
Water Intake and Handgrip Strength in US Adults: A Cross-Sectional Study Based on NHANES 2011–2014 Data

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
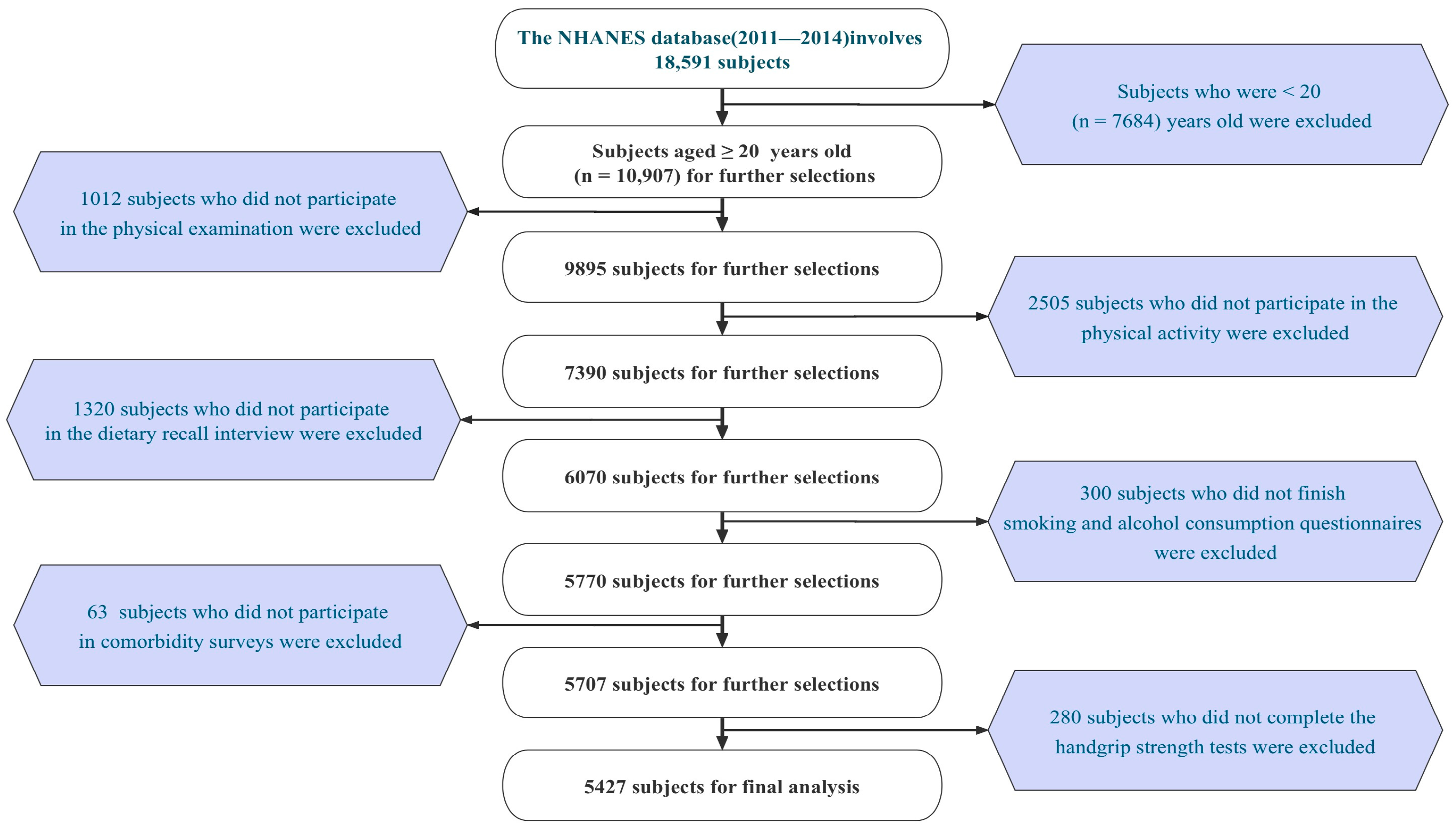
2.1. Study Subjects and Data Sources
2.2. Dietary Assessment
2.3. Daily Total Intake of Water
2.4. Handgrip Strength
2.5. Covariate
2.6. Statistical Methods
3. Results
3.1. Baseline Characteristics of the Study Population
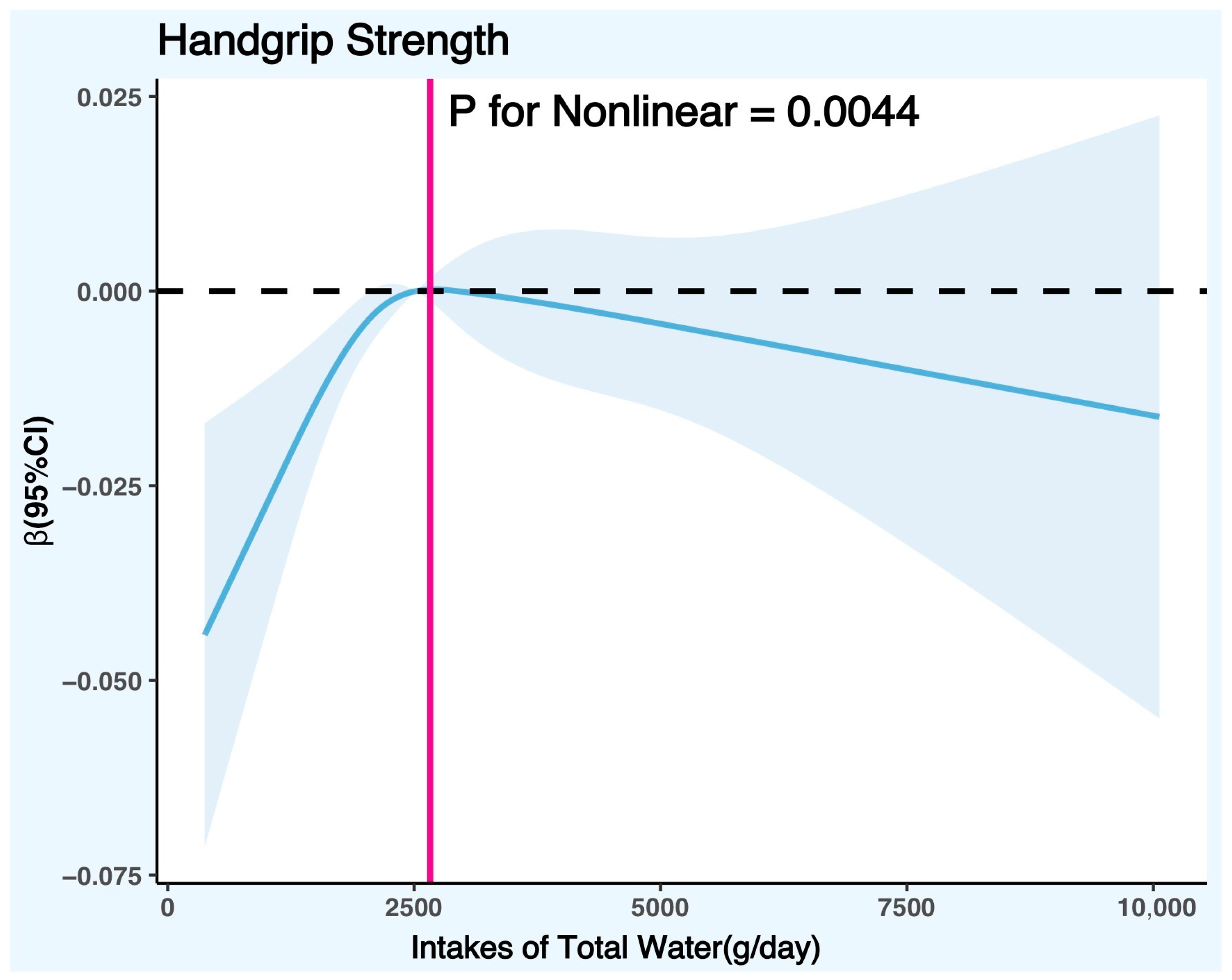
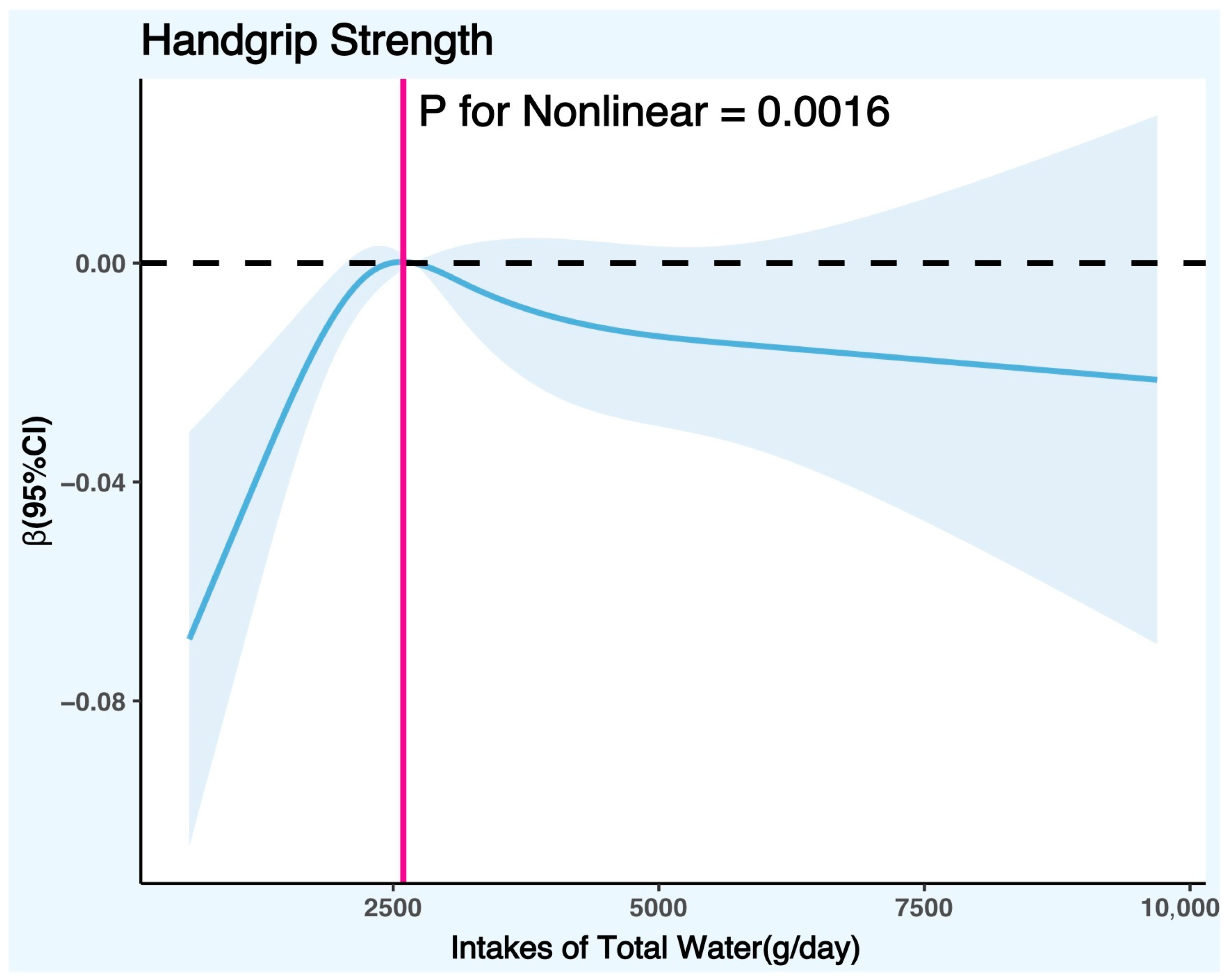
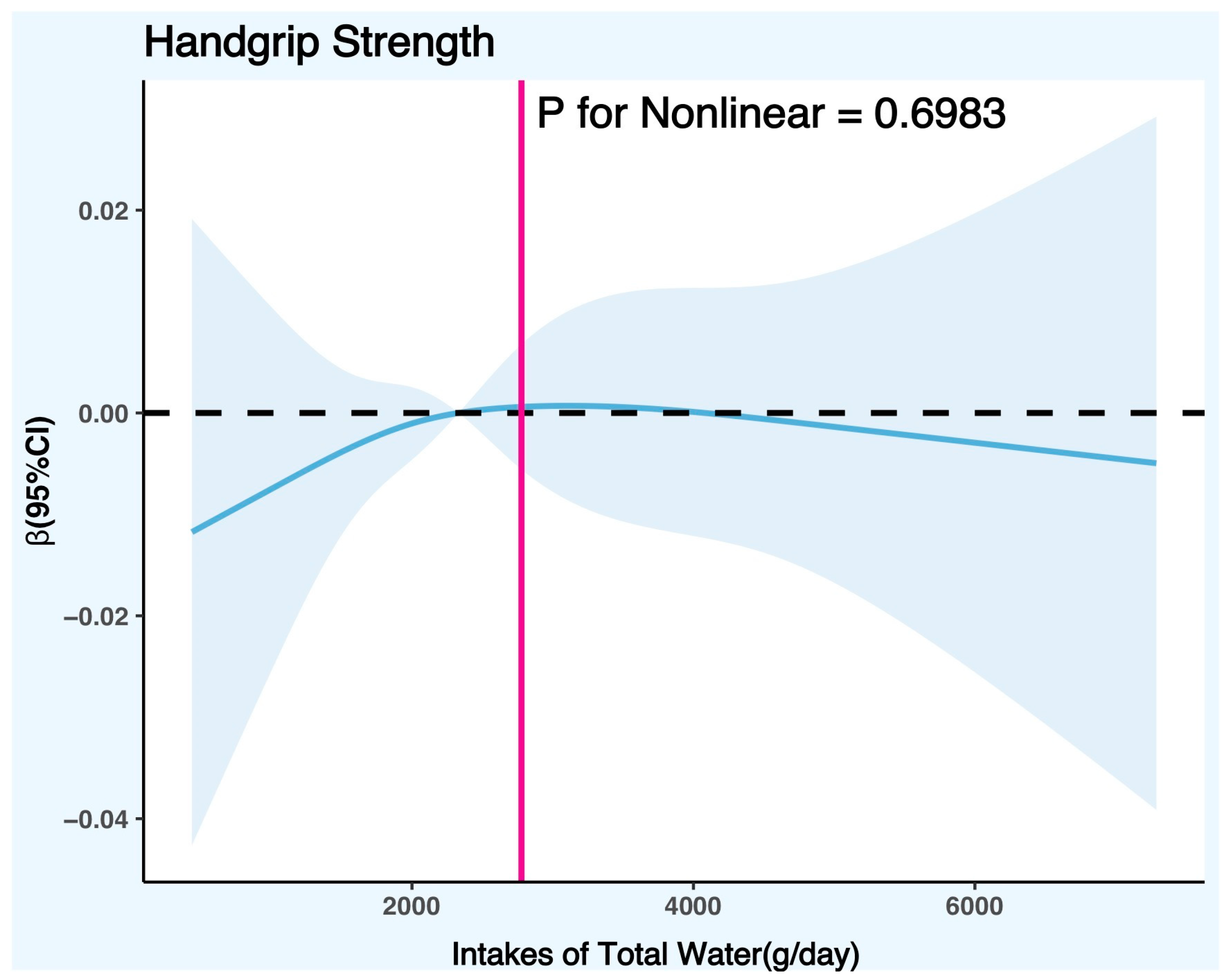
3.2. Association Analysis between Daily Total Intake of Water and Handgrip Strength in American Adults
3.3. Interaction Effect Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M.; D’Anci, K.E.; Rosenberg, I.H. Water, Hydration, and Health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Jéquier, E.; Constant, F. Water as an Essential Nutrient: The Physiological Basis of Hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef]
- Bolignano, D.; Zoccali, C. Vasopressin beyond Water: Implications for Renal Diseases. Curr. Opin. Nephrol. Hypertens 2010, 19, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.F.; Sontrop, J.M.; Macnab, J.J.; Suri, R.S.; Moist, L.; Salvadori, M.; Garg, A.X. Urine Volume and Change in Estimated GFR in a Community-Based Cohort Study. Clin. J. Am. Soc. Nephrol. 2011, 6, 2634–2641. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, T.; Takahashi, T.; Kusunoki, M.; Kantoh, M.; Seino, Y.; Utsunomiya, J. Gallbladder Dynamics and Plasma Cholecystokinin Responses after Meals, Oral Water, or Sham Feeding in Healthy Subjects. Am. J. Med. Sci. 1988, 295, 102–107. [Google Scholar] [CrossRef]
- Chan, J.; Knutsen, S.F.; Blix, G.G.; Lee, J.W.; Fraser, G.E. Water, Other Fluids, and Fatal Coronary Heart Disease: The Adventist Health Study. Am. J. Epidemiol. 2002, 155, 827–833. [Google Scholar] [CrossRef]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The Role of Water Homeostasis in Muscle Function and Frailty: A Review. Nutrients 2019, 11, 1857. [Google Scholar] [CrossRef]
- Hooper, L.; Bunn, D.; Jimoh, F.O.; Fairweather-Tait, S.J. Water-Loss Dehydration and Aging. Mech. Ageing Dev. 2014, 136–137, 50–58. [Google Scholar] [CrossRef]
- Goulet, E.D.B.; Mélançon, M.O.; Lafrenière, D.; Paquin, J.; Maltais, M.; Morais, J.A. Impact of Mild Hypohydration on Muscle Endurance, Power, and Strength in Healthy, Active Older Men. J. Strength Cond. Res. 2018, 32, 3405–3415. [Google Scholar] [CrossRef]
- Gosmanov, A.R.; Schneider, E.G.; Thomason, D.B. NKCC Activity Restores Muscle Water during Hyperosmotic Challenge Independent of Insulin, ERK, and P38 MAPK. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R655–R665. [Google Scholar] [CrossRef]
- Fernández-Elías, V.E.; Ortega, J.F.; Nelson, R.K.; Mora-Rodriguez, R. Relationship between Muscle Water and Glycogen Recovery after Prolonged Exercise in the Heat in Humans. Eur. J. Appl. Physiol. 2015, 115, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Mendes, J.; Padrão, P.; Moreira, P.; Santos, A.; Borges, N.; Afonso, C.; Negrão, R.; Amaral, T.F. Handgrip Strength and Its Association With Hydration Status and Urinary Sodium-to-Potassium Ratio in Older Adults. J. Am. Coll. Nutr. 2020, 39, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.-I.; Choi, H.; Song, S.-Y.; Park, K.-S.; Lee, D.-H.; Ha, Y.-C. Relationship between Water Intake and Skeletal Muscle Mass in Elderly Koreans: A Nationwide Population-Based Study. Nutrition 2018, 53, 38–42. [Google Scholar] [CrossRef]
- Manini, T.M.; Clark, B.C. Dynapenia and Aging: An Update. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M.; Bolanowski, S.J.; Ploutz-Snyder, L.L. Adaptations in Human Neuromuscular Function Following Prolonged Unweighting: II. Neurological Properties and Motor Imagery Efficacy. J. Appl. Physiol. 2006, 101, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D. Analysis of 2009–2012 Nutrition Health and Examination Survey (NHANES) Data to Estimate the Median Water Intake Associated with Meeting Hydration Criteria for Individuals Aged 12–80 Years in the US Population. Nutrients 2019, 11, 657. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.-L.; Wei, M.-H.; Cui, Y.; Di, D.-S.; Song, W.-J.; Zhang, R.-Y.; Liu, J.-A.; Wang, Q. Association between Water Intake and Mortality Risk-Evidence from a National Prospective Study. Front. Nutr. 2022, 9, 822119. [Google Scholar] [CrossRef]
- Yang, M.; Chun, O.K. Consumptions of Plain Water, Moisture in Foods and Beverages, and Total Water in Relation to Dietary Micronutrient Intakes and Serum Nutrient Profiles among US Adults. Public Health Nutr. 2015, 18, 1180–1186. [Google Scholar] [CrossRef]
- Ji, C.; Xia, Y.; Tong, S.; Wu, Q.; Zhao, Y. Association of Handgrip Strength with the Prevalence of Metabolic Syndrome in US Adults: The National Health and Nutrition Examination Survey. Aging 2020, 12, 7818–7829. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Wang, Y.-C.; Yen, S.-C.; Grogan, K.A. Handgrip Strength: A Comparison of Values Obtained from the NHANES and NIH Toolbox Studies. Am. J. Occup. Ther. 2019, 73, 7302205080p1–7302205080p9. [Google Scholar] [CrossRef]
- Wu, R.; Delahunt, E.; Ditroilo, M.; Lowery, M.; De Vito, G. Effects of Age and Sex on Neuromuscular-Mechanical Determinants of Muscle Strength. Age 2016, 38, 57. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.E.; MacDougall, J.D.; Tarnopolsky, M.A.; Sale, D.G. Gender Differences in Strength and Muscle Fiber Characteristics. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 66, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Bchini, S.; Hammami, N.; Selmi, T.; Zalleg, D.; Bouassida, A. Influence of Muscle Volume on Jumping Performance in Healthy Male and Female Youth and Young Adults. BMC Sports Sci. Med. Rehabil. 2023, 15, 26. [Google Scholar] [CrossRef] [PubMed]
- Sung, E.-S.; Han, A.; Hinrichs, T.; Vorgerd, M.; Platen, P. Impact of Body Mass Index on Muscle Strength, Thicknesses, and Fiber Composition in Young Women. Int. J. Environ. Res. Public Health 2022, 19, 9789. [Google Scholar] [CrossRef]
- Pothisiri, W.; Prasitsiriphon, O.; Saikia, N.; Aekplakorn, W. Education and Grip Strength among Older Thai Adults: A Mediation Analysis on Health-Related Behaviours. SSM Popul. Health 2021, 15, 100894. [Google Scholar] [CrossRef]
- Hoge, C.; Bowling, C.B.; Lim, S.S.; Drenkard, C.; Plantinga, L.C. Association of Poverty Income Ratio with Physical Functioning in a Cohort of Patients with Systemic Lupus Erythematosus. J. Rheumatol. 2020, 47, 983–990. [Google Scholar] [CrossRef]
- Cui, Y.; Huang, C.; Momma, H.; Sugiyama, S.; Niu, K.; Nagatomi, R. The Longitudinal Association between Alcohol Consumption and Muscle Strength: A Population-Based Prospective Study. J. Musculoskelet Neuronal Interact. 2019, 19, 294–299. [Google Scholar]
- Prieto-Alhambra, D.; Turkiewicz, A.; Reyes, C.; Timpka, S.; Rosengren, B.; Englund, M. Smoking and Alcohol Intake but Not Muscle Strength in Young Men Increase Fracture Risk at Middle Age: A Cohort Study Linked to the Swedish National Patient Registry. J. Bone Miner. Res. 2020, 35, 498–504. [Google Scholar] [CrossRef]
- Wang, L.; van Iersel, L.E.J.; Pelgrim, C.E.; Lu, J.; van Ark, I.; Leusink-Muis, T.; Gosker, H.R.; Langen, R.C.J.; Schols, A.M.W.J.; Argilés, J.M.; et al. Effects of Cigarette Smoke on Adipose and Skeletal Muscle Tissue: In Vivo and In Vitro Studies. Cells 2022, 11, 2893. [Google Scholar] [CrossRef]
- Caron, M.-A.; Morissette, M.C.; Thériault, M.-E.; Nikota, J.K.; Stämpfli, M.R.; Debigaré, R. Alterations in Skeletal Muscle Cell Homeostasis in a Mouse Model of Cigarette Smoke Exposure. PLoS ONE 2013, 8, e66433. [Google Scholar] [CrossRef]
- Shozi, S.; Monyeki, M.A.; Moss, S.J.; Pienaar, C. Relationships between Physical Activity, Body Mass Index, Waist Circumference and Handgrip Strength amongst Adults from the North West Province, South Africa: The PURE Study. Afr. J. Prim. Health Care Fam. Med. 2022, 14, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Choi, H.Y.; Ki, M. Association between Levels of Physical Activity and Low Handgrip Strength: Korea National Health and Nutrition Examination Survey 2014–2019. Epidemiol. Health 2022, 44, e2022027. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Goldman, J.D.; Sahyoun, N.R.; Moshfegh, A.J. Association between Dietary Protein Intake and Grip Strength among Adults Aged 51 Years and over: What We Eat in America, National Health and Nutrition Examination Survey 2011–2014. PLoS ONE 2018, 13, e0191368. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.K.; Hairi, N.N.; Jalaludin, M.Y.; Majid, H.A. Dietary Intake, Physical Activity and Muscle Strength among Adolescents: The Malaysian Health and Adolescents Longitudinal Research Team (MyHeART) Study. BMJ Open 2019, 9, e026275. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Rossignon, F.; Carayon, A.; Capel, F.; Rigaudière, J.-P.; De Saint Vincent, S.; Le-Bacquer, O.; Salles, J.; Giraudet, C.; Patrac, V.; et al. Deleterious Effect of High-Fat Diet on Skeletal Muscle Performance Is Prevented by High-Protein Intake in Adult Rats but Not in Old Rats. Front. Physiol. 2021, 12, 749049. [Google Scholar] [CrossRef]
- Margolis, L.M.; Pasiakos, S.M. Low Carbohydrate Availability Impairs Hypertrophy and Anaerobic Performance. Curr. Opin. Clin. Nutr. Metab. Care 2023, 26, 347–352. [Google Scholar] [CrossRef]
- Cholewa, J.M.; Newmire, D.E.; Zanchi, N.E. Carbohydrate Restriction: Friend or Foe of Resistance-Based Exercise Performance? Nutrition 2019, 60, 136–146. [Google Scholar] [CrossRef]
- Doyev, R.; Axelrod, R.; Keinan-Boker, L.; Shimony, T.; Goldsmith, R.; Nitsan, L.; Dichtiar, R.; Sinai, T. Energy Intake Is Highly Associated with Handgrip Strength in Community-Dwelling Elderly Adults. J. Nutr. 2021, 151, 1249–1255. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, P.; Song, Y.; Ma, N.; Lu, J. Association between Sugar-Sweetened Beverage Consumption Frequency and Muscle Strength: Results from a Sample of Chinese Adolescents. BMC Public Health 2023, 23, 1010. [Google Scholar] [CrossRef]
- Peinado, A.B.; Rojo-Tirado, M.A.; Benito, P.J. Sugar and exercise: Its importance in athletes. Nutr. Hosp. 2013, 28 (Suppl. S4), 48–56. [Google Scholar] [CrossRef]
- Ji, C.; Zheng, L.; Zhang, R.; Wu, Q.; Zhao, Y. Handgrip Strength Is Positively Related to Blood Pressure and Hypertension Risk: Results from the National Health and Nutrition Examination Survey. Lipids Health Dis. 2018, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, L.; Peng, X.; Xie, Y.; Bao, X.; Huang, J.; Wang, P. Association of Handgrip Strength with Hypertension among Middle-Aged and Elderly People in Southern China: A Cross-Sectional Study. Clin. Exp. Hypertens 2020, 42, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Miranda, H.; Bentes, C.; Resende, M.; Netto, C.C.; Nasser, I.; Willardson, J.; Marinheiro, L. Association between Handgrip Strength and Body Composition, Physical Fitness, and Biomarkers in Postmenopausal Women with Metabolic Syndrome. Rev. Assoc. Med. Bras. 2022, 68, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Wang, F.; Huang, Y.; Yuan, Y.; Huang, F.; Zhu, P. Handgrip Strength Weakness and Asymmetry Together Are Associated with Cardiovascular Outcomes in Older Outpatients: A Prospective Cohort Study. Geriatr. Gerontol. Int. 2022, 22, 759–765. [Google Scholar] [CrossRef]
- Li, D.; Guo, G.; Xia, L.; Yang, X.; Zhang, B.; Liu, F.; Ma, J.; Hu, Z.; Li, Y.; Li, W.; et al. Relative Handgrip Strength Is Inversely Associated with Metabolic Profile and Metabolic Disease in the General Population in China. Front. Physiol. 2018, 9, 59. [Google Scholar] [CrossRef]
- Suda, N.; Manda, C.; Gallagher, J.; Wagatsuma, Y. Observational Study: Handgrip Strength, Body Composition and Diabetes Mellitus. BMC Res. Notes 2021, 14, 332. [Google Scholar] [CrossRef]
- Manda, C.M.; Nakanga, W.P.; Mkandawire, J.; Muula, A.S.; Nyirenda, M.J.; Crampin, A.C.; Wagatsuma, Y. Handgrip Strength as a Simple Measure for Screening Prediabetes and Type 2 Diabetes Mellitus Risk among Adults in Malawi: A Cross-Sectional Study. Trop Med. Int. Health 2021, 26, 1709–1717. [Google Scholar] [CrossRef]
- Jang, B.N.; Nari, F.; Kim, S.; Park, E.-C. Association between Relative Handgrip Strength and Prediabetes among South Korean Adults. PLoS ONE 2020, 15, e0240027. [Google Scholar] [CrossRef]
- Zhuang, C.-L.; Zhang, F.-M.; Li, W.; Wang, K.-H.; Xu, H.-X.; Song, C.-H.; Guo, Z.-Q.; Shi, H.-P. Associations of Low Handgrip Strength with Cancer Mortality: A Multicentre Observational Study. J. Cachexia Sarcopenia Muscle 2020, 11, 1476–1486. [Google Scholar] [CrossRef]
- López-Bueno, R.; Andersen, L.L.; Calatayud, J.; Casaña, J.; Grabovac, I.; Oberndorfer, M.; Del Pozo Cruz, B. Associations of Handgrip Strength with All-Cause and Cancer Mortality in Older Adults: A Prospective Cohort Study in 28 Countries. Age Ageing 2022, 51, afac117. [Google Scholar] [CrossRef]
- Jiang, R.; Westwater, M.L.; Noble, S.; Rosenblatt, M.; Dai, W.; Qi, S.; Sui, J.; Calhoun, V.D.; Scheinost, D. Associations between Grip Strength, Brain Structure, and Mental Health in >40,000 Participants from the UK Biobank. BMC Med. 2022, 20, 286. [Google Scholar] [CrossRef] [PubMed]
- Mey, R.; Calatayud, J.; Casaña, J.; Cuenca-Martínez, F.; Suso-Martí, L.; Andersen, L.L.; López-Bueno, R. Handgrip Strength in Older Adults with Chronic Diseases from 27 European Countries and Israel. Eur. J. Clin. Nutr. 2023, 77, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Wang, H.; Bai, Y.; Huang, L.; Zhang, H. Handgrip Strength and All-Cause Mortality in Patients with Chronic Kidney Disease: An Updated Systematic Review and Meta-Analysis of Cohort Studies. Int. Urol. Nephrol. 2023, 55, 2857–2865. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Wang, H.; Wang, W.; Qing, C.; Zhang, W.; Gao, X.; Shi, Y.; Li, Y.; Zheng, Z. Association between Composite Dietary Antioxidant Index and Handgrip Strength in American Adults: Data from National Health and Nutrition Examination Survey (NHANES, 2011–2014). Front. Nutr. 2023, 10, 1147869. [Google Scholar] [CrossRef]
- Kim, H.; Beom, S.H.; Kim, T.H.; Kim, B.-J. Association of Water Intake with Hand Grip Strength in Community-Dwelling Older Adults. Nutrients 2021, 13, 1756. [Google Scholar] [CrossRef]
- He, W.A.; Berardi, E.; Cardillo, V.M.; Acharyya, S.; Aulino, P.; Thomas-Ahner, J.; Wang, J.; Bloomston, M.; Muscarella, P.; Nau, P.; et al. NF-κB-Mediated Pax7 Dysregulation in the Muscle Microenvironment Promotes Cancer Cachexia. J. Clin. Investig. 2013, 123, 4821–4835. [Google Scholar] [CrossRef]
- Goodman, A.B.; Blanck, H.M.; Sherry, B.; Park, S.; Nebeling, L.; Yaroch, A.L. Behaviors and Attitudes Associated with Low Drinking Water Intake among US Adults, Food Attitudes and Behaviors Survey, 2007. Prev. Chronic Dis. 2013, 10, E51. [Google Scholar] [CrossRef]
- Pouramin, P.; Nagabhatla, N.; Miletto, M. A Systematic Review of Water and Gender Interlinkages: Assessing the Intersection with Health. Front. Water 2020, 2, 6. [Google Scholar] [CrossRef]
- Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academies Press: Washington, DC, USA, 2005; p. 10925.
- Lang, T.F. The Bone-Muscle Relationship in Men and Women. J. Osteoporos. 2011, 2011, 702735. [Google Scholar] [CrossRef]
- Fairchild Saidi, G.; Branscum, P. Gender Differences for Theory-Based Determinants of Muscle-Strengthening Physical Activity in College-Aged Students: A Moderation Analysis. Transl. Behav. Med. 2020, 10, 781–791. [Google Scholar] [CrossRef]
- Nuzzo, J.L. Narrative Review of Sex Differences in Muscle Strength, Endurance, Activation, Size, Fiber Type, and Strength Training Participation Rates, Preferences, Motivations, Injuries, and Neuromuscular Adaptations. J. Strength Cond. Res. 2023, 37, 494–536. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Howley, E.T. Exercise Physiology: Theory and Application to Fitness and Performances; McGraw-Hill: New York, NY, USA, 1995; Volume 27, p. 466. [Google Scholar]
- El-Sharkawy, A.M.; Sahota, O.; Lobo, D.N. Acute and Chronic Effects of Hydration Status on Health. Nutr. Rev. 2015, 73 (Suppl. S2), 97–109. [Google Scholar] [CrossRef] [PubMed]
- Powers, J.D.; Malingen, S.A.; Regnier, M.; Daniel, T.L. The Sliding Filament Theory Since Andrew Huxley: Multiscale and Multidisciplinary Muscle Research. Annu. Rev. Biophys. 2021, 50, 373–400. [Google Scholar] [CrossRef] [PubMed]
- Bolli, R. William Harvey and the Discovery of the Circulation of the Blood. Circ. Res. 2019, 124, 1300–1302. [Google Scholar] [CrossRef]
- Barley, O.R.; Chapman, D.W.; Abbiss, C.R. Reviewing the Current Methods of Assessing Hydration in Athletes. J. Int. Soc. Sports Nutr. 2020, 17, 52. [Google Scholar] [CrossRef]
- Negoianu, D.; Goldfarb, S. Just Add Water. J. Am. Soc. Nephrol. 2008, 19, 1041–1043. [Google Scholar] [CrossRef]
- Wolfe, R.R. The Underappreciated Role of Muscle in Health and Disease. Am. J. Clin. Nutr. 2006, 84, 475–482. [Google Scholar] [CrossRef]
- Phillips, S.M.; Van Loon, L.J.C. Dietary Protein for Athletes: From Requirements to Optimum Adaptation. J. Sports Sci. 2011, 29 (Suppl. S1), S29–S38. [Google Scholar] [CrossRef]
- Kandel, E.R.; Schwartz, J.H.; Jessell, T.M. Principles of Neural Science, 4th ed.; McGraw-Hill, Health Professions Division: New York, NY, USA, 2000; ISBN 978-0-8385-7701-1. [Google Scholar]
- Purves, E. Neuroscience, 6th ed.; Augustine, G.J., Fitzpatrick, D., Hall, W.C., LaMantia, A.-S., Mooney, R.D., Platt, M.L., White, L.E., Eds.; Oxford University Press: Oxford, UK; New York, NY, USA, 2017; ISBN 978-1-60535-380-7. [Google Scholar]
- Lieberman, H.R. Hydration and Cognition: A Critical Review and Recommendations for Future Research. J. Am. Coll. Nutr. 2007, 26, 555S–561S. [Google Scholar] [CrossRef]
- Martínez García, R.M.; Jiménez Ortega, A.I.; Lorenzo-Mora, A.M.; Bermejo, L.M. Importance of hydration in cardiovascular health and cognitive function. Nutr. Hosp. 2022, 39, 17–20. [Google Scholar] [CrossRef]
- Glaser, G.H. Neurologic Symptoms with Electrolyte and Water Imbalance. Postgrad. Med. 1971, 50, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Van Acker, G.M.; Luchies, C.W.; Cheney, P.D. Timing of Cortico-Muscle Transmission During Active Movement. Cereb. Cortex 2016, 26, 3335–3344. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, J.; Del Vecchio, A.; Rothwell, J.C.; Baker, S.N.; Farina, D. Only the Fastest Corticospinal Fibers Contribute to β Corticomuscular Coherence. J. Neurosci. 2021, 41, 4867–4879. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | Quartile 1 [6.93, 1855.685] | Quartile 2 (1855.685, 2517.15] | Quartile 3 (2517.15, 3358.675] | Quartile 4 (3358.675, 15,829.6] | p-Value |
|---|---|---|---|---|---|---|
| N | 5427 | 1357 | 1357 | 1356 | 1357 | |
| Handgrip Strength, kg/weight (kg) | 0.93 (0.01) | 0.90 (0.01) | 0.91 (0.01) | 0.93 (0.01) | 0.97 (0.01) | <0.0001 |
| Gender, n (weighted %) | <0.0001 | |||||
| Female | 2577 (48.37) | 760 (58.28) | 715 (54.20) | 623 (47.19) | 479 (37.62) | |
| Male | 2850 (51.63) | 597 (41.72) | 642 (45.80) | 733 (52.81) | 878 (62.38) | |
| Age, years, n (weighted %) | <0.0001 | |||||
| 20–29 | 1089 (20.06) | 330 (26.32) | 251 (18.91) | 219 (15.82) | 289 (21.39) | |
| 30–39 | 993 (18.29) | 216 (15.65) | 215 (14.46) | 265 (18.57) | 297 (19.42) | |
| 40–49 | 974 (17.94) | 201 (16.25) | 248 (18.83) | 251 (19.16) | 274 (21.13) | |
| 50–59 | 889 (16.38) | 177 (16.07) | 229 (19.55) | 236 (20.67) | 247 (21.24) | |
| ≥60 | 1483 (27.32) | 433 (25.72) | 414 (28.26) | 386 (25.78) | 250 (16.83) | |
| Race, n (weighted %) | <0.0001 | |||||
| Non-Hispanic Black | 1211 (10.21) | 433 (18.27) | 328 (11.29) | 242 (7.63) | 208 (6.04) | |
| Mexican American | 567 (7.21) | 133 (8.45) | 145 (7.17) | 136 (6.06) | 153 (7.43) | |
| Non-Hispanic White | 2406 (70.76) | 464 (57.92) | 594 (70.77) | 666 (75.70) | 682 (75.18) | |
| Other race (including multi-racial and other Hispanic) | 1243 (11.82) | 327 (15.36) | 290 (10.78) | 312 (10.61) | 314 (11.35) | |
| Body mass index, kg/m2, n (weighted %) | 0.08 | |||||
| <25 | 1713 (31.19) | 445 (32.52) | 447 (32.75) | 430 (32.53) | 391 (27.71) | |
| 25–29.9 | 1800 (34.96) | 440 (35.48) | 413 (32.73) | 488 (35.88) | 459 (35.63) | |
| ≥30 | 1914 (33.85) | 472 (32.00) | 497 (34.52) | 438 (31.59) | 507 (36.66) | |
| Education level, n (weighted %) | <0.0001 | |||||
| Above | 863 (11.14) | 281 (14.64) | 220 (11.62) | 189 (10.29) | 173 (9.06) | |
| High school | 1126 (19.50) | 313 (23.37) | 288 (19.71) | 257 (18.07) | 268 (17.95) | |
| Below | 3438 (69.36) | 763 (61.99) | 849 (68.66) | 910 (71.64) | 916 (73.00) | |
| Poverty to income ratio, n (weighted %) | <0.0001 | |||||
| <1.3 | 1642 (20.53) | 526 (30.80) | 394 (19.34) | 349 (17.16) | 373 (17.47) | |
| 1.3–3.49 | 1882 (34.33) | 458 (34.11) | 491 (35.80) | 472 (34.19) | 461 (33.36) | |
| ≥3.5 | 1903 (45.14) | 373 (35.09) | 472 (44.86) | 535 (48.65) | 523 (49.16) | |
| Smoking status, n (weighted %) | 0.002 | |||||
| Former smoker | 1268 (24.43) | 250 (18.52) | 304 (24.27) | 353 (26.46) | 361 (26.83) | |
| Non-smoker | 3126 (57.57) | 838 (61.35) | 818 (59.82) | 766 (57.56) | 704 (53.06) | |
| Current smoker | 1033 (17.99) | 269 (20.13) | 235 (15.91) | 237 (15.98) | 292 (20.11) | |
| Alcohol status, n (weighted %) | <0.0001 | |||||
| Former | 821 (12.56) | 240 (15.40) | 220 (13.60) | 186 (11.73) | 175 (10.45) | |
| Never | 666 (9.51) | 220 (13.86) | 182 (10.95) | 146 (7.65) | 118 (6.98) | |
| Mild | 1947 (37.55) | 454 (32.26) | 499 (39.17) | 560 (44.96) | 434 (33.04) | |
| Moderate | 904 (18.95) | 208 (18.07) | 212 (17.23) | 224 (17.99) | 260 (21.88) | |
| Heavy | 1089 (21.44) | 235 (20.42) | 244 (19.04) | 240 (17.66) | 370 (27.66) | |
| Physical activity, MET min/wk, n (weighted %) | <0.001 | |||||
| Q1 [40, 800] | 1373 (23.77) | 400 (28.06) | 390 (27.34) | 312 (21.86) | 271 (19.53) | |
| Q2 (800, 1920] | 1341 (25.16) | 328 (23.37) | 330 (27.41) | 363 (26.76) | 320 (23.03) | |
| Q3 (1920, 5040] | 1378 (26.09) | 323 (25.65) | 351 (24.30) | 349 (25.75) | 355 (28.20) | |
| Q4 (5040, 59,040] | 1335 (24.99) | 306 (22.92) | 286 (20.95) | 332 (25.62) | 411 (29.24) | |
| Daily total intake of protein, g/day, n (weighted %) | <0.0001 | |||||
| Q1 [0, 53.57] | 1358 (23.48) | 602 (44.12) | 338 (23.95) | 246 (17.86) | 172 (13.83) | |
| Q2 (53.57, 75.575] | 1356 (24.65) | 400 (28.96) | 380 (27.58) | 316 (24.48) | 260 (19.33) | |
| Q3 (75.575, 102.52] | 1357 (26.58) | 227 (17.84) | 371 (29.89) | 416 (31.28) | 343 (25.58) | |
| Q4 (102.52, 474.19] | 1356 (25.29) | 128 (9.08) | 268 (18.58) | 378 (26.39) | 582 (41.26) | |
| Daily total intake of energy, kcal/day, n (weighted %) | <0.0001 | |||||
| Q1 [93, 1498.5] | 1357 (22.43) | 479 (33.03) | 354 (22.48) | 301 (20.12) | 223 (17.09) | |
| Q2 (1498.5, 2007] | 1358 (24.93) | 356 (26.41) | 368 (28.69) | 352 (26.61) | 282 (19.18) | |
| Q3 (2007, 2688.5] | 1355 (26.13) | 287 (21.73) | 359 (27.69) | 351 (26.61) | 358 (27.44) | |
| Q4 (2688.5, 12,108] | 1357 (26.52) | 235 (18.82) | 276 (21.14) | 352 (26.66) | 494 (36.29) | |
| Daily total intake of carbohydrates, g/day, n (weighted %) | <0.0001 | |||||
| Q1 [3.8, 175.005] | 1357 (23.87) | 444 (30.74) | 338 (24.69) | 311 (22.14) | 264 (19.98) | |
| Q2 (175.005, 242.16] | 1356 (24.58) | 348 (25.73) | 356 (25.87) | 357 (26.23) | 295 (21.16) | |
| Q3 (242.16, 326.935] | 1357 (26.04) | 323 (24.11) | 374 (28.50) | 322 (25.62) | 338 (25.72) | |
| Q4 (326.935, 1362.55] | 1357 (25.51) | 242 (19.43) | 289 (20.94) | 366 (26.01) | 460 (33.14) | |
| Daily total intake of sugars, g/day, n (weighted %) | 0.07 | |||||
| Q1 [0.1, 61.08] | 1357 (24.34) | 382 (25.28) | 348 (25.98) | 314 (23.89) | 313 (22.72) | |
| Q2 (61.08, 99.43] | 1357 (24.73) | 343 (25.24) | 331 (24.28) | 367 (27.06) | 316 (22.61) | |
| Q3 (99.43, 149.34] | 1356 (25.25) | 354 (26.17) | 360 (26.14) | 334 (25.00) | 308 (24.11) | |
| Q4 (149.34, 1048.48] | 1357 (25.68) | 278 (23.32) | 318 (23.60) | 341 (24.05) | 420 (30.57) | |
| Daily total intake of fat, g/day, n (weighted %) | <0.0001 | |||||
| Q1 [0.33, 50] | 1357 (22.37) | 437 (29.39) | 353 (22.47) | 308 (20.57) | 259 (19.03) | |
| Q2 (50, 74.58] | 1356 (24.59) | 377 (28.66) | 354 (26.01) | 338 (23.96) | 287 (21.13) | |
| Q3 (74.58,105.715] | 1357 (26.87) | 286 (22.34) | 369 (30.06) | 347 (28.80) | 355 (25.59) | |
| Q4 (105.715,548.38] | 1357 (26.17) | 257 (19.61) | 281 (21.46) | 363 (26.67) | 456 (34.25) | |
| Diabetes, n (weighted %) | 0.55 | |||||
| No | 4617 (88.90) | 1121 (88.10) | 1166 (88.65) | 1158 (88.67) | 1172 (89.87) | |
| Yes | 810 (11.10) | 236 (11.90) | 191 (11.35) | 198 (11.33) | 185 (10.13) | |
| Hypertension, n (weighted %) | 0.62 | |||||
| No | 3334 (64.85) | 812 (63.38) | 807 (64.06) | 838 (64.93) | 877 (66.45) | |
| Yes | 2093 (35.15) | 545 (36.62) | 550 (35.94) | 518 (35.07) | 480 (33.55) | |
| Hyperlipidemia, n (weighted %) | 0.02 | |||||
| No | 1814 (32.45) | 480 (36.00) | 417 (29.25) | 432 (30.42) | 485 (34.52) | |
| Yes | 3613 (67.55) | 877 (64.00) | 940 (70.75) | 924 (69.58) | 872 (65.48) | |
| Cancer, n (weighted %) | 0.05 | |||||
| No | 4951 (89.93) | 1252 (92.47) | 1228 (89.02) | 1211 (87.97) | 1260 (90.72) | |
| Yes | 476 (10.07) | 105 (7.53) | 129 (10.98) | 145 (12.03) | 97 (9.28) |
| Crude Model | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Daily Total Intake of Water (g/day) | 95%CI | p | 95%CI | p | 95%CI | p |
| Q1 | ref | ref | ref | |||
| Q2 | 0.01 (−0.02, 0.03) | 0.63 | 0.01 (−0.01, 0.02) | 0.93 | 0.01 (−0.01, 0.02) | 0.48 |
| Q3 | 0.03 (0.01, 0.05) | 0.01 | 0 (−0.02, 0.02) | 0.17 | 0 (−0.02, 0.02) | 0.87 |
| Q4 | 0.07 (0.04, 0.09) | <0.0001 | 0.01 (−0.01, 0.03) | 0.46 | 0.01 (0.00, 0.03) | 0.15 |
| p for trend | <0.0001 | 0.25 | 0.21 | |||
| Gender: Male | Crude Model | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| Daily total intake of water (g/day) | 95%CI | p | 95%CI | p | 95%CI | p |
| Q1 | ref | ref | ref | |||
| Q2 | 0.02 (−0.02, 0.05) | 0.34 | 0.01 (−0.01, 0.04) | 0.34 | 0.01 (−0.01, 0.04) | 0.31 |
| Q3 | 0.01 (−0.02, 0.05) | 0.44 | 0.01 (−0.01, 0.04) | 0.28 | 0.02 (−0.01, 0.04) | 0.27 |
| Q4 | 0.03 (−0.01, 0.07) | 0.10 | 0.02 (−0.01, 0.05) | 0.15 | 0.02 (−0.01, 0.05) | 0.13 |
| p for trend | 0.13 | 0.16 | 0.15 | |||
| Gender: Female | Crude Model | Model 1 | Model 2 | |||
| Daily total intake of water (g/day) | 95%CI | p | 95%CI | p | 95%CI | p |
| Q1 | ref | ref | ref | |||
| Q2 | −0.02 (−0.05, 0.00) | 0.08 | 0 (−0.02, 0.01) | 0.77 | 0 (−0.02, 0.01) | 0.62 |
| Q3 | −0.01 (−0.03, 0.01) | 0.48 | −0.01 (−0.03, 0.01) | 0.20 | −0.01 (−0.03, 0.01) | 0.25 |
| Q4 | −0.01 (−0.03, 0.01) | 0.42 | 0 (−0.02, 0.02) | 0.95 | 0 (−0.02, 0.02) | 0.99 |
| p for trend | 0.71 | 0.65 | 0.77 | |||
| Q1 | Q2 | p | Q3 | p | Q4 | p | p for Trend | p for Interaction | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | 0.2 | ||||||||
| Female | ref | 0 (−0.02, 0.01) | 0.62 | −0.01 (−0.03, 0.01) | 0.25 | 0 (−0.02, 0.02) | 0.99 | 0.59 | |
| Male | ref | 0.01 (−0.02, 0.04) | 0.48 | 0.01 (−0.01, 0.04) | 0.31 | 0.02 (−0.01, 0.05) | 0.22 | 0.69 | |
| Age | 0.44 | ||||||||
| 20–29 | ref | −0.01 (−0.05, 0.02) | 0.49 | −0.01 (−0.06, 0.03) | 0.51 | 0.01 (−0.03, 0.05) | 0.62 | 0.53 | |
| 30–39 | ref | −0.01 (−0.04, 0.01) | 0.3 | −0.01 (−0.03, 0.02) | 0.61 | 0 (−0.04, 0.03) | 0.94 | 0.46 | |
| 40–49 | ref | 0.01 (−0.02, 0.04) | 0.54 | 0.01 (−0.02, 0.04) | 0.44 | 0.02 (−0.01, 0.06) | 0.21 | 0.5 | |
| 50–59 | ref | −0.01 (−0.06, 0.04) | 0.72 | −0.04 (−0.08, 0.01) | 0.15 | −0.03 (−0.07, 0.02) | 0.22 | 0.21 | |
| ≥60 | ref | 0.02 (0.00, 0.05) | 0.07 | 0.02 (−0.01, 0.05) | 0.16 | 0.03 (0.00, 0.06) | 0.09 | 0.6 | |
| Race | 0.24 | ||||||||
| Non-Hispanic Black | ref | 0 (−0.03, 0.03) | 0.82 | 0 (−0.03, 0.04) | 0.92 | 0 (−0.05, 0.04) | 0.87 | 0.81 | |
| Mexican American | ref | 0.03 (−0.02, 0.08) | 0.23 | 0.02 (−0.03, 0.07) | 0.47 | 0.01 (−0.04, 0.05) | 0.81 | 0.91 | |
| Non-Hispanic White | ref | 0 (−0.02, 0.01) | 0.62 | −0.01 (−0.03, 0.01) | 0.42 | 0.01 (−0.01, 0.03) | 0.32 | 0.18 | |
| Other race | ref | 0.03 (0.00, 0.06) | 0.03 | 0.03 (0.00, 0.07) | 0.07 | 0.02 (−0.03, 0.06) | 0.41 | 0.73 | |
| Body mass index | 0.18 | ||||||||
| <25 | ref | −0.01 (−0.04, 0.02) | 0.57 | 0 (−0.04, 0.04) | 0.94 | 0.01 (−0.02, 0.05) | 0.46 | 0.34 | |
| 25–29.9 | ref | 0.01 (−0.01, 0.04) | 0.27 | 0 (−0.03, 0.02) | 0.74 | 0.02 (0.00, 0.04) | 0.1 | 0.24 | |
| ≥30 | ref | 0 (−0.02, 0.03) | 0.67 | 0 (−0.02, 0.03) | 0.75 | 0 (−0.02, 0.02) | 0.94 | 0.68 | |
| Education level | 0.54 | ||||||||
| Above | ref | 0.01 (−0.03, 0.06) | 0.54 | 0.02 (−0.02, 0.06) | 0.32 | 0.02 (−0.03, 0.07) | 0.53 | 0.9 | |
| High school | ref | 0.02 (−0.01, 0.05) | 0.19 | 0.01 (−0.03, 0.04) | 0.68 | 0.03 (0.00, 0.06) | 0.03 | 0.08 | |
| Below | ref | −0.01 (−0.03, 0.02) | 0.6 | −0.01 (−0.03, 0.02) | 0.68 | 0 (−0.02, 0.02) | 0.88 | 0.81 | |
| Poverty to income ratio | 0.39 | ||||||||
| <1.3 | ref | 0.03 (0.00, 0.06) | 0.07 | 0.02 (−0.01, 0.05) | 0.12 | 0.03 (0.00, 0.05) | 0.06 | 0.73 | |
| 1.3–3.49 | ref | −0.01 (−0.04, 0.02) | 0.44 | −0.01 (−0.03, 0.02) | 0.56 | 0.02 (−0.01, 0.05) | 0.22 | 0.06 | |
| ≥3.5 | ref | 0 (−0.02, 0.03) | 0.9 | −0.01 (−0.03, 0.02) | 0.72 | −0.01 (−0.03, 0.02) | 0.68 | 0.74 | |
| Smoke status | 0.23 | ||||||||
| Former smoker | ref | 0 (−0.02, 0.02) | 0.68 | 0 (−0.02, 0.02) | 0.87 | 0.01 (−0.01, 0.03) | 0.43 | 0.67 | |
| Non-smoker | ref | 0.02 (−0.01, 0.05) | 0.24 | 0.03 (0.00, 0.06) | 0.03 | 0.04 (0.01, 0.06) | 0.01 | 0.14 | |
| Current smoker | ref | −0.01 (−0.05, 0.04) | 0.71 | −0.02 (−0.07, 0.02) | 0.26 | 0 (−0.04, 0.04) | 0.99 | 0.19 | |
| Alcohol status | 0.15 | ||||||||
| Former | ref | 0 (−0.04, 0.03) | 0.75 | 0.02 (−0.02, 0.06) | 0.25 | 0.03 (−0.01, 0.06) | 0.11 | 0.94 | |
| Never | ref | 0.02 (−0.01, 0.05) | 0.18 | 0 (−0.03, 0.04) | 0.8 | 0.04 (0.01, 0.07) | 0.02 | 0.1 | |
| Mild | ref | 0.02 (−0.01, 0.06) | 0.16 | 0 (−0.03, 0.03) | 0.78 | 0.01 (−0.02, 0.04) | 0.58 | 0.13 | |
| Moderate | ref | −0.03 (−0.07, 0.01) | 0.09 | −0.03 (−0.06, 0.00) | 0.07 | −0.01 (−0.05, 0.03) | 0.47 | 0.26 | |
| Heavy | ref | 0.01 (−0.03, 0.05) | 0.54 | 0.02 (−0.02, 0.07) | 0.32 | 0.02 (−0.02, 0.06) | 0.33 | 0.76 | |
| Physical activity | 0.09 | ||||||||
| Q1 | ref | 0.04 (0.01, 0.07) | 0.02 | 0.01 (−0.02, 0.03) | 0.67 | 0.03 (0.00, 0.06) | 0.08 | 0.02 | |
| Q2 | ref | −0.01 (−0.04, 0.01) | 0.25 | −0.02 (−0.05, 0.01) | 0.21 | −0.03 (−0.06, 0.01) | 0.1 | 0.38 | |
| Q3 | ref | 0.01 (−0.02, 0.04) | 0.6 | 0 (−0.04, 0.03) | 0.98 | 0.01 (−0.02, 0.04) | 0.51 | 0.74 | |
| Q4 | ref | −0.01 (−0.05, 0.03) | 0.67 | 0.02 (−0.02, 0.06) | 0.3 | 0.02 (−0.02, 0.06) | 0.27 | 0.78 | |
| Daily total intake of protein | 0.65 | ||||||||
| Q1 | ref | −0.01 (−0.03, 0.02) | 0.65 | 0 (−0.03, 0.03) | 0.99 | 0 (−0.03, 0.03) | 0.95 | 1 | |
| Q2 | ref | 0.02 (−0.01, 0.04) | 0.27 | 0.02 (−0.01, 0.06) | 0.17 | 0.02 (−0.01, 0.05) | 0.16 | 0.93 | |
| Q3 | ref | 0 (−0.03, 0.04) | 0.82 | −0.02 (−0.06, 0.03) | 0.44 | −0.01 (−0.04, 0.03) | 0.68 | 0.71 | |
| Q4 | ref | −0.03 (−0.08, 0.01) | 0.11 | −0.02 (−0.07, 0.03) | 0.4 | −0.01 (−0.05, 0.04) | 0.75 | 0.38 | |
| Daily total intake of energy | 0.57 | ||||||||
| Q1 | ref | 0 (−0.03, 0.03) | 0.81 | 0.01 (−0.03, 0.04) | 0.76 | 0.01 (−0.02, 0.04) | 0.43 | 0.39 | |
| Q2 | ref | 0.01 (−0.03, 0.04) | 0.64 | −0.02 (−0.05, 0.01) | 0.3 | −0.02 (−0.05, 0.02) | 0.37 | 0.21 | |
| Q3 | ref | 0.02 (−0.01, 0.05) | 0.16 | 0.01 (−0.02, 0.05) | 0.48 | 0.03 (0.00, 0.07) | 0.05 | 0.09 | |
| Q4 | ref | −0.01 (−0.04, 0.02) | 0.48 | 0.01 (−0.02, 0.05) | 0.53 | 0.02 (−0.02, 0.05) | 0.42 | 0.02 | |
| Daily total intake of carbohydrates | 0.65 | ||||||||
| Q1 | ref | −0.01 (−0.04, 0.01) | 0.31 | 0 (−0.03, 0.03) | 0.76 | −0.01 (−0.04, 0.03) | 0.72 | 0.56 | |
| Q2 | ref | 0.02 (−0.01, 0.05) | 0.29 | 0 (−0.03, 0.03) | 0.95 | 0.02 (−0.01, 0.05) | 0.24 | 0.17 | |
| Q3 | ref | 0.01 (−0.02, 0.04) | 0.68 | −0.01 (−0.03, 0.02) | 0.53 | 0 (−0.03, 0.03) | 0.95 | 0.22 | |
| Q4 | ref | 0.01 (−0.03, 0.05) | 0.61 | 0.02 (−0.02, 0.06) | 0.29 | 0.03 (−0.01, 0.07) | 0.18 | 0.14 | |
| Daily total intake of sugars | 0.77 | ||||||||
| Q1 | ref | 0 (−0.03, 0.03) | 0.97 | −0.02 (−0.05, 0.02) | 0.29 | 0.01 (−0.03, 0.05) | 0.62 | 0.06 | |
| Q2 | ref | 0.01 (−0.03, 0.04) | 0.73 | −0.01 (−0.03, 0.02) | 0.67 | −0.01 (−0.05, 0.03) | 0.48 | 0.53 | |
| Q3 | ref | 0.01 (−0.02, 0.03) | 0.6 | 0.01 (−0.02, 0.03) | 0.57 | 0.01 (−0.02, 0.04) | 0.41 | 0.79 | |
| Q4 | ref | 0.01 (−0.03, 0.05) | 0.62 | 0.02 (−0.03, 0.06) | 0.39 | 0.03 (−0.02, 0.07) | 0.22 | 0.73 | |
| Daily total intake of fat | 0.08 | ||||||||
| Q1 | ref | 0.01 (−0.02, 0.04) | 0.34 | 0.01 (−0.02, 0.03) | 0.61 | 0.03 (0.00, 0.06) | 0.04 | 0.08 | |
| Q2 | ref | 0.02 (−0.02, 0.05) | 0.34 | −0.02 (−0.05, 0.02) | 0.31 | 0.01 (−0.03, 0.04) | 0.79 | 0.55 | |
| Q3 | ref | −0.01 (−0.04, 0.03) | 0.7 | −0.01 (−0.04, 0.02) | 0.6 | −0.02 (−0.05, 0.02) | 0.33 | 0.68 | |
| Q4 | ref | −0.01 (−0.04, 0.02) | 0.54 | 0.01 (−0.02, 0.05) | 0.44 | 0.02 (−0.01, 0.05) | 0.19 | 0.61 | |
| Diabetes | 0.5 | ||||||||
| No | ref | 0 (−0.02, 0.02) | 0.8 | 0 (−0.02, 0.02) | 0.9 | 0.01 (−0.01, 0.03) | 0.26 | 0.37 | |
| Yes | ref | 0.02 (0.00, 0.04) | 0.12 | 0.01 (−0.03, 0.05) | 0.57 | 0.01 (−0.02, 0.04) | 0.38 | 0.92 | |
| Hypertension | 0.44 | ||||||||
| No | ref | −0.01 (−0.03, 0.01) | 0.53 | 0 (−0.03, 0.02) | 0.8 | 0.01 (−0.02, 0.03) | 0.65 | 0.96 | |
| Yes | ref | 0.02 (−0.01, 0.06) | 0.19 | 0.01 (−0.02, 0.04) | 0.67 | 0.02 (−0.01, 0.05) | 0.22 | 0.3 | |
| Hyperlipidemia | 0.83 | ||||||||
| No | ref | 0.01 (−0.01, 0.04) | 0.36 | 0.01 (−0.01, 0.04) | 0.33 | 0.02 (−0.01, 0.05) | 0.24 | 0.7 | |
| Yes | ref | 0 (−0.02, 0.02) | 0.82 | −0.01 (−0.03, 0.01) | 0.52 | 0.01 (−0.01, 0.02) | 0.51 | 0.58 | |
| Cancer | 0.53 | ||||||||
| No | ref | 0 (−0.01, 0.02) | 0.57 | 0 (−0.02, 0.02) | 0.85 | 0.01 (−0.01, 0.03) | 0.28 | 0.67 | |
| Yes | ref | 0 (−0.04, 0.04) | 0.9 | 0.03 (−0.02, 0.08) | 0.21 | 0.03 (0.00, 0.07) | 0.07 | 0.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, D.; Qu, C.; Huang, P.; Geng, X.; Zhang, J.; Shen, Y.; Rao, Z.; Zhao, J. Water Intake and Handgrip Strength in US Adults: A Cross-Sectional Study Based on NHANES 2011–2014 Data. Nutrients 2023, 15, 4477. https://doi.org/10.3390/nu15204477
Wu D, Qu C, Huang P, Geng X, Zhang J, Shen Y, Rao Z, Zhao J. Water Intake and Handgrip Strength in US Adults: A Cross-Sectional Study Based on NHANES 2011–2014 Data. Nutrients. 2023; 15(20):4477. https://doi.org/10.3390/nu15204477
Chicago/Turabian StyleWu, Dongzhe, Chaoyi Qu, Peng Huang, Xue Geng, Jianhong Zhang, Yulin Shen, Zhijian Rao, and Jiexiu Zhao. 2023. "Water Intake and Handgrip Strength in US Adults: A Cross-Sectional Study Based on NHANES 2011–2014 Data" Nutrients 15, no. 20: 4477. https://doi.org/10.3390/nu15204477
APA StyleWu, D., Qu, C., Huang, P., Geng, X., Zhang, J., Shen, Y., Rao, Z., & Zhao, J. (2023). Water Intake and Handgrip Strength in US Adults: A Cross-Sectional Study Based on NHANES 2011–2014 Data. Nutrients, 15(20), 4477. https://doi.org/10.3390/nu15204477