
Association between Serum 25-Hydroxyvitamin D Concentrations and Academic Performance among Adolescent Schoolchildren: A Cross-Sectional Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
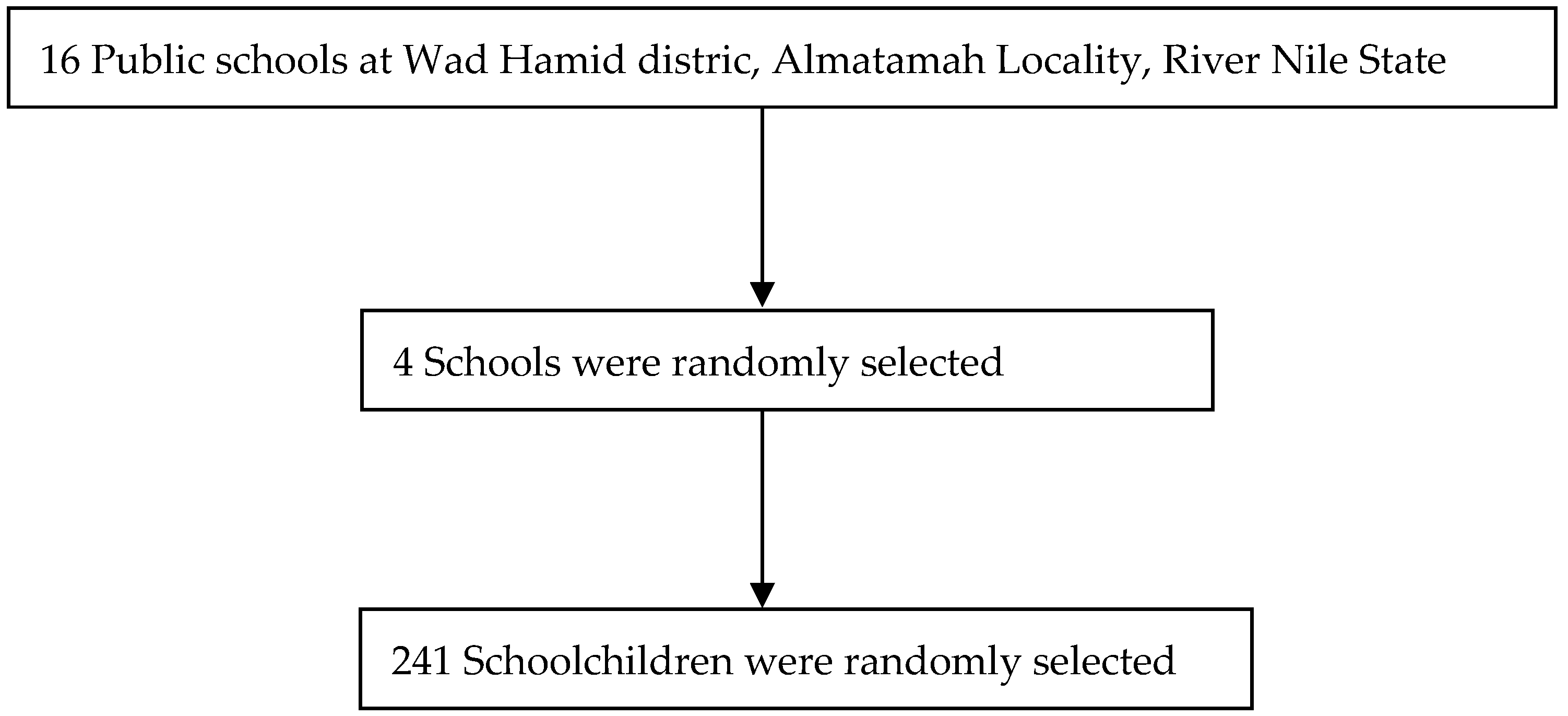
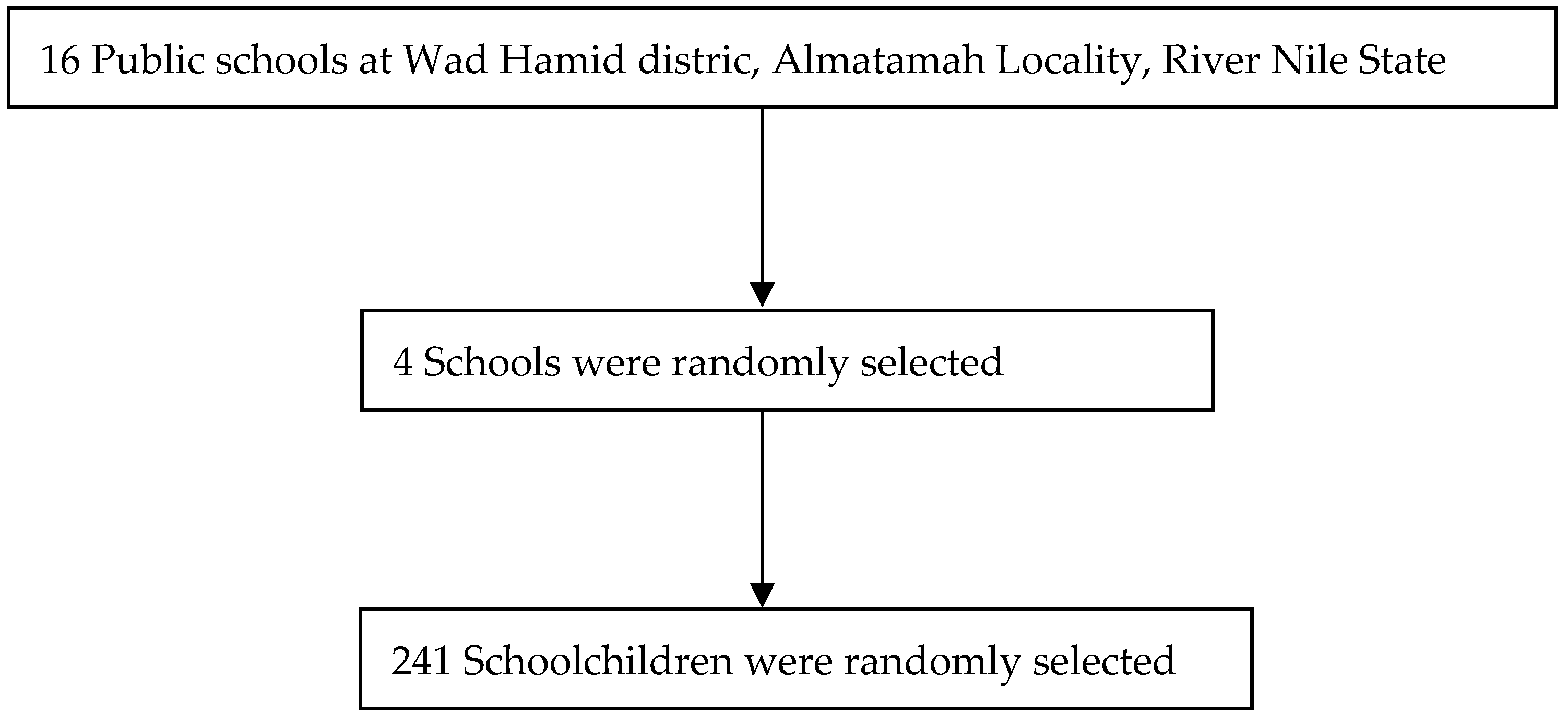
2.1. Study Area
2.2. Study Population and Design
2.3. The Inclusion and Exclusion Criteria
2.4. Procedures
2.5. Processing of Blood Samples
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. General Characteristics
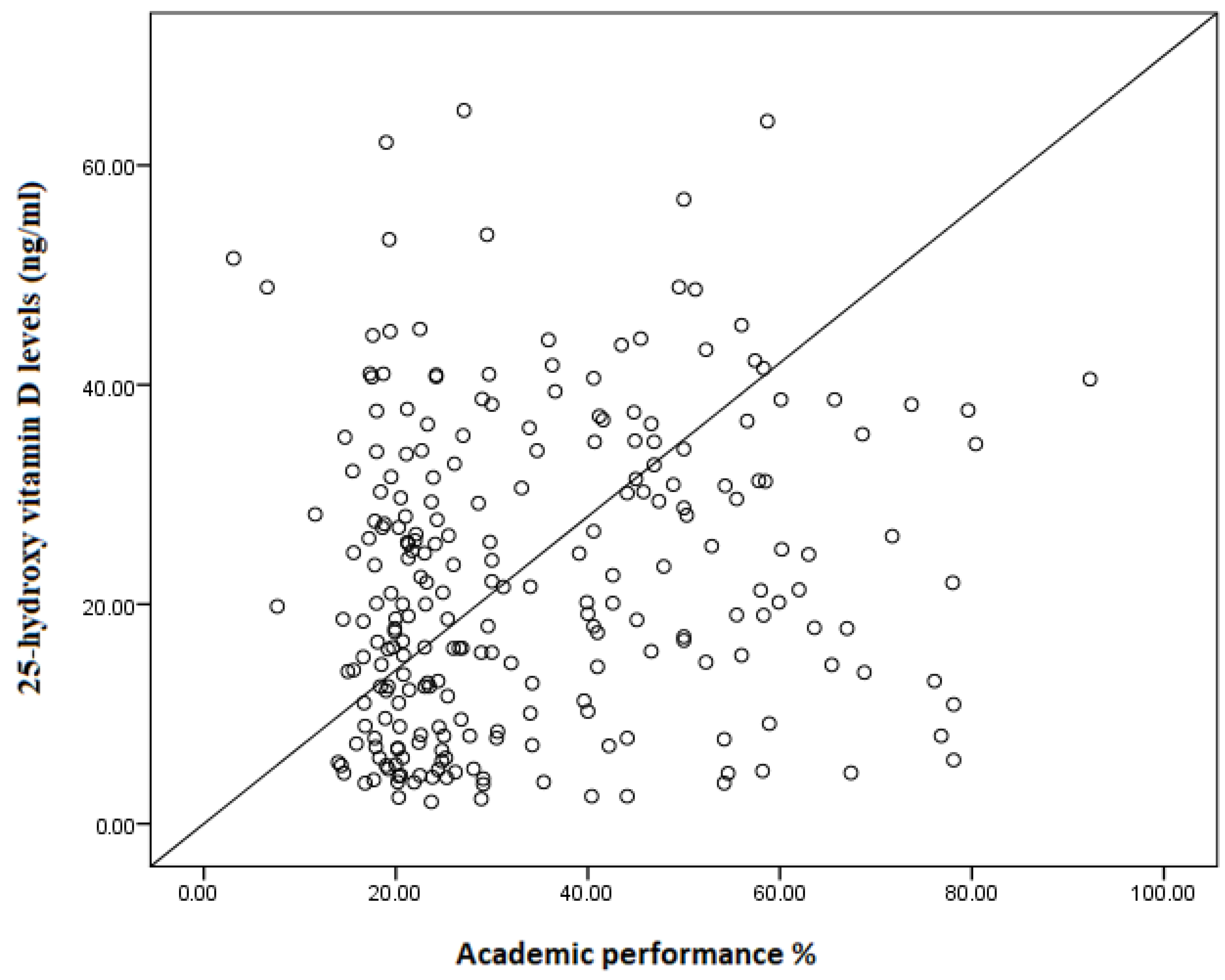
3.2. Factors Associated with Academic Performance in %
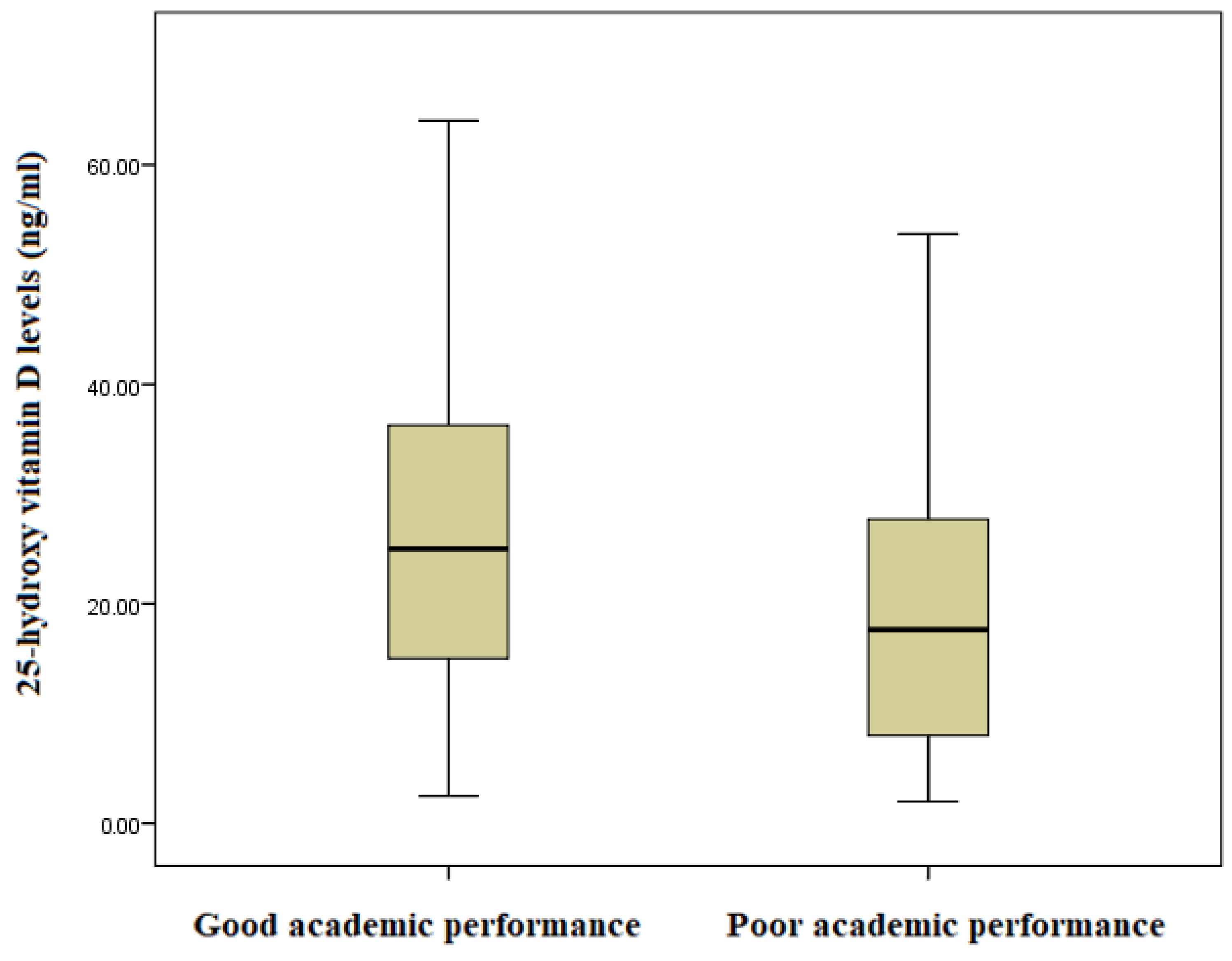
3.3. Factors Associated with Academic Performance (Good vs. Poor)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hale, D.R.; Viner, R.M. How adolescent health influences education and employment: Investigating longitudinal associations and mechanisms. J. Epidemiol. Community Health 2018, 72, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Raghupathi, V.; Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public Health 2020, 78, 20. [Google Scholar] [CrossRef] [PubMed]
- Wijsman, L.A.; Warrens, M.J.; Saab, N.; van Driel, J.H.; Westenberg, P.M. Declining trends in student performance in lower secondary education. Eur. J. Psychol. Educ. 2016, 31, 595–612. [Google Scholar] [CrossRef]
- United Nations. Children in Africa Five Times Less Likely to Learn Basics: New Report. Available online: https://news.un.org/en/story/2022/10/1129727#:~:text=The%20ability%20of%20education%20systems,likely%20to%20learn%20the%20basics (accessed on 22 May 2023).
- Moloko, L.; Mhlauli, M.B. An investigation on students academic performance for junior secondary schools in Botswana. Eur. J. Educ. Res. 2014, 3, 111–127. [Google Scholar] [CrossRef]
- Katiso, S.W.; Kerbo, A.A.; Dake, S.K. Adolescents’ nutritional status and its association with academic performance in South Ethiopia; a facility-based cross-sectional study. BMC Nutr. 2021, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Haile, D.; Nigatu, D.; Gashaw, K.; Demelash, H. Height for age z score and cognitive function are associated with academic performance among school children aged 8–11 years old. Arch. Public Health 2016, 74, 17. [Google Scholar] [CrossRef]
- Soleimani, N.; Abbaszadeh, N. Relationship between anaemia, caused from the iron deficiency, and academic achievement among third grade high school female students. Procedia-Soc. Behav. Sci. 2011, 29, 1877–1884. [Google Scholar] [CrossRef]
- Mosiño, A.; Villagómez-Estrada, K.P.; Prieto-Patrón, A. Association between school performance and anemia in adolescents in mexico. Int. J. Environ. Res. Public Health 2020, 17, 51466. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Walia, M.; Pant, A.; Menon, P.; Scott, S. Changes in anemia and anthropometry during adolescence predict learning outcomes: Findings from a 3-year longitudinal study in India. Am. J. Clin. Nutr. 2022, 115, 1549–1558. [Google Scholar] [CrossRef]
- Nair, A.B.; Devika, J. Prevalence of vitamin D deficiency in adolescents with recent onset poor Scholastic Performance. IMA Kerala Med. J. 2017, 10, 152–155. [Google Scholar]
- AlZahrani, W.I.; Oommen, A. Role of vitamin D in the academic performance of health sciences students in Saudi Arabia. Arab. Gulf J. Sci. Res. 2023, 41, 40–47. [Google Scholar] [CrossRef]
- Dell’isola, G.B.; Tulli, E.; Sica, R.; Vinti, V.; Mencaroni, E.; Di Cara, G.; Striano, P.; Verrotti, A. The vitamin d role in preventing primary headache in adult and pediatric population. J. Clin. Med. 2021, 10, 5983. [Google Scholar] [CrossRef] [PubMed]
- Almuqbil, M.; Almadani, M.E.; Albraiki, S.A.; Alamri, A.M.; Alshehri, A.; Alghamdi, A.; Alshehri, S.; Asdaq, S.M.B. Impact of Vitamin D Deficiency on Mental Health in University Students: A Cross-Sectional Study. Healthcare 2023, 11, 2097. [Google Scholar] [CrossRef] [PubMed]
- Prono, F.; Bernardi, K.; Ferri, R.; Bruni, O. The role of vitamin D in sleep disorders of children and adolescents: A systematic review. Int. J. Mol. Sci. 2022, 23, 31430. [Google Scholar] [CrossRef] [PubMed]
- Tuohimaa, P. Vitamin D, and chronic diseases. Vitam. D Oxidative Stress Immun. Aging 2012, 8, 385–406. [Google Scholar] [CrossRef]
- Rahman, A.; Al-Taiar, A.; Shaban, L.; Al-Sabah, R.; Al-Harbi, A.; Mojiminiyi, O. Plasma 25-hydroxy vitamin D is not associated with neither cognitive function nor academic performance in adolescents. Nutrients 2018, 10, 197. [Google Scholar] [CrossRef]
- United Nations Educational Scientific and Cultural Organization. Sudan Education Policy Review Paving the Road to 2030. 2018. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000265447 (accessed on 11 June 2023).
- Mogire, R.M.; Morovat, A.; Muriuki, J.M.; Mentzer, A.J.; Webb, E.L.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Cutland, C.L.; Sirima, S.B.; et al. Prevalence and predictors of vitamin D deficiency in young African children. BMC Med. 2021, 19, 115. [Google Scholar] [CrossRef]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.M.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of vitamin D deficiency in Africa: A systematic review and meta-analysis. Lancet Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef]
- Ahmed, A.; Burbur, A.; Babiker, S.; Mohamed, S.; ELseed, M.; Saad, F. Impact of type 1 diabetes mellitus on the academic performance of diabetic school children in Khartoum, Sudan. Sudan. J. Paediatr. 2021, 21, 123–130. [Google Scholar] [CrossRef]
- Zafar, M.; Omer, E.O.M.; Hassan, M.E.; Ansari, K.A. Association of sleep disorder with academic performance among medical students in Sudan. Russ. Open Med. J. 2020, 9, e0208. [Google Scholar] [CrossRef]
- Husain, N.E.; Suliman, A.A.B.; Abdelrahman, I.; Bedri, S.A.; Musa, R.M.; Osman, H.E.; Mustafa, A.H.; Gafer, N.; Farah, E.; Abdel Satir, A.; et al. Vitamin D level and its determinants among Sudanese women: Does it matter in a sunshine African country? J. Fam. Med. Prim. Care 2017, 6, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.E.; Mohammed, M.A. Vitamin D status of Sudanese children with sickle cell anemia. Glob. J. Med. Res. 2018, 18, 13–20. [Google Scholar]
- United Nations Children’s Fund. Sudan Education. 2019. Available online: https://open.unicef.org/sites/transparency/files/2020-06/Sudan-TP4-2018.pdf (accessed on 25 June 2023).
- 5th Sudan Population and Housing Census. 2008. Available online: https://microdata.worldbank.org/index.php/catalog/1014 (accessed on 26 June 2023).
- Bilal, J.A.; Osman, A.A.; Al-Nafeesah, A.; AlEed, A.; Adam, I. Prevalence and associated factors of stunting and thinness among adolescent Sudanese schoolchildren: A cross-sectional study. Trans. R. Soc. Trop. Med. Hyg. 2023, trad055. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Lapo Ordoñez, D.; Quintana Salinas, M. Relationship between nutritional status by anthropometry and eating habits with academic performance in adolescents. Rev. Arch. Med. Camaguey 2018, 22, 755–774. [Google Scholar]
- World Health Organization. Sudan Takes Action to Improve the Health of Its Youth—AA-HA! 2019. Available online: https://www.who.int/news/item/14-08-2019-sudan-takes-action-to-improve-the-health-of-its-youth-aa-ha! (accessed on 22 July 2023).
- BMI-For-Age (5–19 Years). Available online: https://www.who.int/toolkits/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 29 January 2023).
- Abdelrahman, E.G.; Gasim, G.I.; Musa, I.R.; Elbashir, L.M.; Adam, I. Red blood cell distribution width and iron deficiency anemia among pregnant Sudanese women. Diagn. Pathol. 2012, 7, 168. [Google Scholar] [CrossRef] [PubMed]
- Hassan, A.A.; Abdelbagi, O.; Osman, O.E.; Adam, I. Association between serum 25-hydroxyvitamin D concentrations and hypertension among adults in North Sudan: A community-based cross-sectional study. BMC Cardiovasc. Disord. 2023, 23, 402. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Vitamin and Mineral Nutrition Information System. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Available online: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?ua=1 (accessed on 2 September 2023).
- International Osteoporosis Foundation. Vitamin D. 2023. Available online: https://www.osteoporosis.foundation/health-professionals/prevention/nutrition/vitamin-d (accessed on 25 July 2023).
- Voortman, T.; Van den Hooven, E.H.; Heijboer, A.C.; Hofman, A.; Jaddoe, V.W.V.; Franco, O.H. Vitamin D deficiency in school-age children is associated with sociodemographic and lifestyle factors. J. Nutr. 2015, 145, 791–798. [Google Scholar] [CrossRef]
- Alyahya, K.O. Vitamin D levels in schoolchildren: A cross-sectional study in Kuwait. BMC Pediatr. 2017, 17, 213. [Google Scholar] [CrossRef]
- Bujang, M.A.; Baharum, N.; Mara, T.; Alam, S. Sample size guideline for correlation analysis. World J. Soc. Sci. Res. 2016, 3. [Google Scholar] [CrossRef]
- Hernandez, J. The Missing Vitamin in Humans! The Impact of Vitamin D Deficiency on Mental Health in Adolescents: A Cross-Sectional Study. J. Adv. Med. Med. Res. 2023, 35, 103–107. [Google Scholar] [CrossRef]
- Tolppanen, A.M.; Sayers, A.; Fraser, W.D.; Lawlor, D.A. Association of serum 25-hydroxyvitamin D3 and D2 with academic performance in childhood: Findings from a prospective birth cohort. J. Epidemiol. Community Health 2012, 66, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Saeed, B.Q.; Jairoun, A.A.; Khamis, A.A.; Abdelrahim, L.H.; Aljomhi, A.A.; Adrees, A.O.; Fahady, K.S.; Al-Hajjaj, M.S. Vitamin D deficiency and insufficiency among university students: Prevalence, risk factors, and the association between vitamin D deficiency and episodes of respiratory tract infections. Risk Manag. Healthc. Policy 2021, 14, 2733–2741. [Google Scholar] [CrossRef] [PubMed]
- Nimri, L.F. Vitamin D status of female UAE college students and associated risk factors. J. Public Health 2018, 40, e284–e290. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.B.; Szperka, C.L.; Hershey, A.D.; Law, E.F.; Palermo, T.M.; Groenewald, C.B. Association of headache with school functioning among children and adolescents in the United States. JAMA Pediatr. 2021, 175, 522–524. [Google Scholar] [CrossRef] [PubMed]
- Ulrike Glatt, D.; McSorley, E.; Pourshahidi, L.K.; Revuelta Iniesta, R.; McCluskey, J.; Beggan, L.; Slevin, M.; Gleeson, N.; Cobice, D.F.; Dobbin, S.; et al. Vitamin D Status and Health Outcomes in School Children in Northern Ireland: Year One Results from the D-VinCHI Study. Nutrients 2022, 14, 804. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Salih, L.M.A.; Saeed, E. Awareness of medical students about vitamin D deficiency at Ahfad University for women, Sudan. Sudan. J. Paediatr. 2019, 19, 117–125. [Google Scholar] [CrossRef]
- Karchynskaya, V.; Kopcakova, J.; Klein, D.; Gába, A.; Madarasova-Geckova, A.; van Dijk, J.P.; de Winter, A.F.; Reijneveld, S.A. Is BMI a valid indicator of overweight and obesity for adolescents? Int. J. Environ. Res. Public Health 2020, 17, 34815. [Google Scholar] [CrossRef]
- Khwanchuea, R.; Punsawad, C. Associations Between Body Composition, Leptin, and Vitamin D Varied by the Body Fat Percentage in Adolescents. Front. Endocrinol. 2022, 13, 876231. [Google Scholar] [CrossRef]
- Correa-Burrows, P.; Blanco, E.; Reyes, M.; Castillo, M.; Peirano, P.; Algarín, C.; Lozoff, B.; Gahagan, S.; Burrows, R. Leptin status in adolescence is associated with academic performance in high school: A cross-sectional study in a Chilean birth cohort. BMJ Open 2016, 6, e010972. [Google Scholar] [CrossRef]
- Buhl-Wiggers, J.; Jones, S.; Thornton, R. Boys lagging behind: Unpacking gender differences in academic achievement across East Africa. Int. J. Educ. Dev. 2021, 83, 102382. [Google Scholar] [CrossRef]
- Marcenaro–Gutierrez, O.; Lopez–Agudo, L.A.; Ropero-García, M.A. Gender Differences in Adolescents’ Academic Achievement. Young 2018, 26, 250–270. [Google Scholar] [CrossRef]
- Tadese, M.; Yeshaneh, A.; Mulu, G.B. Determinants of good academic performance among university students in Ethiopia: A cross-sectional study. BMC Med. Educ. 2022, 22, 395. [Google Scholar] [CrossRef] [PubMed]
- Masud, S.; Mufarrih, S.H.; Qureshi, N.Q.; Khan, F.; Khan, S.; Khan, M.N. Academic Performance in Adolescent Students: The Role of Parenting Styles and Socio-Demographic Factors—A Cross Sectional Study from Peshawar, Pakistan. Front. Psychol. 2019, 10, 2497. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.J.; García-Rubio, J.; Olivares, P.R. The relative age effect and its influence on academic performance. PLoS ONE 2015, 10, e141895. [Google Scholar] [CrossRef]
- Lara, L.; Saracostti, M. Effect of parental involvement on children’s academic achievement in Chile. Front. Psychol. 2019, 10, 1464. [Google Scholar] [CrossRef] [PubMed]
- Vega-Franco, L.; Mejía, A.M.; Robles, B.; Moreno, L.; Pérez, Y. The intelligence quotient and malnutrition. Iron deficiency and the lead concentration as confusing variables. Bol. Med. Hosp. Infant. Mex. 1991, 48, 826–831. [Google Scholar] [PubMed]
- More, S.; Shivkumar, V.B.; Gangane, N.; Shende, S. Effects of iron deficiency on cognitive function in school going adolescent females in rural area of central India. Anemia 2013, 2013, 819136. [Google Scholar] [CrossRef]
- Nam, K. Until when does the effect of age on academic achievement persist? Evidence from Korean data. Econ. Educ. Rev. 2014, 40, 106–122. [Google Scholar] [CrossRef]
- Kuang, W.; Chen, Z.; Shi, K.; Sun, H.; Li, H.; Huang, L.; Bi, J. Adverse health effects of lead exposure on physical growth, erythrocyte parameters and school performances for school-aged children in eastern China. Environ. Int. 2020, 145, 106130. [Google Scholar] [CrossRef]
- Haapala, E.A.; Poikkeus, A.M.; Kukkonen-Harjula, K.; Tompuri, T.; Lintu, N.; Väistö, J.; Leppänen, P.H.T.; Laaksonen, D.E.; Lindi, V.; Lakka, T.A. Associations of physical activity and sedentary behavior with academic skills—A follow-up study among primary school children. PLoS ONE 2014, 9, e107031. [Google Scholar] [CrossRef] [PubMed]
- Sember, V.; Jurak, G.; Kovač, M.; Morrison, S.A.; Starc, G. Children’s physical activity, academic performance, and cognitive functioning: A systematic review and meta-analysis. Front. Public Health 2020, 8, 307. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | ||
|---|---|---|
| Mean (standard deviation) | ||
| Age, years | 15.1 (1.6) | |
| Median (interquartile range) | ||
| Body mass index for age Z-score | −0.46 (−1.59–0.50) | |
| 25-hydroxy vitamin D concentration, ng/mL | 20.10 (10.56–31.87) | |
| Frequency (proportions) | ||
| Gender | Female | 129 (53.5) |
| Male | 112 (46.5) | |
| Mother’s education level | ≥secondary | 156 (64.7) |
| <secondary | 85 (35.3) | |
| Mother’s occupation | Housewife | 211 (87.6) |
| Employed | 30 (12.4) | |
| Father’s occupation | Laborer | 143 (59.3) |
| Farmer | 98 (40.7) | |
| Father’s education | ≥secondary | 162 (67.2) |
| <secondary | 79 (32.8) | |
| Vitamin D status | Normal ≥ 20 ng/mL | 124 (51.5) |
| Deficient < 20 ng/ml | 117 (48.5) | |
| Anemia | No | 184 (76.3) |
| Yes | 57 (23.7) | |
| Variable | Academic Performance Score in % | ||
|---|---|---|---|
| Coefficient (Standard Error) | p Value | ||
| Age, years | 3.23 (0.67) | <0.001 | |
| Body mass index for age Z-score | 1.40 (0.78) | 0.075 | |
| 25-hydroxy vitamin concentration (ng/mL) | 0.20 (0.08) | 0.010 | |
| Anemia | −0.491 (2.45) | 0.841 | |
| Gender | Male | Reference | |
| Female | 7.62 (2.37) | 0.002 | |
| Mother’s education | ≥secondary | Reference | |
| <secondary | −0.77 (2.35) | 0.743 | |
| Mother’s occupation | Housewife | Reference | |
| Employed | 6.27 (3.13) | 0.049 | |
| Father’s education | ≥secondary | Reference | |
| <secondary | −3.47 (2.51) | 0.167 | |
| Father’s occupation | Laborer | Reference | |
| Farmer | −0.73 (2.10) | 0.730 | |
| Anemia | No | Reference | |
| Yes | −0.491 (2.45) | 0.841 | |
| Variable | Poor Academic Performance (Score < 3.74%) (n = 0.146) | Good Academic Performance (Score ≥ 33.74%) (n = 95) | Odds Ratio | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|
| Mean (standard deviation) | ||||||
| Age, years | 14.6 (1.6) | 15.8 (1.3) | 0.59 | 0.49–0.72 | <0.001 | |
| Median (interquartile range) | ||||||
| Body mass index for age Z-score | −0.55 (−1.66–0.37) | −0.30 (−1.36–0.74) | 0.86 | 0.71–1.03 | 0.107 | |
| 25-hydroxy vitamin D concentration (ng/mL) | 17.65 (8.0–27.78) | 25.0 (14.72–36.44) | 0.98 | 0.96–0.99 | 0.008 | |
| Frequency (proportions) | ||||||
| Gender | Female | 73 (50.0) | 56 (58.9) | Reference | 0.174 | |
| Male | 73 (50.0) | 39 (41.1) | 1.44 | 0.85–2.42 | ||
| Mother’s education level | ≥secondary | 95 (65.1) | 61 (64.2) | Reference | 0.892 | |
| <secondary | 51 (34.9) | 34 (35.8) | 1.04 | 0.61–1.79 | ||
| Mother’s occupation | Housewife | 131 (89.7) | 80 (84.2) | Reference | 0.208 | |
| Employed | 15 (10.3) | 15 (15.8) | 0.61 | 0.28–1.32 | ||
| Father’s occupation | Laborer | 64 (43.8) | 34 (35.8) | Reference | 0.215 | |
| Farmer | 82 (56.2) | 61 (64.2) | 1.40 | 0.82–2.38 | ||
| Father’s education | ≥secondary | 53 (36.3) | 69 (72.6) | Reference | 0.150 | |
| <secondary | 93 (63.7) | 26 (27.4) | 1.52 | 0.86–2.63 | ||
| vitamin D status | Normal ≥ 20 | 65 (44.5) | 59 (62.1) | Reference | 0.008 | |
| Deficient < 20 | 81 (55.5) | 36 (37.9) | 2.04 | 1.21–3.46 | ||
| Anemia | Non-anemic | 108 (74.0) | 76 (80.0) | Reference | 0.283 | |
| Yes | 38 (26.0) | 19 (20.0) | 1.41 (0.75–2.63) | |||
| Variable | Adjusted Odds Ratio (95% Confidence Interval) | p Value | |
|---|---|---|---|
| Age, years | 0.59 (0.48–0.72) | <0.001 | |
| Body mass index for age Z-score | 0.86 (0.70–1.05) | 0.139 | |
| 25-hydroxy vitamin concentration (ng/mL) * | 0.97 (0.95–0.99) | 0.016 | |
| Gender | Female | Reference | |
| Male | 1.60 (0.88–2.92) | 0.126 | |
| Father’s education | ≥secondary | Reference | |
| <secondary | 1.64 (0.88–3.03 | 0.121 | |
| Vitamin D status * | Normal ≥ 20 ng/mL | Reference | |
| Deficient < 20 ng/mL | 2.18 (1.20 –3.96) | 0.011 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, A.A.; Elbashir, M.I.; Al-Nafeesah, A.; AlEed, A.; Adam, I. Association between Serum 25-Hydroxyvitamin D Concentrations and Academic Performance among Adolescent Schoolchildren: A Cross-Sectional Study. Nutrients 2023, 15, 4552. https://doi.org/10.3390/nu15214552
Hassan AA, Elbashir MI, Al-Nafeesah A, AlEed A, Adam I. Association between Serum 25-Hydroxyvitamin D Concentrations and Academic Performance among Adolescent Schoolchildren: A Cross-Sectional Study. Nutrients. 2023; 15(21):4552. https://doi.org/10.3390/nu15214552
Chicago/Turabian StyleHassan, Ahmed A., Mustafa I. Elbashir, Abdullah Al-Nafeesah, Ashwaq AlEed, and Ishag Adam. 2023. "Association between Serum 25-Hydroxyvitamin D Concentrations and Academic Performance among Adolescent Schoolchildren: A Cross-Sectional Study" Nutrients 15, no. 21: 4552. https://doi.org/10.3390/nu15214552
APA StyleHassan, A. A., Elbashir, M. I., Al-Nafeesah, A., AlEed, A., & Adam, I. (2023). Association between Serum 25-Hydroxyvitamin D Concentrations and Academic Performance among Adolescent Schoolchildren: A Cross-Sectional Study. Nutrients, 15(21), 4552. https://doi.org/10.3390/nu15214552