
Incidence of the Risk of Malnutrition and Excess Fat Mass, and Gait Speed as Independent Associated Factors in Community-Dwelling Older Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Study Design
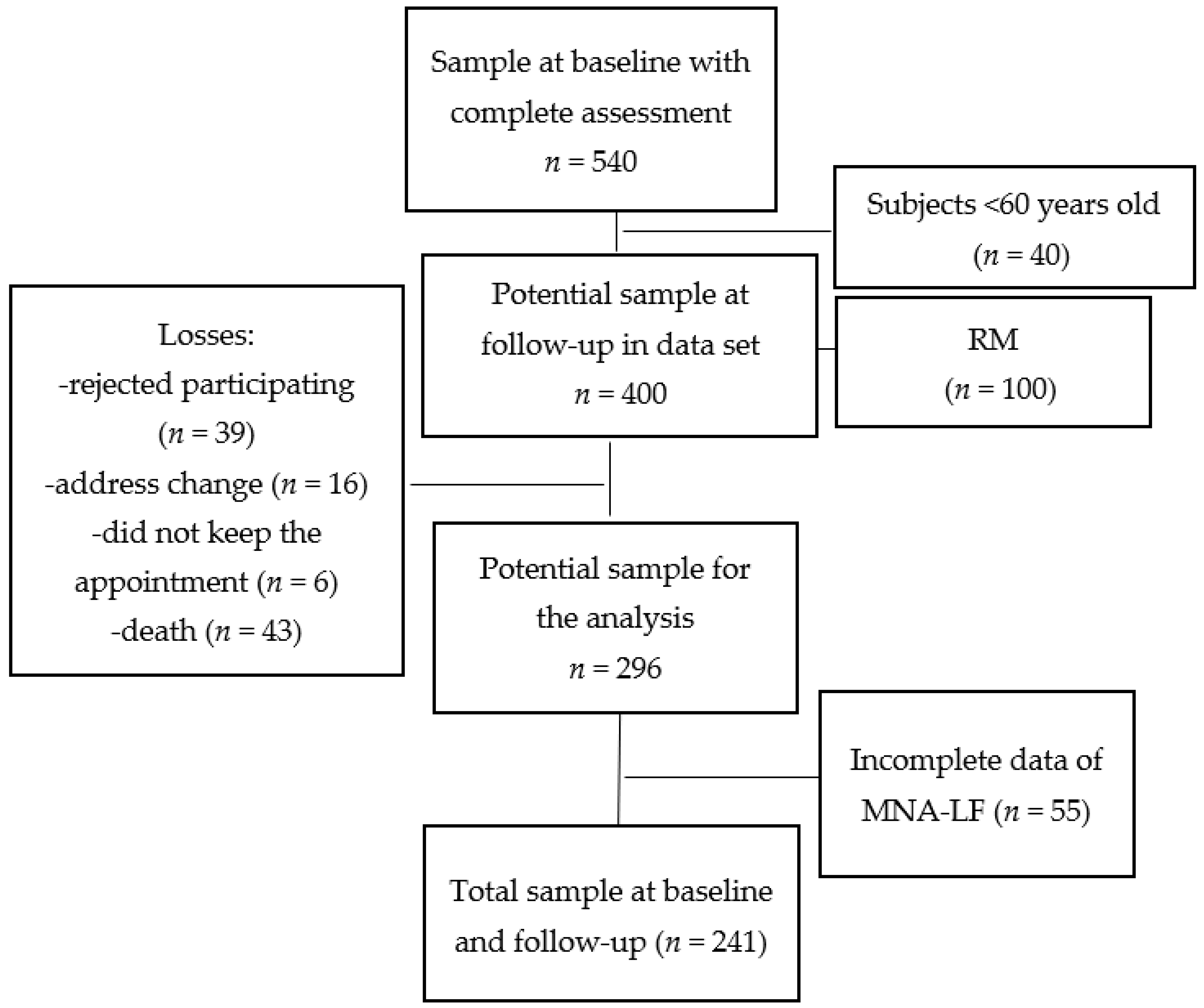
2.2. Study Population
2.3. Risk of Malnutrition as the Main Response Variable
2.4. Anthropometry
2.5. Body Composition Measured by DXA
2.6. Physical Performance Assessment
2.7. Association between the Exposition Variables and RM
2.8. Assessment of Covariates
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Final Models of the Association between the Exposition Variables and RM at 4.1 Years of Follow-Up
4. Discussion
4.1. Previous Studies Related to the Causality of Risk of Malnutrition
4.2. Potential Biological Mechanisms
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Drop-Outs, n = 61 | Follow-Up, n = 241 | p-Value | |
|---|---|---|---|
| Age, years | 73.36 ± 8.0 | 75.6 ± 7.8 | 0.064 |
| Height, m | 1.53 ± 0.0 | 1.50 ± 0.0 | 0.006 |
| Body weight, kg | 66.3 ± 12.2 | 65.2 ± 12.9 | 0.425 |
| Body mass index, kg/m2 | 28.23 ± 4.6 | 28.7 ± 5.0 | 0.484 |
| Total mass by DXA, kg | 63.7 ± 14.6 | 62.7 ± 14.3 | 0.604 |
| Fat mass, kg | 25.4 ± 8.3 | 26.2 ± 8.4 | 0.491 |
| Total lean tissue, kg | 36.5 ± 8.4 | 34.1 ± 8.1 | 0.140 |
| Bone mineral content, kg | 1.73 ± 0.6 | 1.69 ± 0.80 | 0.719 |
| MNA-LF score | 25.6 ± 2.4 | 24.19 ± 3.23 | 0.102 |
| Gender Women Men | 46 (75.4) 15 (24.6) | 201 (83.4) 40 (16.6) | 0.140 |
| Marital status Married Single, divorced, or separated Widowed | 19 (31.1) 24 (39.3) 18 (29.5) | 74 (30.7) 67 (27.8) 100 (41.4) | 0.139 |
| Education Years of schooling <10 years ≥10 years | 27 (44.2) 34 (55.8) | 144 (59.7) 97 (40.2) | 0.383 |
| Self-perception of health Bad Good | 7 (11.4) 54 (88.6) | 35 (14.5) 206 (85.5) | 0.538 |
| Depression symptoms/CESD-7 No, ≤4 CESD-7 scale Yes, ≥5 CESD-7 scale | 38 (62.2) 23 (37.8) | 139 (57.6) 102 (42.3) | 0.512 |
| Comorbidity No, ≤2 diseases Yes, ≥3 diseases | 42 (68.8) 19 (31.2) | 176 (73.0) 65 (36.2) | 0.515 |
| Cognitive impairment/MMSE No Yes | 57 (93.4) 4 (6.6) | 212 (87.9) 29 (12.0) | 0.220 |
| Polypharmacy No, ≤4 drugs/day Yes, ≥5 drugs/day | 40 (65.5) 21 (34.4) | 117 (48.5) 124 (51.4) | 0.017 |
| Dry mouth No Yes | 54 (88.5) 7 (11.4) | 205 (85.0) 36 (15.0) | 0.489 |
| Dependency by BADL No Yes | 55 (90.1) 6 (9.9) | 207 (85.8) 34 (14.2) | 0.379 |
| Dependency by IADL No Yes | 47 (77.0) 14 (23.0) | 163 (67.6) 78 (32.4) | 0.153 |
| Gait speed, m/s | 0.89 ± 0.03 | 0.88 ± 0.04 | 0.82 |
| Handgrip strength, kg | 15.8 ± 6.1 | 15.6 ± 7.5 | 0.100 |
References
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of malnutrition in older adults: A multinational perspective using the mini nutritional assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Ülger, Z.; Halil, M.; Kalan, I.; Yavuz, B.B.; Cankurtaran, M.; Güngör, E.; Arioğul, S. Comprehensive assessment of malnutrition risk and related factors in a large group of community-dwelling older adults. Clin. Nutr. 2010, 29, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Damião, R.; Santos, Á.D.S.; Matijasevich, A.; Menezes, P.R. Factors associated with risk of malnutrition in the elderly in south-eastern Brazil. Rev. Bras. Epidemiol. 2017, 20, 598–610. [Google Scholar] [CrossRef]
- Chuansangeam, M.; Wuthikraikun, C.; Supapueng, O.; Muangpaisan, W. Prevalence and risk for malnutrition in older Thai people: A systematic review and meta-analysis. Asia Pac. J. Clin. Nutr. 2022, 31, 128–141. [Google Scholar] [CrossRef]
- Kushwaha, S.; Khanna, P.; Srivastava, R.; Jain, R.; Singh, T.; Kiran, T. Estimates of malnutrition and risk of malnutrition among the elderly (≥60 years) in India: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 63, 101137. [Google Scholar] [CrossRef]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Mini Nutritional Assessment: A practical assessment tool for grading the nutritional state of elderly patients. In Facts and Research in Gerontology; Serdi Publishing Company: Paris, France, 1994; pp. 15–60. [Google Scholar]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Franco-Alvarez, N.; Avila-Funes, J.A.; Ruiz-Arreguí, L.; Gutiérrez-Robledo, L.M. Determinantes del riesgo de desnutrición en los adultos mayores de la comunidad: Análisis secundario del estudio Salud, Bienestar y Envejecimiento (SABE) en México. Rev. Panam. Salud Pública 2007, 22, 369–375. [Google Scholar] [CrossRef]
- Rodríguez-Tadeo, A.; Wall-Medrano, A.; Gaytan-Vidaña, M.E.; Campos, A.; Ornelas-Contreras, M.; Novelo-Huerta, H.I. Malnutrition risk factors among the elderly from the US-Mexico border: The “one thousand” study. J. Nutr. Health Aging 2012, 16, 426–431. [Google Scholar] [CrossRef]
- Alemán-Mateo, H.; Tavano Colaizzi, L.; Pérez-Lizaur, A.B. Nutritional status and its association with body composition compartments in physically independent, elderly Mexican subjects. J. Aging Res. Clin. Pract. 2013, 2, 211–215. [Google Scholar]
- González-Franco, L.R.; González Arellanes, R.; Ramírez Torres, M.; Alemán-Mateo, H. Riesgo de desnutrición y factores asociados en una muestra de adultos mayores en la comunidad e institucionalizados de Yucatán, México. Arch. Latinoam. Nutr. 2020, 70, 30–39. [Google Scholar] [CrossRef]
- López-Teros, M.T.; Rosas-Carrasco, O.; Sánchez-García, S.; Castro-Porras, L.; Luna-López, A.; Agudelo-Botero, M. The association of osteosarcopenia with functional disability in community-dwelling Mexican adults 50 and older. Front. Med. 2021, 8, 674724. [Google Scholar] [CrossRef] [PubMed]
- Fuentes-Pimentel, L.E.; Camacho-Guerrero, A. Prevalencia del estado de desnutrición en los adultos mayores de la Unidad Médica Familiar Núm. 53 de León, Guanajuato, México. Residente 2020, 15, 4–11. [Google Scholar] [CrossRef]
- Avila, J.C.; Samper-Ternent, R.; Wong, R. Malnutrition risk among older mexican adults in the mexican health and aging study. Nutrients 2021, 13, 1615. [Google Scholar] [CrossRef]
- Johansson, Y.; Bachrach-Lindström, M.; Carstensen, J.; Ek, A.C. Malnutrition in a home-living older population: Prevalence, incidence and risk factors. A prospective study. J. Clin. Nurs. 2009, 18, 1354–1364. [Google Scholar] [CrossRef]
- Nuotio, M.; Tuominen, P.; Luukkaala, T. Association of nutritional status as measured by the mini-nutritional assessment short form with changes in mobility, institutionalization and death after hip fracture. Eur. J. Clin. Nutr. 2016, 70, 393–398. [Google Scholar] [CrossRef]
- Kiesswetter, E.; Pohlhausen, S.; Uhlig, K.; Diekmann, R.; Lesser, S.; Uter, W.; Heseker, H.; Stehle, P.; Sieber, C.C.; Volkert, D. Prognostic differences of the Mini Nutritional Assessment short form and long form in relation to 1-year functional decline and mortality in community-dwelling older adults receiving home care. J. Am. Geriatr. Soc. 2014, 62, 512–517. [Google Scholar] [CrossRef]
- Sato, P.H.R.; Ferreira, A.A.; Rosado, E.L. The prevalence and risk factors for sarcopenia in older adults and long-living older adults. Arch. Gerontol. Geriatr. 2020, 89, 104089. [Google Scholar] [CrossRef]
- Lu, Y.; Karagounis, L.G.; Ng, T.P.; Carre, C.; Narang, V.; Wong, G.; Tan, C.T.Y.; Zin Nyunt, M.S.; Gao, Q.; Abel, B.; et al. Systemic and metabolic signature of sarcopenia in community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Shakersain, B.; Santoni, G.; Faxén-Irving, G.; Rizzuto, D.; Fratiglioni, L.; Xu, W. Nutritional status and survival among old adults: An 11-year population-based longitudinal study. Eur. J. Clin. Nutr. 2016, 70, 320–325. [Google Scholar] [CrossRef]
- Reinders, I.; Volkert, D.; de Groot, L.C.P.G.M.; Beck, A.M.; Feldblum, I.; Jobse, I.; Neelemaat, F.; de van der Schueren, M.A.E.; Shahar, D.R.; Smeets, E.T.H.C.; et al. Effectiveness of nutritional interventions in older adults at risk of malnutrition across different health care settings: Pooled analyses of individual participant data from nine randomized controlled trials. Clin. Nutr. 2019, 38, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Nykänen, I.; Lönnroos, E.; Kautiainen, H.; Sulkava, R.; Hartikainen, S. Nutritional screening in a population-based cohort of community-dwelling older people. Eur. J. Public Health 2013, 23, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Chatindiara, I.; Williams, V.; Sycamore, E.; Richter, M.; Allen, J.; Wham, C. Associations between nutrition risk status, body composition and physical performance among community-dwelling older adults. Aust. N. Z. J. Public Health 2018, 43, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Besora-Moreno, M.; Llauradó, E.; Tarro, L.; Solà, R. Social and economic factors and malnutrition or the risk of malnutrition in the elderly: A systematic review and meta-analysis of observational studies. Nutrients 2020, 12, 737. [Google Scholar] [CrossRef]
- Rosas-Carrasco, O.; Cruz-Arenas, E.; Parra-Rodríguez, L.; García-González, A.I.; Contreras-González, L.H.; Szlejf, C. Cross-Cultural Adaptation and Validation of the FRAIL Scale to Assess Frailty in Mexican Adults. J. Am. Med. Dir. Assoc. 2016, 17, 1094–1098. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky-Solís, F.; López-Arango, G.; Ardila, A. Sensitivity and specificity of the mini-mental state examination in a spanish-speaking population. Appl. Neuropsychol. 2000, 7, 25–31. [Google Scholar] [CrossRef]
- WHO. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2000; Volume 894, pp. i–xii. [Google Scholar]
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.; Pierson, R.N., Jr. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef]
- Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual energy X-ray absorptiometry body composition reference values from NHANES. PLoS ONE 2009, 4, e7038. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Fess, E.; Moran, C. Clinical Assessment Recommendations, 1st ed.; American Society of Hand Therapists: Indianapolis, IN, USA, 1981. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Salinas-Rodríguez, A.; Manrique-Espinoza, B.; Acosta-Castillo, G.I.; Franco-Nuñez, A.; Rosas-Carrasco, O.; Gutiérrez-Robledo, L.M.; Sosa-Ortíz, A.L. Validation of a cutoff point for the short version of the depression scale of the center for epidemiologic studies in older Mexican adults. Salud Pública México 2014, 56, 279–285. [Google Scholar] [CrossRef]
- Kaipainen, T.; Tiihonen, M.; Hartikainen, S.; Nykänen, I. Prevalence of risk of malnutrition and associated factors in home care clients. J. Nurs. Home Res. Sci. 2015, 1, 47–51. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Carrasco, O.; González-Flores, E.; Brito-Carrera, A.M.; Vázquez-Valdez, O.E.; Peschard-Sáenz, E.; Gutiérrez-Robledo, L.M.; García-Mayo, E.J. Assessment of comorbidity in the elderly. Rev. Médica Inst. Mex. Seguro Soc. 2011, 49, 153–162. [Google Scholar]
- Shah, B.M.; Hajjar, E.R. Polypharmacy, adverse drug reactions, and geriatric syndromes. Clin. Geriatr. Med. 2012, 28, 173–186. [Google Scholar] [CrossRef]
- Guilbert, J.J. The world health report 2002—Reducing risks, promoting healthy life. Educ. Health 2003, 16, 230. [Google Scholar] [CrossRef]
- World Health Organization. Intergovernmental Negotiating Body on the WHO Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Hussein, S.; Kantawalla, R.F.; Dickie, S.; Suarez-Durall, P.; Enciso, R.; Mulligan, R. Association of oral health and mini nutritional assessment in older adults: A systematic review with meta-analyses. J. Prosthodont. Res. 2022, 66, 208–220. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. Med. J. 1965, 14, 2. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Kramer, C.S.; Groenendijk, I.; Beers, S.; Wijnen, H.H.; van de Rest, O.; de Groot, L.C.P.G.M. The association between malnutrition and physical performance in older adults: A systematic review and meta-analysis of observational studies. Curr. Dev. Nutr. 2022, 6, nzac007. [Google Scholar] [CrossRef]
- Ramírez Torres, M.; Ruiz Valenzuela, R.E.; Esparza-Romero, J.; López Teros, M.T.; Alemán-Mateo, H. The fat mass index, not the fat-free mass index, is associated with impaired physical performance in older adult subjects: Evidence from a cross-sectional study. Clin. Nutr. 2019, 38, 877–882. [Google Scholar] [CrossRef]
- Schaap, L.A.; Koster, A.; Visser, M. Adiposity, muscle mass, and muscle strength in relation to functional decline in older persons. Epidemiol. Rev. 2013, 35, 51–65. [Google Scholar] [CrossRef]
- Böhm, A.; Heitmann, B.L. The use of bioelectrical impedance analysis for body composition in epidemiological studies. Eur. J. Clin. Nutr. 2013, 67 Suppl. S1, S79–S85. [Google Scholar] [CrossRef]
- Bigaard, J.; Frederiksen, K.; Tjønneland, A.; Thomsen, B.L.; Overvad, K.; Heitmann, B.L.; Sørensen, T.I. Body fat and fat-free mass and all-cause mortality. Obes. Res. 2004, 12, 1042–1049. [Google Scholar] [CrossRef]
- Gonzalez-Arellanes, R.; Urquidez-Romero, R.; Rodriguez-Tadeo, A.; Esparza-Romero, J.; Mendez-Estrada, R.O.; Ramirez-Lopez, E.; Robles-Sardin, A.-E.; Pacheco-Moreno, B.-I.; Alemán-Mateo, H. Predictive equations for fat mass in older Hispanic adults with excess adiposity using the 4-compartment model as a reference method. Eur. J. Clin. Nutr. 2023, 77, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Huerta, R.H.; Esparza-Romero, J.; Urquidez, R.; Pacheco, B.I.; Valencia, M.E.; Alemán-Mateo, H. Validez de una ecuación basada en antropometría para estimar la grasa corporal en adultos mayores [Validity of an equation based on anthropometry to estimate body fat in older adults]. Arch. Latinoam. Nutr. 2007, 57, 357–365. [Google Scholar]
- Aleman-Mateo, H.; Rush, E.; Esparza-Romero, J.; Ferriolli, E.; Ramirez-Zea, M.; Bour, A.; Yuchingtat, G.; Ndour, R.; Mokhtar, N.; Valencia, M.E.; et al. Prediction of fat-free mass by bioelectrical impedance analysis in older adults from developing countries: A cross-validation study using the deuterium dilution method. J. Nutr. Health Aging 2010, 14, 418–426. [Google Scholar] [CrossRef]
- Brach, J.S.; VanSwearingen, J.M.; Newman, A.B.; Kriska, A.M. Identifying early decline of physical function in community-dwelling older women: Performance-based and self-report measures. Phys. Ther. 2002, 82, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Taekema, D.G.; Gussekloo, J.; Westendorp, R.G.; de Craen, A.J.; Maier, A.B. Predicting survival in oldest old people. Am. J. Med. 2012, 125, 1188–1194.e1. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait speed predicts incident disability: A pooled analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Van der Pols-Vijlbrief, R.; Wijnhoven, H.A.; Molenaar, H.; Visser, M. Factors associated with (risk of) undernutrition in community-dwelling older adults receiving home care: A cross-sectional study in the Netherlands. Public Health Nutr. 2016, 19, 2278–2289. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.; Finlayson, G.; Duarte, C.; Whybrow, S.; Ritz, P.; Horgan, G.W.; Blundell, J.E.; Stubbs, R.J. Modelling the associations between fat-free mass, resting metabolic rate and energy intake in the context of total energy balance. Int. J. Obes. 2016, 40, 312–318. [Google Scholar] [CrossRef] [PubMed]

| Variables | Body Composition | Physical Performance | ||||||
|---|---|---|---|---|---|---|---|---|
| Fat Mass | Total Lean Tissue | Gait Speed | Handgrip Strength | |||||
| Excess Fat Mass a n = 206 | Normal Fat Mass n = 35 | Low TLT b n = 51 | Normal TLT n = 190 | Low GS c n = 80 | Normal GS n = 161 | Low HGS d n = 91 | Normal HGS n = 150 | |
| Gender Women Man | 171 (83.0) 35 (16.9) | 30 (85.7) 5 (14.3) | 39 (76.5) 12 (23.5) | 162 (85.3) 28 (14.7) | 64 (80.0) 16 (20.0) | 137 (85.1) 24 (14.9) | 75 (82.4) 16 (17.6) | 126 (84.0) 24 (16.1) |
| Age, years | 75.1 ± 7.9 | 79.1 ± 7.2 * | 77.1 ± 8.2 | 79.1 ± 7.2 * | 79.1 ± 7.8 | 73.9 ± 7.6 * | 78.7 ± 7.6 | 73.8 ± 7.7 * |
| Anthropometry Height, m | 1.5 ± 0.0 | 1.4 ± 0.0 | 1.5 ± 0.0 | 1.5 ± 0.0 | 1.49 ± 0.0 | 1.50 ± 0.0 | 1.49 ± 0.0 | 1.51 ± 0.0 |
| Body weight, kg | 60.6 ± 12.1 | 51.4 ± 7.6 * | 57.7 ± 10.4 | 67.3 ± 12.8 * | 65.4 ± 14.2 | 65.2 ± 12.3 | 64.1 ± 14.9 | 65.9 ± 11.5 |
| BMI, kg/m2 | 29.7 ± 4.7 | 23.1 ± 2.8 * | 24.8 ± 3.8 | 29.8 ± 4.8 * | 29.1 ± 5.6 | 28.6 ± 4.8 | 28.5 ± 5.7 | 28.9 ± 4.6 |
| Body composition Total mass by DXA, kg | 65.6 ± 12.4 | 45.7 ± 13.2 | 51.1 ± 14.4 | 65.9 ± 12.6 * | 62.7 ± 15.7 | 62.8 ± 13.6 | 61.7 ± 16.5 | 63.4 ± 12.8 |
| Fat mass, kg | 28.1 ± 7.2 | 16.2 ± 3.2 * | 22.2 ± 6.2 | 27.6 ± 7.9 * | 26.8 ± 8.8 | 26.4 ± 7.5 | 26.4 ± 9.6 | 26.6 ± 6.7 |
| Fat mass index, kg/m2 Total lean tissue, kg | 12.4 ± 3.2 35.7 ± 7.6 | 7.2 ± 1.3 * 31.3 ± 4.7 * | 9.5 ± 2.6 29.8 ± 6.9 | 12.3 ± 3.5 * 36.5 ± 7.0 * | 11.9 ± 3.9 35.1 ± 7.6 | 11.6 ± 3.3 35.1 ± 7.4 | 11.8 ± 4.1 34.5 ± 7.5 | 11.7 ± 3.1 35.5 ± 7.5 |
| BMC, kg | 1.7 ± 0.8 | 1.3 ± 0.5 * | 1.5 ± 0.5 | 1.7 ± 0.9 * | 1.6 ± 0.5 | 1.7 ± 0.9 | 1.7 ± 1.2 | 1.7 ± 1.6 |
| Marital status Married Single, divorced or separated Widowed | 60 (29.1) 58 (28.2) 88 (42.7) | 14 (40.0) 9 (25.7) 12 (34.3) | 15 (29.4) 15 (29.4) 21 (41.2) | 59 (31.1) 52 (27.4) 79 (41.6) | 18 (22.5) 19 (23.8) 43 (53.8) | 56 (34.8) 48 (29.8) 57 (35.4) | 29 (31.9) 22 (24.2) 40 (43.9) | 45 (30.0) 45 (30.0) 60 (40.0) |
| Living arrangements/living alone No Yes | 157 (76.2) 49 (23.8) | 27 (77.1) 8 (22.9) | 62 (77.5) 18 (22.5) | 122 (77.5) 39 (24.2) | 62 (77.5) 18 (22.5) | 122 (75.8) 39 (24.2) | 66 (72.5) 25 (27.5) | 118 (78.7) 32 (21.3) |
| Education/years of schooling <10 years ≥10 years | 122 (58.2) 13 (37.4) | 22 (62.9) 84 (40.8) | 27 (52.9) 24 (47.1) | 117 (61.6) 73 (38.4) | 56 (70.0) 24 (30.0) | 88 (54.7) 73 (45.3) * | 56 (61.5) 35 (38.5) | 88 (58.7) 62 (41.3) |
| Income source Pension No Yes | 65 (31.5) 141 (68.5) | 9 (25,7) 26 (74.3) | 23 (45.1) 28 (54.9) | 51 (26.8) 139 (73.2) * | 23 (28.8) 57 (71.3) | 51(31.7) 110 (68.3) | 29 (31.9) 62 (68.1) | 45 (30.0) 105 (70.0) |
| Medical services None Government Private or other | 8 (3.9) 187 (90.8) 11 (5.3) | 1 (2.9) 32 (91.5) 2 (5.7) | 1 (1.9) 172 (90.5) 10 (5.3) | 8 (4.2) 47 (92.2) 3 (5.9) | 2 (2.5) 73 (91.3) 5 (6.3) | 7 (4.3) 146 (90.7) 8 (4.9) | 1 (1.1) 85 (93.4) 5 (5.5) | 8 (5.3) 134 (89.3) 8 (5.3) |
| Self-perception of health Bad Good | 27 (13.1) 179 (86.9) | 8 (22.9) 27 (77.1) | 11 (21.6) 49 (78.4) | 24 (12.6) 166 (87.4) | 19 (23.8) 61 (76.3) | 16 (9.9) 145 (90.1) * | 19 (20.9) 72 (79.1) | 16 (10.7) 134 (89.3) * |
| Depression symptoms/CESD-7 e No, ≤4 CESD-7 scale Yes, ≥5 CESD-7 scale | 120 (58.3) 86 (41.8) | 19 (54.3) 16 (45.7) | 31 (60.8) 20 (39.2) | 108 (56.8) 82 (43.2) | 36 (45.0) 44 (55.0) | 103 (63.9) 58 (36.0) * | 54 (59.3) 37 (40.7) | 85 (56.7) 56 (43.3) |
| Comorbidity No, ≤2 diseases Yes, ≥3 diseases | 153 (74.3) 53 (25.7) | 23 (65.7) 12 (34.3) | 32 (62.7) 19 (37.3) | 144 (75.8) 46 (24.2) | 57 (71.3) 23 (28.8) | 119 (73.9) 42 (26.1) | 65 (71.4) 26 (28.6) | 111 (74.9) 39 (26.0) |
| Cognitive impairment/MMSE f No Yes | 181 (87.9) 25 (12.1) | 31 (88.6) 4 (11.4) | 45 (88.2) 6 (11.8) | 167 (87.9) 23 (12.1) | 59 (73.8) 21 (26.3) | 153 (95.0) 8 (4.9) * | 77 (84.6) 14 (15.4) | 135 (90.0) 15 (10.0) |
| Other diseases Osteoarthritis No Yes | 148 (72.2) 57 (27.8) | 22 (64.7) 12 (35.3) | 38 (76.0) 12 (24.0) | 132 (69.8) 57 (30.2) | 54 (69.2) 24 (30.8) | 116 (72.1) 45 (27.9) | 62 (68.9) 28 (31.1) | 109 (72.5) 41 (27.5) |
| Alcohol consumption <2 glasses/day >2 glasses/day | 110 (53.4) 96 (46.6) | 17 (50.0) 17 (50.0) | 26 (50.9) 25 (49.0) | 101 (53.3) 88 (46.6) | 49 (61.3) 31 (38.8) | 78 (48.8) 82 (51.3) | 47 (51.7) 44 (48.4) | 80 (53.7) 69 (46.3) |
| Smoking No Yes | 187 (90.8) 19 (9.2) | 33 (94.3) 2 (5.7) | 49 (96.1) 2 (3.9) | 171 (90.0) 19 (10.0) | 76 (95.0) 4 (5.0) | 144 (89.4) 17 (10.6) | 87 (95.6) 4 (4.4) | 133 (88.7) 17 (11.3) * |
| Polypharmacy No, ≤4 drugs/day Yes, ≥5 drugs/day | 102 (49.5) 104 (50.5) | 15 (42.9) 20 (57.1) | 25 (49.0) 26 (50.9) | 92 (48.4) 98 (51.6) | 34 (42.5) 46 (57.5) | 83 (51.6) 78 (48.5) | 40 (43.9) 51 (56.0) | 77 (51.3) 73 (48.7) |
| Oral health/dry mouth No Yes | 179 (86.8) 27 (13.2) | 26 (74.3) 9 (25.7) * | 41 (80.4) 10 (19.6) | 163 (86.2) 26 (13.8) | 64 (79.8) 16 (20.3) | 141 (87.6) 20 (12.4) | 78 (85.7) 13 (14.3) | 126 (84.6) 23 (15.4) |
| Nutritional status MNA score g | 25.3 ± 2.7 | 23.8 ± 3.4 * | 24.1 ± 2.9 | 25.3 ± 2.7* | 24.2 ± 2.9 | 25.5 ± 2.7 * | 24.4 ± 2.78 | 25.5 ± 2.8 * |
| Dependency/BADL h No Yes | 177 (85.9) 29 (14.1) | 30 (85.7) 5 (14.3) | 42 (82.4) 9 (17.7) | 165 (86.8) 25 (13.2) | 60 (75.0) 20 (25.0) | 147 (91.3) 14 (8.7)* | 75 (82.4) 16 (17.6) | 132 (88.0) 18 (12.0) |
| Dependency IADL i No Yes | 141 (68.5) 65 (31.6) | 22 (62.9) 13 (37.1) | 34 (66.7) 17 (33.3) | 129 (67.9) 61 (32.1) | 35 (43.8) 45 (56.3) | 128 (79.5) 33 (20.5) * | 52 (57.1) 39 (42.9) | 111 (74.0) 39 (26.9) * |
| HGS, kg | 14.4 ± 6.4 | 13.1 ± 6.2 | 13.4 ± 6.0 | 14.4 ± 6.4 | 12.8 ± 6.2 | 14.8 ± 6.3 * | 8.9 ± 3.8 | 17.4 ± 5.2 |
| GS, m/s | 0.88 ± 0.0 | 0.88 ± 0.0 | 0.88 ± 0.0 | 0.89 ± 0.0 | 0.87 ± 0.0 | 0.89 ± 0.0 * | 0.88 ± 0.0 | 0.89 ± 0.0 |
| Variables | Incidence of RM | p-Value | |
|---|---|---|---|
| Yes (n = 69) | No (n = 172) | ||
| Fat mass Excess (n = 206) Normal (n = 35) | 52 (25.2) 17 (48.5) | 154 (74.8) 18 (51.5) | 0.004 |
| Total lean tissue Low (n= 51) Normal (n = 190) | 22 (41.1) 47 (24.7) | 29 (58.9) 143 (75.3) | 0.009 |
| Gait speed Low (n = 80) Normal (n = 161) | 33 (41.2) 36 (23.8) | 47 (58.8) 125 (76.2) | 0.002 |
| Handgrip strength Low (n = 91) Normal (n = 150) | 33 (36.2) 36 (24.0) | 52 (63.8) 114 (76) | 0.041 |
| Variables | Baseline | Follow-Up | p-Value | ∆ |
|---|---|---|---|---|
| Age, years | 74.3 ± 7.6 | 78.6 ± 7.7 | 0.000 | 5.0 |
| Anthropometry | ||||
| Height, m | 1.5 ± 0.0 | 1.5 ± 0.1 | 0.028 | −9.5 |
| Body weight, kg | 64.7 ± 12.6 | 62.1 ± 12.8 | 0.000 | −4.1 |
| Body mass index, kg/m2 | 28.5 ± 4.9 | 27.5 ± 5.0 | 0.000 | −3.6 |
| Body composition | ||||
| Total mass by DXA, kg | 62.2 ± 12.8 | 60.6 ± 8.2 | 0.009 | −2.6 |
| Fat mass, kg | 26.2 ± 7.7 | 24.8 ± 7.9 | 0.000 | −5.6 |
| Fat mass index, kg/m2 | 11.6 ± 3.3 | 11.0 ± 3.3 | 0.000 | −5.4 |
| Total lean tissue, kg | 34.4 ± 6.4 | 34.1 ± 6.3 | 0.601 | −1.0 |
| Total lean tissue index, kg/m2 | 15.2 ± 2.2 | 15.1 ± 2.2 | 0.826 | −0.6 |
| Bone mineral content, kg | 1.7 ± 0.3 | 1.7 ± 0.5 | 0.087 | −1.1 |
| Nutritional status | ||||
| MNA, score | 25.5 ± 2.8 | 23.0 ± 3.1 | 0.000 | −10.8 |
| Physical performance | ||||
| HGS, kg | 14.6 ± 6.3 | 13.7 ± 5.9 | 0.064 | −6.5 |
| GS, m/s | 0.9 ± 0.0 | 0.8 ± 0.0 | 0.012 | −12.5 |
| Variables | OR | p-Value | CI 95% |
|---|---|---|---|
| Excess fat mass, kg/m2 | 0.35 | 0.006 | 0.17–0.74 |
| Low TLT, kg/m2 | 2.30 | 0.011 | 1.21–4.39 |
| Gender, women | 1.06 | 0.862 | 0.50–2.28 |
| Age, years | 1.01 | 0.274 | 0.98–1.05 |
| Marital status Single, divorced, or separated Widowed | 0.55 0.93 | 0.125 0.841 | 0.25–1.18 0.49–1.78 |
| Living alone | 0.67 | 0.267 | 0.33–1.35 |
| Education, <10 years of schooling | 1.98 | 0.025 | 0.27–0.91 |
| Without a pension | 1.23 | 0.500 | 0.66–2.29 |
| Without medical services | 1.35 | 0.674 | 0.32–5.59 |
| Good self-perception of health | 0.15 | 0.000 | 0.06–0.32 |
| Depression symptoms, ≥5 CESD-7 scale | 1.48 | 0.168 | 0.84–2.60 |
| Cognitive impairment | 1.91 | 0.110 | 0.86–4.26 |
| Comorbidity, ≥3 diseases | 1.87 | 0.042 | 1.02–3.43 |
| Osteoarthritis | 0.93 | 0.842 | 0.50–1.75 |
| Polypharmacy, ≥5 drugs/day | 1.57 | 0.118 | 0.89–2.76 |
| Dry mouth | 3.95 | 0.000 | 1.90–8.21 |
| Dependency by the BADL | 6.24 | 0.000 | 2.87–13.54 |
| Dependency by the IADL | 2.82 | 0.000 | 1.57–5.06 |
| Low gait speed, m/s | 1.96 | 0.020 | 1.11–3.45 |
| Low handgrip strength, kg | 1.80 | 0.042 | 1.02–3.18 |
| Alcohol consumption, >2 glasses/day | 1.41 | 0.547 | 0.45–4.38 |
| Smoking | 0.76 | 0.610 | 0.26–2.16 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| OR Unadjusted (CI 95%) | p-Value | OR Adjusted (CI 95%) | p-Value | OR Adjusted (CI 95%) | p-Value | |
| Fat mass Normal Excess | 1.00 0.35 (0.17–0.74) | 0.006 | 1.00 0.24 (0.09–0.64) | 0.005 | 1.00 0.35 (0.16–0.82) | 0.015 |
| Total lean tissue Normal Low | 1.00 2.30 (1.21–4.39) | 0.011 | 1.00 2.06 (0.98–4.32) | 0.054 | 1.00 2.04 (0.97–4.26) | 0.057 |
| Gait speed, m/s Normal Low | 1.00 2.43 (1.36–4.32) | 0.003 | 1.00 2.01 (1.06–3.83) | 0.032 | 1.00 1.96 (1.03–3.72) | 0.038 |
| Handgrip strength, kg Normal Low | 1.00 1.80 (1.02–3.18) | 0.042 | 1.00 1.68 (0.90–3.16) | 0.061 | 1.00 1.63 (0.87–3.05) | 0.125 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Teros, M.T.; Vidaña-Espinoza, H.J.; Esparza-Romero, J.; Rosas-Carrasco, O.; Luna-López, A.; Alemán-Mateo, H. Incidence of the Risk of Malnutrition and Excess Fat Mass, and Gait Speed as Independent Associated Factors in Community-Dwelling Older Adults. Nutrients 2023, 15, 4419. https://doi.org/10.3390/nu15204419
López-Teros MT, Vidaña-Espinoza HJ, Esparza-Romero J, Rosas-Carrasco O, Luna-López A, Alemán-Mateo H. Incidence of the Risk of Malnutrition and Excess Fat Mass, and Gait Speed as Independent Associated Factors in Community-Dwelling Older Adults. Nutrients. 2023; 15(20):4419. https://doi.org/10.3390/nu15204419
Chicago/Turabian StyleLópez-Teros, Miriam T., Helen J. Vidaña-Espinoza, Julián Esparza-Romero, Oscar Rosas-Carrasco, Armando Luna-López, and Heliodoro Alemán-Mateo. 2023. "Incidence of the Risk of Malnutrition and Excess Fat Mass, and Gait Speed as Independent Associated Factors in Community-Dwelling Older Adults" Nutrients 15, no. 20: 4419. https://doi.org/10.3390/nu15204419
APA StyleLópez-Teros, M. T., Vidaña-Espinoza, H. J., Esparza-Romero, J., Rosas-Carrasco, O., Luna-López, A., & Alemán-Mateo, H. (2023). Incidence of the Risk of Malnutrition and Excess Fat Mass, and Gait Speed as Independent Associated Factors in Community-Dwelling Older Adults. Nutrients, 15(20), 4419. https://doi.org/10.3390/nu15204419