
Maternal Urinary Iodine Concentration during Pregnancy and Its Impact on Child Growth and Neurodevelopment: An 11-Year Follow-Up Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
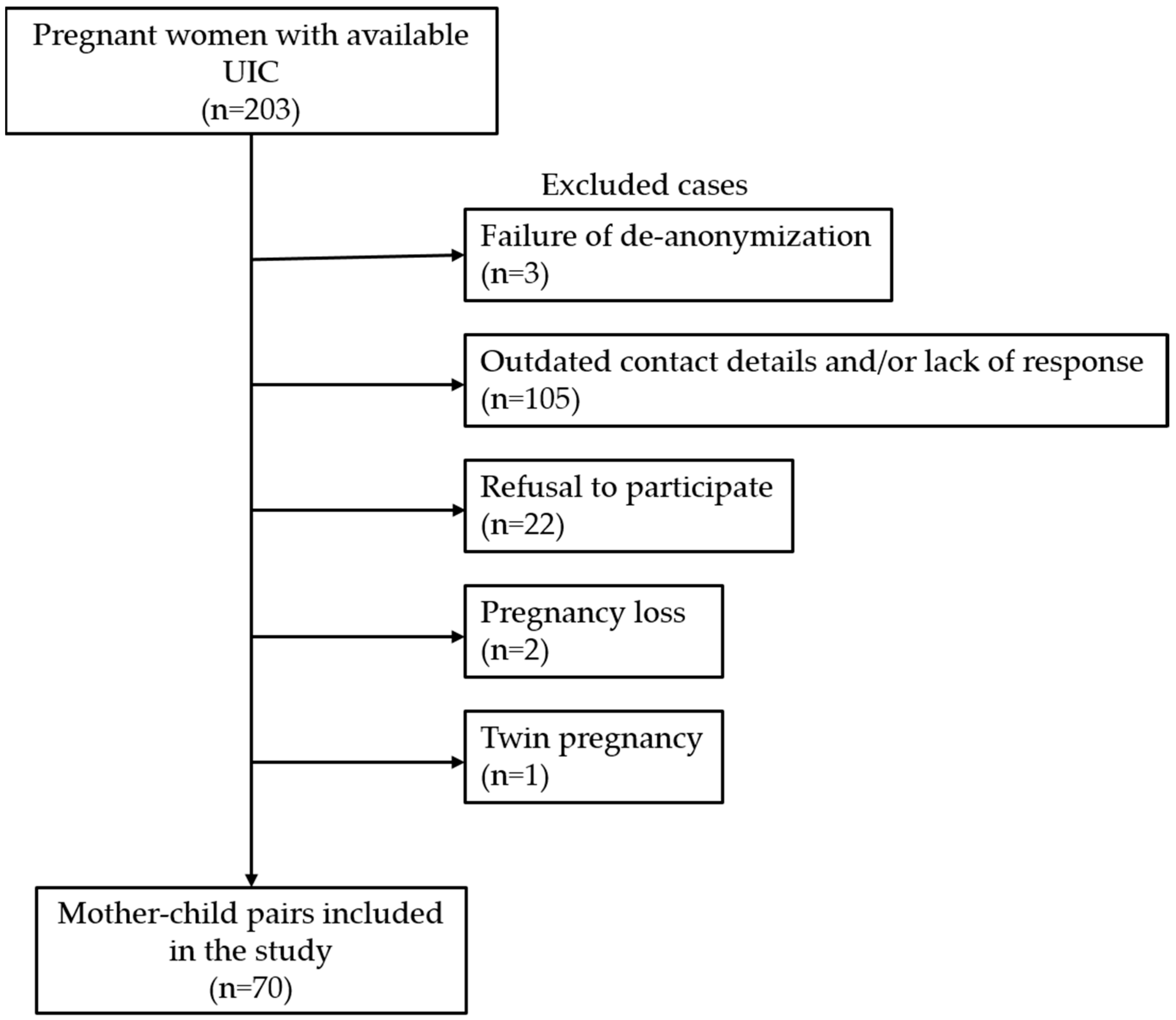
2.1. Subjects
2.2. Pregnancy and Neonatal Parameters
2.3. Socioeconomic Parameters
2.4. Assessment of Child Development
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iannuzzo, G.; Campanozzi, A.; Trevisani, V.; Rutigliano, I.; Abate, V.; Rendina, D.; De Filippo, G. Iodine Requirements in Pediatrics: From Fetal Life to Adolescence. Front. Endocrinol. 2022, 13, 929176. [Google Scholar] [CrossRef]
- Rodriguez-Diaz, E.; Pearce, E.N. Iodine status and supplementation before, during, and after pregnancy. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101430. [Google Scholar] [CrossRef]
- Patriota, E.S.O.; Lima, I.C.C.; Nilson, E.A.F.; Franceschini, S.C.C.; Goncalves, V.S.S.; Pizato, N. Prevalence of insufficient iodine intake in pregnancy worldwide: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2022, 76, 703–715. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization/United Nations Children’s Fund/International Council for the Control of Iodine Deficiency Disorders. Assessment of the Iodine Deficiency Disorders and Monitoring Their Elimination. A Guide for Programme Managers, 3rd ed.; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Megier, C.; Dumery, G.; Luton, D. Iodine and Thyroid Maternal and Fetal Metabolism during Pregnancy. Metabolites 2023, 13, 633. [Google Scholar] [CrossRef] [PubMed]
- Toloza, F.J.K.; Motahari, H.; Maraka, S. Consequences of Severe Iodine Deficiency in Pregnancy: Evidence in Humans. Front. Endocrinol. 2020, 11, 409. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Zimmermann, M.B. The Prevention of Iodine Deficiency: A History. Thyroid 2023, 33, 143–149. [Google Scholar] [CrossRef]
- Zimmermann, M.B. The remarkable impact of iodisation programmes on global public health. Proc. Nutr. Soc. 2023, 82, 113–119. [Google Scholar] [CrossRef]
- Van Mil, N.H.; Tiemeier, H.; Bongers-Schokking, J.J.; Ghassabian, A.; Hofman, A.; Hooijkaas, H.; Jaddoe, V.W.; de Muinck Keizer-Schrama, S.M.; Steegers, E.A.; Visser, T.J.; et al. Low urinary iodine excretion during early pregnancy is associated with alterations in executive functioning in children. J. Nutr. 2012, 142, 2167–2174. [Google Scholar] [CrossRef]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Hynes, K.L.; Otahal, P.; Hay, I.; Burgess, J.R. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. J. Clin. Endocrinol. Metab. 2013, 98, 1954–1962. [Google Scholar] [CrossRef]
- Hynes, K.L.; Otahal, P.; Burgess, J.R.; Oddy, W.H.; Hay, I. Reduced Educational Outcomes Persist into Adolescence Following Mild Iodine Deficiency in Utero, Despite Adequacy in Childhood: 15-Year Follow-Up of the Gestational Iodine Cohort Investigating Auditory Processing Speed and Working Memory. Nutrients 2017, 9, 1354. [Google Scholar] [CrossRef] [PubMed]
- Murcia, M.; Espada, M.; Julvez, J.; Llop, S.; Lopez-Espinosa, M.J.; Vioque, J.; Basterrechea, M.; Riano, I.; Gonzalez, L.; Alvarez-Pedrerol, M.; et al. Iodine intake from supplements and diet during pregnancy and child cognitive and motor development: The INMA Mother and Child Cohort Study. J. Epidemiol. Community Health 2018, 72, 216–222. [Google Scholar] [CrossRef]
- Markhus, M.W.; Dahl, L.; Moe, V.; Abel, M.H.; Brantsaeter, A.L.; Oyen, J.; Meltzer, H.M.; Stormark, K.M.; Graff, I.E.; Smith, L.; et al. Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood. Nutrients 2018, 10, 1270. [Google Scholar] [CrossRef]
- Murcia, M.; Rebagliato, M.; Iniguez, C.; Lopez-Espinosa, M.J.; Estarlich, M.; Plaza, B.; Barona-Vilar, C.; Espada, M.; Vioque, J.; Ballester, F. Effect of iodine supplementation during pregnancy on infant neurodevelopment at 1 year of age. Am. J. Epidemiol. 2011, 173, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Rebagliato, M.; Murcia, M.; Alvarez-Pedrerol, M.; Espada, M.; Fernandez-Somoano, A.; Lertxundi, N.; Navarrete-Munoz, E.M.; Forns, J.; Aranbarri, A.; Llop, S.; et al. Iodine supplementation during pregnancy and infant neuropsychological development. INMA Mother and Child Cohort Study. Am. J. Epidemiol. 2013, 177, 944–953. [Google Scholar] [CrossRef]
- Ghassabian, A.; Steenweg-de Graaff, J.; Peeters, R.P.; Ross, H.A.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; White, T.; Tiemeier, H. Maternal urinary iodine concentration in pregnancy and children’s cognition: Results from a population-based birth cohort in an iodine-sufficient area. BMJ Open 2014, 4, e005520. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Brandlistuen, R.E.; Caspersen, I.H.; Aase, H.; Torheim, L.E.; Meltzer, H.M.; Brantsaeter, A.L. Language delay and poorer school performance in children of mothers with inadequate iodine intake in pregnancy: Results from follow-up at 8 years in the Norwegian Mother and Child Cohort Study. Eur. J. Nutr. 2019, 58, 3047–3058. [Google Scholar] [CrossRef]
- Zhou, S.J.; Condo, D.; Ryan, P.; Skeaff, S.A.; Howell, S.; Anderson, P.J.; McPhee, A.J.; Makrides, M. Association Between Maternal Iodine Intake in Pregnancy and Childhood Neurodevelopment at Age 18 Months. Am. J. Epidemiol. 2019, 188, 332–338. [Google Scholar] [CrossRef]
- Threapleton, D.E.; Snart, C.J.P.; Keeble, C.; Waterman, A.H.; Taylor, E.; Mason, D.; Reid, S.; Azad, R.; Hill, L.J.B.; Meadows, S.; et al. Maternal iodine status in a multi-ethnic UK birth cohort: Associations with child cognitive and educational development. Paediatr. Perinat. Epidemiol. 2021, 35, 236–246. [Google Scholar] [CrossRef]
- Kampouri, M.; Tofail, F.; Rahman, S.M.; Gustin, K.; Vahter, M.; Kippler, M. Gestational and childhood urinary iodine concentrations and children’s cognitive function in a longitudinal mother-child cohort in rural Bangladesh. Int. J. Epidemiol. 2023, 52, 144–155. [Google Scholar] [CrossRef]
- Croce, L.; Chiovato, L.; Tonacchera, M.; Petrosino, E.; Tanda, M.L.; Moleti, M.; Magri, F.; Olivieri, A.; Pearce, E.N.; Rotondi, M. Iodine status and supplementation in pregnancy: An overview of the evidence provided by meta-analyses. Rev. Endocr. Metab. Disord. 2023, 24, 241–250. [Google Scholar] [CrossRef]
- Nguyen, C.T. An update: Maternal iodine supplementation, thyroid function tests, and child neurodevelopmental outcomes. Curr. Opin. Endocrinol. Diabetes Obes. 2023, 30, 265–272. [Google Scholar] [CrossRef]
- Levie, D.; Korevaar, T.I.M.; Bath, S.C.; Murcia, M.; Dineva, M.; Llop, S.; Espada, M.; van Herwaarden, A.E.; de Rijke, Y.B.; Ibarluzea, J.M.; et al. Association of Maternal Iodine Status with Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019, 104, 5957–5967. [Google Scholar] [CrossRef]
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Jacome de Castro, J.; Carrilho, F.; Oliveira, M.J.; Reguengo, H.; et al. Iodine intake in Portuguese pregnant women: Results of a countrywide study. Eur. J. Endocrinol. 2010, 163, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Limbert, E.; Prazeres, S.; Sao Pedro, M.; Madureira, D.; Miranda, A.; Ribeiro, M.; Carrilho, F.; Jacome de Castro, J.; Lopes, M.S.; Cardoso, J.; et al. Iodine intake in Portuguese school children. Acta Med. Port. 2012, 25, 29–36. [Google Scholar]
- Lopes, C.A.; Prazeres, S.; Martinez-de-Oliveira, J.; Limbert, E.; Lemos, M.C. Iodine Supplementation in Pregnancy in an Iodine-Deficient Region: A Cross-Sectional Survey. Nutrients 2022, 14, 1393. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde (DGS). Orientação da Direção-Geral da Saúde. Aporte de Iodo em Mulheres na Preconceção, Gravidez e Amamentação (Iodine Intake in Preconception, Pregnancy and Breastfeeding Women). Orientação nº 011/2013 de 26/08/2013. Available online: http://www.dgs.pt/?cr=24648 (accessed on 29 September 2023).
- Gnat, D.; Dunn, A.D.; Chaker, S.; Delange, F.; Vertongen, F.; Dunn, J.T. Fast colorimetric method for measuring urinary iodine. Clin. Chem. 2003, 49, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Von Stumm, S.; Plomin, R. Socioeconomic status and the growth of intelligence from infancy through adolescence. Intelligence 2015, 48, 30–36. [Google Scholar] [CrossRef] [PubMed]
- McCrory, C.; O’Leary, N.; Fraga, S.; Ribeiro, A.I.; Barros, H.; Kartiosuo, N.; Raitakari, O.; Kivimaki, M.; Vineis, P.; Layte, R.; et al. Socioeconomic differences in children’s growth trajectories from infancy to early adulthood: Evidence from four European countries. J. Epidemiol. Community Health 2017, 71, 981–989. [Google Scholar] [CrossRef]
- Samson, L.; Hircsu, I.; Katko, M.; Bodor, M.; Gazdag, A.; Gazso, A.A.; Kovacs, B.; Posta, J.; Balogh, E.; Mocsary, P.; et al. Lower educational status interferes with maternal iodine intake during both pregnancy and lactation. Endocr. Connect. 2021, 10, 742–749. [Google Scholar] [CrossRef]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef] [PubMed]
- De Groot, L.; Abalovich, M.; Alexander, E.K.; Amino, N.; Barbour, L.; Cobin, R.H.; Eastman, C.J.; Lazarus, J.H.; Luton, D.; Mandel, S.J.; et al. Management of thyroid dysfunction during pregnancy and postpartum: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 2543–2565. [Google Scholar] [CrossRef]
- Monaghan, A.M.; Mulhern, M.S.; McSorley, E.M.; Strain, J.J.; Dyer, M.; van Wijngaarden, E.; Yeates, A.J. Associations between maternal urinary iodine assessment, dietary iodine intakes and neurodevelopmental outcomes in the child: A systematic review. Thyroid. Res. 2021, 14, 14. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Maternal UIC (µg/L) | ||||||
|---|---|---|---|---|---|---|
| All | <25 | 25–50 | 50–100 | 100–150 | >150 | |
| Number, n | 70 | 7 | 15 | 27 | 16 | 5 |
| Sex (M/F), n | 39/31 | 5/2 | 8/7 | 13/14 | 10/6 | 3/2 |
| Gestational age at iodine status (weeks), mean ± SD | 29.6 ± 9.3 | 27.0 ± 9.2 | 30.9 ± 9.6 | 27.2 ± 9.5 | 31.5 ± 9.7 | 35.0 ± 2.6 |
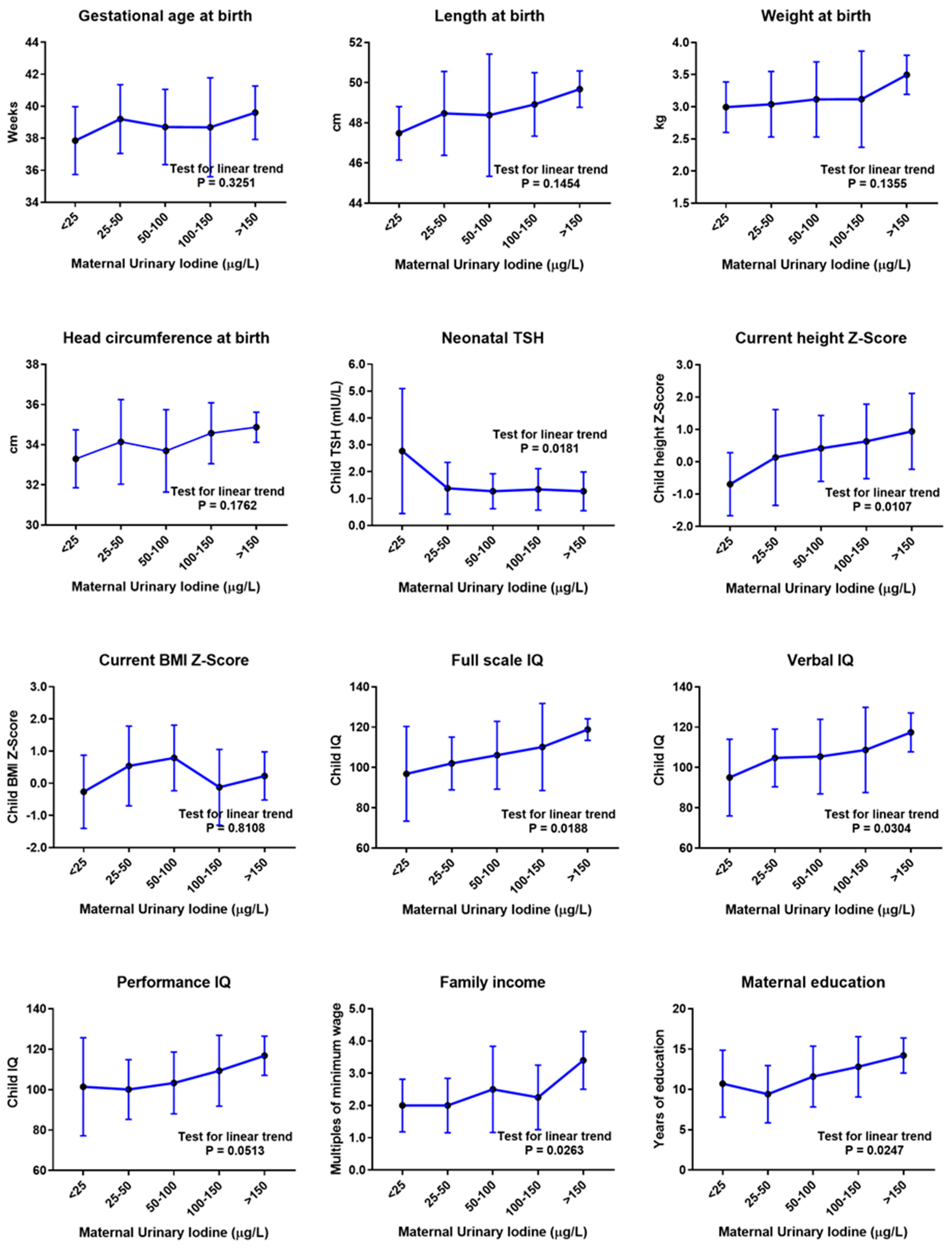
| Gestational age at birth (weeks), mean ± SD | 38.8 ± 2.4 | 37.9 ± 2.1 | 39.2 ± 2.1 | 38.7 ± 2.4 | 38.7 ± 3.1 | 39.6 ± 1.7 |
| Length at birth (cm), mean ± SD | 48.5 ± 2.3 | 47.5 ± 1.3 | 48.5 ± 2.1 | 48.4 ± 3.0 | 48.9 ± 1.6 | 49.7 ± 0.9 |
| Weight at birth (kg), mean ± SD | 3.11 ± 0.58 | 2.99 ± 0.39 | 3.04 ± 0.51 | 3.12 ± 0.58 | 3.12 ± 0.75 | 3.50 ± 0.30 |
| Head circumference at birth (cm), mean ± SD | 34.0 ± 1.9 | 33.3 ± 1.4 | 34.1 ± 2.1 | 33.7 ± 2.1 | 34.6 ± 1.5 | 34.9 ± 0.8 |
| Neonatal TSH (mIU/L), mean ± SD | 1.46 ± 1.09 | 2.77 ± 2.33 | 1.39 ± 0.96 | 1.27 ± 0.62 | 1.34 ± 0.77 | 1.27 ± 0.72 |
| Age at IQ evaluation (years), mean ± SD | 11.3 ± 0.7 | 11.4 ± 0.9 | 11.3 ± 0.8 | 11.3 ± 0.8 | 11.1 ± 0.7 | 10.9 ± 0.2 |
| Current height Z-score, mean ± SD | 0.33 ± 1.21 | −0.69 ± 0.98 | 0.13 ± 1.48 | 0.41 ± 1.02 | 0.63 ± 1.15 | 0.94 ± 1.17 |
| Current BMI Z-score, mean ± SD | 0.38 ± 1.15 | −0.27 ± 1.14 | 0.54 ± 1.24 | 0.79 ± 1.02 | −0.12 ± 1.18 | 0.23 ± 0.75 |
| Verbal IQ, mean ± SD | 105.8 ± 18.1 | 95.0 ± 19.0 | 104.7 ± 14.3 | 105.4 ± 18.5 | 108.7 ± 21.1 | 117.4 ± 9.6 |
| Performance IQ, mean ± SD | 104.8 ± 16.7 | 101.4 ± 24.3 | 100.1 ± 14.7 | 103.3 ± 15.3 | 109.4 ± 17.5 | 116.8 ± 9.7 |
| Full-scale IQ, mean ± SD | 106.1 ± 17.9 | 96.9 ± 23.5 | 102.0 ± 13.1 | 106.1 ± 16.9 | 110.2 ± 21.6 | 118.8 ± 5.4 |
| Family income (multiples of minimum wage), mean ± SD | 2.3 ± 1.1 | 2.0 ± 0.8 | 2.0 ± 0.9 | 2.5 ± 1.3 | 2.3 ± 1.0 | 3.4 ± 0.9 |
| Maternal education (years), mean ± SD | 11.6 ± 3.8 | 10.7 ± 4.2 | 9.4 ± 3.6 | 11.6 ± 3.8 | 12.8 ± 3.7 | 14.2 ± 2.4 |
| Independent Variables | ||
|---|---|---|
| Maternal UIC | Maternal Education | |
| Maternal UIC | - | β = 0.317 p = 0.018 * |
| Gestational age at birth | β = −0.046 p = 0.649 | β = 0.004 p = 0.967 |
| Length at birth | β = 0.112 p = 0.424 | β = 0.287 p = 0.033 * |
| Weight at birth | β = 0.035 p = 0.718 | β = −0.062 p = 0.528 |
| Head circumference at birth | β = 0.121 p = 0.217 | β = 0.040 p = 0.687 |
| Neonatal TSH | β = −0.175 p = 0.212 | β = −0.280 p = 0.038 * |
| Current height Z-score | β = 0.185 p = 0.167 | β = 0.394 p = 0.003 * |
| Current BMI Z-score | β = −0.132 p = 0.344 | β = −0.195 p = 0.176 |
| Verbal IQ | β = 0.135 p = 0.319 | β = 0.383 p = 0.004 * |
| Performance IQ | β = 0.156 p = 0.241 | β = 0.407 p = 0.002 * |
| Full-scale IQ | β = 0.173 p = 0.187 | β = 0.430 p = 0.001 * |
| Family income | β = 0.105 p = 0.413 | β = 0.478 p < 0.001 * |
| Maternal education | β = 0.212 p = 0.089 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, C.A.; Duarte, M.; Prazeres, S.; Carvalho, I.; Vilarinho, L.; Martinez-de-Oliveira, J.; Limbert, E.; Lemos, M.C. Maternal Urinary Iodine Concentration during Pregnancy and Its Impact on Child Growth and Neurodevelopment: An 11-Year Follow-Up Study. Nutrients 2023, 15, 4447. https://doi.org/10.3390/nu15204447
Lopes CA, Duarte M, Prazeres S, Carvalho I, Vilarinho L, Martinez-de-Oliveira J, Limbert E, Lemos MC. Maternal Urinary Iodine Concentration during Pregnancy and Its Impact on Child Growth and Neurodevelopment: An 11-Year Follow-Up Study. Nutrients. 2023; 15(20):4447. https://doi.org/10.3390/nu15204447
Chicago/Turabian StyleLopes, Carla A., Marta Duarte, Susana Prazeres, Ivone Carvalho, Laura Vilarinho, José Martinez-de-Oliveira, Edward Limbert, and Manuel C. Lemos. 2023. "Maternal Urinary Iodine Concentration during Pregnancy and Its Impact on Child Growth and Neurodevelopment: An 11-Year Follow-Up Study" Nutrients 15, no. 20: 4447. https://doi.org/10.3390/nu15204447
APA StyleLopes, C. A., Duarte, M., Prazeres, S., Carvalho, I., Vilarinho, L., Martinez-de-Oliveira, J., Limbert, E., & Lemos, M. C. (2023). Maternal Urinary Iodine Concentration during Pregnancy and Its Impact on Child Growth and Neurodevelopment: An 11-Year Follow-Up Study. Nutrients, 15(20), 4447. https://doi.org/10.3390/nu15204447