
Impact of Maternal Fish Consumption on Serum Docosahexaenoic Acid (DHA) Levels in Breastfed Infants: A Cross-Sectional Study of a Randomized Clinical Trial in Japan

Abstract
:1. Introduction
2. Materials and Methods
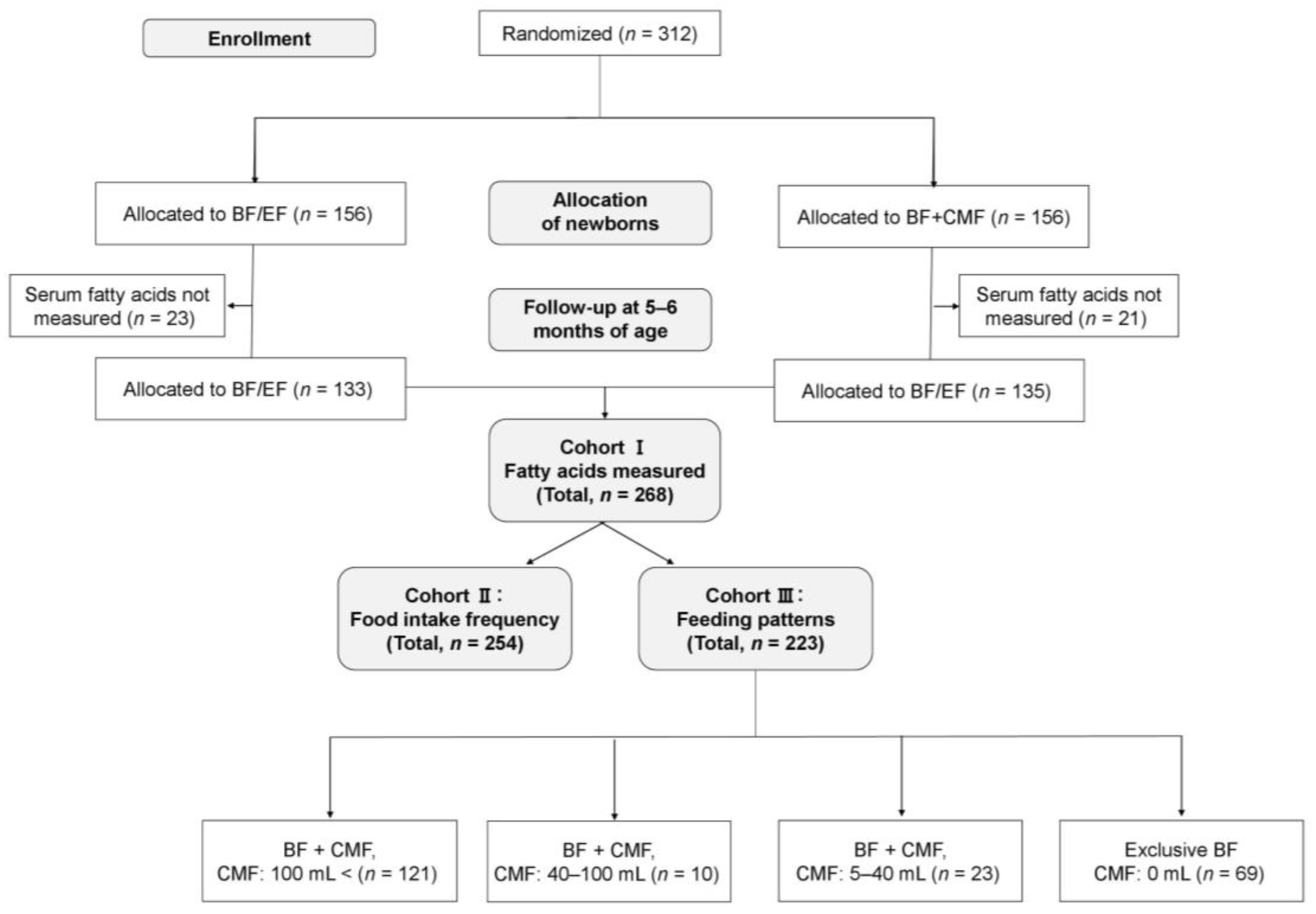
2.1. Study Design
2.2. Study Population
2.3. Infant Formula and Intervention
2.4. Sample Size
2.5. Data Collection
2.6. Serum Fatty Acid Measurements and Primary/Secondary Outcomes
2.7. Statistical Analysis
3. Results
3.1. Study Population
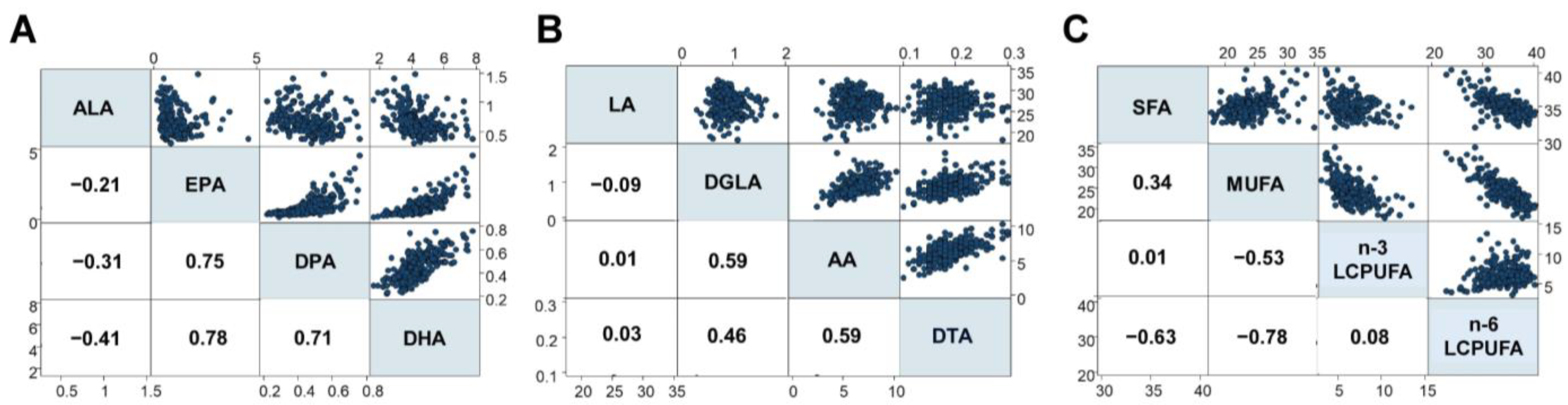
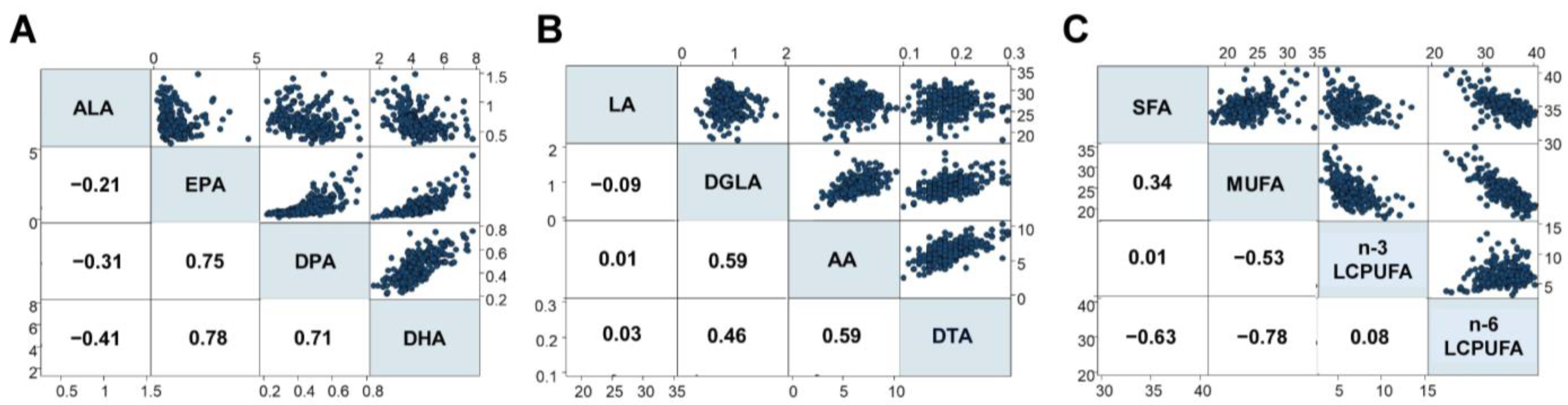
3.2. Serum Fatty Acid Compositions at 5–6 Months of Age
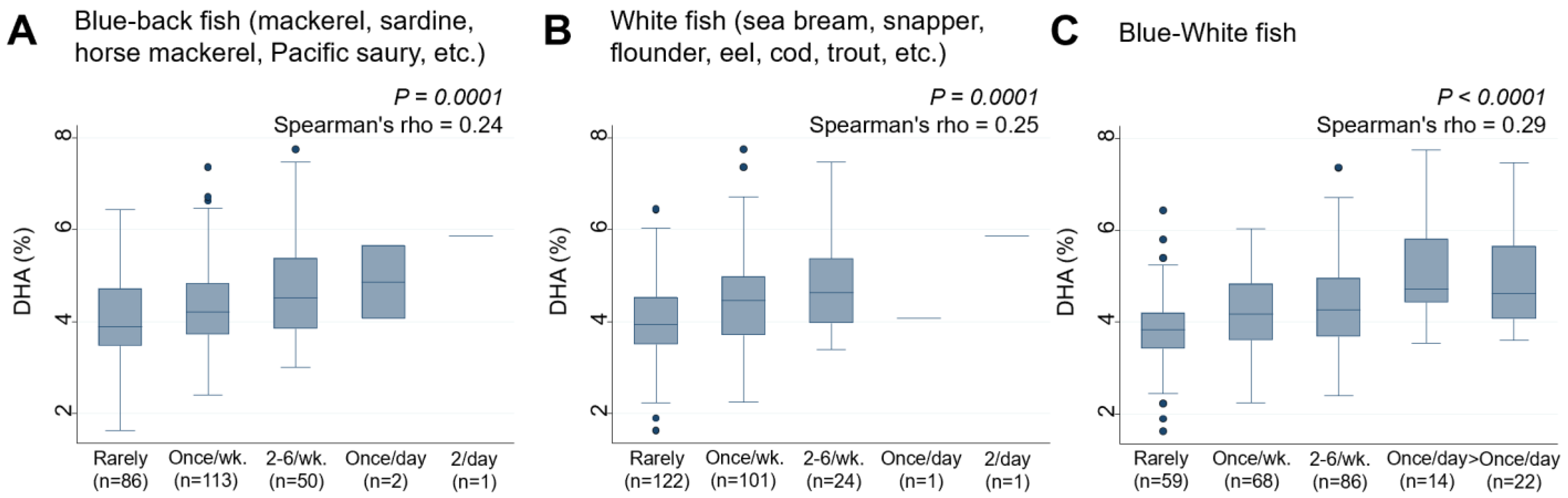
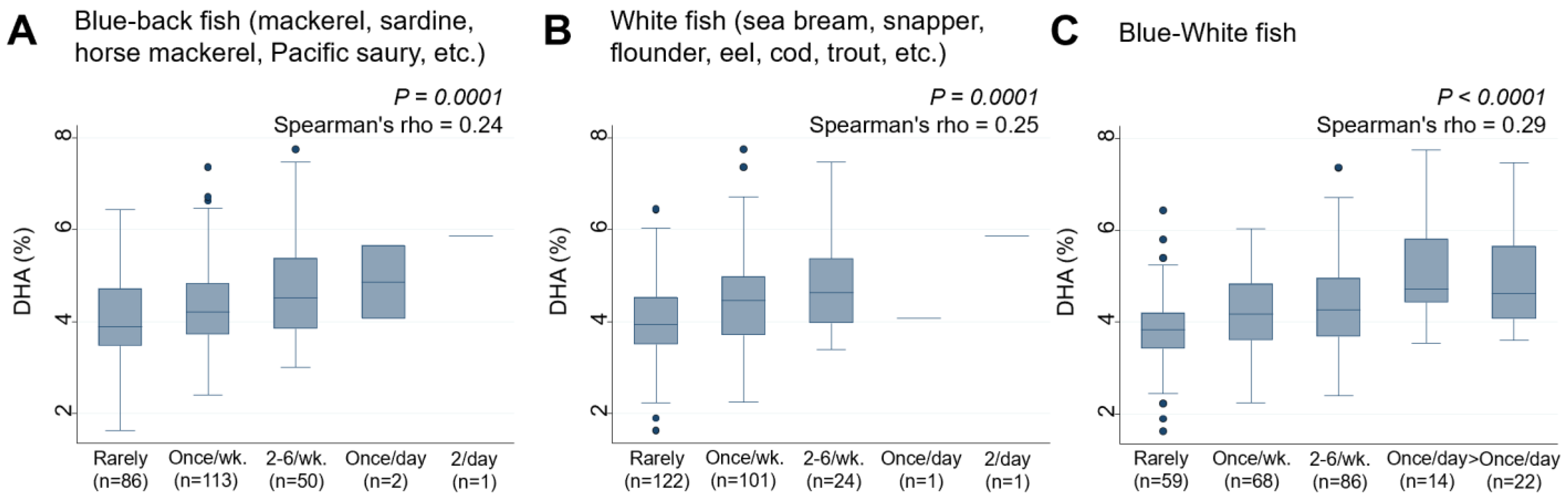
3.3. Frequency of Maternal Intake of the Listed Items and Serum DHA Levels in Infants
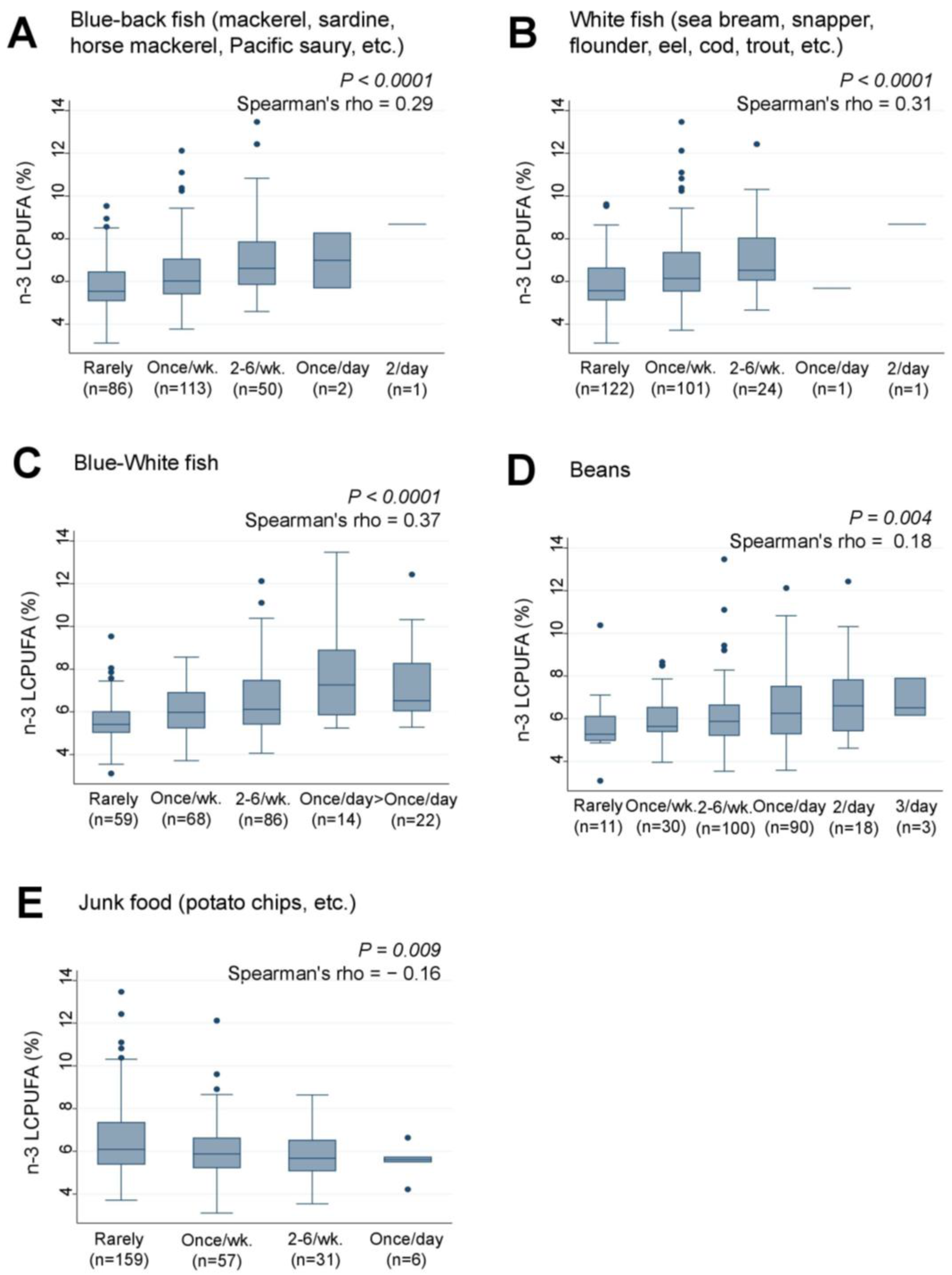
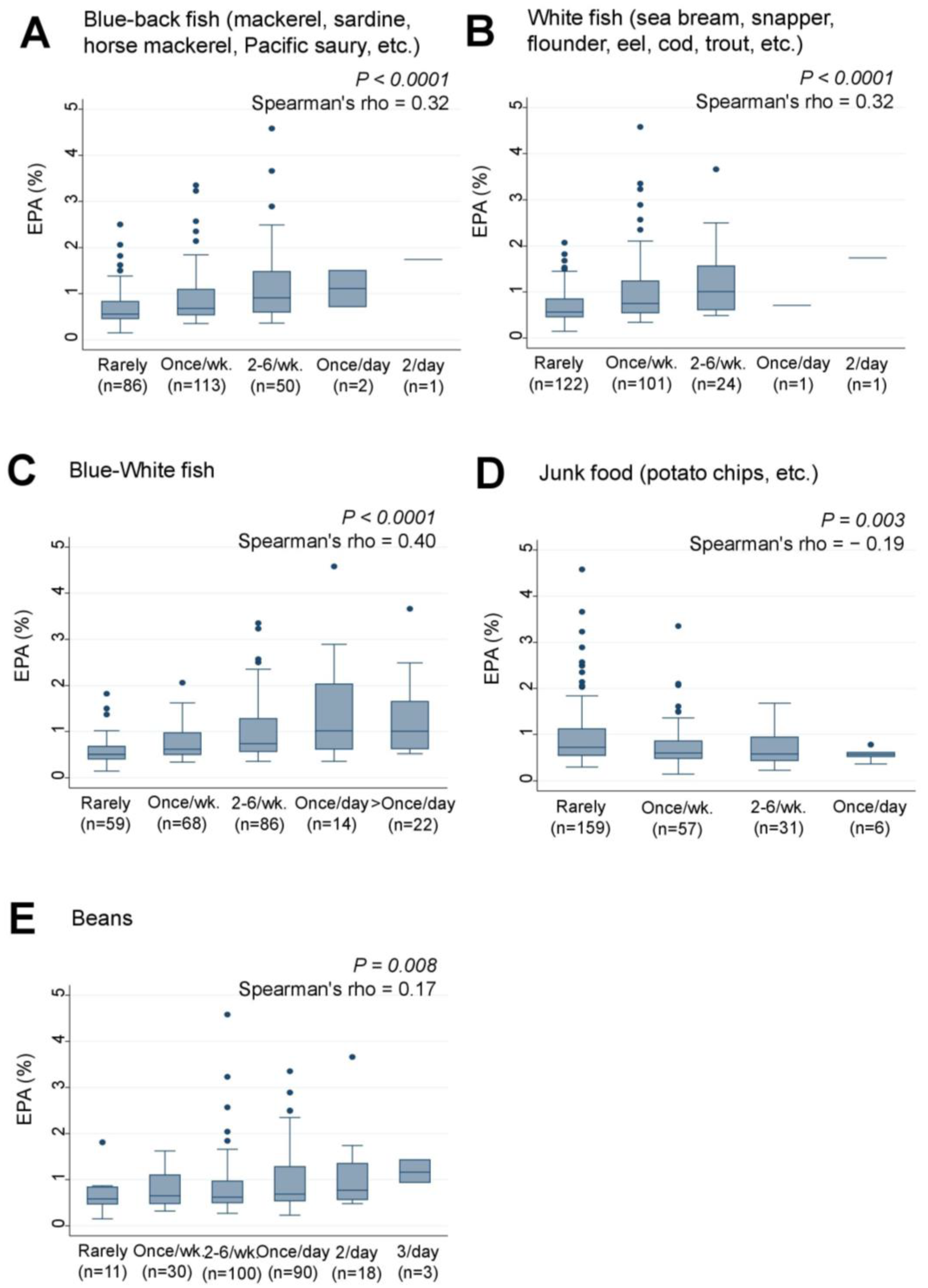
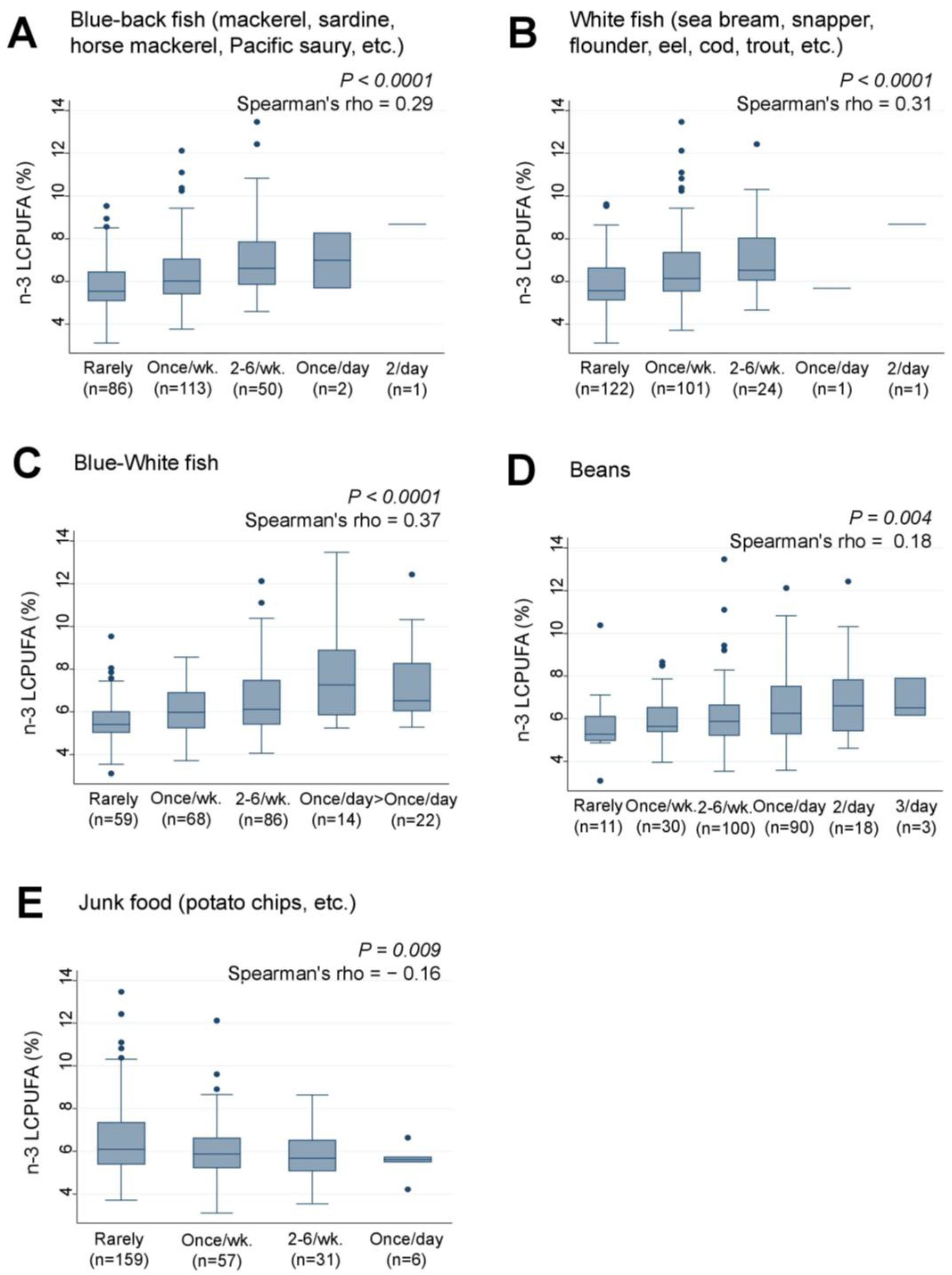
3.4. Frequency of Maternal Intake of the Listed Items and Serum EPA and Other LCPUFA Levels in Infants
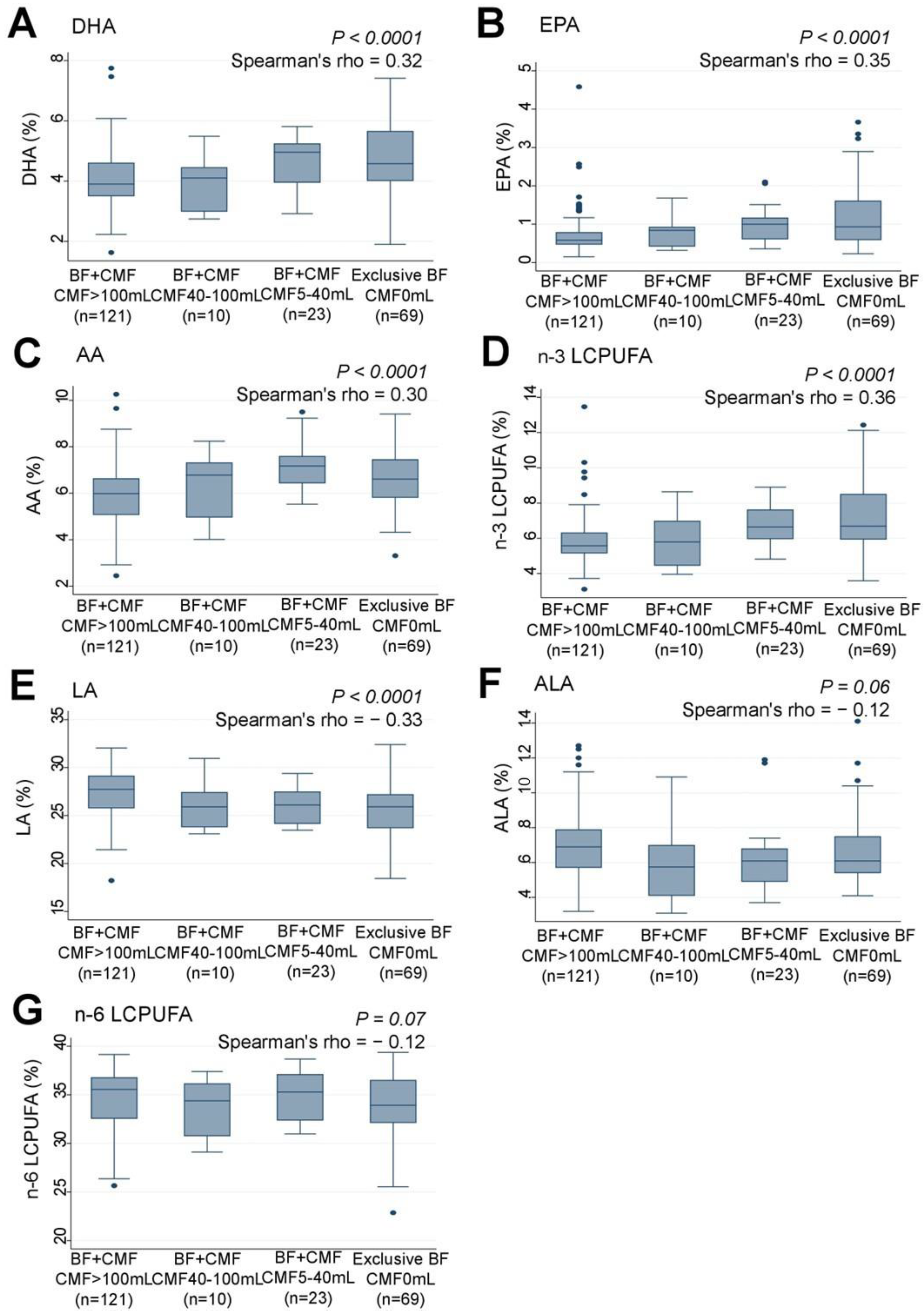
3.5. Feeding Patterns and Serum DHA and Other n-3 LCPUFA Levels in Infants
3.6. Factors Associated with Serum DHA Levels in Infants: Univariate and Multivariate Regression Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meek, J.Y.; Noble, L.; Section on Breastfeeding. Policy statement: Breastfeeding and the use of human milk. Pediatrics 2022, 150, e2022057988. [Google Scholar] [CrossRef]
- World Health Organization. Breastfeeding; World Health Organization: Geneva, Switzerland, 2018.
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Horwood, L.J.; Darlow, B.A.; Mogridge, N. Breast milk feeding and cognitive ability at 7–8 years. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 84, F23–F27. [Google Scholar] [CrossRef] [PubMed]
- Plunkett, B.A.; Mele, L.; Casey, B.M.; Varner, M.W.; Sorokin, Y.; Reddy, U.M.; Wapner, R.J.; Thorp, J.M., Jr.; Saade, G.R.; Tita, A.T.N.; et al. Association of breastfeeding and child IQ score at age 5 Years. Obstet. Gynecol. 2021, 137, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Decsi, T.; Thiel, I.; Koletzko, B. Essential fatty acids in full term infants fed breast milk or formula. Arch. Dis. Child. Fetal Neonatal Ed. 1995, 72, F23–F28. [Google Scholar] [CrossRef] [PubMed]
- Boehm, G.; Borte, M.; Bohles, H.J.; Muller, H.; Kohn, G.; Moro, G. Docosahexaenoic and arachidonic acid content of serum and red blood cell membrane phospholipids of preterm infants fed breast milk, standard formula or formula supplemented with n-3 and n-6 long-chain polyunsaturated fatty acids. Eur. J. Pediatr. 1996, 155, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Foreman-van Drongelen, M.M.; van Houwelingen, A.C.; Kester, A.D.; Blanco, C.E.; Hasaart, T.H.; Hornstra, G. Influence of feeding artificial-formula milks containing docosahexaenoic and arachidonic acids on the postnatal long-chain polyunsaturated fatty acid status of healthy preterm infants. Br. J. Nutr. 1996, 76, 649–667. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, J. Docosahexaenoic acid (DHA): An ancient nutrient for the modern human brain. Nutrients 2011, 3, 529–554. [Google Scholar] [CrossRef] [PubMed]
- Schneider, N.; Bruchhage, M.M.K.; O’Neill, B.V.; Hartweg, M.; Tanguy, J.; Steiner, P.; Mutungi, G.; O’Regan, J.; McSweeney, S.; D’Sa, V.; et al. A nutrient formulation affects developmental myelination in term infants: A randomized clinical trial. Front Nutr. 2022, 9, 823–893. [Google Scholar] [CrossRef] [PubMed]
- Hortensius, L.M.; Hellstrom, W.; Savman, K.; Heckemann, R.A.; Bjorkman-Burtscher, I.M.; Groenendaal, F.; Andersson, M.X.; Nilsson, A.K.; Tataranno, M.L.; van Elburg, R.M.; et al. Serum docosahexaenoic acid levels are associated with brain volumes in extremely preterm born infants. Pediatr. Res. 2021, 90, 1177–1185. [Google Scholar] [CrossRef]
- Lauritzen, L.; Brambilla, P.; Mazzocchi, A.; Harslof, L.B.; Ciappolino, V.; Agostoni, C. DHA effects in brain development and function. Nutrients 2016, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Jasani, B.; Simmer, K.; Patole, S.K.; Rao, S.C. Long chain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst. Rev. 2017, 3, CD000376. [Google Scholar] [CrossRef] [PubMed]
- Moon, K.; Rao, S.C.; Schulzke, S.M.; Patole, S.K.; Simmer, K. Longchain polyunsaturated fatty acid supplementation in preterm infants. Cochrane Database Syst. Rev. 2016, 12, CD000375. [Google Scholar] [CrossRef] [PubMed]
- Newberry, S.J.; Chung, M.; Booth, M.; Maglione, M.A.; Tang, A.M.; O’Hanlon, C.E.; Wang, D.D.; Okunogbe, A.; Huang, C.; Motala, A.; et al. Omega-3 fatty acids and maternal and child health: An updated systematic review. Evid. Rep. Technol. Assess. 2016, 224, 1–826. [Google Scholar]
- Gould, J.F.; Makrides, M.; Gibson, R.A.; Sullivan, T.R.; McPhee, A.J.; Anderson, P.J.; Best, K.P.; Sharp, M.; Cheong, J.L.Y.; Opie, G.F.; et al. Neonatal docosahexaenoic acid in preterm infants and intelligence at 5 years. N. Engl. J. Med. 2022, 387, 1579–1588. [Google Scholar] [CrossRef]
- Henriksen, C.; Haugholt, K.; Lindgren, M.; Aurvag, A.K.; Ronnestad, A.; Gronn, M.; Solberg, R.; Moen, A.; Nakstad, B.; Berge, R.K.; et al. Improved cognitive development among preterm infants attributable to early supplementation of human milk with docosahexaenoic acid and arachidonic acid. Pediatrics 2008, 121, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Lepping, R.J.; Honea, R.A.; Martin, L.E.; Liao, K.; Choi, I.Y.; Lee, P.; Papa, V.B.; Brooks, W.M.; Shaddy, D.J.; Carlson, S.E.; et al. Long-chain polyunsaturated fatty acid supplementation in the first year of life affects brain function, structure, and metabolism at age nine years. Dev. Psychobiol. 2019, 61, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Liao, K.; McCandliss, B.D.; Carlson, S.E.; Colombo, J.; Shaddy, D.J.; Kerling, E.H.; Lepping, R.J.; Sittiprapaporn, W.; Cheatham, C.L.; Gustafson, K.M. Event-related potential differences in children supplemented with long-chain polyunsaturated fatty acids during infancy. Dev. Sci. 2017, 20, e12455. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. The Dietary Guidelines for Americans, 2020–2025, 9th ed.; U.S. Department of Agriculture: Washington, DC, USA, 2020.
- Bravi, F.; Wiens, F.; Decarli, A.; Dal Pont, A.; Agostoni, C.; Ferraroni, M. Impact of maternal nutrition on breast-milk composition: A systematic review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef]
- Bondia-Martinez, E.; Lopez-Sabater, M.C.; Castellote-Bargallo, A.I.; Rodriguez-Palmero, M.; Gonzalez-Corbella, M.J.; Rivero-Urgell, M.; Campoy-Folgoso, C.; Bayes-Garcia, R. Fatty acid composition of plasma and erythrocytes in term infants fed human milk and formulae with and without docosahexaenoic and arachidonic acids from egg yolk lecithin. Early Hum. Dev. 1998, 53 (Suppl. 1), S109–S119. [Google Scholar] [CrossRef]
- Schwartz, J.; Drossard, C.; Dube, K.; Kannenberg, F.; Kunz, C.; Kalhoff, H.; Kersting, M. Dietary intake and plasma concentrations of PUFA and LC-PUFA in breastfed and formula fed infants under real-life conditions. Eur. J. Nutr. 2010, 49, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Visentin, S.; Vicentin, D.; Magrini, G.; Santandreu, F.; Disalvo, L.; Sala, M.; Fasano, V.; Gonzalez, H.F. Red blood cell membrane fatty acid composition in infants fed formulas with different lipid profiles. Early Hum. Dev. 2016, 100, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Uhl, O.; Fleddermann, M.; Hellmuth, C.; Demmelmair, H.; Koletzko, B. Phospholipid species in newborn and 4 month old infants after consumption of different formulas or breast milk. PLoS ONE 2016, 11, e0162040. [Google Scholar] [CrossRef]
- Iso, H.; Sato, S.; Folsom, A.R.; Shimamoto, T.; Terao, A.; Munger, R.G.; Kitamura, A.; Konishi, M.; Iida, M.; Komachi, Y. Serum fatty acids and fish intake in rural Japanese, urban Japanese, Japanese American and Caucasian American men. Int. J. Epidemiol. 1989, 18, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Mezawa, H.; Okuyama, M.; Urashima, T.; Hirano, D.; Gocho, N.; Tachimoto, H. Primary prevention of cow’s milk sensitization and food allergy by avoiding supplementation with cow’s milk formula at birth: A randomized clinical trial. JAMA Pediatr. 2019, 173, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, A.; Takayanagi, K.; Fujita, T.; Hirai, A.; Hamazaki, T.; Terano, T.; Tamura, Y.; Kumagai, A. Determination of long chain fatty acids in human total plasma lipids using gas chromatography. Bunseki Kagaku. 1982, 31, 87–91. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Brenna, J.T.; Varamini, B.; Jensen, R.G.; Diersen-Schade, D.A.; Boettcher, J.A.; Arterburn, L.M. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 2007, 85, 1457–1464. [Google Scholar] [CrossRef]
- Miliku, K.; Duan, Q.L.; Moraes, T.J.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Lefebvre, D.L.; Sears, M.R.; Subbarao, P.; Field, C.J.; et al. Human milk fatty acid composition is associated with dietary, genetic, sociodemographic, and environmental factors in the CHILD Cohort Study. Am. J. Clin. Nutr. 2019, 110, 1370–1383. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.M.; Higurashi, S.; Shimomura, Y.; Wakui, R.; Matsuura, H.; Shiota, M.; Kubouchi, H.; Yamamura, J.I.; Toba, Y.; Kobayashi, T. Association of DHA concentration in human breast milk with maternal diet and use of supplements: A cross-sectional analysis of data from the Japanese human milk study cohort. Curr. Dev. Nutr. 2020, 4, nzaa105. [Google Scholar] [CrossRef] [PubMed]
- Lohner, S.; Fekete, K.; Marosvolgyi, T.; Decsi, T. Gender differences in the long-chain polyunsaturated fatty acid status: Systematic review of 51 publications. Ann. Nutr. Metab. 2013, 62, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Decsi, T.; Kennedy, K. Sex-specific differences in essential fatty acid metabolism. Am. J. Clin. Nutr. 2011, 94, 1914S–1919S. [Google Scholar] [CrossRef] [PubMed]
- Ordnung, M.; Mank, M.; Stahl, B.; Kurz, D.; Marosvolgyi, T.; Decsi, T.; Rothenbacher, D.; Genuneit, J.; Siziba, L.P. Potential sex differences in human milk fatty acids and their association with atopic dermatitis: Results of the Ulm SPATZ health study. Pediatr. Allergy Immunol. 2023, 34, e13992. [Google Scholar] [CrossRef] [PubMed]
- Makrides, M.; Neumann, M.A.; Simmer, K.; Gibson, R.A. Erythrocyte fatty acids of term infants fed either breast milk, standard formula, or formula supplemented with long-chain polyunsaturates. Lipids 1995, 30, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Seifert, J.; Szabo, N.J.; Clare-Salzler, M.; Rewers, M.; Norris, J.M. Erythrocyte membrane fatty acid content in infants consuming formulas supplemented with docosahexaenoic acid (DHA) and arachidonic acid (ARA): An observational study. Matern. Child Nutr. 2010, 6, 338–346. [Google Scholar] [CrossRef]
- Ogunleye, A.; Fakoya, A.T.; Niizeki, S.; Tojo, H.; Sasajima, I.; Kobayashi, M.; Tateishi, S.; Yamaguchi, K. Fatty acid composition of breast milk from Nigerian and Japanese women. J. Nutr. Sci. Vitaminol. 1991, 37, 435–442. [Google Scholar] [CrossRef]
- Yuhas, R.; Pramuk, K.; Lien, E.L. Human milk fatty acid composition from nine countries varies most in DHA. Lipids 2006, 41, 851–858. [Google Scholar] [CrossRef]
- Wang, L.; Shimizu, Y.; Kaneko, S.; Hanaka, S.; Abe, T.; Shimasaki, H.; Hisaki, H.; Nakajima, H. Comparison of the fatty acid composition of total lipids and phospholipids in breast milk from Japanese women. Pediatr. Int. 2000, 42, 14–20. [Google Scholar] [CrossRef]
- Katoku, Y.; Yamada, M.; Yonekubo, A.; Kuwata, T.; Kobayashi, A.; Sawa, A. Effect of the cholesterol content of a formula on the lipid compositions of plasma lipoproteins and red blood cell membranes in early infancy. Am. J. Clin. Nutr. 1996, 64, 871–877. [Google Scholar] [CrossRef]
- Hadley, K.B.; Ryan, A.S.; Forsyth, S.; Gautier, S.; Salem, N., Jr. The essentiality of arachidonic acid in infant development. Nutrients 2016, 8, 216. [Google Scholar] [CrossRef]
- Kawashima, H. Intake of arachidonic acid-containing lipids in adult humans: Dietary surveys and clinical trials. Lipids Health Dis. 2019, 18, 101. [Google Scholar] [CrossRef]
- Crozier, S.R.; Godfrey, K.M.; Calder, P.C.; Robinson, S.M.; Inskip, H.M.; Baird, J.; Gale, C.R.; Cooper, C.; Sibbons, C.M.; Fisk, H.L.; et al. Vegetarian diet during pregnancy is not associated with poorer cognitive performance in children at age 6–7 years. Nutrients 2019, 11, 3029. [Google Scholar] [CrossRef]
- De Caterina, R. n-3 fatty acids in cardiovascular disease. N. Engl. J. Med. 2011, 364, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.R.; Wheaton, D.K.; James, K.J.; Tuazon, M.; Diersen-Schade, D.A.; Harris, C.L.; Stolz, S.; Berseth, C.L. Docosahexaenoic acid in red blood cells of term infants receiving two levels of long-chain polyunsaturated fatty acids. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 287–292. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fatty Acid Measured n = 268 | Fatty Acid Unmeasured n = 42 | |
|---|---|---|
| Maternal age, mean (SD)—years | 35.1 (4.3) | 35.4 (4.8) |
| Maternal body mass index, mean (SD)—kg/m2 | 20.6 (4.3) | 20.9 (2.8) |
| Gestational weeks, median (IQR)—weeks | 39 (38–39) | 39 (38–39) |
| Birth weight, mean (SD)—g | 2993 (314) | 2983 (309) |
| Female, no. (%) | 69 (53.9) | 65 (50.0) |
| No. | Fatty Acids | μg/mL | Weight % | |
|---|---|---|---|---|
| Measured Value | Measured Value | |||
| Median (IQR) Min–Max | Median (IQR) Min–Max | |||
| 1 | Lauric acid | 12:0 | 25.5 (16.0–41.9) 2.9–206 | 0.76 (0.50–1.11) 0.11–2.96 |
| 2 | Myristic acid | 14:0 | 45.6 (31.4–67.4) 16.3–298 | 1.32 (1.04–1.75) 0.57–4.50 |
| 3 | Myristoleic acid | 14:1n-5 | 1.4 (1.0–2.0) 0.30–10.2 | 0.04 (0.03–0.05) 0.01–0.14 |
| 4 | Palmitic acid | 16:0 | 723 (654–934) 434–2280 | 22.3 (21.6–22.9) 19.5–26.0 |
| 5 | Palmitoleic acid | 16:1n-7 | 43.4 (32.3–55.4) 18.8–153 | 1.24 (1.11–1.43) 0.77–2.56 |
| 6 | Stearic acid | 18:0 | 300 (264–348) 180–846 | 8.67 (8.23–9.14) 6.82–10.2 |
| 7 | Oleic acid | 18:1n-9 | 719 (594–925) 327–2758 | 21.1 (19.5–23.1) 14.6–32.8 |
| 8 | Linoleic acid | 18:2n-6 | 931 (818–1072) 540–1840 | 26.9 (24.6–28.8) 18.2–31.8 |
| 9 | γ-linolenic acid | 18:3n-6 | 4.70 (3.85–5.80) 1.50–15.8 | 0.13 (0.11–0.16) 0.05–0.53 |
| 10 | α-linolenic acid | 18:3n-3 | 22.5 (17.0–31.4) 9.7–87.4 | 0.65 (0.53–0.77) 0.31–1.48 |
| 11 | Arachidic acid | 20:0 | 12.9 (11.6–14.6) 6.90–29.4 | 0.36 (0.34–0.40) 0.27–0.55 |
| 12 | Eicosenoic acid | 20:1n-9 | 6.60 (5.00–9.15) 2.50–28.8 | 0.19 (0.16–0.23) 0.10–0.48 |
| 13 | Eicosadienoic acid | 20:2n-6 | 8.90 (7.60–22.1) 4.90–22.1 | 0.26 (0.24–0.27) 0.18–0.35 |
| 14 | 5,8,11-eicosatrienoic acid | 20:3n-9 | 2.1 (1.7–2.6) 0.7–6.1 | 0.06 (0.05–0.07) 0.005–0.17 |
| 15 | Dihomo-γ-linolenic acid | 20:3n-6 | 30.4 (24.3–37.1) 14.0–79.0 | 0.84 (0.72–1.01) 0.30–1.82 |
| 16 | Arachidonic acid | 20:4n-6 | 221 (191–257) 103–437 | 6.22 (5.41–7.15) 2.45–10.3 |
| 17 | Eicosapentaenoic acid | 20:5n-3 | 24.3 (17.2–39.5) 3.9–165 | 0.66 (0.51–1.07) 0.15–4.58 |
| 18 | Behenic acid | 22:0 | 23.1 (20.6–25.6) 13.4–41.0 | 0.66 (0.57–0.75) 0.35–0.99 |
| 19 | Erucic acid | 22:1n-9 | 1.6 (1.2–2.0) 0.5–4.2 | 0.05 (0.04–0.05) 0.005–0.09 |
| 20 | Docosatetraenoic acid | 22:4n-6 | 6.5 (5.7–7.6) 2.8–14.2 | 0.19 (0.16–0.21) 0.10–0.30 |
| 21 | Docosapentaenoic acid | 22:5n-3 | 16.0 (12.6–19.0) 4.6–46.1 | 0.44 (0.36–0.53) 0.22–0.76 |
| 22 | Lignoceric acid | 24:0 | 19.5 (17.4–22.0) 10.3–32.6 | 0.56 (0.48–0.65) 0.26–0.91 |
| 23 | Docosahexaenoic acid | 22:6n-3 | 150.0 (127.4–178.3) 42.8–368.6 | 4.17 (3.69–4.90) 1.63–7.75 |
| 24 | Nervonic acid | 24:1n-9 | 41.7 (35.0–46.8) 24.2–85.0 | 1.19 (0.96–1.41) 0.52–1.98 |
| No. | Food Item | n | rho | p Value |
|---|---|---|---|---|
| Fish | ||||
| 1 | Blue-back fish: Mackerel, sardine, horse mackerel, Pacific saury (including canned) | 252 | 0.24 | 0.0001 |
| 2 | White fish (sea bream, snapper, flounder, eel, cod, trout, etc.) | 249 | 0.25 | 0.0001 |
| 3 | Salmon (including canned salmon) | 250 | 0.03 | 0.64 |
| 4 | Tuna (canned tuna, sashimi, etc.) | 252 | −0.02 | 0.78 |
| 5 | Swordfish | 249 | 0.01 | 0.82 |
| Nuts | ||||
| 6 | Peanuts (including peanut butter) | 249 | −0.06 | 0.36 |
| 7 | Walnuts | 250 | −0.01 | 0.92 |
| 8 | Almonds | 251 | 0.04 | 0.49 |
| 9 | Cashew nuts | 250 | 0.06 | 0.32 |
| 10 | Macadamia nuts | 251 | 0.04 | 0.50 |
| 11 | Hazelnuts | 249 | −0.00 | 0.98 |
| 12 | Coconut (including that in processed foods) | 244 | −0.02 | 0.78 |
| Dairy products | ||||
| 13 | Cow’s milk | 254 | 0.11 | 0.07 |
| 14 | Cheese | 252 | −0.05 | 0.45 |
| 15 | Cream (including cream for coffee) | 254 | −0.11 | 0.07 |
| 16 | Ice cream | 253 | 0.05 | 0.44 |
| 17 | Butter | 249 | 0.01 | 0.90 |
| Egg | ||||
| 18 | Heated eggs | 252 | −0.03 | 0.62 |
| 19 | Raw eggs | 221 | 0.02 | 0.79 |
| 20 | Mayonnaise | 251 | −0.06 | 0.33 |
| 21 | Fish eggs (salmon roe, flying fish roe, sea urchin, dried mullet roe, caviar, etc.) | 250 | −0.02 | 0.81 |
| Vegetable oil | ||||
| 22 | Unspecified vegetable oil | 247 | −0.04 | 0.55 |
| 23 | Olive oil | 250 | 0.03 | 0.61 |
| 24 | Rapeseed oil | 268 | −0.05 | 0.45 |
| 25 | Sesame oil | 268 | −0.08 | 0.21 |
| 26 | Safflower oil | 268 | −0.09 | 0.16 |
| 27 | Other | 268 | −0.01 | 0.92 |
| 28 | Margarine | 248 | −0.07 | 0.25 |
| Fried food | ||||
| 29 | Junk food (potato chips, etc.) | 253 | −0.11 | 0.08 |
| 30 | Instant noodles | 250 | −0.12 | 0.06 |
| 31 | Fried food at home (tempura, fried chicken, fried potatoes, etc.) | 254 | 0.03 | 0.59 |
| 32 | Fried food from outside (tempura, fried chicken, fried potatoes, etc.) | 254 | −0.11 | 0.09 |
| Meat | ||||
| 33 | Beef | 246 | 0.05 | 0.43 |
| 34 | Pork | 252 | 0.05 | 0.46 |
| 35 | Chicken | 251 | 0.08 | 0.23 |
| 36 | Processed meat (sausage, salami, hotdogs, bacon, etc.) | 253 | −0.05 | 0.40 |
| 37 | Hamburger at fast-food restaurant | 248 | −0.08 | 0.22 |
| Beans | ||||
| 38 | Soybean (natto, tofu, miso, green soybeans, soy milk) and sweet red (adzuki) beans | 252 | 0.14 | 0.02 |
| Univariate Analysis | Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Model I | Model II | Model III | |||||||
| CE | 95% CI | p Value | CE | 95% CI | p Value | CE | 95% CI | p Value | |
| Blue-White fish | 0.29 | 0.19–0.39 | <0.001 | 0.29 | 0.18–0.41 | <0.001 | 0.24 | 0.11–0.38 | 0.001 |
| Feeding patterns | 0.25 | 0.15–0.35 | <0.001 | 0.18 | 0.09–0.28 | <0.001 | 0.17 | 0.05–0.29 | 0.006 |
| Allocated group in ABC trial | 0.18 | −0.07–0.44 | 0.15 | 0.07 | −0.23–0.37 | 0.64 | |||
| Maternal age | −0.02 | −0.05–0.01 | 0.27 | 0.01 | −0.02–0.04 | 0.54 | |||
| Maternal body mass index | 0.01 | −0.03–0.04 | 0.74 | 0.00 | −0.03–0.03 | 0.94 | |||
| Gestational weeks | 0.05 | −0.01–0.11 | 0.13 | 0.05 | −0.10–0.19 | 0.54 | |||
| Birth weight | 0.00 | −0.00–0.00 | 0.20 | 0.31 | −0.00–0.00 | 0.72 | |||
| Female | 0.19 | −0.06–0.44 | 0.13 | 0.31 | 0.00–0.63 | 0.05 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasamatsu, A.; Tachimoto, H.; Urashima, M. Impact of Maternal Fish Consumption on Serum Docosahexaenoic Acid (DHA) Levels in Breastfed Infants: A Cross-Sectional Study of a Randomized Clinical Trial in Japan. Nutrients 2023, 15, 4338. https://doi.org/10.3390/nu15204338
Kasamatsu A, Tachimoto H, Urashima M. Impact of Maternal Fish Consumption on Serum Docosahexaenoic Acid (DHA) Levels in Breastfed Infants: A Cross-Sectional Study of a Randomized Clinical Trial in Japan. Nutrients. 2023; 15(20):4338. https://doi.org/10.3390/nu15204338
Chicago/Turabian StyleKasamatsu, Ayu, Hiroshi Tachimoto, and Mitsuyoshi Urashima. 2023. "Impact of Maternal Fish Consumption on Serum Docosahexaenoic Acid (DHA) Levels in Breastfed Infants: A Cross-Sectional Study of a Randomized Clinical Trial in Japan" Nutrients 15, no. 20: 4338. https://doi.org/10.3390/nu15204338
APA StyleKasamatsu, A., Tachimoto, H., & Urashima, M. (2023). Impact of Maternal Fish Consumption on Serum Docosahexaenoic Acid (DHA) Levels in Breastfed Infants: A Cross-Sectional Study of a Randomized Clinical Trial in Japan. Nutrients, 15(20), 4338. https://doi.org/10.3390/nu15204338