
Effectiveness of Chickpeas on Blood Sugar: A Systematic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Searches
2.3. Study Selection
2.3.1. Study Design
2.3.2. Participants
2.3.3. Interventions
2.3.4. Outcome Measures
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis and Synthesis
3. Results
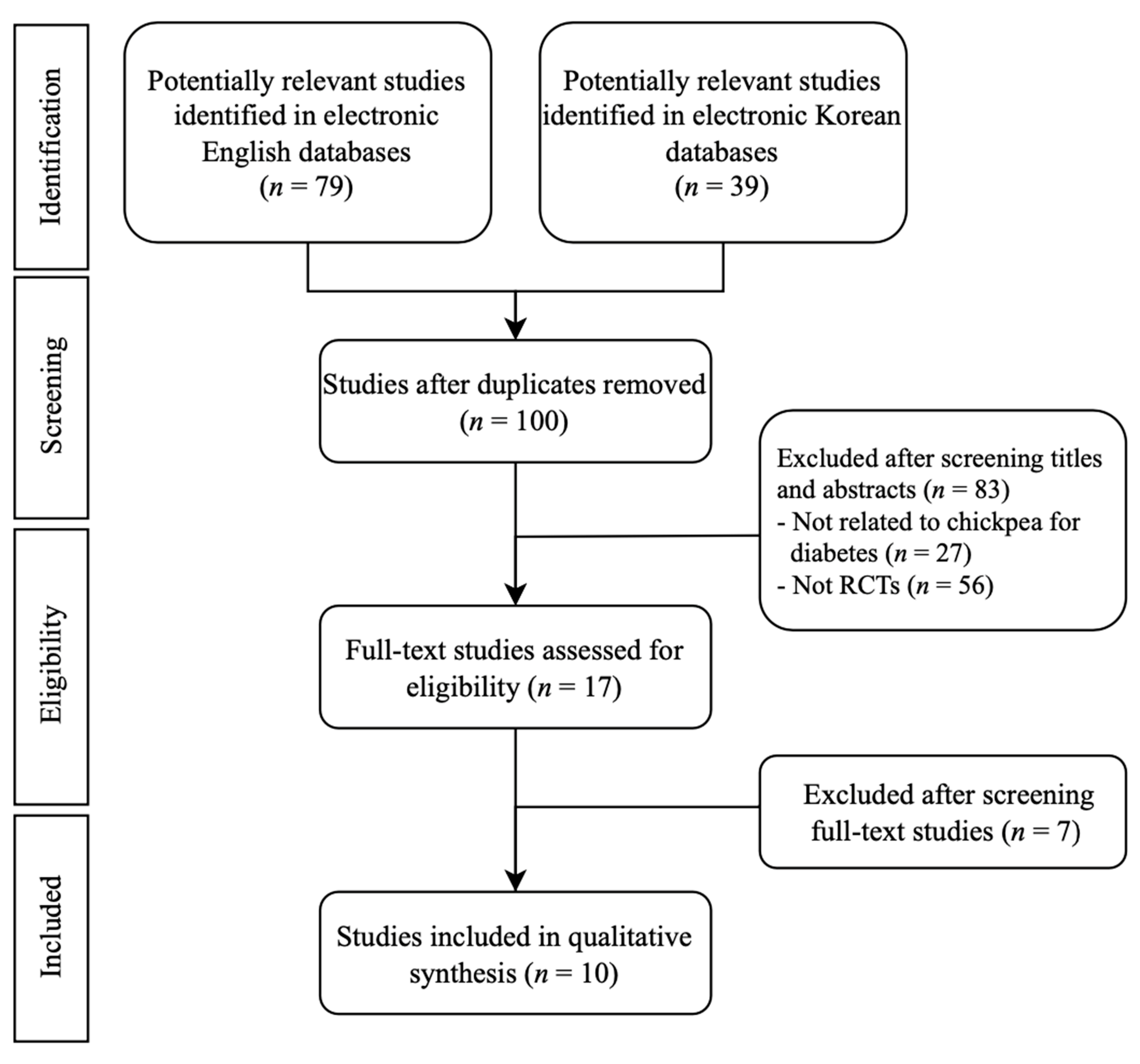
3.1. Study Selection and Description
3.2. Participants
3.3. Outcomes
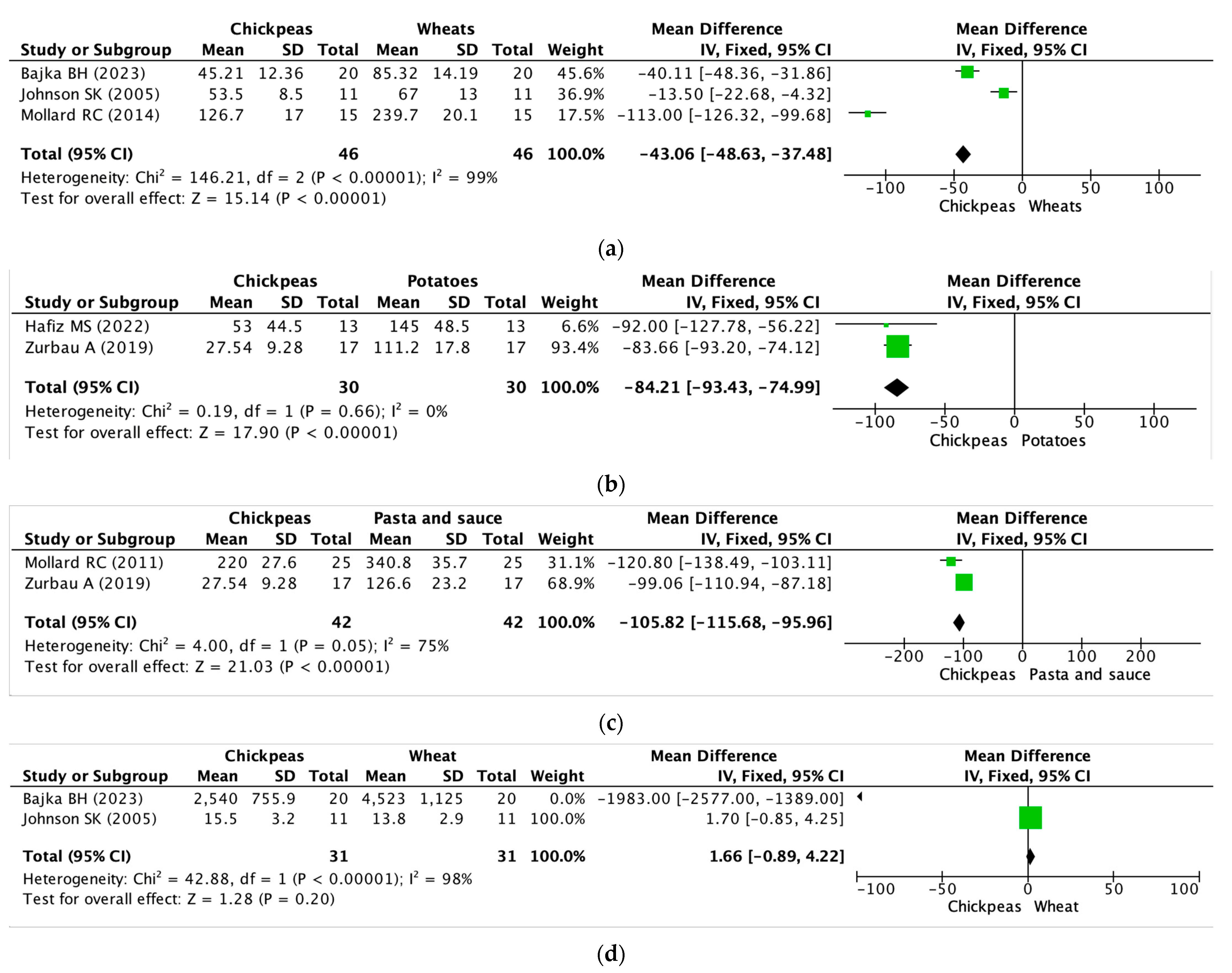
3.3.1. Chickpeas versus Wheat
3.3.2. Chickpeas versus Potatoes
3.3.3. Chickpeas versus Pasta
3.3.4. Chickpeas versus Cheese
3.3.5. Chickpeas versus Rice
3.3.6. Chickpeas versus Corn
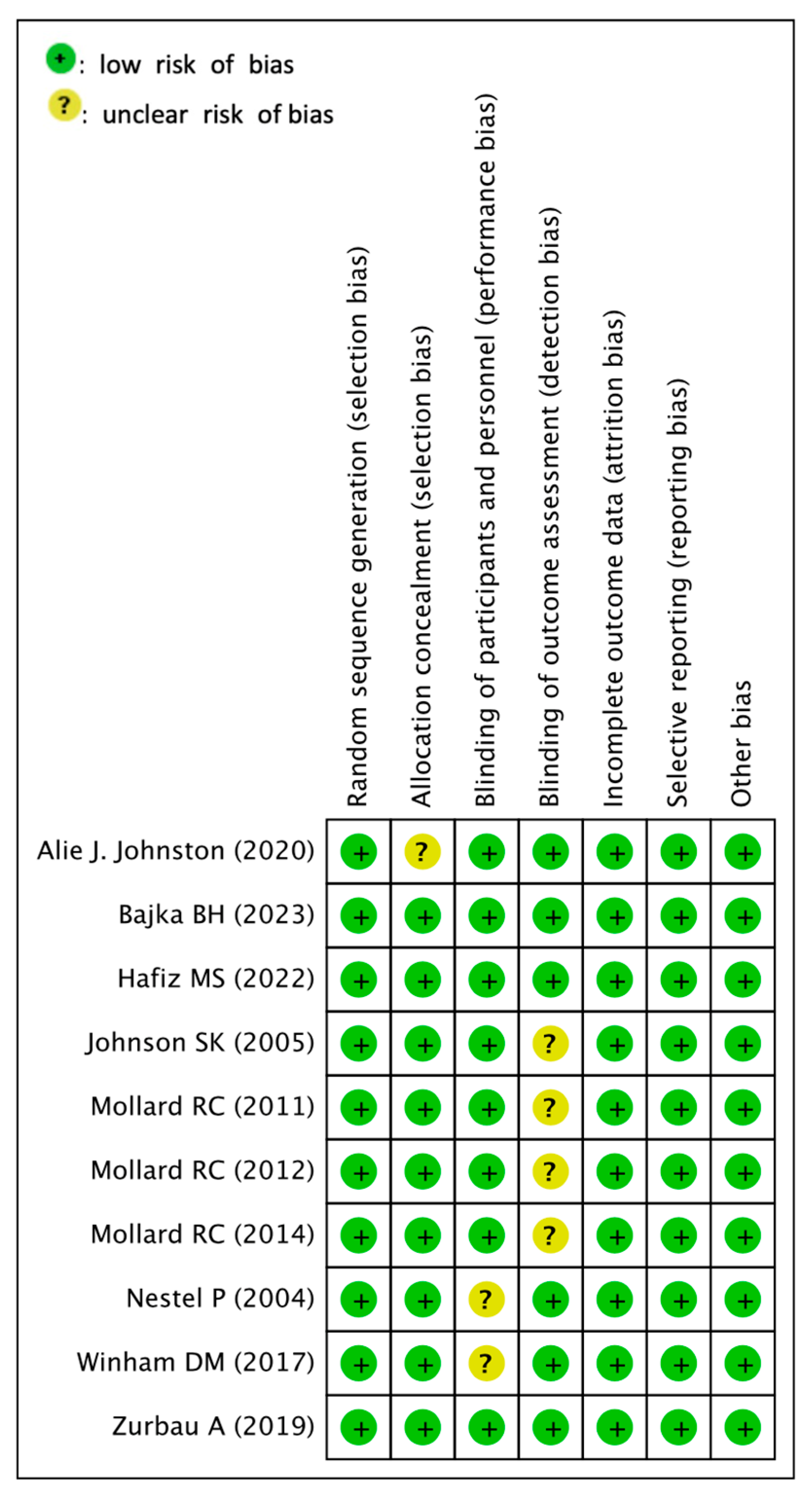
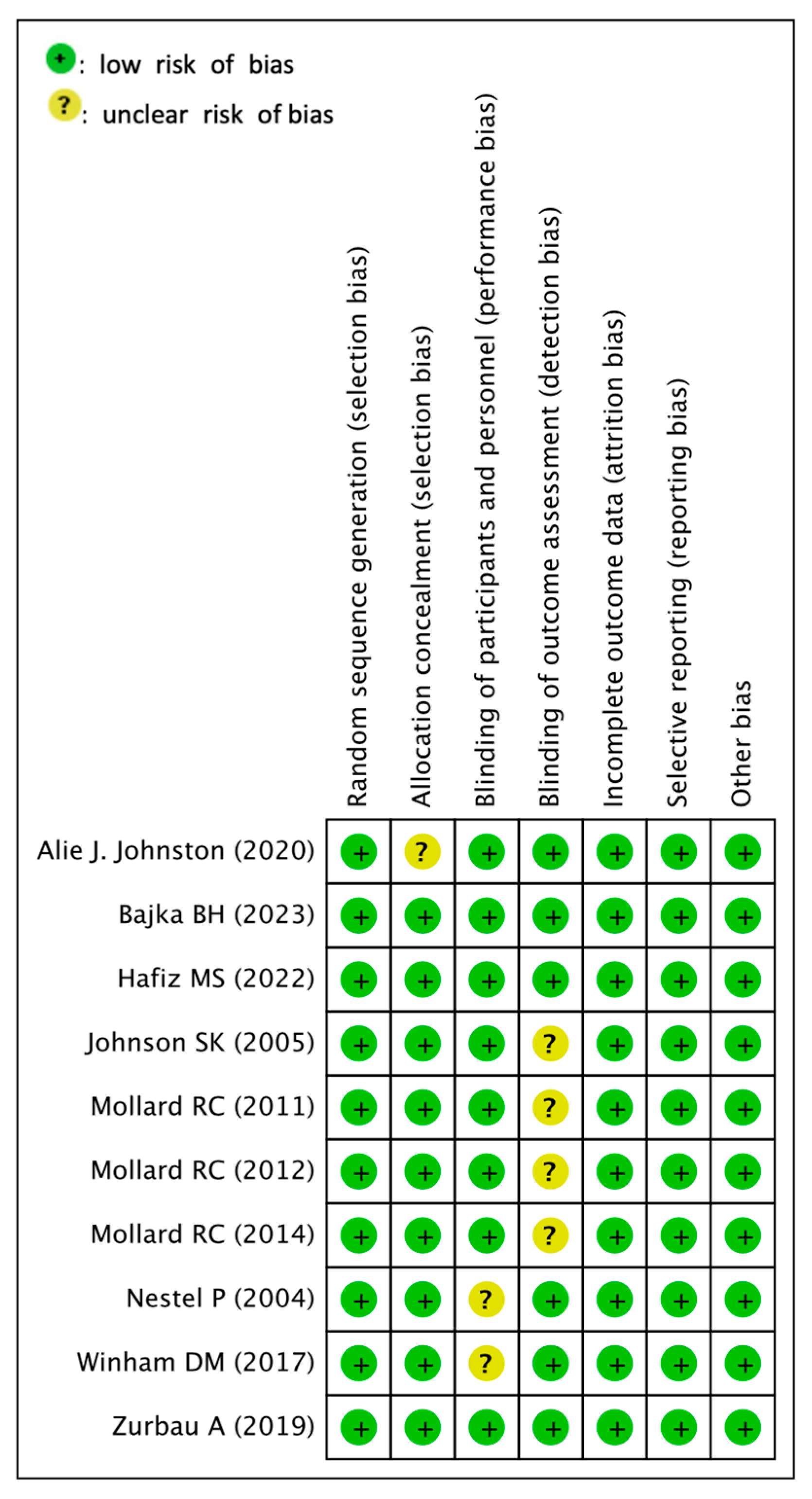
3.4. Assessment for Risk of Bias
3.5. Meta-Analysis or Quantitative Analysis of the Included Articles
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

| NO. | Search Strategy | Item |
|---|---|---|
| #1 | Cicer arietinum OR chickpea OR chick pea | 119 |
| #2 | MeSH descriptor: [Diabetes Mellitus] explode all trees | 45,956 |
| #3 | MeSH descriptor: [Blood Glucose] explode all trees | 19,279 |
| #4 | (“Randomized Controlled Trial”):pt OR (“Controlled Clinical Trial”):pt OR (randomized):ti,ab,kw OR (placebo):ti,ab,kw OR (randomly):ti,ab,kw OR (trial):ti,ab,kw | 140,645 |
| #5 | #1 AND (#2 OR #3) AND #4 | 19 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | Cicer arietinum OR chickpea OR chick pea | 3547 |
| #2 | Diabetes mellitus[Mesh] OR blood sugar[Mesh] | 605,155 |
| #3 | Randomized Controlled Trial OR Controlled Clinical Trial OR randomized OR placebo OR randomly OR trial | 2,784,527 |
| #4 | #1 AND #2 AND #3 | 35 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | . ‘cicer arietinum’/exp OR ‘cicer arietinum’ OR ‘chickpea’/exp OR chickpea OR ‘chick pea’ | 3661 |
| #2 | . ‘diabetes mellitus’ OR diabetes OR ‘blood sugar’ OR ‘blood glucose’ | 1,561,079 |
| #3 | . ‘randomized controlled trial’/exp AND ‘randomized controlled trial’:it OR ‘controlled clinical trial’:it OR randomized:ti,ab,kw OR placebo:ti,ab,kw OR randomly:ti,ab,kw OR trial:ab,ti OR ‘clinical trials’:ti,ab,kw | 2,442,971 |
| #4 | . #1 AND #2 AND #3 | 43 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | Search ( (“cicer arietinum”[ALL]) OR (“chickpea”[ALL]) OR (“chick pea”[ALL])) | 3 |
| #2 | Search ( (diabetes mellitus[MH]) OR (blood sugar[MH]) OR (“diabetes”[ALL])) | 11,533 |
| #3 | Search ( (“randomized”[ALL]) OR (“clinical”[ALL]) OR (“controlled”[ALL]) OR (“trials”[ALL])) | 1100 |
| #4 | #1 AND #2 AND #3 | 0 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | cicer arietinum|chickpea|chick pea|병아리콩 | 920 |
| #2 | blood sugar|blood glucose|diabetes|diabetes mellitus|혈당|당뇨 | 110,535 |
| #3 | #1 AND #2 | 20 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | “전체 = ““cicer arietinum”“ or 전체 = ““chickpea”“ or 전체 = ““병아리콩”“ | 38 |
| NO. | Search Strategy | Item |
|---|---|---|
| #1 | “cicer arietinum”|”chickpea”|”chick pea”|”병아리콩” | 13,510 |
| #2 | “blood sugar”|”blood glucose”|”diabetes”|”diabetes mellitus”|”혈당”|”당뇨” | 1,024,818 |
| #3 | “Randomized Trials”|”Controlled trials”|”Randomized Clinical Trials”|무작위 임상|무작위 시험|placebo|Randomized | 332,557 |
| #4 | #1 AND #2 AND #3 | 2 |
References
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global Aetiology and Epidemiology of Type 2 Diabetes Mellitus and Its Complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, M.; Khursheed, R.; Yadav, A.K.; Singh, S.K.; Gulati, M.; Pandey, D.K.; Prabhakar, P.K.; Kumar, R.; Porwal, O.; Awasthi, A.; et al. A Systematic Review on Synthetic Drugs and Phytopharmaceuticals Used to Manage Diabetes. Curr. Diabetes Rev. 2020, 16, 340–356. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.; Martin, S. Environmental/Lifestyle Factors in the Pathogenesis and Prevention of Type 2 Diabetes. BMC Med. 2017, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Bornfeldt, K.E.; Goldberg, I.J. Cardiovascular Disease in Diabetes, beyond Glucose. Cell Metab. 2021, 33, 1519–1545. [Google Scholar] [CrossRef]
- Cummings, J.; Ortiz, A.; Castellino, J.; Kinney, J. Diabetes: Risk Factor and Translational Therapeutic Implications for Alzheimer’s Disease. Eur. J. Neurosci. 2022, 56, 5727–5757. [Google Scholar] [CrossRef]
- Lei, C.; Duan, J.; Ge, G.; Zhang, M. Association between Neonatal Hyperglycemia and Retinopathy of Prematurity: A Meta-Analysis. Eur. J. Pediatr. 2021, 180, 3433–3442. [Google Scholar] [CrossRef]
- Kozakova, M.; Palombo, C. Diabetes Mellitus, Arterial Wall, and Cardiovascular Risk Assessment. Int. J. Environ. Res. Public Health 2016, 13, 201. [Google Scholar] [CrossRef]
- Shikata, K.; Ninomiya, T.; Kiyohara, Y. Diabetes Mellitus and Cancer Risk: Review of the Epidemiological Evidence. Cancer Sci. 2013, 104, 9–14. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Cusi, K.; Das, S.R.; Gibbons, C.H.; et al. Summary of Revisions: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S5–S9. [Google Scholar] [CrossRef]
- Vlachos, D.; Malisova, S.; Lindberg, F.A.; Karaniki, G. Glycemic Index (GI) or Glycemic Load (GL) and Dietary Interventions for Optimizing Postprandial Hyperglycemia in Patients with T2 Diabetes: A Review. Nutrients 2020, 12, 1561. [Google Scholar] [CrossRef]
- Vega-López, S.; Venn, B.; Slavin, J. Relevance of the Glycemic Index and Glycemic Load for Body Weight, Diabetes, and Cardiovascular Disease. Nutrients 2018, 10, 1361. [Google Scholar] [CrossRef]
- Zafar, M.I.; Mills, K.E.; Zheng, J.; Regmi, A.; Hu, S.Q.; Gou, L.; Chen, L.-L. Low-Glycemic Index Diets as an Intervention for Diabetes: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2019, 110, 891–902. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Lee, D.; Ahmed, A.; Cheung, A.; Khan, T.A.; Blanco, S.; Mejia; Mirrahimi, A.; Jenkins, D.J.A.; Livesey, G.; et al. Effect of Low Glycaemic Index or Load Dietary Patterns on Glycaemic Control and Cardiometabolic Risk Factors in Diabetes: Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2021, 374, n1651. [Google Scholar] [CrossRef]
- Basiak-Rasała, A.; Różańska, D.; Zatońska, K. Food Groups in Dietary Prevention of Type 2 Diabetes. Rocz. Panstw. Zakl. Hig. 2019, 70, 347–357. [Google Scholar] [CrossRef]
- Williams, D.R.R.; James, W.P.T. Fibre and Diabetes. Lancet 1979, 313, 271–272. [Google Scholar] [CrossRef]
- Elia, M.; Ceriello, A.; Laube, H.; Sinclair, A.J.; Engfer, M.; Stratton, R.J. Enteral Nutritional Support and Use of Diabetes-Specific Formulas for Patients with Diabetes. Diabetes Care 2005, 28, 2267–2279. [Google Scholar] [CrossRef]
- Warshaw, H.; Franz, M.; Powers, M.A.; Wheeler, M. Fat Replacers: Their Use in Foods and Role in Diabetes Medical Nutrition Therapy. Diabetes Care 1996, 19, 1294–1301. [Google Scholar] [CrossRef]
- Jiménez-Cortegana, C.; Iglesias, P.; Ribalta, J.; Vilariño-García, T.; Montañez, L.; Arrieta, F.; Aguilar, M.; Durán, S.; Obaya, J.C.; Becerra, A.; et al. Nutrients and Dietary Approaches in Patients with Type 2 Diabetes Mellitus and Cardiovascular Disease: A Narrative Review. Nutrients 2021, 13, 4150. [Google Scholar] [CrossRef]
- Berraaouan, A.; Abid, S.; Bnouham, M. Antidiabetic Oils. Curr. Diabetes Rev. 2013, 9, 499–505. [Google Scholar] [CrossRef]
- Yedjou, C.G.; Grigsby, J.; Mbemi, A.; Nelson, D.; Mildort, B.; Latinwo, L.; Tchounwou, P.B. The Management of Diabetes Mellitus Using Medicinal Plants and Vitamins. Int. J. Mol. Sci. 2023, 24, 9085. [Google Scholar] [CrossRef]
- Reddy, S.; Anoop, S.; Jebasingh, F.K.; Dasgupta, R.; Joseph, M.; Saravanan, B.; Volena, R.; Mani, T.; Somasundaram, S.; Bhattacharji, S.; et al. Differentials in Dietary Intake of Macro and Micronutrients in Patients with Type 2 Diabetes and Foot Ulcers: Observations from a Pilot Study. Clin. Nutr. ESPEN 2022, 47, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Shamim, M.Z.; Mishra, A.K.; Kausar, T.; Mahanta, S.; Sarma, B.; Kumar, V.; Mishra, P.K.; Panda, J.; Baek, K.-H.; Mohanta, Y.K. Exploring Edible Mushrooms for Diabetes: Unveiling Their Role in Prevention and Treatment. Molecules 2023, 28, 2837. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Manickavasagan, A.; Shobana, S.; Mohan, V. Glycemic Index of Pulses and Pulse-Based Products: A Review. Crit. Rev. Food Sci. Nutr. 2021, 61, 1567–1588. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.-J.; Liu, Q.; Hoover, R.; Warkentin, T.D.; Vandenberg, B. In Vitro Starch Digestibility, Expected Glycemic Index, and Thermal and Pasting Properties of Flours from Pea, Lentil and Chickpea Cultivars. Food Chem. 2008, 111, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Altaf, U.; Hussain, S.Z.; Naseer, B.; Amin, T.; Bashir, O. Nutritional and Bioactive Components of Rice-chickpea Based Snacks as Affected by Severe and Mild Extrusion Cooking. J. Sci. Food Agric. 2022, 102, 7126–7135. [Google Scholar] [CrossRef] [PubMed]
- Gkountenoudi-Eskitzi, I.; Kotsiou, K.; Irakli, M.N.; Lazaridis, A.; Biliaderis, C.G.; Lazaridou, A. In Vitro and in Vivo Glycemic Responses and Antioxidant Potency of Acorn and Chickpea Fortified Gluten-Free Breads. Food Res. Int. 2023, 166, 112579. [Google Scholar] [CrossRef]
- Kazemi, M.; McBreairty, L.; Chizen, D.; Pierson, R.; Chilibeck, P.; Zello, G. A Comparison of a Pulse-Based Diet and the Therapeutic Lifestyle Changes Diet in Combination with Exercise and Health Counselling on the Cardio-Metabolic Risk Profile in Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Nutrients 2018, 10, 1387. [Google Scholar] [CrossRef]
- Sievenpiper, J.L.; Kendall, C.W.C.; Esfahani, A.; Wong, J.M.W.; Carleton, A.J.; Jiang, H.Y.; Bazinet, R.P.; Vidgen, E.; Jenkins, D.J.A. Effect of Non-Oil-Seed Pulses on Glycaemic Control: A Systematic Review and Meta-Analysis of Randomised Controlled Experimental Trials in People with and without Diabetes. Diabetologia 2009, 52, 1479–1495. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Augustin, L.S.A.; Mitchell, S.; Sahye-Pudaruth, S.; Blanco Mejia, S.; Chiavaroli, L.; Mirrahimi, A.; Ireland, C.; Bashyam, B.; et al. Effect of Legumes as Part of a Low Glycemic Index Diet on Glycemic Control and Cardiovascular Risk Factors in Type 2 Diabetes Mellitus. Arch. Intern. Med. 2012, 172, 1653. [Google Scholar] [CrossRef]
- Rehm, C.D.; Goltz, S.R.; Katcher, J.A.; Guarneiri, L.L.; Dicklin, M.R.; Maki, K.C. Trends and Patterns of Chickpea Consumption among United States Adults: Analyses of National Health and Nutrition Examination Survey Data. J. Nutr. 2023, 153, 1567–1576. [Google Scholar] [CrossRef] [PubMed]
- Mordor Intelligence Research & Advisory. Chickpea Market Size & Share Analysis—Growth Trends & Forecasts (2023–2028). 2023. Available online: https://www.mordorintelligence.com/industry-reports/chickpea-market (accessed on 9 October 2023).
- Pearce, M.; Fanidi, A.; Bishop, T.R.P.; Sharp, S.J.; Imamura, F.; Dietrich, S.; Akbaraly, T.; Bes-Rastrollo, M.; Beulens, J.W.J.; Byberg, L.; et al. Associations of Total Legume, Pulse, and Soy Consumption with Incident Type 2 Diabetes: Federated Meta-Analysis of 27 Studies from Diverse World Regions. J. Nutr. 2021, 151, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Lonnie, M.; Laurie, I.; Myers, M.; Horgan, G.; Russell, W.; Johnstone, A. Exploring Health-Promoting Attributes of Plant Proteins as a Functional Ingredient for the Food Sector: A Systematic Review of Human Interventional Studies. Nutrients 2020, 12, 2291. [Google Scholar] [CrossRef] [PubMed]
- Nestel, P.; Cehun, M.; Chronopoulos, A. Effects of Long-Term Consumption and Single Meals of Chickpeas on Plasma Glucose, Insulin, and Triacylglycerol Concentrations. Am. J. Clin. Nutr. 2004, 79, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Mollard, R.C.; Wong, C.L.; Luhovyy, B.L.; Cho, F.; Anderson, G.H. Second-Meal Effects of Pulses on Blood Glucose and Subjective Appetite Following a Standardized Meal 2 h Later. Appl. Physiol. Nutr. Metab. 2014, 39, 849–851. [Google Scholar] [CrossRef] [PubMed]
- Winham, D.M.; Hutchins, A.M.; Thompson, S.V. Glycemic Response to Black Beans and Chickpeas as Part of a Rice Meal: A Randomized Cross-Over Trial. Nutrients 2017, 9, 1095. [Google Scholar] [CrossRef]
- Johnson, S.K.; Thomas, S.J.; Hall, R.S. Palatability and Glucose, Insulin and Satiety Responses of Chickpea Flour and Extruded Chickpea Flour Bread Eaten as Part of a Breakfast. Eur. J. Clin. Nutr. 2005, 59, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Mollard, R.C.; Wong, C.L.; Luhovyy, B.L.; Anderson, G.H. First and Second Meal Effects of Pulses on Blood Glucose, Appetite, and Food Intake at a Later Meal. Appl. Physiol. Nutr. Metab. 2011, 36, 634–642. [Google Scholar] [CrossRef]
- Mollard, R.C.; Zykus, A.; Luhovyy, B.L.; Nunez, M.F.; Wong, C.L.; Anderson, G.H. The Acute Effects of a Pulse-Containing Meal on Glycaemic Responses and Measures of Satiety and Satiation within and at a Later Meal. Br. J. Nutr. 2012, 108, 509–517. [Google Scholar] [CrossRef]
- Zurbau, A.; Jenkins, A.L.; Jovanovski, E.; Au-Yeung, F.; Bateman, E.A.; Brissette, C.; Wolever, T.M.S.; Hanna, A.; Vuksan, V. Acute Effect of Equicaloric Meals Varying in Glycemic Index and Glycemic Load on Arterial Stiffness and Glycemia in Healthy Adults: A Randomized Crossover Trial. Eur. J. Clin. Nutr. 2019, 73, 79–85. [Google Scholar] [CrossRef]
- Johnston, A.J.; Mollard, R.C.; Dandeneau, D.; MacKay, D.S.; Ames, N.; Curran, J.; Bouchard, D.R.; Jones, P.J. Acute Effects of Extruded Pulse Snacks on Glycemic Response, Insulin, Appetite, and Food Intake in Healthy Young Adults in a Double Blind, Randomized, Crossover Trial. Appl. Physiol. Nutr. Metab. 2021, 46, 704–710. [Google Scholar] [CrossRef]
- Hafiz, M.S.; Campbell, M.D.; Orsi, N.M.; Mappa, G.; Orfila, C.; Boesch, C. Impact of Food Processing on Postprandial Glycaemic and Appetite Responses in Healthy Adults: A Randomized, Controlled Trial. Food Funct. 2022, 13, 1280–1290. [Google Scholar] [CrossRef] [PubMed]
- Bajka, B.H.; Pinto, A.M.; Perez-Moral, N.; Saha, S.; Ryden, P.; Ahn-Jarvis, J.; van der Schoot, A.; Bland, C.; Berry, S.E.; Ellis, P.R.; et al. Enhanced Secretion of Satiety-Promoting Gut Hormones in Healthy Humans after Consumption of White Bread Enriched with Cellular Chickpea Flour: A Randomized Crossover Study. Am. J. Clin. Nutr. 2023, 117, 477–489. [Google Scholar] [CrossRef]
- McCrory, M.A.; Hamaker, B.R.; Lovejoy, J.C.; Eichelsdoerfer, P.E. Pulse Consumption, Satiety, and Weight Management. Adv. Nutr. 2010, 1, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, I.; Ahmed, A.R.; Senge, B. Dough Rheology and Bread Quality of Wheat–Chickpea Flour Blends. Ind. Crops Prod. 2012, 36, 196–202. [Google Scholar] [CrossRef]
- MacNeil, S.; Rebry, R.M.; Tetlow, I.J.; Emes, M.J.; McKeown, B.; Graham, T.E. Resistant Starch Intake at Breakfast Affects Postprandial Responses in Type 2 Diabetics and Enhances the Glucose-Dependent Insulinotropic Polypeptide—Insulin Relationship Following a Second Meal. Appl. Physiol. Nutr. Metab. 2013, 38, 1187–1195. [Google Scholar] [CrossRef]
- Zhou, J.; Martin, R.J.; Tulley, R.T.; Raggio, A.M.; McCutcheon, K.L.; Shen, L.; Danna, S.C.; Tripathy, S.; Hegsted, M.; Keenan, M.J. Dietary Resistant Starch Upregulates Total GLP-1 and PYY in a Sustained Day-Long Manner through Fermentation in Rodents. Am. J. Physiol. Endocrinol. Metab. 2008, 295, E1160–E1166. [Google Scholar] [CrossRef]
- D’Alessio, D.A.; Denney, A.M.; Hermiller, L.M.; Prigeon, R.L.; Martin, J.M.; Tharp, W.G.; Saylan, M.L.; He, Y.; Dunning, B.E.; Foley, J.E.; et al. Treatment with the Dipeptidyl Peptidase-4 Inhibitor Vildagliptin Improves Fasting Islet-Cell Function in Subjects with Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2009, 94, 81–88. [Google Scholar] [CrossRef]
- Dhital, S.; Bhattarai, R.R.; Gorham, J.; Gidley, M.J. Intactness of Cell Wall Structure Controls the in Vitro Digestion of Starch in Legumes. Food Funct. 2016, 7, 1367–1379. [Google Scholar] [CrossRef]
- Edwards, C.H.; Ryden, P.; Mandalari, G.; Butterworth, P.J.; Ellis, P.R. Structure–Function Studies of Chickpea and Durum Wheat Uncover Mechanisms by Which Cell Wall Properties Influence Starch Bioaccessibility. Nat. Food 2021, 2, 118–126. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Misra, A.; Mohan, V.; Taylor, R.; Yancy, W. Dietary and Nutritional Approaches for Prevention and Management of Type 2 Diabetes. BMJ 2018, 361, k2234. [Google Scholar] [CrossRef]
- Gardner, C.D.; Kim, S.; Bersamin, A.; Dopler-Nelson, M.; Otten, J.; Oelrich, B.; Cherin, R. Micronutrient Quality of Weight-Loss Diets That Focus on Macronutrients: Results from the A to Z Study. Am. J. Clin. Nutr. 2010, 92, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Gardner, C.D.; Trepanowski, J.F.; Del Gobbo, L.C.; Hauser, M.E.; Rigdon, J.; Ioannidis, J.P.A.; Desai, M.; King, A.C. Effect of Low-Fat vs Low-Carbohydrate Diet on 12-Month Weight Loss in Overweight Adults and the Association with Genotype Pattern or Insulin Secretion. JAMA 2018, 319, 667. [Google Scholar] [CrossRef]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition Therapy Recommendations for the Management of Adults with Diabetes. Diabetes Care 2013, 36, 3821–3842. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}

| Study ID | Nutritional Ingredients | Intervention | Control | |
|---|---|---|---|---|
| Nestel P (2004) [34] | Energy (kJ/day) | 7424 ± 2938 | 7524 ± 3947 | |
| Total fat (g/day) | 62 ± 34 | 67 ± 44 | ||
| Saturated fat (g/day) | 22 ± 14 | 26 ± 19 | ||
| Monounsaturated fat (g/day) | 20 ± 13 | 24 ± 17 | ||
| Polyunsaturated fat (g/day) | 11 ± 7 | 10 ± 7 | ||
| Protein (g/day) | 83 ± 32 | 89 ± 49 | ||
| Carbohydrates (g/day) | 222 ± 81 | 211 ± 100 | ||
| Fiber (g/day) | 33 ± 8 | 26 ± 13 | ||
| Cholesterol (mg/day) | 200 ± 119 | 235 ± 167 | ||
| Johnson SK (2005) [37] | Energy (kJ) | 1342 | 1251 | |
| Protein (g) | 11 | 9 | ||
| Fat (g) | 7 | 6 | ||
| Available carbohydrates (g) | 50 | 50 | ||
| Total dietary fiber (g) | 6 | 3 | ||
| Mollard RC (1) (2011) [38] | Energy (kcal) | 603.2 | 604.1 | |
| Weight (g) | 757.7 | 446.5 | ||
| Energy density (kcal·g−1) | 0.8 | 1.4 | ||
| Volume (mL) | 850.0 | 650.0 | ||
| Available carbohydrates (g/100 g) | 98.7 | 100.4 | ||
| Fiber (g) | 18.3 | 2.8 | ||
| Protein (g) | 26.1 | 22.8 | ||
| Fat (g) | 12.5 | 12.6 | ||
| Mollard RC (2) (2012) [39] | Energy (kJ/100 g) | 324.5 | 322.0 | |
| Fat (g/100 g) | 1.7 | 1.3 | ||
| Available carbohydrates (g/100 g) | 12.0 | 13.7 | ||
| Fiber (g/100 g) | 2.1 | 0.9 | ||
| Protein (g/100 g) | 3.5 | 2.6 | ||
| Mollard RC (3) (2014) [35] | Energy (kcal) | 300 | 300 | |
| Available carbohydrates (g) | 47.8 | 64.0 | ||
| Protein (g) | 16.1 | 9.9 | ||
| Fiber (g) | 11.3 | 2.8 | ||
| Fat (g) | 4.9 | 0.5 | ||
| Winham DM (2017) [36] | Energy (kcal) | 258.0 | 232.0 | |
| Carbohydrates (g) | 53.1 | 49.5 | ||
| Available CHO (g) | 47.6 | 49.5 | ||
| Fiber (g) | 5.5 | 0.7 | ||
| Protein (g) | 9.2 | 4.8 | ||
| Fat (g) | 2.3 | 0.5 | ||
| Zurbau A (2019) [40] | Potato | Pasta | ||
| GI | 28 | 85 | 45 | |
| GL | 14 | 42 | 42 | |
| Energy (kcal) | 418 | 423 | 462 | |
| Available CHO (g) | 50 | 50 | 94 | |
| Dietary fiber (g) | 20 | 6 | 5 | |
| Fat (g) | 14 | 15 | 2 | |
| Protein (g) | 23 | 22 | 17 | |
| Na (g) | 1.18 | 1.18 | 1.18 | |
| Alie J. Johnston (2020) [41] | Energy (kcal) | 202.0 | 200.0 | |
| Available CHO (%db) | 77.2 | 94.7 | ||
| Protein (%db) | 12.7 | 5.2 | ||
| Resistant starch (%db) | 0.2 | 0.2 | ||
| Insoluble dietary fiber (%db) | 5.5 | 2.3 | ||
| Soluble dietary fiber (%db) | 2.0 | 0.6 | ||
| Starch damage (%db) | 61.8 | 73.3 | ||
| Fat (%db) | 3.4 | 1.4 | ||
| Hafiz MS (2022) [42] | Weight (g) | 250.0 | 425.0 | |
| CHO (g) | 50.0 | 50.0 | ||
| Fiber (g) | 15.3 | 4.7 | ||
| Fat (g) | 8.0 | 8.0 | ||
| Protein (g) | 19.3 | 6.2 | ||
| Salt (g) | 0.8 | 0.8 | ||
| Energy (kJ) | 1447.6 | 1241.9 | ||
| Bajka BH (2023) [43] | Energy (kJ/serving) | 1823.1 | 1301.8 | |
| Protein (g/serving) | 27.16 | 12.88 | ||
| Fat (g/serving) | 8.84 | 3.33 | ||
| Starch (g/serving) | 42.5 | 45.3 | ||
| Available CHO (g/serving) | 48.2 | 48.1 | ||
| Available dietary fiber (g/serving) | 10.65 | 2.64 | ||
| Available sodium (g/serving) | 0.752 | 0.419 | ||
| Study ID | Nation | Study Design | Period | Sample Size (F/M) | Experimental Group | Control Group | Outcome Measurement | Assessment |
|---|---|---|---|---|---|---|---|---|
| Nestel P (2004) [34] | Australia | Crossover RCT | 6 weeks | 19 (12/7) middle-aged people | Chickpea-based diet | Wheat-based diet | Blood glucose | Positive |
| Johnson SK (2005) [37] | Australia | Crossover RCT | 1 week | 11 (2/9) healthy people | Chickpea flour bread | Wheat bread (White bread) | (1) IAUC glucose (2) IAUC insulin | Positive |
| Mollard RC (1) (2011) [38] | Canada | Crossover RCT | 5 weeks | 25 (0/25) healthy males | Chickpeas * | Pasta and sauce * | Blood glucose iAUC | Positive |
| Mollard RC (2) (2012) [39] | Canada | Crossover RCT | 4 weeks | 24 (0/25) healthy males | Macaroni and chickpeas * | Macaroni and cheese * | Blood glucose iAUC | Positive |
| Mollard RC (3) (2014) [35] | Canada | Crossover RCT | 5 weeks | 15 (0/15) healthy males | Chickpeas * | Wheat bread * (White bread) | Blood glucose iAUC | Positive |
| Winham DM (2017) [36] | USA | Crossover RCT | 3 weeks | 12 (12/0) healthy females | Chickpeas and white rice | Rice only | (1) Glucose iAUC (2) Insulin iAUC | Positive: (1) NSD: (2) |
| Zurbau A (2019) [40] | Canada | Crossover RCT | Over 12 days | 17 (9/8) healthy adults | Chickpeas ** | Potato ** | Blood glucose iAUC | Positive |
| Pasta | Blood glucose iAUC | Positive | ||||||
| Alie J. Johnston (2020) [41] | Canada | Crossover RCT | 5 days | 26 (12/14) normoglycemic adults | Chickpeas | Corn | Plasma glucose iAUC Insulin iAUC | Positive |
| Hafiz MS (2022) [42] | UK | Crossover RCT | 2 weeks | 13 (9/4) normoglycemic adults | Whole chickpeas | Mashed potatoes | Blood glucose iAUC | Positive |
| Bajka BH (2023) [43] | UK | Crossover RCT | Over 12 days | 20 (10/10) healthyindividuals | 60% CCP and 40% wheat flour *** | 100% wheat flour *** | (1) Plasma glucose iAUC (2) Insulin iAUC | Positive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, T.; Kim, A.; Oh, Y. Effectiveness of Chickpeas on Blood Sugar: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2023, 15, 4556. https://doi.org/10.3390/nu15214556
Nam T, Kim A, Oh Y. Effectiveness of Chickpeas on Blood Sugar: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2023; 15(21):4556. https://doi.org/10.3390/nu15214556
Chicago/Turabian StyleNam, Taegwang, Anna Kim, and Yongtaek Oh. 2023. "Effectiveness of Chickpeas on Blood Sugar: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 15, no. 21: 4556. https://doi.org/10.3390/nu15214556
APA StyleNam, T., Kim, A., & Oh, Y. (2023). Effectiveness of Chickpeas on Blood Sugar: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 15(21), 4556. https://doi.org/10.3390/nu15214556