

Effectiveness of Technology-Enabled, Low Carbohydrate Dietary Interventions, in the Prevention or Treatment of Type 2 Diabetes Mellitus in Adults: A Systematic Literature Review of Randomised Controlled and Non-Randomised Trials


Abstract
:1. Introduction
Objective
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Information Sources
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Risk of Bias and Quality Assessment in Individual Studies
2.6. Summary Measures
2.7. Data Synthesis
2.8. Meta-Bias/Risk of Bias across Studies
3. Results
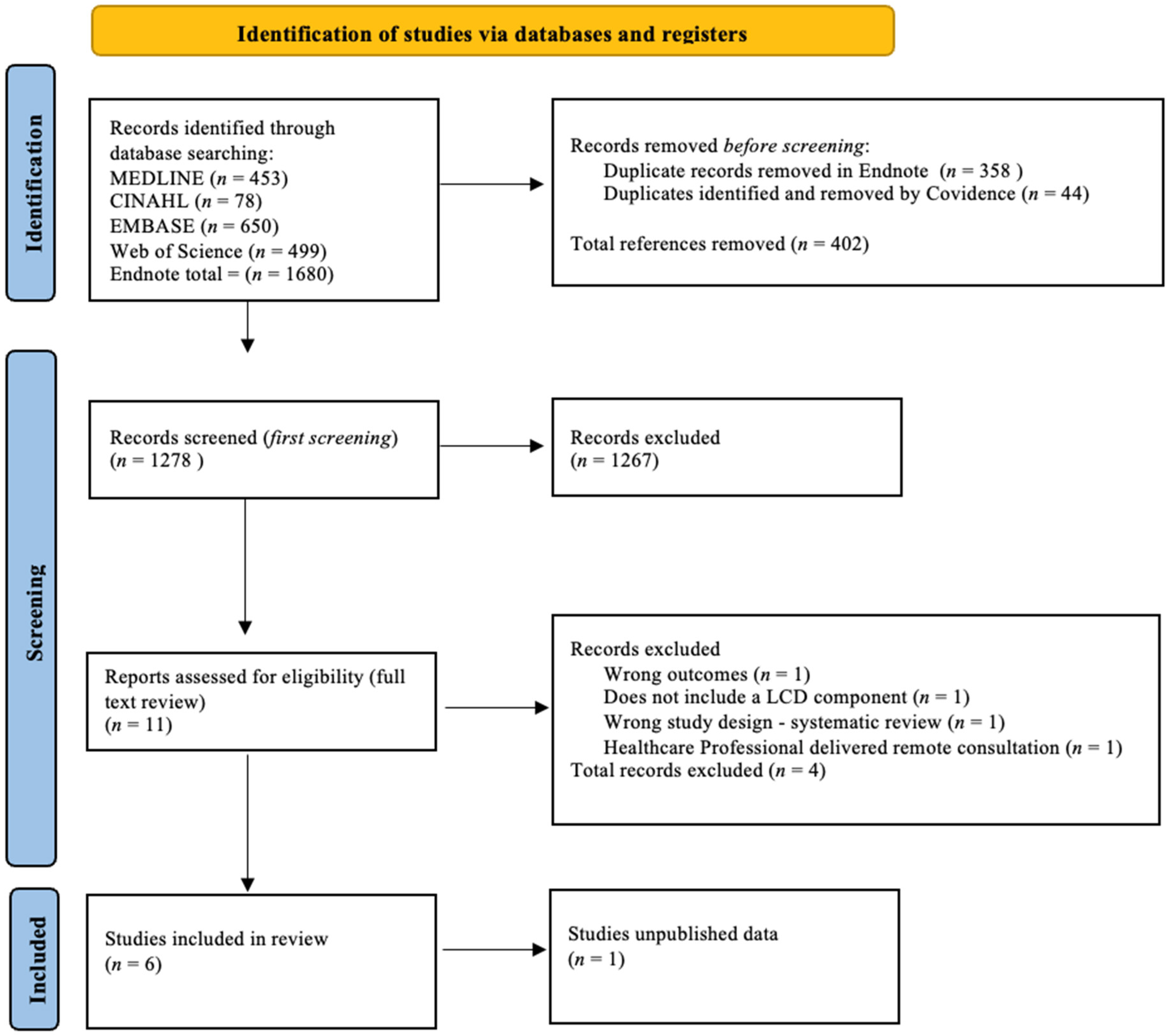
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Recruitment, Sample Size and Follow-Up Period
3.2.2. Characteristics of Interventions
3.2.3. Carbohydrate Recommendations
3.2.4. Comparator Interventions
3.3. Risk of Bias
3.3.1. Risk of Bias in Included RCTs
3.3.2. Risk of Bias in Included Non-RCTs
3.4. Results of Individual Studies
3.4.1. Summary Measures
3.4.2. LCD and VLCD Effectiveness on HbA1c
3.4.3. LCD and VLCD Effectiveness on Body Weight
3.4.4. LCD and VLCD Effectiveness on Body Mass Index
3.4.5. LCD and VLCD Effectiveness on T2DM Remission
3.4.6. Retention and Engagement
3.4.7. Outcome Reporting
4. Discussion
4.1. Key Findings and Interpretation
4.2. Limitations and Strengths
4.2.1. Limitations
4.2.2. Strengths
4.3. Implications and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of type 2 diabetes mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Hearts D: Diagnosis and Management of Type 2 Diabetes. Available online: https://www.who.int/publications/i/item/who-ucn-ncd-20.1 (accessed on 6 March 2023).
- Centers for Disease Control and Prevention. Diabetes Tests. Available online: https://www.cdc.gov/diabetes/basics/getting-tested.html (accessed on 3 March 2023).
- World Health Organisation. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 6 March 2023).
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Wu, T.; Zhang, M.; Li, C.; Liu, Q.; Li, F. Prevalence, awareness and control of type 2 diabetes mellitus and risk factors in Chinese elderly population. BMC Public Health 2022, 22, 1382. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas. Diabetes around the World in 2021. Key Global Findings. 2021. Available online: https://www.diabetesatlas.org (accessed on 9 April 2023).
- Australian Institute of Health and Welfare. Diabetes Risk Factors. Available online: https://www.aihw.gov.au/reports/diabetes/diabetes/contents/risk-factors (accessed on 16 March 2023).
- Centers for Disease Control and Prevention. Gestational Diabetes. Available online: https://www.cdc.gov/diabetes/basics/gestational.html (accessed on 3 March 2023).
- Hruby, A.; Manson, J.E.; Qi, L.; Malik, V.S.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Hu, F.B. Determinants and consequences of obesity. Am. J. Public Health 2016, 106, 1656–1662. [Google Scholar] [CrossRef] [PubMed]
- Leitner, D.R.; Frühbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and type 2 diabetes: Two diseases with a need for combined treatment strategies-EASO can lead the way. Obes. Facts 2017, 10, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Summers, C.; Tobin, S.; Unwin, D. Evaluation of the Low Carb Program Digital Intervention for the Self-Management of Type 2 Diabetes and Prediabetes in an NHS England General Practice: Single-Arm Prospective Study. JMIR Diabetes 2021, 6, e25751. [Google Scholar] [CrossRef]
- Hyde, P.N.; Sapper, T.N.; Crabtree, C.D.; LaFountain, R.A.; Bowling, M.L.; Buga, A.; Fell, B.; McSwiney, F.T.; Dickerson, R.M.; Miller, V.J.; et al. Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight 2019, 4, e128308. [Google Scholar] [CrossRef]
- O’Neill, B.J. Effect of low-carbohydrate diets on cardiometabolic risk, insulin resistance, and metabolic syndrome. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 301–307. [Google Scholar] [CrossRef]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The effects of type 2 diabetes mellitus on organ metabolism and the immune system. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef]
- Chen, X.Y.; Su, H.H.; Kunii, D.; Kudou, K.; Zhang, Y.Y.; Zhao, Y.; Zhang, D.; Xing, Y.Y.; Teng, J.Q.; Nie, Z.Q.; et al. The Effects of Mobile-App-Based Low-Carbohydrate Dietary Guidance on Postprandial Hyperglycemia in Adults with Prediabetes. Diabetes Ther. 2020, 11, 2341–2355. [Google Scholar] [CrossRef] [PubMed]
- Höchsmann, C.; Infanger, D.; Klenk, C.; Königstein, K.; Walz, S.P.; Schmidt-Trucksäss, A. Effectiveness of a behavior change technique–based smartphone game to improve intrinsic motivation and physical activity adherence in patients with type 2 diabetes: Randomized controlled trial. JMIR Serious Games 2019, 7, e11444. [Google Scholar] [CrossRef] [PubMed]
- Jansson, A.K.; Chan, L.X.; Lubans, D.R.; Duncan, M.J.; Plotnikoff, R.C. Effect of resistance training on HbA1c in adults with type 2 diabetes mellitus and the moderating effect of changes in muscular strength: A systematic review and meta-analysis. BMJ Open Diabetes Res. Care 2022, 10, e002595. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Physical Inactivity. Harmful Effects of Not Getting Enough Physical Activity. Available online: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/physical-activity.htm (accessed on 3 March 2023).
- Diabetes Australia. Type 2 Diabetes Remission. Position Statement. Available online: https://www.diabetesaustralia.com.au/wp-content/uploads/2021_Diabetes-Australia-Position-Statement_Type-2-diabetes-remission_2.pdf (accessed on 3 March 2023).
- Lean, M.E.J.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Feinman, R.D.; Pogozelski, W.K.; Astrup, A.; Bernstein, R.K.; Fine, E.J.; Westman, E.C.; Accurso, A.; Frassetto, L.; Gower, B.A.; McFarlane, S.I.; et al. Dietary carbohydrate restriction as the first approach in diabetes management: Critical review and evidence base. Nutrition 2015, 31, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sato, J.; Kanazawa, A.; Makita, S.; Hatae, C.; Komiya, K.; Shimizu, T.; Ikeda, F.; Tamura, Y.; Ogihara, T.; Mita, T.; et al. A randomized controlled trial of 130 g/day low-carbohydrate diet in type 2 diabetes with poor glycemic control. Clin. Nutr. 2017, 36, 992–1000. [Google Scholar] [CrossRef]
- Dorans, K.S.; Bazzano, L.A.; Qi, L.; He, H.; Chen, J.; Appel, L.J.; Chen, C.S.; Hsieh, M.H.; Hu, F.B.; Mills, K.T.; et al. Effects of a Low-Carbohydrate Dietary Intervention on Hemoglobin A1c: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2238645. [Google Scholar] [CrossRef] [PubMed]
- Unwin, D.; Delon, C.; Unwin, J.; Tobin, S.; Taylor, R. What predicts drug-free type 2 diabetes remission? Insights from an 8-year general practice service evaluation of a lower carbohydrate diet with weight loss. BMJ Nutr. Prev. Health 2023, 2023, e000544. [Google Scholar] [CrossRef]
- Goldenberg, J.Z.; Day, A.; Brinkworth, G.D.; Sato, J.; Yamada, S.; Jönsson, T.; Beardsley, J.; Johnson, J.A.; Thabane, L.; Johnston, B.C. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: Systematic review and meta-analysis of published and unpublished randomized trial data. BMJ 2021, 372, m4743. [Google Scholar] [CrossRef]
- Moschonis, G.; Siopis, G.; Jung, J.; Eweka, E.; Willems, R.; Kwasnicka, D.; Asare, B.Y.-A.; Kodithuwakku, V.; Vedanthan, R.; Annemans, L.; et al. Effectiveness, reach, uptake, and feasibility of digital health interventions for adults with type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials. Lancet Digit. Health 2023, 5, e125–e143. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Freeman, V.S. Glucose and Hemoglobin A1c. Lab. Med. 2014, 45, e21–e24. [Google Scholar] [CrossRef]
- Dicianno, B.E.; Parmanto, B.; Fairman, A.D.; Crytzer, T.M.; Yu, D.X.; Pramana, G.; Coughenour, D.; Petrazzi, A.A. Perspectives on the evolution of mobile (mHealth) technologies and application to rehabilitation. Phys. Ther. 2015, 95, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Dening, J.; George, E.S.; Ball, K.; Mohebbi, M.; Shariful Islam, S.M. Randomised controlled trial of a web-based low carbohydrate diet intervention for adults with type 2 diabetes: The T2Diet study protocol. BMJ Open 2022, 12, e054594. [Google Scholar] [CrossRef] [PubMed]
- The Endnote Team. Endnote, version 20; Clarivate Analytics: London, UK, 2020.
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240. [Google Scholar] [CrossRef] [PubMed]
- Covidence Covidence for Systematic Reviews; Veritas Health Innovation: Melbourne, VIC, Australia, 2020.
- Higgins, J.P.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: London, UK, 2023; Available online: www.training.cochrane.org/handbook (accessed on 3 March 2023).
- Academy of Nutrition and Dietetics. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. Available online: https://www.andeal.org/vault/2440/web/files/2016_April_EA_Manual.pdf (accessed on 20 April 2023).
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.; Del Mar, C.; Bennett, S. Evidence-Based Practice across the Health Professions, 2nd ed.; Elsevier: Chatswood, NSW, Australia, 2013. [Google Scholar]
- Athinarayanan, S.J.; Adams, R.N.; Hallberg, S.J.; McKenzie, A.L.; Bhanpuri, N.H.; Campbell, W.W.; Volek, J.S.; Phinney, S.D.; McCarter, J.P. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-randomized Clinical Trial. Front. Endocrinol. 2019, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, S.J.; McKenzie, A.L.; Williams, P.T.; Bhanpuri, N.H.; Peters, A.L.; Campbell, W.W.; Hazbun, T.L.; Volk, B.M.; McCarter, J.P.; Phinney, S.D.; et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018, 9, 583–612. [Google Scholar] [CrossRef]
- Saslow, L.R.; Mason, A.E.; Kim, S.; Goldman, V.; Ploutz-Snyder, R.; Bayandorian, H.; Daubenmier, J.; Hecht, F.M.; Moskowitz, J.T. An Online Intervention Comparing a Very Low-Carbohydrate Ketogenic Diet and Lifestyle Recommendations versus a Plate Method Diet in Overweight Individuals with Type 2 Diabetes: A Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, 16. [Google Scholar] [CrossRef]
- Saslow, L.R.; Summers, C.; Aikens, J.E.; Unwin, D.J. Outcomes of a Digitally Delivered Low-Carbohydrate Type 2 Diabetes Self-Management Program: 1-Year Results of a Single-Arm Longitudinal Study. JMIR Diabetes 2018, 3, e12. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Chaimani, A.; Hoffmann, G.; Schwedhelm, C.; Boeing, H. A network meta-analysis on the comparative efficacy of different dietary approaches on glycaemic control in patients with type 2 diabetes mellitus. Eur. J. Epidemiol. 2018, 33, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, E.; Kizirian, N.V.; Partridge, S.R.; Gill, T.; Colagiuri, S.; Gibson, A.A. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 139, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Snorgaard, O.; Poulsen, G.M.; Andersen, H.K.; Astrup, A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000354. [Google Scholar] [CrossRef] [PubMed]
- Van Zuuren, E.J.; Fedorowicz, Z.; Kuijpers, T.; Pijl, H. Effects of low-carbohydrate- compared with low-fat-diet interventions on metabolic control in people with type 2 diabetes: A systematic review including GRADE assessments. Am. J. Clin. Nutr. 2018, 108, 300–331. [Google Scholar] [CrossRef] [PubMed]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.W.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Huntriss, R.; Campbell, M.; Bedwell, C. The interpretation and effect of a low-carbohydrate diet in the management of type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Clin. Nutr. 2018, 72, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Apovian, C.M.; Okemah, J.; O’Neil, P.M. Body weight considerations in the management of type 2 diabetes. Adv. Ther. 2019, 36, 44–58. [Google Scholar] [CrossRef]
- Chopra, S. Effective primary care management of type 2 diabetes for indigenous populations: A systematic review. PLoS ONE 2022, 17, e0276396. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National Aboriginal and Torres Strait Islander Health Survey. 2018–2019. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/national-aboriginal-and-torres-strait-islander-health-survey/latest-release#diabetes (accessed on 4 March 2023).
- National Health and Medical Research Council. NHMRC. Levels of Evidence and Grades for Recommendations for Developers of Guidelines. Available online: https://www.mja.com.au/sites/default/files/NHMRC.levels.of.evidence.2008-09.pdf (accessed on 28 March 2023).


{kind=link}
| Prediabetes [3] | T2DM [2] | |
|---|---|---|
| Fasting Blood Glucose (FBG) | 6–6.9 mmol/L (100–125 mg/dL) | >7 mmol/L (126 mg/dL) |
| HbA1c | 5.7−6.4% (39–46 mmol/mol) | >6.5% (48 mmol/mol) |
| Oral glucose tolerance test (2-h plasma glucose) | 7.8–11.0 mmol/L (140–199 mg/dL) | >11.1 mmol/L (200 mg/dL) |
| Author, Year, Study Design, Location | Sample Size N | Population Characteristics | Participants, N, Program Name Characteristics of Digital Intervention | Type of Diets Prescribed Intervention/Control | Primary Outcomes | Intervention/Follow-Up Period | Retention, Adherence | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Saslow et al. (2017) Pilot RCT a Parallel-group, USA [42] | 25 | Overweight adults (>18) with T2DM b, mean age 53.0 (IG c), 58.2 (CG d) years Patients receiving insulin (except for metformin) excluded | IG c—N = 12, dietary instruction provided via weekly email lessons with lifestyle recommendations and mindfulness training CG d—N = 13 dietary instructions provided via weekly emailed lessons. No lifestyle recommendations or mindfulness training included | IG c: VLCD e ad libitum. (20–50 g/carbs per day), to induce nutritional ketosis CG d: ADA f “create your plate” plan from the American Diabetic Association (low-fat diet) | HbA1c change | 16-week intervention, 32-week follow-up | 92% retention Drop out: IG c: 8% (1/12) CG d: 46% (6/13) | Positive No Blinding Self-report dietary intake |
| Chen et al. (2020) Pilot RCT a Single blinded China [17] | 100 | Adults (30–80 years) with prediabetes, mean age 54.9 (IG c), 51.9 (CG d) years. Patients taking medication excluded | IG c N = 57 Health management support service system. Mobile app (CAReNA). Receive LCD g dietary guidance CG d—N = 43 Received early education in diabetes diet management | IG c: LCD g (70–130 g/carbs per day). CG d: Diabetes diet education. No LCD g intervention. | HbA1c change | 3 months | - | Positive |
| Author, Year, Study Design, Location | Sample Size N | Population Characteristics | Participants, N, Program Name, Characteristics of Digital Intervention | Type of Diets Prescribed Intervention/Control | Primary Outcomes | Intervention/Follow-Up Period | Retention Adherence | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Hallberg et al. (2018) Open-label, non-RCT a before-and-after study USA [41] | N = 349 | Adults (21–65 years) with T2DM b, mean age 53.7 years (CCI e) Participants taking any diabetes medication included | N = 262 (CCI e) IG c: Virta Health, digitally delivered via the Virta app. CG d: (N = 87) Usual diabetes care education by a dietitian | IG c: VLCD f (<30 g/carbs per day) to induce nutritional ketosis CG d: Usual diabetes diet (low fat) | HbA1c, body weight and medication use change | 12 months | 83% retention 25% remission | Positive selection bias; conflict of interest |
| Athinarayanan et al. (2019) Open-label non- RCT a before-and-after study USA [40] | N = 349 | Adults (21–65 years) with T2DM b, mean age 53.8 years (CCI e) Participants taking any diabetes medication included | N = 262 (CCI e) IG c: Virta Health Digitally delivered via Virta app. CG d: (N = 87) Usual diabetes care education by a dietitian | IG c: VLCD f (<30 g/carbs per day) to induce nutritional ketosis CG d: Usual diabetes diet (low fat) | HbA1c, body weight changes and retention | 24 months | 74% retention 17.6% remission | Positive selection bias; conflict of interest |
| Summers et al. (2021) Single arm pre-post prospective real-world study/intervention UK [13] | N = 45 | Obese adults (>18) with T2DM b or prediabetes, mean age 54.8 years Participants taking any diabetes medication included | N = 45 The Low Carb Program—12 weeks digitally delivered. Included behavioural change techniques | LCD g—(<130 g/carbs per day) based on visual plate representation | HbA1c and body weight change | 12 months | 82% retention | Neutral; no comparison; self-reporting outcome data; funding unclear |
| Saslow et al. (2018) Open-label single-arm, pre-post intervention USA [43] | N = 1000 | Adults (>18) with T2DM b, mean age 56.1 years. Participants taking any diabetes medication included | N = 1000 The Low Carb Program—10-week digitally delivered. Included behavioural change techniques | LCD g—(<130 g/carbs per day) based on visual plate representation | HbA1c and body weight change | 12 months | 71% retention 26% remission | Neutral; no comparison; self-reporting outcome data |
| Saslow et al. (2017) [42] | Chen et al. (2020) [17] | Hallberg et al. (2108) [41] | Athinarayanan et al. (2109) [40] | Saslow et al. (2108) [43] | Summers et al. (2021) [13] | ||
|---|---|---|---|---|---|---|---|
| Overall rating |  | | | |  | | |
| Relevance Questions | |||||||
| 1 | Would implementing the studied intervention or procedure (if found successful) result in improved outcomes for the patients/clients/population group? (NA for some Epi studies) |  | | | | | |
| 2 | Did the authors study an outcome (dependent variable) or topic that the patients/clients/population group would care about? | | | | | | |
| 3 | Is the focus of the intervention or procedure (independent variable) or topic of study a common issue of concern to dietetics practice? | | | | | | |
| 4 | Is the intervention or procedure feasible? (NA for some epidemiological studies) | | | | | | |
| Validity Questions | |||||||
| 1 | Was the research question clearly stated? | | | | | | |
| 2 | Was the selection of study subjects/patients free from bias? | | | | | | |
| 3 | Were study groups comparable? | | | | |  | |
| 4 | Was method of handling withdrawals described? | | | | | | |
| 5 | Was blinding used to prevent introduction of bias? |  | | | | | |
| 6 | Were intervention/therapeutic regimens/exposure factor or procedure and any comparison(s) described in detail? Were intervening factors described? | | | | | | |
| 7 | Were outcomes clearly defined and the measurements valid and reliable? | | | | | | |
| 8 | Was the statistical analysis appropriate for the study design and type of outcome indicators? | | | | | | |
| 9 | Are conclusions supported by results with biases and limitations taken into consideration? | | | | | | |
| 10 | Is bias due to study’s funding or sponsorship unlikely? | | |  | | | |
Overall positive Risk of Bias Score; If most of the answers to the above validity question are “Yes” (including criteria 2, 3, 6, 7 and at least one additional “Yes”). Neutral Risk of Bias Score; If the answers to the validity criteria question 2, 3, 6 and 7 do not indicate that the study is exceptionally strong. Negative Risk of Bias Score; If most (six or more) of the answers to the above validity question are “No”. Yes, No, Unclear, Not applicable.| Author/Date/Reported Mean and Outcomes Measure | Baseline | Interim Follow-Up | Final Follow-Up | Within Group Change (p Value) | Between-Group Difference at Final Follow-Up (p Value) |
|---|---|---|---|---|---|
| Saslow et al. (2017) mean (SD b) and mean EMM c (95% CI) [42] | |||||
| HbA1c a (%) | 7.1 (0.4) | 16 weeks = 6.2 (−1.1, −0.6) | 32 weeks = 6.3 (−1.1, −0.6) | −0.8 (−1.1, −0.6) | −0.5 (−0.8, −0.2) 0.002 |
| Weight (kg) | 109.7 (24.9) | 16 weeks = 101.4 (−11.9, −5.2) | 32 weeks = 96.3 (−7.3, 1.3) | −12.7 (−16.1 to −9.2) | −9.6 (−14.0, −5.3) <0.001 |
| Remission (%) | - | - | 32 weeks = 55% | - | - |
| Chen et al. (2020) mean (SD), (95% CI e) [17] | |||||
| HbA1c (%) | 6.00 (0.39) | - | 12 weeks = 5.77 (0.34) | <0.001 | −0.10 (95% CI e, 0.22, −0.03) 0.120 |
| Weight (kg) | 67.8 (11.7) | - | 12 weeks = 65.6 (11.7) | <0.001 | −1.4 (95% CI e 2.2, −0.6) <0.001 |
| BMI d (kg/m2) | 25.5 (2.9) | - | 12 weeks = 24.8 (2.9) | <0.001 | −0.5 (95% CI e 0.9, −0.2) 0.006 |
| Author/Date/Reported Mean and Outcomes Measure | Baseline | Interim Follow-Up | Final Follow-Up | Within Group Change Mean Change (SD) (p Value) |
|---|---|---|---|---|
| Hallberg et al. (2018) mean (SD) [41] | ||||
| HbA1c a (%) Completers (n = 204) | 7.5 (1.4) | - | 1-year = 6.20 (0.9) | −1.3 (1.3) <10−16 |
| Weight (kg), mean (SD) Completers (n = 184) | 115.4 (24.6) | - | 1-year = 101.2 (22.06) | −14.2 (10.3) <10−16 |
| Remission | 1-year = 25% | |||
| Athinarayanan et al. (2019) mean (SD) [40] | ||||
| HbA1c a (%) | 7.6 (1.5) | 1-year = 6.2 (0.9) | 2-years = 6.6 (1.3) | −0.9 (±0.1) 0.01 |
| Weight (kg) | 116.5 (25.9) | 1-year = 101.1 (22.2) | 2-years = 102.5 (25.2) | −11.9 ± 0.9 4.6 × 10−26 |
| Remission (%) | - | - | 2-years = 17.6% | - |
| Summers et al. (2021) mean (SD) [13] | ||||
| HbA1c a | 7.5 (1.65) | - | 1-year = 7.1 (1.44) | −0.4% <0.001 |
| Weight (kg) Completers (>9 modules) | 91.5 (15.1) | - | 1-year = 87.7 (14.5) | −3.8 (2.4) <0.001 |
| Saslow et al. (2018) mean (SD) [43] | ||||
| HbA1c a (%) Completers (n = 528) | 7.4 (1.8) | - | 1-year = 6.2 (1.2) | −1.2 (1.4) <0.001 |
| Weight (kg), Completers (n = 528) | 88.8 (22.2) | - | 1-year = 81.4 (17.9) | −7.5 (12.6) <0.001 |
| Remission | - | - | 1-year = 26.2% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jooste, B.R.; Kolivas, D.; Brukner, P.; Moschonis, G. Effectiveness of Technology-Enabled, Low Carbohydrate Dietary Interventions, in the Prevention or Treatment of Type 2 Diabetes Mellitus in Adults: A Systematic Literature Review of Randomised Controlled and Non-Randomised Trials. Nutrients 2023, 15, 4362. https://doi.org/10.3390/nu15204362
Jooste BR, Kolivas D, Brukner P, Moschonis G. Effectiveness of Technology-Enabled, Low Carbohydrate Dietary Interventions, in the Prevention or Treatment of Type 2 Diabetes Mellitus in Adults: A Systematic Literature Review of Randomised Controlled and Non-Randomised Trials. Nutrients. 2023; 15(20):4362. https://doi.org/10.3390/nu15204362
Chicago/Turabian StyleJooste, Bernice Rozemai, Despina Kolivas, Peter Brukner, and George Moschonis. 2023. "Effectiveness of Technology-Enabled, Low Carbohydrate Dietary Interventions, in the Prevention or Treatment of Type 2 Diabetes Mellitus in Adults: A Systematic Literature Review of Randomised Controlled and Non-Randomised Trials" Nutrients 15, no. 20: 4362. https://doi.org/10.3390/nu15204362
APA StyleJooste, B. R., Kolivas, D., Brukner, P., & Moschonis, G. (2023). Effectiveness of Technology-Enabled, Low Carbohydrate Dietary Interventions, in the Prevention or Treatment of Type 2 Diabetes Mellitus in Adults: A Systematic Literature Review of Randomised Controlled and Non-Randomised Trials. Nutrients, 15(20), 4362. https://doi.org/10.3390/nu15204362