
Adherence to a Mediterranean Diet for 6 Months Improves the Dietary Inflammatory Index in a Western Population: Results from the MedLey Study

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Methods
2.1. Calculating the DII and E-DII Scores
2.2. Statistical Analysis
2.2.1. Statistical Analysis of Changes in DII and E-DII Scores with Dietary Intervention
2.2.2. Statistical Analysis of Intervention Impacts Relating to DII and E-DII Scores
2.2.3. Statistical Analysis of Cross-Sectional Relationships of DII® and E-DII with Health Parameters
3. Results
3.1. Dietary Adherence to a MedDiet
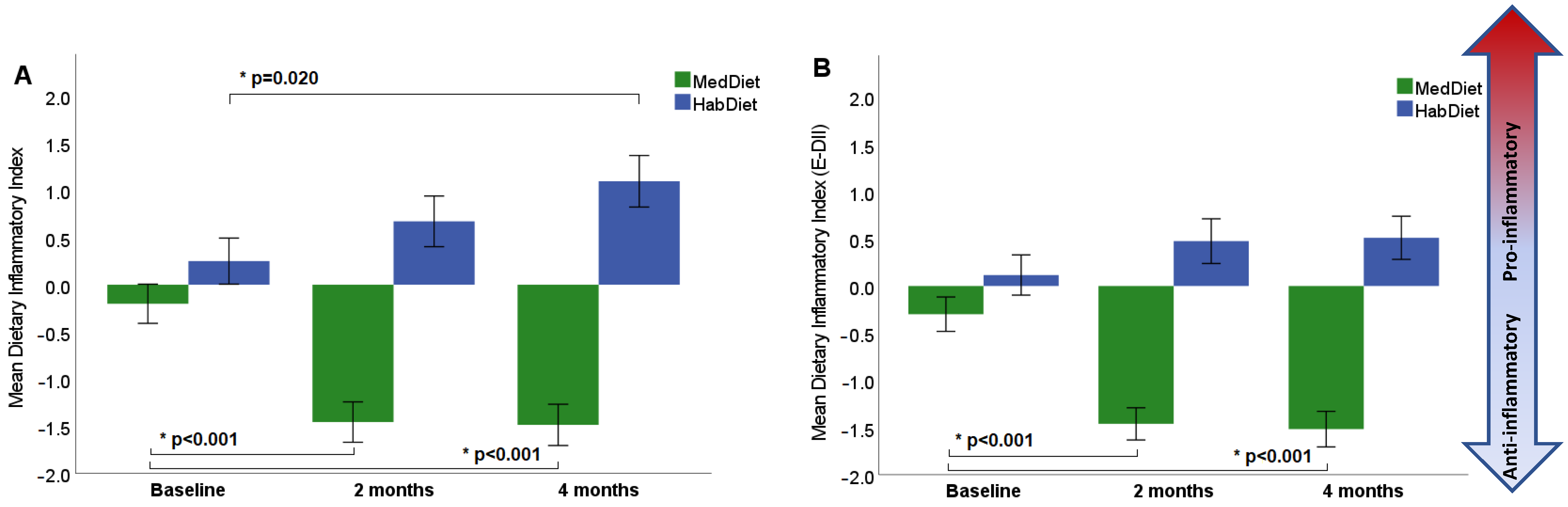
3.2. Dietary Inflammatory Index
3.3. Cardiometabolic Health Outcomes of the MedLey Trial
3.4. Relationship of DII® to Changes in MedLey Outcome Measures
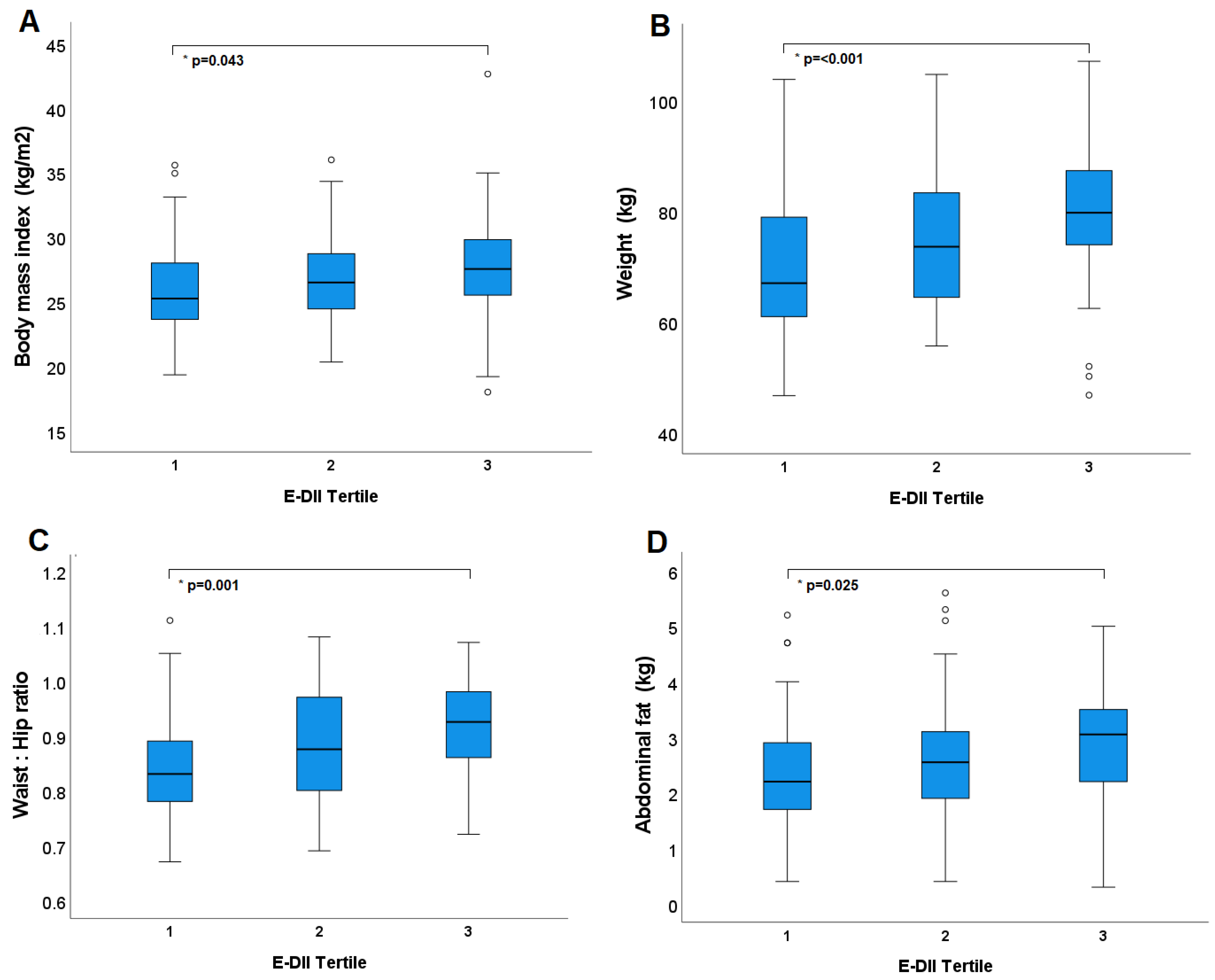
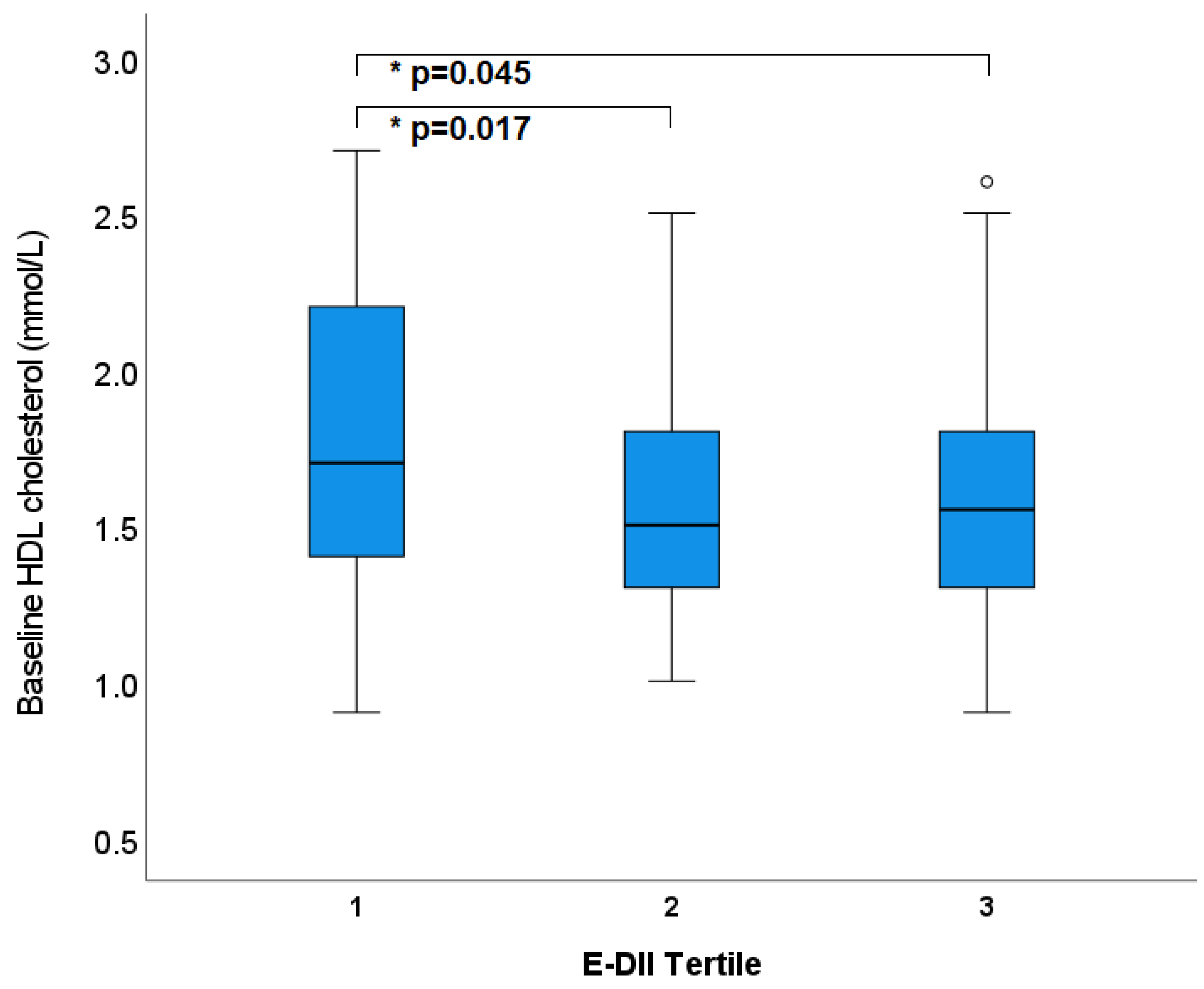
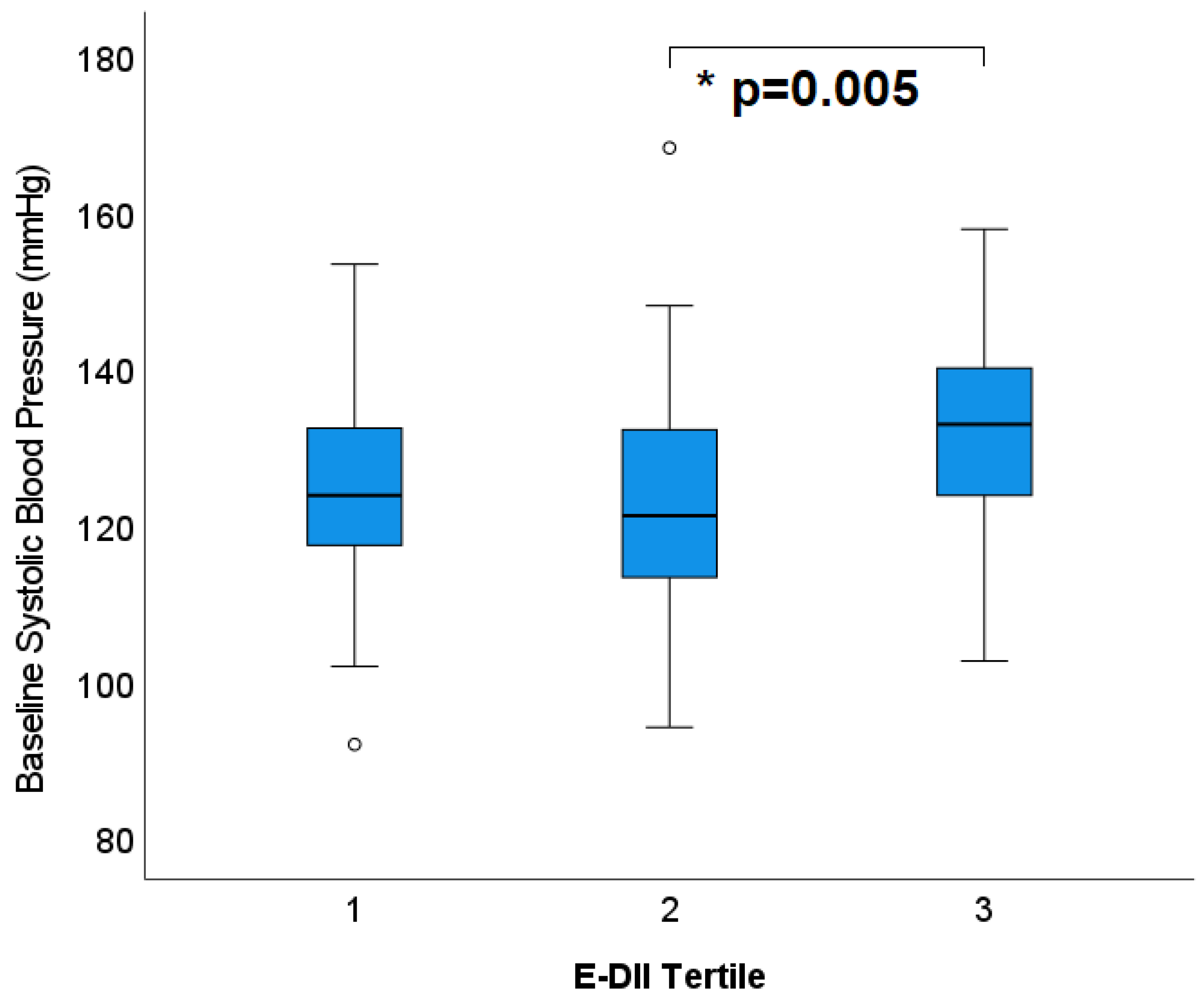
3.5. Cross-Sectional Relationships of DII® with Health Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Caan, B.; Hou, L.; Johnson, K.C.; Mossavar-Rahmani, Y.; Shivappa, N.; et al. The association between dietary inflammatory index and risk of colorectal cancer among postmenopausal women: Results from the Women’s Health Initiative. Cancer Causes Control CCC 2015, 26, 399–408. [Google Scholar] [CrossRef]
- Shivappa, N.; Bosetti, C.; Zucchetto, A.; Serraino, D.; La Vecchia, C.; Hébert, J.R. Dietary inflammatory index and risk of pancreatic cancer in an Italian case-control study. Br. J. Nutr. 2015, 113, 292–298. [Google Scholar] [CrossRef]
- Pimenta, A.M.; Toledo, E.; Rodriguez-Diez, M.C.; Gea, A.; Lopez-Iracheta, R.; Shivappa, N.; Hébert, J.R.; Martinez-Gonzalez, M.A. Dietary indexes, food patterns and incidence of metabolic syndrome in a Mediterranean cohort: The SUN project. Clin. Nutr. (Edinb. Scotl.) 2015, 34, 508–514. [Google Scholar] [CrossRef]
- Garcia-Arellano, A.; Ramallal, R.; Ruiz-Canela, M.; Salas-Salvado, J.; Corella, D.; Shivappa, N.; Schroder, H.; Hebert, J.R.; Ros, E.; Gomez-Garcia, E.; et al. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study. Nutrients 2015, 7, 4124–4138. [Google Scholar] [CrossRef] [PubMed]
- Ramallal, R.; Toledo, E.; Martínez-González, M.A.; Hernández-Hernández, A.; García-Arellano, A.; Shivappa, N.; Hébert, J.R.; Ruiz-Canela, M. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the SUN Cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef] [PubMed]
- Nettleton, J.A.; Steffen, L.M.; Mayer-Davis, E.J.; Jenny, N.S.; Jiang, R.; Herrington, D.M.; Jacobs, D.R., Jr. Dietary patterns are associated with biochemical markers of inflammation and endothelial activation in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2006, 83, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Chrysohoou, C.; Panagiotakos Demosthenes, B.; Pitsavos, C.; Das Undurti, N.; Stefanadis, C. Adherence to the Mediterranean diet attenuates inflammation and coagulation process in healthy adults. J. Am. Coll. Cardiol. 2004, 44, 152–158. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.Á.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-Style Diet on Cardiovascular Risk Factors. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hébert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R., Jr.; Steck, S.E.; Hébert, J.R. Association between inflammatory potential of diet and mortality in the Iowa Women’s Health study. Eur. J. Nutr. 2016, 55, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Guo, L.; Zhang, L.; Li, Y.; He, R.; Cheng, G. Inflammatory potential of diet and risk of cardiovascular disease or mortality: A meta-analysis. Sci. Rep. 2017, 7, 6367. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Cardiovascular Risk and Mortality-A Meta-Analysis. Nutrients 2018, 10, 200. [Google Scholar] [CrossRef]
- Wrottesley, S.V.; Shivappa, N.; Prioreschi, A.; Hébert, J.R.; Norris, S.A. Anti-inflammatory diets reduce the risk of excessive gestational weight gain in urban South Africans from the Soweto First 1000-Day Study (S1000). Eur. J. Nutr. 2022, 61, 3929–3941. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposito, K. The Effects of Diet on Inflammation. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Bryan, J.; Wilson, C.; Hodgson, J.; Dhillon, V.; Murphy, K. A randomised controlled intervention trial evaluating the efficacy of an Australianised Mediterranean diet compared to the habitual Australian diet on cognitive function, psychological wellbeing and cardiovascular health in healthy older adults (MedLey study): Protocol paper. BMC Nutr. 2015, 1, 35. [Google Scholar]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.; Murphy, K. A randomised controlled intervention trial evaluating the efficacy of a Mediterranean dietary pattern on cognitive function and psychological wellbeing in healthy older adults: The MedLey study. BMC Geriatr. 2015, 15, 55. [Google Scholar] [CrossRef]
- Xinying, P.X.; Noakes, M.; Keogh, J. Can a food frequency questionnaire be used to capture dietary intake data in a 4 week clinical intervention trial? Asia Pac. J. Clin. Nutr. 2004, 13, 318–323. [Google Scholar]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Hébert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)-Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. (Bethesda Md.) 2019, 10, 185–195. [Google Scholar] [CrossRef]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.M.; Davis, C.R.; Murphy, K.J. The Mediterranean Diet and Cognitive Function among Healthy Older Adults in a 6-Month Randomised Controlled Trial: The MedLey Study. Nutrients 2016, 8, 579. [Google Scholar] [CrossRef] [PubMed]
- Tonkin, A.; Barter, P.; Best, J.; Boyden, A.; Furler, J.; Hossack, K.; Sullivan, D.; Thompson, P.; Vale, M.; Cooper, C.; et al. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Position statement on lipid management--2005. Heart Lung Circ. 2005, 14, 275–291. [Google Scholar] [CrossRef] [PubMed]
- Gabb, G.M.; Mangoni, A.A.; Anderson, C.S.; Cowley, D.; Dowden, J.S.; Golledge, J.; Hankey, G.J.; Howes, F.S.; Leckie, L.; Perkovic, V.; et al. Guideline for the diagnosis and management of hypertension in adults-2016. Med. J. Aust. 2016, 205, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. New Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Davis, C.; Hodgson, J.; Bryan, J.; Garg, M.; Woodman, R.; Murphy, K. Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study. Nutrients 2017, 9, 534. [Google Scholar] [CrossRef]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Woodman, R.; Murphy, K.J. A Mediterranean Diet Reduces F2-Isoprostanes and Triglycerides among Older Australian Men and Women after 6 Months. J. Nutr. 2017, 147, 1348–1355. [Google Scholar] [CrossRef]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef]
- Alkerwi, A.; Shivappa, N.; Crichton, G.; Hébert, J.R. No significant independent relationships with cardiometabolic biomarkers were detected in the Observation of Cardiovascular Risk Factors in Luxembourg study population. Nutr. Res. 2014, 34, 1058–1065. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Hodge, A.M.; Bassett, J.K.; Dugué, P.A.; Shivappa, N.; Hébert, J.R.; Milne, R.L.; English, D.R.; Giles, G.G. Dietary inflammatory index or Mediterranean diet score as risk factors for total and cardiovascular mortality. Nutr. Metab. Cardiovasc. Dis. NMCD 2018, 28, 461–469. [Google Scholar] [CrossRef]
- Ruiz-Canela, M.; Zazpe, I.; Shivappa, N.; Hébert, J.R.; Sánchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Lamuela-Raventós, R.M.; Rekondo, J.; et al. Dietary inflammatory index and anthropometric measures of obesity in a population sample at high cardiovascular risk from the PREDIMED (PREvención con DIeta MEDiterránea) trial. Br. J. Nutr. 2015, 113, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Thomas, C.J.; Tierney, A.C.; Kucianski, T.; George, E.S.; Ruiz-Canela, M.; Hebert, J.R.; Shivappa, N.; Itsiopoulos, C. Randomization to 6-month Mediterranean diet compared with a low-fat diet leads to improvement in Dietary Inflammatory Index scores in patients with coronary heart disease: The AUSMED Heart Trial. Nutr. Res. 2018, 55, 94–107. [Google Scholar] [CrossRef]
- Ramallal, R.; Toledo, E.; Martínez, J.A.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A.; Ruiz-Canela, M. Inflammatory potential of diet, weight gain, and incidence of overweight/obesity: The SUN cohort. Obes. (Silver Spring Md.) 2017, 25, 997–1005. [Google Scholar] [CrossRef]
- Mazidi, M.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Kengne, A.P. Greater Dietary Inflammatory Index score is associated with higher likelihood of chronic kidney disease. Br. J. Nutr. 2018, 120, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Karim, M.N.; Hébert, J.R.; Shivappa, N.; Milne, R.L.; de Courten, B. Diet scores and prediction of general and abdominal obesity in the Melbourne collaborative cohort study. Public Health Nutr. 2021, 24, 6157–6168. [Google Scholar] [CrossRef]
- Oliveira, T.M.S.; Bressan, J.; Pimenta, A.M.; Martínez-González, M.-Á.; Shivappa, N.; Hébert, J.R.; Hermsdorff, H.H.M. Dietary inflammatory index and prevalence of overweight and obesity in Brazilian graduates from the Cohort of Universities of Minas Gerais (CUME project). Nutrition 2020, 71, 110635. [Google Scholar] [CrossRef] [PubMed]
- Abdollahzad, H.; Pasdar, Y.; Nachvak, S.M.; Rezaeian, S.; Saber, A.; Nazari, R. The Relationship Between the Dietary Inflammatory Index and Metabolic Syndrome in Ravansar Cohort Study. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 477–487. [Google Scholar] [CrossRef]
- Shivappa, N.; Bonaccio, M.; Hebert, J.R.; Di Castelnuovo, A.; Costanzo, S.; Ruggiero, E.; Pounis, G.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Association of proinflammatory diet with low-grade inflammation: Results from the Moli-sani study. Nutrition 2018, 54, 182–188. [Google Scholar] [CrossRef]
- Yarizadeh, H.; Mirzababaei, A.; Ghodoosi, N.; Pooyan, S.; Djafarian, K.; Clark, C.C.T.; Mirzaei, K. The interaction between the dietary inflammatory index and mc4r gene variants on cardiovascular risk factors. Clin. Nutr. (Edinb. Scotl.) 2021, 40, 488–495. [Google Scholar] [CrossRef]
- Abdurahman, A.A.; Azadbakhat, L.; Rasouli, M.; Chamari, M.; Qorbani, M.; Dorosty, A.R. Association of dietary inflammatory index with metabolic profile in metabolically healthy and unhealthy obese people. Nutr. Diet. J. Dietit. Assoc. Aust. 2019, 76, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, H.F.L.; van Baak, M.A.; Mariman, E.C.; Sulistyoningrum, D.C.; Huriyati, E.; Lee, Y.Y.; Wan Muda, W.A.M. Dietary inflammatory index score and its association with body weight, blood pressure, lipid profile, and leptin in indonesian adults. Nutrients 2019, 11, 148. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Shivappa, N.; Nasreddine, L.; Kharroubi, S.; Itani, L.; Hwalla, N.; Mehio Sibai, A.; Hebert, J.R. Role of inflammation in the association between the western dietary pattern and metabolic syndrome among lebanese adults. Int. J. Food Sci. Nutr. 2017, 68, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Namazi, N.; Larijani, B.; Azadbakht, L. Dietary Inflammatory Index and its Association with the Risk of Cardiovascular Diseases, Metabolic Syndrome, and Mortality: A Systematic Review and Meta-Analysis. Horm. Metab. Res. 2018, 50, 345–358. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Kotsakis, G.A.; Panagiotakos, D.; Shivappa, N.; Wirth, M.D.; Hébert, J.R.; Haro, J.M. Dietary inflammatory potential is linked to cardiovascular disease risk burden in the US adult population. Int. J. Cardiol. 2017, 240, 409–413. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SEM | MedDiet | Diet x Visit Interaction | Diet | Visit | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 month | 2 month | 4 month | Change 0–2 month | Change 0–4 month | ||||||||
| (n = 79) | (n = 69) | (n = 70) | mean change | p value | 95%CI | mean change | p value | 95%CI | p value | p value | p value | |
| DII | −0.20 ± 0.22 | −1.27 ± 0.22 | −1.32 ± 0.22 | 1.07 ± 0.23 | <0.001 | 0.51, 1.63 | 1.11 ± 0.26 | <0.001 | 0.49, 1.74 | <0.001 | <0.001 | 0.108 |
| E-DII | −0.30 ± 0.19 | −1.40 ± 0.20 | −1.47 ± 0.20 | 1.10 ± 0.22 | <0.001 | 0.57–1.63 | 1.17 ± 0.22 | <0.001 | 0.63, 1.71 | <0.001 | <0.001 | 0.034 |
| HabDiet | ||||||||||||
| 0 month | 2 month | 4 month | Change 0–2 month | Change 0–4 month | ||||||||
| (n = 71) | (n = 67) | (n = 65) | mean change | p value | 95%CI | mean change | p value | 95%CI | ||||
| DII | 0.24 ± 0.23 | 0.62 ± 0.23 | 0.98 ± 0.23 | −0.37 ± 0.24 | 0.36 | −0.21, 0.95 | −0.73 ± 0.27 | 0.02 | −1.38, −0.09 | |||
| E-DII | 0.12 ± 0.20 | 0.47 ± 0.21 | 0.54 ± 0.21 | −0.35 ± 0.22 | 0.35 | −0.90, 0.19 | −0.43 ± 0.23 | 0.21 | −0.99, 0.14 | |||
| Model | Tertile 1 | Tertile 2 | Tertile 3 | Trend | |
|---|---|---|---|---|---|
| Low | Medium | High | (ANOVA) | ||
| BMI | 1 | 25.71 ± 0.54 (24.65, 26.76) ¥ | 26.41 ± 0.54 (25.35, 27.47) ¥ | 28.41 ± 0.52 (27.37, 29.45) ӿ† | p = 0.001 |
| 2 | 26.07 ± 0.54 (24.99, 27.14) ¥ | 26.57 ± 0.54 (25.50, 27.64) | 27.98 ± 0.55 (26.89, 29.06) ӿ | p = 0.040 | |
| Weight (kg) | 1 | 70.41 ± 1.77 (66.91, 73.90) ¥ | 72.99 ± 1.77 (69.50, 76.49) ¥ | 80.09 ± 1.73 (76.66, 83.51) ӿ† | p < 0.0005 |
| 2 | 69.76 ± 1.75 (66.30, 73.23) ¥ | 74.39 ± 1.75 (70.92, 77.85) | 79.67 ± 1.77 (76.17, 83.17) ӿ | p = 0.001 | |
| WHR | 1 | 0.88 ± 0.01 (0.85, 0.90) | 0.86 ± 0.01 (0.83, 0.88) ¥ | 0.91 ± 0.01 (0.89, 0.94) † | p = 0.008 |
| 2 | 0.85 ± 0.01 (0.82, 0.87) ¥ | 0.88 ± 0.01 (0.85, 0.90) | 0.92 ± 0.01 (0.89, 0.94) ӿ | p = 0.001 | |
| Abdominal fat (kg) | 1 | 2.18 ± 0.15 (1.89, 2.47) ¥ | 2.65 ± 0.15 (2.35, 2.94) | 3.05 ± 0.15 (2.77, 3.34) ӿ | p = 0.000 |
| 2 | 2.33 ± 0.15 (2.03, 2.63) ¥ | 2.64 ± 0.15 (2.34, 2.94) | 2.91 ± 0.15 (2.61, 3.21) ӿ | p = 0.030 | |
| HDL-C (mmol/L) | 1 | 1.69 ± 0.06 (1.58, 1.81) | 1.68 ± 0.06 (1.56, 1.79) | 1.52 ± 0.06 (1.40, 1.64) | p = 0.087 |
| 2 | 1.78 ± 0.06 (1.67, 1.90) †¥ | 1.55 ± 0.06 (1.43, 1.67) ӿ | 1.57 ± 0.06 (1.45, 1.69) ӿ | p = 0.010 | |
| Total:HDL-C | 1 | 3.25 ± 0.12 (3.00, 3.49) | 3.33 ± 0.12 (3.09, 3.75) | 3.53 ± 0.12 (3.29, 3.77) | p = 0.249 |
| 2 | 3.07 ± 0.12 (2.83, 3.31) †¥ | 3.54 ± 0.12 (3.30, 3.78) ӿ | 3.49 ± 0.12 (3.25, 3.73) ӿ | p = 0.012 | |
| SBP (mmHg) | 1 | 124.7 ± 1.9 (121.0, 128.5) | 124.3 ± 1.9 (120.5, 128.1) | 129.6 ± 1.9 (125.9, 133.3) | p = 0.093 |
| 2 | 124.9 ± 1.8 (121.2, 128.5) ¥ | 122.7 ± 1.9 (119.0, 126.4) ¥ | 131.1 ± 1.8 (127.5, 134.8) ӿ† | p = 0.005 | |
| DBP (mmHg) | 1 | 70.9 ± 1.2 (68.4, 73.3) | 71.8 ± 1.3 (69.4, 74.3) | 72.9 ± 1.2 (70.5, 75.3) | p = 0.502 |
| 2 | 71.1 ± 1.2 (68.6, 73.5) | 71.3 ± 1.2 (68.9, 73.8) | 73.2 ± 1.2 (70.8, 75.6) | p = 0.414 | |
| HR (bpm) | 1 | 65.0 ± 1.1 (62.9, 67.2) † | 68.9 ± 1.1 (66.7, 71.1) ӿ | 66.7 ± 1.1 (64.6, 68.8) | p = 0.045 |
| 2 | 66.2 ± 1.1 (64.0, 68.4) | 68.3 ± 1.1 (66.1, 70.5) | 66.1 ± 1.1 (63.9, 68.3) | p = 0.290 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clark, J.S.; Dyer, K.A.; Davis, C.R.; Shivappa, N.; Hébert, J.R.; Woodman, R.; Hodgson, J.M.; Murphy, K.J. Adherence to a Mediterranean Diet for 6 Months Improves the Dietary Inflammatory Index in a Western Population: Results from the MedLey Study. Nutrients 2023, 15, 366. https://doi.org/10.3390/nu15020366
Clark JS, Dyer KA, Davis CR, Shivappa N, Hébert JR, Woodman R, Hodgson JM, Murphy KJ. Adherence to a Mediterranean Diet for 6 Months Improves the Dietary Inflammatory Index in a Western Population: Results from the MedLey Study. Nutrients. 2023; 15(2):366. https://doi.org/10.3390/nu15020366
Chicago/Turabian StyleClark, Jessie S., Kathryn A. Dyer, Courtney R. Davis, Nitin Shivappa, James R. Hébert, Richard Woodman, Jonathan M. Hodgson, and Karen J. Murphy. 2023. "Adherence to a Mediterranean Diet for 6 Months Improves the Dietary Inflammatory Index in a Western Population: Results from the MedLey Study" Nutrients 15, no. 2: 366. https://doi.org/10.3390/nu15020366
APA StyleClark, J. S., Dyer, K. A., Davis, C. R., Shivappa, N., Hébert, J. R., Woodman, R., Hodgson, J. M., & Murphy, K. J. (2023). Adherence to a Mediterranean Diet for 6 Months Improves the Dietary Inflammatory Index in a Western Population: Results from the MedLey Study. Nutrients, 15(2), 366. https://doi.org/10.3390/nu15020366