRP compared to the placebo group. |
| Barale et al., 2020 [65] | Open-label randomized-controlled pilot study; Italy | T2D patients, 30 | 16; 11 (68.8) | 71.6 ± 3.5 | 500 IU oral cholecalciferol once a week for one year. | Vitamin D supplementation showed no significant difference in lipid profiles compared to the placebo group. |
| Hajj et al., 2020 [76] | Randomized controlled double-blind study; Lebanon | T2D patients, 88 | 45; 23 (51) | 66.9 ± 4.1 | 10,000 IU cholecalciferol three times per week for six months. | Vitamin D supplementation significantly reduced CRP and TNF-α levels compared to baseline data. No significant changes were observed in terms of IL-6 when compared to baseline data. |
| Imanparast et al., 2020 [56] | Randomized placebo-controlled trial; Iran | T2D patients, 92 | 23; 11 (47.8) | 53.63 ± 12.29 | 50,000 IU of vitamin D3 per week for four months | Vitamin D supplementation significantly decreased TC and TNF-α levels, with no significant changes in LDL, HDL, and triglyceride (TG) levels compared to the placebo group. |
| Meng et al., 2020 [59] | Double-blinded randomized placebo-controlled trial USA | T2D patients, 127 | 56; 43 (76.8) | 65 ± 8.0 | 4000 IU per day of vitamin D3 for 24 weeks. | Vitamin D supplementation showed no significant difference in serum LDL and HDL-c compared to the placebo. |
| Mirzavandi et al., 2020 [55] | Randomized, controlled clinical trial; Iran | T2D patients, 50 | 25; 5 (20) | 46 ± 1.0 | Two intramuscular injections of a 200,000 IU vitamin D supplement at 0 and 4 weeks. | Vitamin D supplementation led to a significant decrease in the levels of CRP and TG in comparison to baseline data. |
| Dadrass et al., 2019 [54] | Randomized, placebo-controlled, double-blinded clinical trial; Iran | T2D patients, 24 | 12; 12 (100) | 53.83 ± 6.61 | 50,000 IU per 2 weeks for three months | Vitamin D supplementation significantly decreased IL-6 and TNF-α without change in CRP compared to placebo. |
| Omidian et al., 2019 a [52] | Randomized double-blinded placebo-controlled trial; Iran | T2D patients, 66 | 32; 19 (59.4) | 49.7 ± 6.5 | 4000 IU vitamin D daily for 12 weeks. | Vitamin D supplementation significantly increased TG levels compared to baseline data. |
| Omidian et al., 2019 b [53] | Parallel randomized double-blind placebo-controlled clin- ical trial; Iran | T2D patients, 47 | 24; 10 (41.6) | 51.3 ± 4.7 | 4000 IU vitamin D daily for 12 weeks. | Vitamin D supplementation significantly decreased IL-6 and MCP-1 levels compared to baseline data. |
| Wenclewska et al., 2019 [77] | Randomized controlled trial; Poland | T2D patients, 92 | 48; 14 (29) | 63.43 ±1.57 | 2000 IU of vitamin D3 per day for three months. | Vitamin D supplementation increased HDL compared to baseline data. |
| Angellotti et al., 2019 [60] | Randomized, double-blind, placebo-controlled clinical trial; USA | T2D patients, 114 | 66; 49 (71) | 60.1 ± 8.4 | 4000 units of vitamin D3 for 48 weeks. | Vitamin D supplementation revealed no significant in CRP, with a significant reduction in TG levels. |
| Fazelian et al., 2018 [51] | Randomized double-blind placebo-controlled clinical trial; Iran | T2D patients, 51 | 26; 0 (0) | 48.5 ± 7.58 | one oral pearl of 50,000 IU vitamin D3 for 16 weeks. | Vitamin D supplementation significantly reduced CRP and increased IL-10 levels. |
| Upreti et al., 2018 [70] | Parallel randomized, placebo-controlled trial; India | T2D patients, 60 | 30; 15 (50) | 48.3 ± 9.8 | 60,000 IU weekly for six weeks, followed by once every four weeks for 24 weeks. | Vitamin D supplementation led to a significant difference in total cholesterol compared to the placebo group. |
| Barchetta et al., 2016 [64] | Randomized, double-blind, placebo-controlled trial; Italy | T2D patients, 65 | 26; 18 (50) | 57.4 ± 10.7 | 2000 IU cholecalciferol per day for 24 weeks. | Vitamin D supplementation showed a significant difference in LDL, HDL, and TG without any significant difference in CRP levels. |
| Dalan et al., 2016 [74] | Parallel randomized, double-blind, placebo-con- trolled trial; Singapore | T2D patients, 61 | 31; 14 (45) | 52.2 ± 8.2 | 4000 IU vitamin D (oral cholecalciferol) and 2000 IU for 16 weeks. | Vitamin D supplementation showed no significant effect on lipid profiles and CRP in comparison to baseline data. |
| Sadiya et al., 2015 [47] | Randomized, double-blind clinical trial; United Arab Emirates | T2D patients with obesity, 82. | 43; 9 (20.9) | 49 ± 8.0 | Vitamin D (6000 IU) per day, followed by 3000 IU vitamin D3 daily for six months. | Vitamin D supplementation showed no significant differences in lipids and CRP compared to placebo groups. |
| Muñoz-Aguirre et al., 2014 [73] | Randomized, double-blind, placebo- controlled trial; Mexico | T2D patients, 104. | 52; 0 (0) | 56.1 ± 5.1 | 4000 IU of vitamin D daily for six months. | Vitamin D supplementation revealed no significant changes in LDL, and TC levels significantly decreased TG compared to the placebo. |
| Gagnon et al., 2014 [67] | Randomized, double-blinded, placebo-controlled trial; Australia | T2D patients, 80. | 35; 10 (28.6) | 53.8 ± 11.9 | 2000 IU of vitamin D3 for six months. | Vitamin D supplementation showed no difference in inflammatory markers compared to placebo. |
| Jehle et al., 2014 [75] | Prospective, randomized, double-blind, placebo-con- trolled pilot; Switzerland | T2D patients, 55. | 29; 10 (34.5) | 66.9 ± 3.1 | A single 300,000 IU intramuscular injection of vitamin D3 for six months. | Vitamin D supplementation revealed no significant difference in levels of CRP compared to placebo groups. |
| Kampmann et al., 2014 [69] | Randomized, double-blind, placebo-controlled trial; Denmark | T2D patients, 16. | 8; 6 (75) | 61.6 ± 4.4 | 11,200 IU cholecalciferol per day for ten weeks | Vitamin D supplementation resulted in no significant difference in HDL, LDL, TC, TG, CRP, TNF-α, IL-6, and IL-8 compared to placebo groups. |
| Maggi et al., 2014 [66] | Randomized, double-blind, placebo-controlled clinical trial; Italy | T2D patients, 30 | 14; 9 (64) | 69 ± 4.5 | Single oral dose of 300,000 IU of Vitamin D3 for 24 weeks. | Vitamin D supplementation led to no significant difference in TNF-α levels compared to the group on placebo. |
| Ryu et al., 2014 [72] | Prospective, randomized, double-blind- ed, placebo-controlled trial; Korea | T2D patients, 158 | 79; NR | 54.8 ± 7.6 | 1000 IU of vitamin D3 with a combined 100 mg of calcium twice daily for 24 weeks. | Vitamin D supplementation showed no significant difference in lipid profiles and inflammatory markers compared to placebo groups. |
| Tabesh et al., 2014 [50] | Parallel- randomized placebo- controlled clinical trial; Iran | T2D patients, 118 | 29; 15 (51.7) | 50.2 ± 6.6 | 50,000 IU vitamin D3 per week for eight weeks. | Vitamin D supplementation showed no significant effect on serum levels of HDL, LDL, and TG compared to a placebo group. |
| Akbarzadeh et al., 2013 [49] | Randomized double-blind placebo-controlled trial; Iran | T2D patients, 70 | 35; 35 (100) | 53.8 ± 8.9 | Two tablets of Calcitriol (0.25 μg 1,25-dihydroxy cholecalciferol) (≈10 IU) per day for 12 weeks. | Vitamin D supplementation showed no significant effect on the marker of inflammation, including CRP, IL-6, and IL-18 levels, compared to baseline data. |
| Breslavsky et al., 2013 [71] | Randomized, double-blind, placebo-controlled trial; Israel | T2D patients, 47 | 24; 11 (45.8) | 66.8 ± 9.2 | 1000 IU Vitamin D daily for 12 months. | Vitamin D supplementation had no significant effect on lipid profile and CRP compared to the placebo group. |
| Neyestani et al., 2012 [48] | Randomized, double-blinded controlled trial; Iran | T2D Patients, 60 | 30; NR. | 51.5 ± 5.4 | 500 IU vitamin D3 and 150 calcium for 12 weeks. | Vitamin D supplementation significantly decreased CRP, IL-1β, and IL-6 compared to placebo. |
| Punthakee et al., 2012 [62] | Randomized, double-blind placebo-controlled trial; Canada | T2D patients, 1332 | 607; 362 (59.6) | 66.7 ± 6.7 | 1000 IU daily for five and a half years. | Vitamin D supplementation showed no significant effect on HDL, LDL, TG, and TC in comparison to placebo. |
| Witham et al., 2010 [61] | Parallel, randomized, placebo- controlled trial; Canada | T2D patients, 95 | 37; 13 (35) | 64.27 ± 10.27 | A single dose of 100,000 IU vitamin D3 or 200,000 IU vitamin D3 for 16 weeks. | There was no significant difference in TC levels between the vitamin D and placebo groups. |
3.3. The Methodological Quality of Included RCTs
3.4. Effect of Vitamin D on Markers of Inflammation
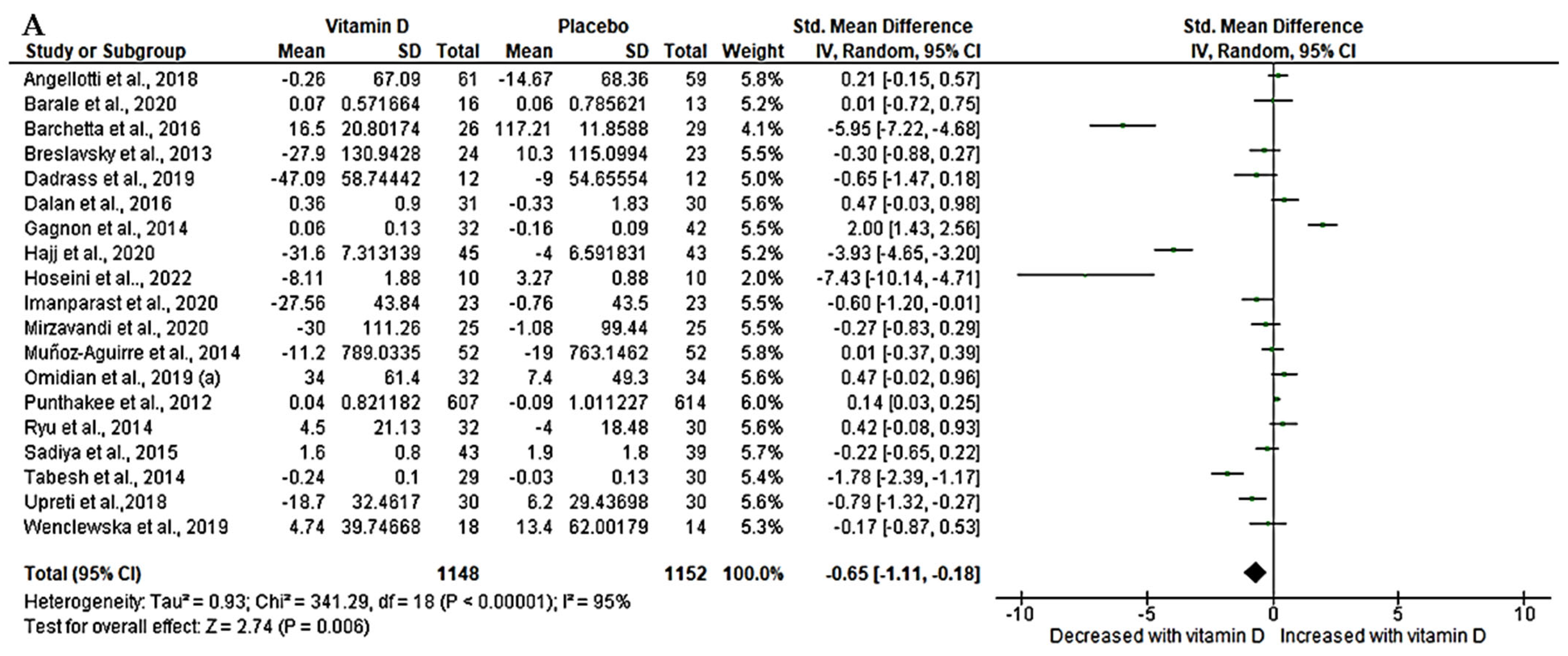
3.4.1. Effect of Vitamin D on High Sensitivity-C-Reactive Protein (hs-CRP) in T2D Patients
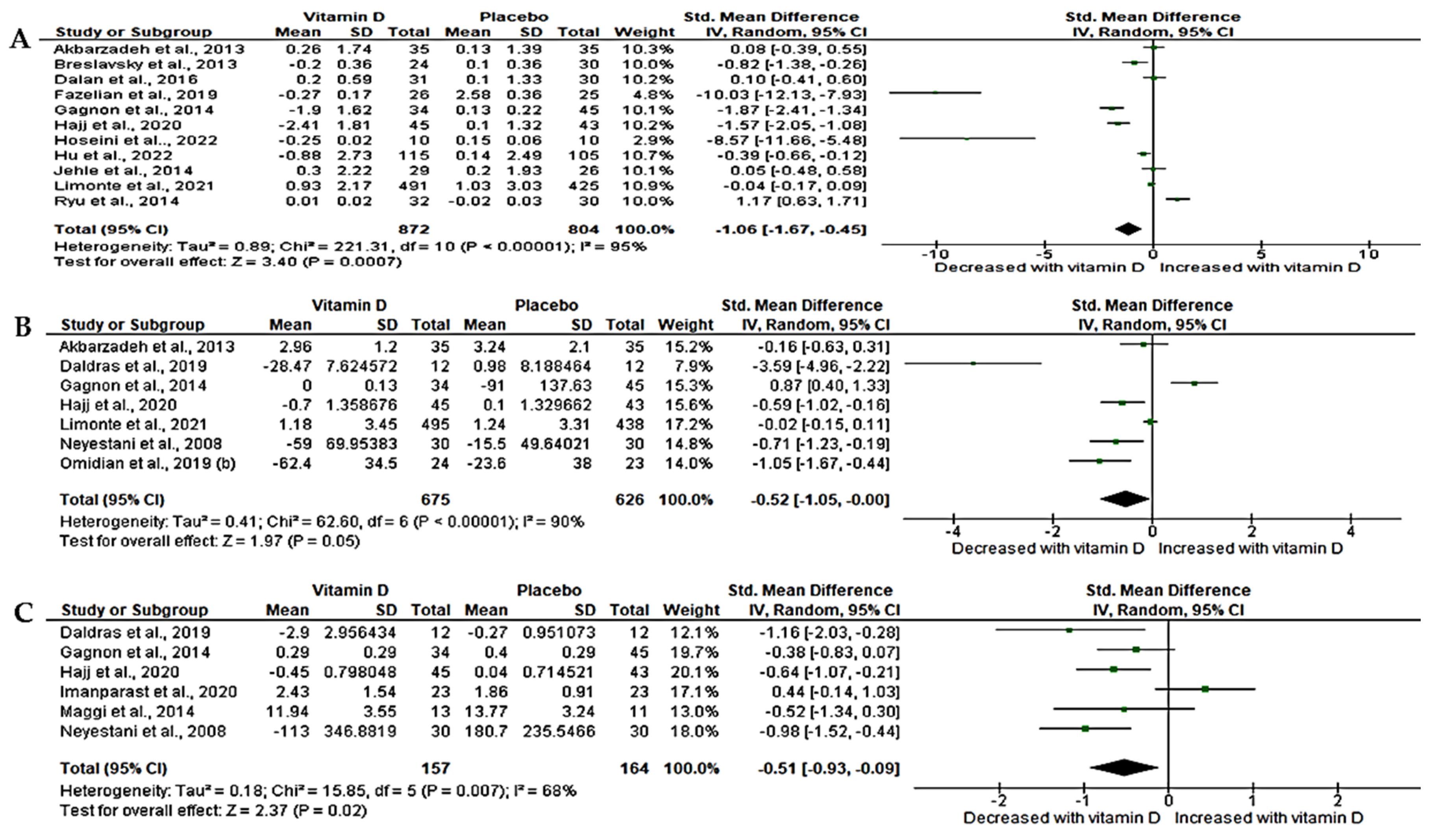
3.4.2. Effect of Vitamin D on Interleukin-6 (IL-6)
3.4.3. Effect of Vitamin D on Tumor Necrosis Factor-Alpha (TNF-α)
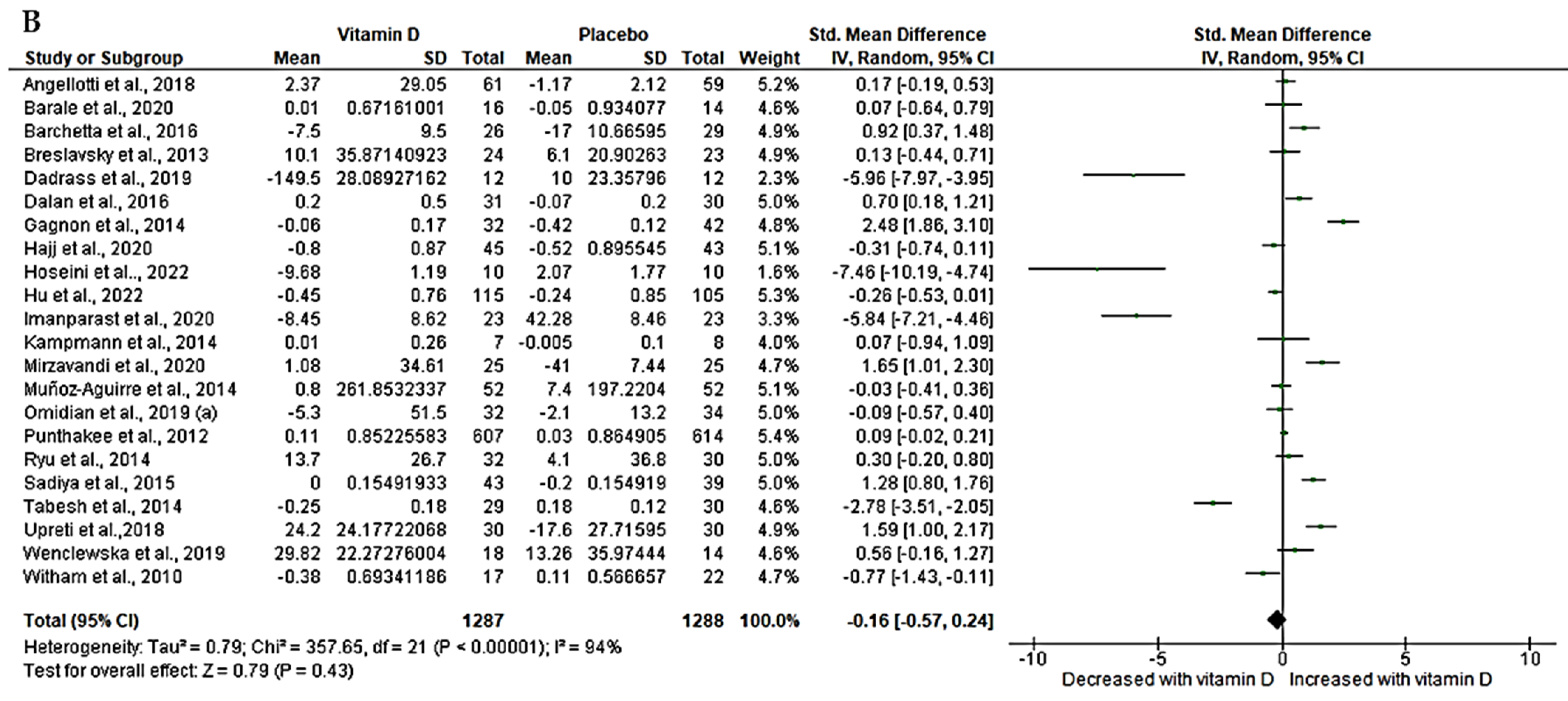
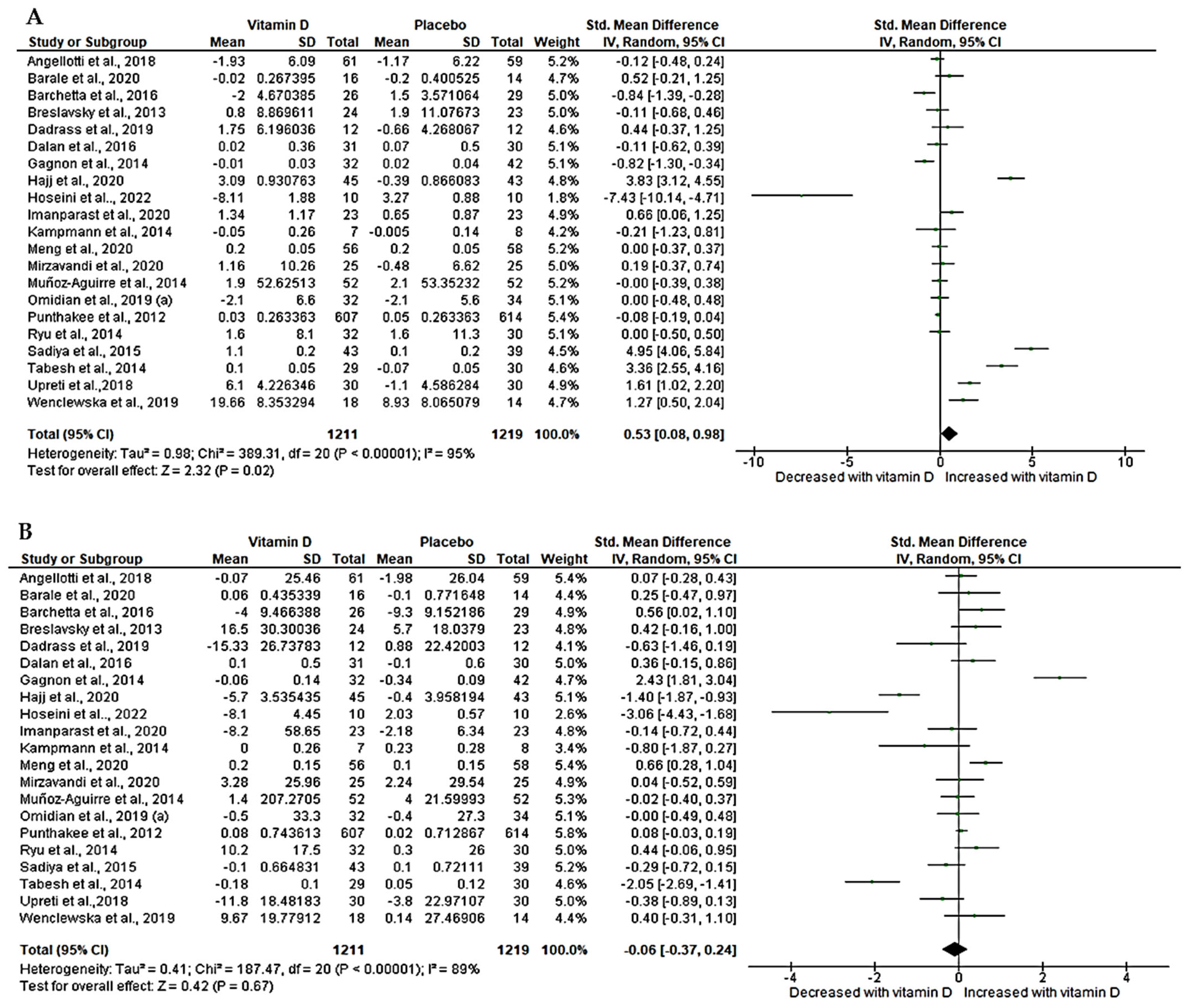
3.5. Effect of Vitamin D on Lipid Profiles (Triglycerides and Total Cholesterol)
3.6. Effect of Vitamin D on Lipid Profiles (HDL and LDL)
3.7. Subgroup Analysis
3.8. Sensitivity Analysis
3.9. Publication Bias
3.10. Certainty of Evidence
4. Discussion
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence intervals. |
| CRP | C-reactive protein. |
| CVD | Cardiovascular disease. |
| GRADE | Grading of Recommendation Assessment, Development, and Evaluation. |
| HDL | High-density lipoprotein. |
| IDF | International Diabetes Federation. |
| IFγ | Interferon-gamma. |
| IL-6 | Interleukin-6. |
| IQR | Interquartile Range. |
| IU | International Unit. |
| LDL | Low-density lipoprotein. |
| MCP-1 | Monocyte-Chemoattractant Protein-1. |
| MD | Mean difference. |
| NF-kβ | Nuclear Factor kappa beta. |
| NO | Nitric oxide. |
| NR | Not Reported. |
| oxLDL | Oxidised Low-density lipoprotein. |
| PRISMA | Preferred Reporting Items for Systematic Review and Meta-analysis. |
| RM | Randomized Model. |
| SD | Standard deviation. |
| SEM | Standard Error of Mean. |
| SMD | Standard mean difference. |
| T2D | Type 2 diabetes. |
| TNF-α | Tumor necrosis factor-alpha. |
References
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation (IDF). IDF Diabetes Atlas 10th Edition. Available online: www.diabetesatlas.org (accessed on 21 July 2023).
- Mutyambizi, C.; Pavlova, M.; Chola, L.; Hongoro, C.; Groot, W. Cost of Diabetes Mellitus in Africa: A Systematic Review of Existing Literature. Glob. Health 2018, 14, 3. [Google Scholar] [CrossRef]
- World Health Organization. Global Expenditure on Health: Public Spending on the Rise? Available online: https://www.who.int/publications-detail-redirect/9789240041219 (accessed on 20 July 2023).
- Matheus, A.S.D.M.; Tannus, L.R.M.; Cobas, R.A.; Palma, C.C.S.; Negrato, C.A.; Gomes, M.D.B. Impact of Diabetes on Cardiovascular Disease: An Update. Int. J. Hypertens. 2013, 2013, 653789. [Google Scholar] [CrossRef] [PubMed]
- Yen, F.S.; Wei, J.C.C.; Chiu, L.T.; Hsu, C.C.; Hwu, C.M. Diabetes, Hypertension, and Cardiovascular Disease Development. J. Transl. Med. 2022, 20, 9. [Google Scholar] [CrossRef]
- Rohm, T.V.; Meier, D.T.; Olefsky, J.M.; Donath, M.Y. Inflammation in Obesity, Diabetes, and Related Disorders. Immunity 2022, 55, 31–55. [Google Scholar] [CrossRef]
- Sowers, J.R.; Epstein, M.; Frohlich, E.D. Diabetes, Hypertension, and Cardiovascular Disease: An Update Hypertension in the Diabetic Patient. Hypertension 2001, 37, 1053–1059. [Google Scholar] [CrossRef]
- Meza, C.A.; La Favor, J.D.; Kim, D.H.; Hickner, R.C. Endothelial Dysfunction: Is There a Hyperglycemia-Induced Imbalance of NOX and NOS? Int. J. Mol. Sci. 2019, 20, 3775. [Google Scholar] [CrossRef]
- Funk, S.D.; Yurdagul, A.; Orr, A.W. Hyperglycemia and Endothelial Dysfunction in Atherosclerosis: Lessons from Type 1 Diabetes. Int. J. Vasc. Med. 2012, 2012, 569654. [Google Scholar] [CrossRef]
- Castellon, X.; Bogdanova, V. Chronic Inflammatory Diseases and Endothelial Dysfunction. Aging Dis. 2016, 7, 81–89. [Google Scholar] [CrossRef]
- Ghosal, S. The Side Effects of Metformin—A Review. Diabetes Metab. Disord. 2019, 6, 1–7. [Google Scholar] [CrossRef]
- Shurrab, N.T.; Arafa, E.-S.A. Metformin: A Review of Its Therapeutic Efficacy and Adverse Effects. Obes. Med. 2020, 17, 100186. [Google Scholar] [CrossRef]
- Infante, M.; Leoni, M.; Caprio, M.; Fabbri, A. Long-Term Metformin Therapy and Vitamin B12 Deficiency: An Association to Bear in Mind. World J. Diabetes 2021, 12, 916–931. [Google Scholar] [CrossRef] [PubMed]
- Kanwugu, O.N.; Glukhareva, T.V.; Danilova, I.G.; Kovaleva, E.G. Natural Antioxidants in Diabetes Treatment and Management: Prospects of Astaxanthin. Crit. Rev. Food Sci. Nutr. 2021, 62, 5005–5028. [Google Scholar] [CrossRef] [PubMed]
- Mokgalaboni, K.; Ntamo, Y.; Ziqubu, K.; Nyambuya, T.M.; Nkambule, B.B.; Mazibuko-Mbeje, S.E.; Gabuza, K.B.; Chellan, N.; Tiano, L.; Dludla, P.V. Curcumin Supplementation Improves Biomarkers of Oxidative Stress and Inflammation in Conditions of Obesity, Type 2 Diabetes and NAFLD: Updating the Status of Clinical Evidence. Food Funct. 2021, 12, 12235–12249. [Google Scholar] [CrossRef]
- Mokgalaboni, K.; Lebelo, L.S.; Modjadji, P.; Ghaffary, S. Okra Ameliorates Hyperglycaemia in Pre-Diabetic and Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis of the Clinical Evidence. Front. Pharmacol. 2023, 14, 1132650. [Google Scholar] [CrossRef]
- Matough, F.A.; Budin, S.B.; Hamid, Z.A.; Alwahaibi, N.; Mohamed, J. The Role of Oxidative Stress and Antioxidants in Diabetic Complications. SQU Med. J. 2012, 12, 5–18. [Google Scholar]
- Mokgalaboni, K.; Nkambule, B.B.; Ntamo, Y.; Ziqubu, K.; Nyambuya, T.M.; Mazibuko-Mbeje, S.E.; Gabuza, K.B.; Chellan, N.; Cirilli, I.; Tiano, L.; et al. Vitamin K: A Vital Micronutrient with the Cardioprotective Potential against Diabetes-Associated Complications. Life Sci. 2021, 286, 120068. [Google Scholar] [CrossRef]
- Ross, A.C.; Institute of Medicine (U.S.). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In DRI, Dietary Reference Intakes: Calcium, Vitamin D; National Academies Press: Washington, DC, USA, 2011; ISBN 978-0-30916-394-1. [Google Scholar]
- National Institute of Health; Office of Dietary Supplements. Vitamin D Fact Sheet for Consumer. Available online: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/ (accessed on 21 July 2023).
- Riis, J.L.; Johansen, C.; Gesser, B.; Møller, K.; Larsen, C.G.; Kragballe, K.; Iversen, L. 1α,25(OH)2D3 Regulates NF-ΚB DNA Binding Activity in Cultured Normal Human Keratinocytes through an Increase in IκBα Expression. Arch. Dermatol. Res. 2004, 296, 195–202. [Google Scholar] [CrossRef]
- Mousa, A.; Naderpoor, N.; Johnson, J.; Sourris, K.; de Courten, M.P.J.; Wilson, K.; Scragg, R.; Plebanski, M.; de Courten, B. Effect of Vitamin D Supplementation on Inflammation and Nuclear Factor Kappa-B Activity in Overweight/Obese Adults: A Randomized Placebo-Controlled Trial. Sci. Rep. 2017, 7, 15154. [Google Scholar] [CrossRef]
- Harinarayan, C.V.; Arvind, S.; Joshi, S.; Thennarasu, K.; Vedavyas, V.; Baindur, A. Improvement in Pancreatic β-Cell Function with Vitamin d and Calcium Supplementation in Vitamin d-Deficient Nondiabetic Subjects. Endocr. Pract. 2014, 20, 129–138. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, L.; Xu, H.J.; Li, Y.; Hu, C.M.; Yang, J.Y.; Sun, M.Y. The Anti-Inflammatory Effects of Vitamin D in Tumorigenesis. Int. J. Mol. Sci. 2018, 19, 2736. [Google Scholar] [CrossRef] [PubMed]
- Ponvilawan, B.; Charoenngam, N. Vitamin D and Uric Acid: Is Parathyroid Hormone the Missing Link? J. Clin. Transl. Endocrinol. 2021, 25, 100263. [Google Scholar] [CrossRef] [PubMed]
- Szymczak-Pajor, I.; Drzewoski, J.; Śliwińska, A. The Molecular Mechanisms by Which Vitamin d Prevents Insulin Resistance and Associated Disorders. Int. J. Mol. Sci. 2020, 21, 6644. [Google Scholar] [CrossRef] [PubMed]
- George, P.S.; Pearson, E.R.; Witham, M.D. Effect of Vitamin D Supplementation on Glycaemic Control and Insulin Resistance: A Systematic Review and Meta-Analysis. Diabet. Med. 2012, 29, e142–e150. [Google Scholar] [CrossRef]
- Nikooyeh, B.; Neyestani, T.R. Oxidative Stress, Type 2 Diabetes and Vitamin D: Past, Present and Future. Diabetes Metab. Res. Rev. 2016, 32, 260–267. [Google Scholar] [CrossRef]
- Mousa, A.; Naderpoor, N.; Teede, H.; Scragg, R.; de Courten, B. Vitamin D Supplementation for Improvement of Chronic Low-Grade Inflammation in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutr. Rev. 2018, 76, 380–394. [Google Scholar] [CrossRef]
- Yu, Y.; Tian, L.; Xiao, Y.; Huang, G.; Zhang, M. Effect of Vitamin D Supplementation on Some Inflammatory Biomarkers in Type 2 Diabetes Mellitus Subjects: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Nutr. Metab. 2018, 73, 62–73. [Google Scholar] [CrossRef]
- Jafari, T.; Fallah, A.A.; Barani, A. Effects of Vitamin D on Serum Lipid Profile in Patients with Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. 2016, 35, 1259–1268. [Google Scholar] [CrossRef]
- Frandsen, T.F.; Bruun Nielsen, M.F.; Lindhardt, C.L.; Eriksen, M.B. Using the Full PICO Model as a Search Tool for Systematic Reviews Resulted in Lower Recall for Some PICO Elements. J. Clin. Epidemiol. 2020, 127, 69–75. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- MacGirlley, R.; Mokgalaboni, K. The Effect of Vitamin D on Inflammation and Dyslipidemia in Type 2 Diabetes Mellitus: Protocol for a Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR Res. Protoc. 2023, 12, e42193. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Andrew Moore, R.; Carroll, D.; Jenkinson, C.; John Reynolds, D.M.; Gavaghan, D.J.; McQuay DM, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Luis Aguayo-Albasini, J.; Flores-Pastor, B.; Soria-Aledo, V. GRADE System: Classification of Quality of Evidence and Strength of Recommendation. Cir. Esp. 2014, 92, 82–88. [Google Scholar] [CrossRef]
- Sedgwick, P. Meta-Analyses: Heterogeneity and Subgroup Analysis. BMJ 2013, 346, f4040. [Google Scholar] [CrossRef]
- Doleman, B.; Freeman, S.C.; Lund, J.N.; Williams, J.P.; Sutton, A.J. Funnel Plots May Show Asymmetry in the Absence of Publication Bias with Continuous Outcomes Dependent on Baseline Risk: Presentation of a New Publication Bias Test. Res. Synth. Methods 2020, 11, 522–534. [Google Scholar] [CrossRef]
- Cochrane Handbook 6.1.3.2 Imputing Standard Deviations for Changes from Baseline. Available online: https://handbook-5-1.cochrane.org/chapter_16/16_1_3_2_imputing_standard_deviations_for_changes_from_baseline.htm (accessed on 28 July 2023).
- Yagiz, G.; Akaras, E.; Kubis, H.P.; Owen, J.A. The Effects of Resistance Training on Architecture and Volume of the Upper Extremity Muscles: A Systematic Review of Randomised Controlled Trials and Meta-Analyses. Appl. Sci. 2022, 12, 1593. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T. Statistical Algorithms in Review Manager 5. Available online: https://training.cochrane.org/handbook/current/chapter-10-statistical-algorithms-revman-5-1 (accessed on 28 July 2023).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 1–10. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Hassani, H.; Ghodsi, M.; Howell, G. A Note on Standard Deviation and Standard Error. Teach. Math. Appl. 2010, 29, 108–112. [Google Scholar] [CrossRef]
- Schroll, J.B.; Moustgaard, R.; Gøtzsche, P.C. Dealing with Substantial Heterogeneity in Cochrane Reviews. Cross-Sectional Study. BMC Med. Res. Methodol. 2011, 11, 22. [Google Scholar] [CrossRef]
- Sadiya, A.; Ahmed, S.M.; Carlsson, M.; Tesfa, Y.; George, M.; Ali, S.H.; Siddieg, H.H.; Abusnana, S. Vitamin D Supplementation in Obese Type 2 Diabetes Subjects in Ajman, UAE: A Randomized Controlled Double-Blinded Clinical Trial. Eur. J. Clin. Nutr. 2015, 69, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Neyestani, T.R.; Nikooyeh, B.; Alavi-Majd, H.; Shariatzadeh, N.; Kalayi, A.; Tayebinejad, N.; Heravifard, S.; Salekzamani, S.; Zahedirad, M. Improvement of Vitamin D Status via Daily Intake of Fortified Yogurt Drink Either with or without Extra Calcium Ameliorates Systemic Inflammatory Biomarkers, Including Adipokines, in the Subjects with Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2012, 97, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Akbarzadeh, M.; Eftekhari, M.H.; Dabbaghmanesh, M.H.; Hasanzadeh, J.; Bakhshayeshkaram, M. Serum IL-18 and HsCRP Correlate with Insulin Resistance without Effect of Calcitriol Treatment on Type 2 Diabetes. Iran. J. Immunol. 2013, 10, 167–176. [Google Scholar]
- Tabesh, M.; Azadbakht, L.; Faghihimani, E.; Tabesh, M.; Esmaillzadeh, A. Effects of Calcium–Vitamin D Co-Supplementation on Metabolic Profiles in Vitamin D Insufficient People with Type 2 Diabetes: A Randomised Controlled Clinical Trial. Diabetologia 2014, 57, 2038–2047. [Google Scholar] [CrossRef]
- Fazelian, S.; Paknahad, Z.; Khajehali, L.; Kheiri, S.; Amani, R. The Effects of Supplementation with Vitamin D on Inflammatory Biomarkers, Omentin, and Vaspin in Women with Type 2 Diabetes: A Randomized Double-Blind Placebo-Controlled Clinical Trial. J. Food Biochem. 2018, 42, e12631. [Google Scholar] [CrossRef]
- Omidian, M.; Mahmoudi, M.; Abshirini, M.; Eshraghian, M.R.; Javanbakht, M.H.; Zarei, M.; Hasani, H.; Djalali, M. Effects of Vitamin D Supplementation on Depressive Symptoms in Type 2 Diabetes Mellitus Patients: Randomized Placebo-Controlled Double-Blind Clinical Trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2375–2380. [Google Scholar] [CrossRef] [PubMed]
- Omidian, M.; Mahmoudi, M.; Javanbakht, M.H.; Eshraghian, M.R.; Abshirini, M.; Daneshzad, E.; Hasani, H.; Alvandi, E.; Djalali, M. Effects of Vitamin D Supplementation on Circulatory YKL-40 and MCP-1 Biomarkers Associated with Vascular Diabetic Complications: A Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2873–2877. [Google Scholar] [CrossRef]
- Dadrass, A.; Mohamadzadeh Salamat, K.; Hamidi, K.; Azizbeigi, K. Anti-Inflammatory Effects of Vitamin D and Resistance Training in Men with Type 2 Diabetes Mellitus and Vitamin D Deficiency: A Randomized, Double-Blinded, Placebo-Controlled Clinical Trial. J. Diabetes Metab. Disord. 2019, 18, 323–331. [Google Scholar] [CrossRef]
- Mirzavandi, F.; Talenezhad, N.; Razmpoosh, E.; Nadjarzadeh, A.; Mozaffari-Khosravi, H. The Effect of Intramuscular Megadose of Vitamin D Injections on E-Selectin, CRP and Biochemical Parameters in Vitamin D-Deficient Patients with Type-2 Diabetes Mellitus: A Randomized Controlled Trial. Complement. Ther. Med. 2020, 49, 102346. [Google Scholar] [CrossRef]
- Imanparast, F.; Javaheri, J.; Kamankesh, F.; Rafiei, F.; Salehi, A.; Mollaaliakbari, Z.; Rezaei, F.; Rahimi, A.; Abbasi, E. The Effects of Chromium and Vitamin D3 Co-Supplementation on Insulin Resistance and Tumor Necrosis Factor-Alpha in Type 2 Diabetes: A Randomized Placebo-Controlled Trial. Appl. Physiol. Nutr. Metab. 2019, 45, 471–477. [Google Scholar] [CrossRef]
- Hoseini, R.; Rahim, H.A.; Ahmed, J.K. Decreased Inflammatory Gene Expression Accompanies the Improvement of Liver Enzyme and Lipid Profile Following Aerobic Training and Vitamin D Supplementation in T2DM Patients. BMC Endocr. Disord. 2022, 22, 245. [Google Scholar] [CrossRef] [PubMed]
- Limonte, C.P.; Zelnick, L.R.; Ruzinski, J.; Hoofnagle, A.N.; Thadhani, R.; Melamed, M.L.; Lee, I.M.; Buring, J.E.; Sesso, H.D.; Manson, J.A.E.; et al. Effects of Long-Term Vitamin D and n-3 Fatty Acid Supplementation on Inflammatory and Cardiac Biomarkers in Patients with Type 2 Diabetes: Secondary Analyses from a Randomised Controlled Trial. Diabetologia 2021, 64, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Matthan, N.R.; Angellotti, E.; Pittas, A.G.; Lichtenstein, A.H. Exploring the Effect of Vitamin D3 Supplementation on Surrogate Biomarkers of Cholesterol Absorption and Endogenous Synthesis in Patients with Type 2 Diabetes-Randomized Controlled Trial. Am. J. Clin. Nutr. 2020, 112, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Angellotti, E.; D’Alessio, D.; Dawson-Hughes, B.; Chu, Y.; Nelson, J.; Hu, P.; Cohen, R.M.; Pittas, A.G. Effect of Vitamin D Supplementation on Cardiovascular Risk in Type 2 Diabetes. Clin. Nutr. 2019, 38, 2449–2453. [Google Scholar] [CrossRef]
- Witham, M.D.; Dove, F.J.; Dryburgh, M.; Sugden, J.A.; Morris, A.D.; Struthers, A.D. The Effect of Different Doses of Vitamin D3 on Markers of Vascular Health in Patients with Type 2 Diabetes: A Randomised Controlled Trial. Diabetologia 2010, 53, 2112–2119. [Google Scholar] [CrossRef]
- Punthakee, Z.; Bosch, J.; Dagenais, G.; Diaz, R.; Holman, R.; Probstfield, J.L.; Ramachandran, A.; Riddle, M.C.; Rydén, L.E.; Zinman, B.; et al. Design, History and Results of the Thiazolidinedione Intervention with Vitamin D Evaluation (TIDE) Randomised Controlled Trial. Diabetologia 2012, 55, 36–45. [Google Scholar] [CrossRef]
- Lemieux, P.; John Weisnagel, S.; Caron, A.Z.; Julien, A.S.; Morisset, A.S.; Carreau, A.M.; Poirier, J.; Tchernof, A.; Robitaille, J.; Bergeron, J.; et al. Effects of 6-Month Vitamin D Supplementation on Insulin Sensitivity and Secretion: A Randomised, Placebo-Controlled Trial. Eur. J. Endocrinol. 2019, 181, 287–299. [Google Scholar] [CrossRef]
- Barchetta, I.; Del Ben, M.; Angelico, F.; Di Martino, M.; Fraioli, A.; La Torre, G.; Saulle, R.; Perri, L.; Morini, S.; Tiberti, C.; et al. No Effects of Oral Vitamin D Supplementation on Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. BMC Med. 2016, 14, 92. [Google Scholar] [CrossRef]
- Barale, M.; Rossetto Giaccherino, R.; Ghigo, E.; Procopio, M. Effect of 1-Year Oral Cholecalciferol on a Metabolic Profile and Blood Pressure in Poor-Controlled Type 2 Diabetes Mellitus: An Open-Label Randomized Controlled Pilot Study. J. Endocrinol. Investig. 2021, 44, 791–802. [Google Scholar] [CrossRef]
- Maggi, S.; Siviero, P.; Brocco, E.; Albertin, M.; Romanato, G.; Crepaldi, G. Vitamin D Deficiency, Serum Leptin and Osteoprotegerin Levels in Older Diabetic Patients: An Input to New Research Avenues. Acta Diabetol. 2014, 51, 461–469. [Google Scholar] [CrossRef]
- Gagnon, C.; Daly, R.M.; Carpentier, A.; Lu, Z.X.; Shore-Lorenti, C.; Sikaris, K.; Jean, S.; Ebeling, P.R. Effects of Combined Calcium and Vitamin D Supplementation on Insulin Secretion, Insulin Sensitivity and β-Cell Function in Multi-Ethnic Vitamin D-Deficient Adults at Risk for Type 2 Diabetes: A Pilot Randomized, Placebo-Controlled Trial. PLoS ONE 2014, 9, e109607. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Zhi, X.; Li, J.; Li, B.; Wang, J.; Zhu, J.; Zhang, Z. Effects of Long-Term Vitamin D Supplementation on Metabolic Profile in Middle-Aged and Elderly Patients with Type 2 Diabetes. J. Steroid Biochem. Mol. Biol. 2022, 225, 106198. [Google Scholar] [CrossRef] [PubMed]
- Kampmann, U.; Mosekilde, L.; Juhl, C.; Moller, N.; Christensen, B.; Rejnmark, L.; Wamberg, L.; Orskov, L. Effects of 12 Weeks High Dose Vitamin D3 Treatment on Insulin Sensitivity, Beta Cell Function, and Metabolic Markers in Patients with Type 2 Diabetes and Vitamin D Insufficiency—A Double-Blind, Randomized, Placebo-Controlled Trial. Metabolism 2014, 63, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Upreti, V.; Maitri, V.; Dhull, P.; Handa, A.; Prakash, M.S.; Behl, A. Effect of Oral Vitamin D Supplementation on Glycemic Control in Patients with Type 2 Diabetes Mellitus with Coexisting Hypovitaminosis D: A Parellel Group Placebo Controlled Randomized Controlled Pilot Study. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Breslavsky, A.; Frand, J.; Matas, Z.; Boaz, M.; Barnea, Z.; Shargorodsky, M. Effect of High Doses of Vitamin D on Arterial Properties, Adiponectin, Leptin and Glucose Homeostasis in Type 2 Diabetic Patients. Clin. Nutr. 2013, 32, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Ryu, O.H.; Chung, W.; Lee, S.; Hong, K.S.; Choi, M.G.; Yoo, H.J. The Effect of High-Dose Vitamin D Supplementation on Insulin Resistance and Arterial Stiffness in Patients with Type 2 Diabetes. Korean J. Intern. Med. 2014, 29, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Aguirre, P.; Flores, M.; Macias, N.; Quezada, A.D.; Denova-Gutiérrez, E.; Salmerón, J. The Effect of Vitamin D Supplementation on Serum Lipids in Postmenopausal Women with Diabetes: A Randomized Controlled Trial. Clin. Nutr. 2015, 34, 799–804. [Google Scholar] [CrossRef]
- Dalan, R.; Liew, H.; Assam, P.N.; Chan, E.S.Y.; Siddiqui, F.J.; Tan, A.W.K.; Chew, D.E.K.; Boehm, B.O.; Leow, M.K.S. A Randomised Controlled Trial Evaluating the Impact of Targeted Vitamin D Supplementation on Endothelial Function in Type 2 Diabetes Mellitus: The DIMENSION Trial. Diab Vasc. Dis. Res. 2016, 13, 192–200. [Google Scholar] [CrossRef]
- Jehle, S.; Lardi, A.; Felix, B.; Hulter, H.N.; Stettler, C.; Krapf, R. Effect of Large Doses of Parenteral Vitamin D on Glycaemic Control and Calcium/Phosphate Metabolism in Patients with Stable Type 2 Diabetes Mellitus: A Randomised, Placebo-Controlled, Prospective Pilot Study. Swiss Med. Wkly. 2014, 144, w13942. [Google Scholar] [CrossRef]
- El Hajj, C.; Walrand, S.; Helou, M.; Yammine, K. Effect of Vitamin D Supplementation on Inflammatory Markers in Non-Obese Lebanese Patients with Type 2 Diabetes: A Randomized Controlled Trial. Nutrients 2020, 12, 2033. [Google Scholar] [CrossRef]
- Wenclewska, S.; Szymczak-Pajor, I.; Drzewoski, J.; Bunk, M.; Śliwińska, A. Vitamin d Supplementation Reduces Both Oxidative Dna Damage and Insulin Resistance in the Elderly with Metabolic Disorders. Int. J. Mol. Sci. 2019, 20, 2891. [Google Scholar] [CrossRef] [PubMed]
- Hoseini, R.; Damirchi, A.; Babaei, P. Vitamin D Increases PPARγ Expression and Promotes Beneficial Effects of Physical Activity in Metabolic Syndrome. Nutrition 2017, 36, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.C.; Wu, Y.G.; Huang, W.G.; Fan, X.J.; Chen, X.H.; Zhou, B.; Lin, Z.J.; Feng, X.L. Effect of Vitamin D on Oxidative Stress and Serum Inflammatory Factors in the Patients with Type 2 Diabetes. J. Clin. Lab. Anal. 2022, 36, e24430. [Google Scholar] [CrossRef] [PubMed]
- Calton, E.K.; Keane, K.N.; Newsholme, P.; Soares, M.J. The Impact of Vitamin D Levels on Inflammatory Status: A Systematic Review of Immune Cell Studies. PLoS ONE 2015, 10, e0141770. [Google Scholar] [CrossRef]
- Jorde, R.; Grimnes, G. Increased Calcium Intake Is Associated Lower Serum 25-Hydroxyvitamin D Levels in Subjects with Adequate Vitamin D Intake: A Population-Based Observational Study. BMC Nutr. 2020, 6, 49. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Vatanparast, H. Impact of Vitamin D Supplementation on C-Reactive Protein; A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BMC Nutr. 2018, 4, 1. [Google Scholar] [CrossRef]
- Caetano, D.G.; Ribeiro-Alves, M.; Hottz, E.D.; Vilela, L.M.; Cardoso, S.W.; Hoagland, B.; Grinsztejn, B.; Veloso, V.G.; Morgado, M.G.; Bozza, P.T.; et al. Increased Biomarkers of Cardiovascular Risk in HIV-1 Viremic Controllers and Low Persistent Inflammation in Elite Controllers and Art-Suppressed Individuals. Sci. Rep. 2022, 12, 6569. [Google Scholar] [CrossRef]
- Gao, B.; Tsukamoto, H. Inflammation in Alcoholic and Non-alcoholic Fatty Liver Disease: Friend or Foe? Gastroenterology 2016, 150, 1704–1709. [Google Scholar] [CrossRef]
- Chen, N.; Wan, Z.; Han, S.F.; Li, B.Y.; Zhang, Z.L.; Qin, L.Q. Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2014, 6, 2206–2216. [Google Scholar] [CrossRef]
- Agbalalah, T.; Hughes, S.F.; Freeborn, E.J.; Mushtaq, S. Impact of Vitamin D Supplementation on Endothelial and Inflammatory Markers in Adults: A Systematic Review. J. Steroid Biochem. Mol. Biol. 2017, 173, 292–300. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Chertow, G.M.; Devarajan, P.; Levin, A.; Andreoli, S.P.; Bangalore, S.; Warady, B.A. Chronic Inflammation in Chronic Kidney Disease Progression: Role of Nrf2. Kidney Int. Rep. 2021, 6, 1775–1787. [Google Scholar] [CrossRef]
- Wöbke, T.K.; Sorg, B.L.; Steinhilber, D. Vitamin D in Inflammatory Diseases. Front. Physiol. 2014, 7, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Leung, D.Y.M.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W.; Goleva, E. Vitamin D Inhibits Monocyte/Macrophage Pro-inflammatory Cytokine Production by Targeting MAPK Phosphatase-1. J. Immunol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Lahore, G.F.; Raposo, B.; Lagerquist, M.; Ohlsson, C.; Sabatier, P.; Xu, B.; Aoun, M.; James, J.; Cai, X.; Zubarev, R.M.; et al. Vitamin D3 Receptor Polymorphisms Regulate T Cells and T Cell-Dependent Inflammatory Diseases. Proc. Natl. Acad. Sci USA 2020, 117, 24986–24997. [Google Scholar] [CrossRef] [PubMed]
- Kongsbak, M.; Levring, T.B.; Geisler, C.; von Essen, M.R. The Vitamin D Receptor and T Cell Function. Front. Immunol. 2013, 4, 148. [Google Scholar] [CrossRef] [PubMed]
- Riek, A.E.; Oh, J.; Darwech, I.; Worthy, V.; Lin, X.; Ostlund, R.E.; Zhang, R.M.; Bernal-Mizrachi, C. Vitamin D 3 Supplementation Decreases a Unique Circulating Monocyte Cholesterol Pool in Patients with Type 2 Diabetes. J. Steroid Biochem. Mol. Biol. 2018, 177, 187–192. [Google Scholar] [CrossRef]
- Yiu, Y.F.; Yiu, K.H.; Siu, C.W.; Chan, Y.H.; Li, S.W.; Wong, L.Y.; Lee, S.W.L.; Tam, S.; Wong, E.W.K.; Lau, C.P.; et al. Randomized Controlled Trial of Vitamin D Supplement on Endothelial Function in Patients with Type 2 Diabetes. Atherosclerosis 2013, 227, 140–146. [Google Scholar] [CrossRef]
- Qi, K.J.; Zhao, Z.T.; Zhang, W.; Yang, F. The Impacts of Vitamin D Supplementation in Adults with Metabolic Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Pharmacol. 2022, 13, 1033026. [Google Scholar] [CrossRef]
- Li, S.; He, Y.; Lin, S.; Hao, L.; Ye, Y.; Lv, L.; Sun, Z.; Fan, H.; Shi, Z.; Li, J.; et al. Increase of Circulating Cholesterol in Vitamin D Deficiency Is Linked to Reduced Vitamin D Receptor Activity via the Insig-2/SREBP-2 Pathway. Mol. Nutr. Food Res. 2016, 60, 798–809. [Google Scholar] [CrossRef]
- Wang, X.X.; Jiang, T.; Shen, Y.; Santamaria, H.; Solis, N.; Arbeeny, C.; Levi, M.; Levi, M. Vitamin D Receptor Agonist Doxercalciferol Modulates Dietary Fat-Induced Renal Disease and Renal Lipid Metabolism. Am. J. Physiol. Ren. Physiol. 2011, 300, 801–810. [Google Scholar] [CrossRef]
- Asano, L.; Watanabe, M.; Ryoden, Y.; Usuda, K.; Yamaguchi, T.; Khambu, B.; Takashima, M.; Sato, S.-i.; Sakai, J.; Nagasawa, K.; et al. Vitamin D Metabolite, 25-Hydroxyvitamin D, Regulates Lipid Metabolism by Inducing Degradation of SREBP/SCAP. Cell Chem. Biol. 2017, 24, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Larrick, B.M.; Kim, K.H.; Donkin, S.S.; Teegarden, D. 1,25-Dihydroxyvitamin D Regulates Lipid Metabolism and Glucose Utilization in Differentiated 3T3-L1 Adipocytes. Nutr. Res. 2018, 58, 72–83. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacGirlley, R.; Phoswa, W.N.; Mokgalaboni, K. Modulatory Properties of Vitamin D in Type 2 Diabetic Patients: A Focus on Inflammation and Dyslipidemia. Nutrients 2023, 15, 4575. https://doi.org/10.3390/nu15214575
MacGirlley R, Phoswa WN, Mokgalaboni K. Modulatory Properties of Vitamin D in Type 2 Diabetic Patients: A Focus on Inflammation and Dyslipidemia. Nutrients. 2023; 15(21):4575. https://doi.org/10.3390/nu15214575
Chicago/Turabian StyleMacGirlley, Rizqah, Wendy N. Phoswa, and Kabelo Mokgalaboni. 2023. "Modulatory Properties of Vitamin D in Type 2 Diabetic Patients: A Focus on Inflammation and Dyslipidemia" Nutrients 15, no. 21: 4575. https://doi.org/10.3390/nu15214575
APA StyleMacGirlley, R., Phoswa, W. N., & Mokgalaboni, K. (2023). Modulatory Properties of Vitamin D in Type 2 Diabetic Patients: A Focus on Inflammation and Dyslipidemia. Nutrients, 15(21), 4575. https://doi.org/10.3390/nu15214575