
Postoperative Probiotics Administration Attenuates Gastrointestinal Complications and Gut Microbiota Dysbiosis Caused by Chemotherapy in Colorectal Cancer Patients

 , ,
, ,  ,
,  and
and Highlights
- Earlier research confirmed the improved effectiveness of probiotic preparations in cancer treatment.
- We thoroughly elucidated the role of the gut microbiota and its metabolites in cancer development by combining high-throughput sequencing and metabolomics.
- This study provided a new treatment strategy to alleviate the side effects of gastrointestinal dysfunction caused by chemotherapy in CRC patients, and it also expanded new indications for the probiotic product in cancer adjuvant improvement.
Abstract
1. Introduction
2. Materials and Methods
2.1. Probiotic and Placebo Tablets
2.2. Participants
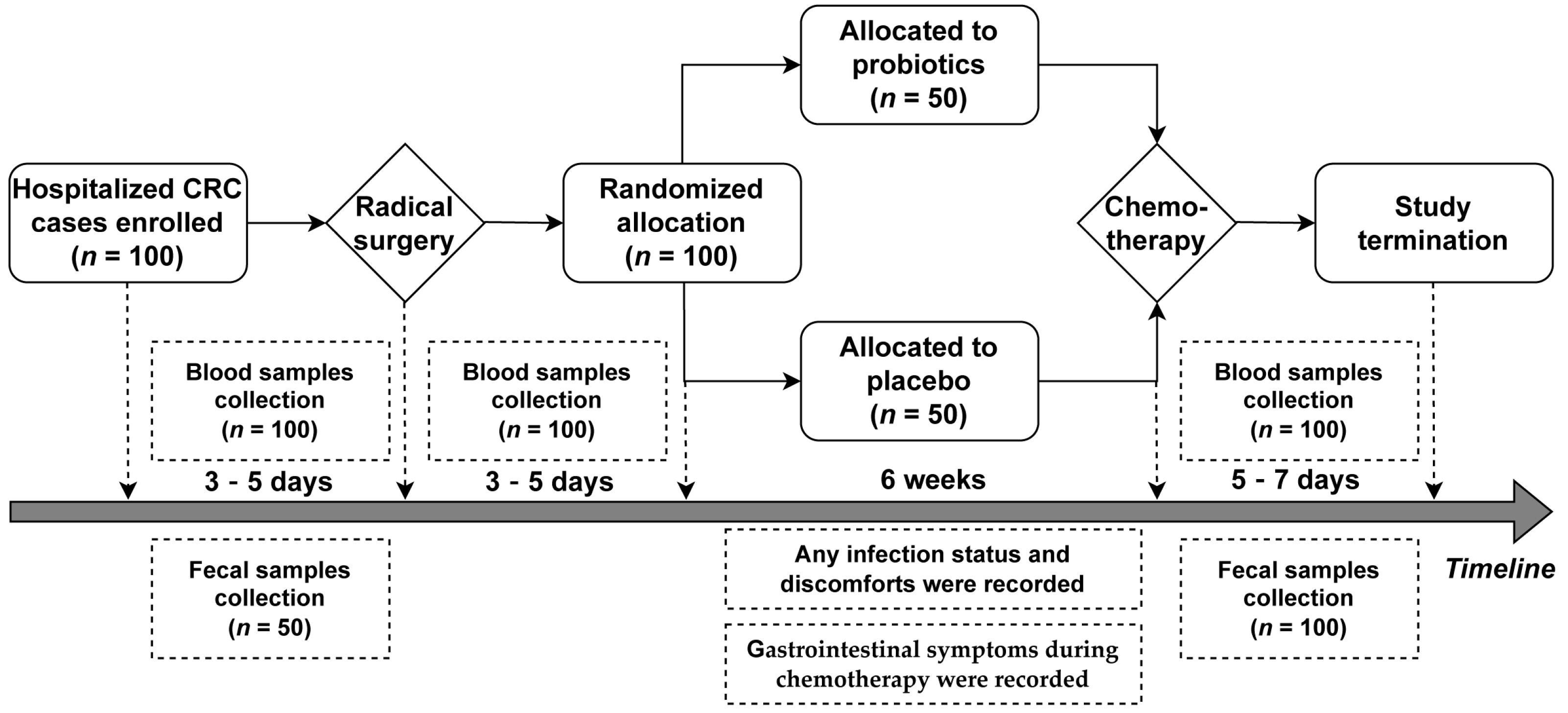
2.3. Treatment Procedure
2.4. Microbial DNA Extraction and 16S rRNA Sequencing Analysis
2.5. Detection of Short Chain Fatty Acids (SCFAs)
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of CRC Patients
3.2. Probiotics Improve Gastrointestinal Complications Induced by Chemotherapy
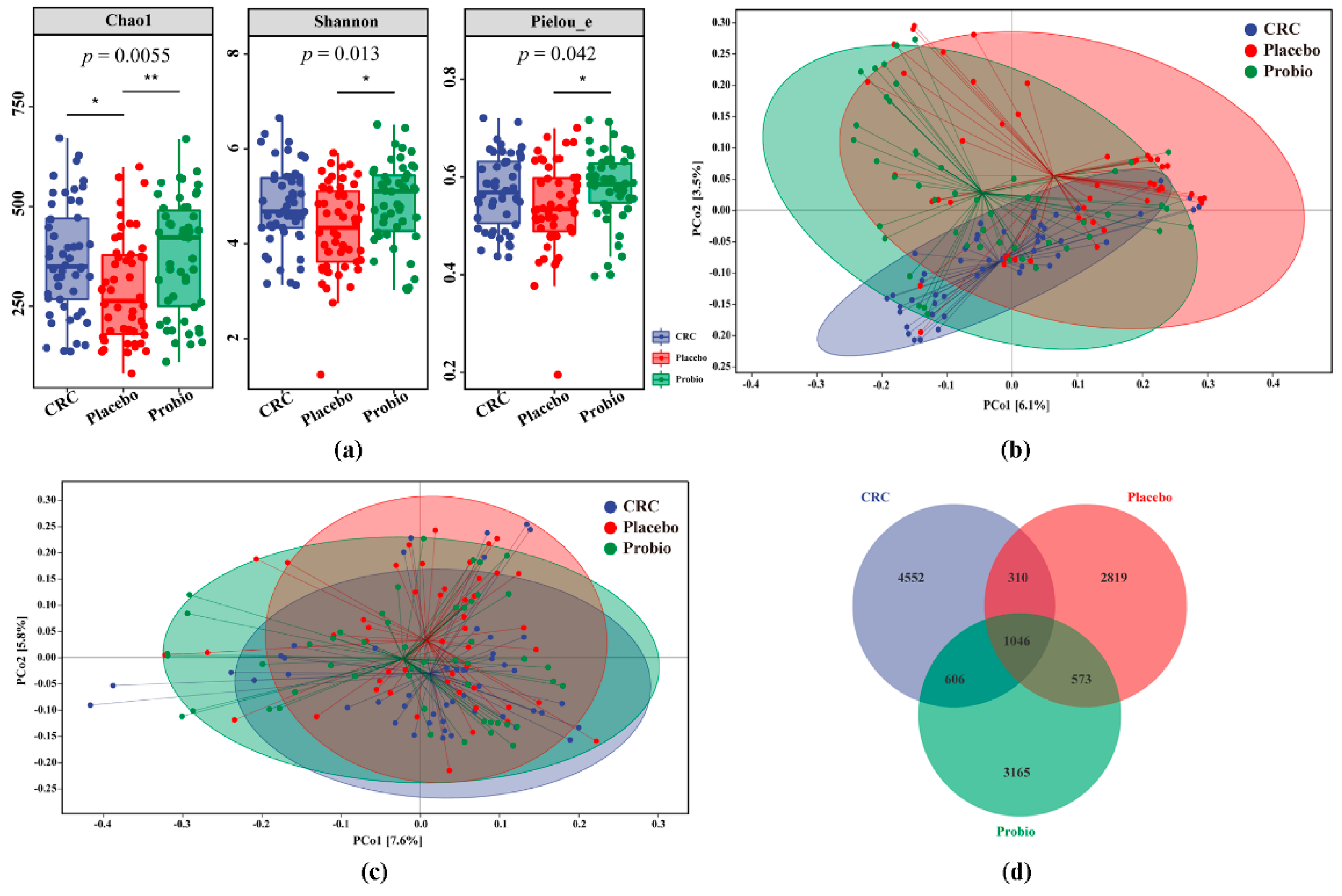
3.3. Probiotics Remodel the Disturbed Intestinal Bacterial Diversity
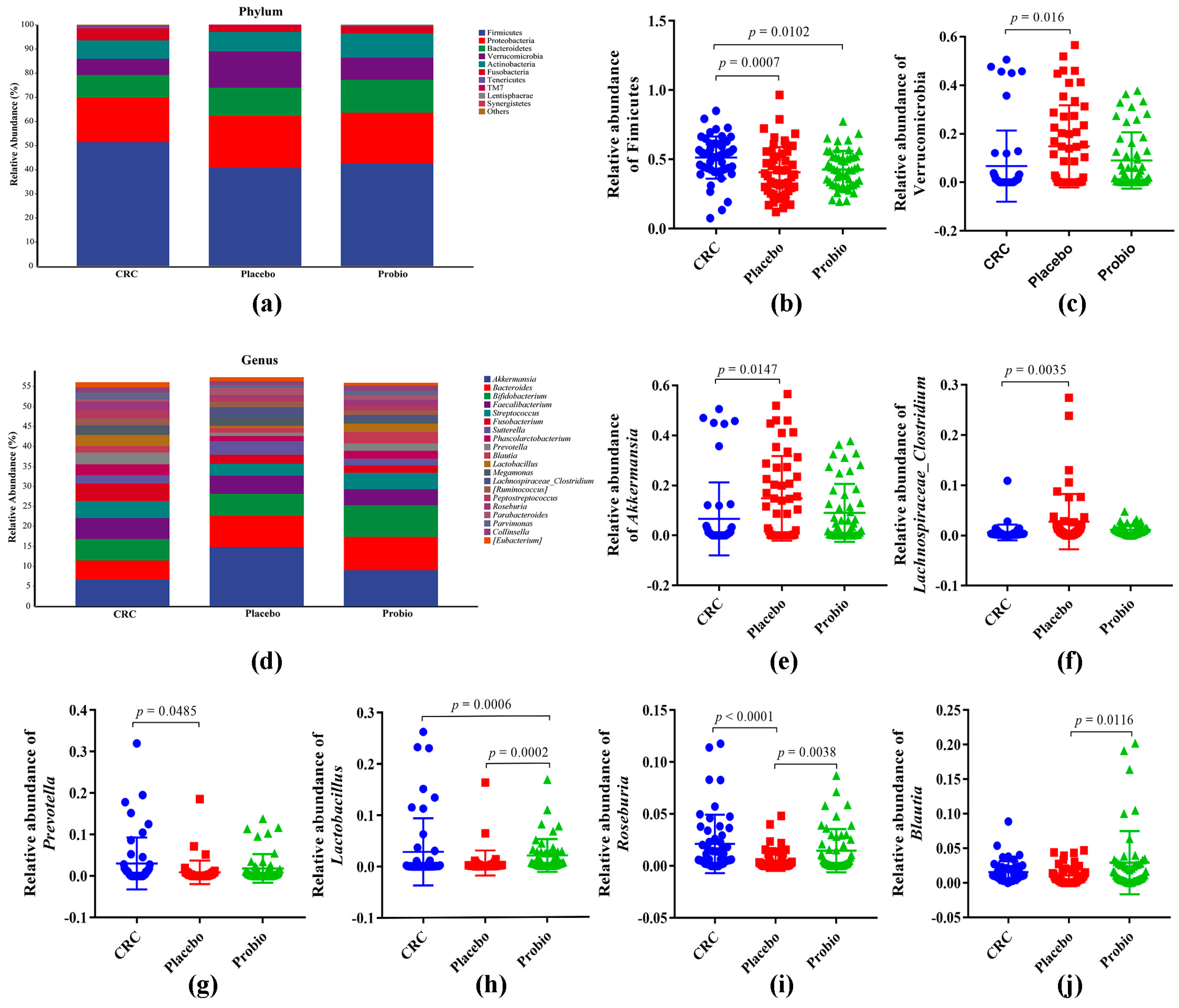
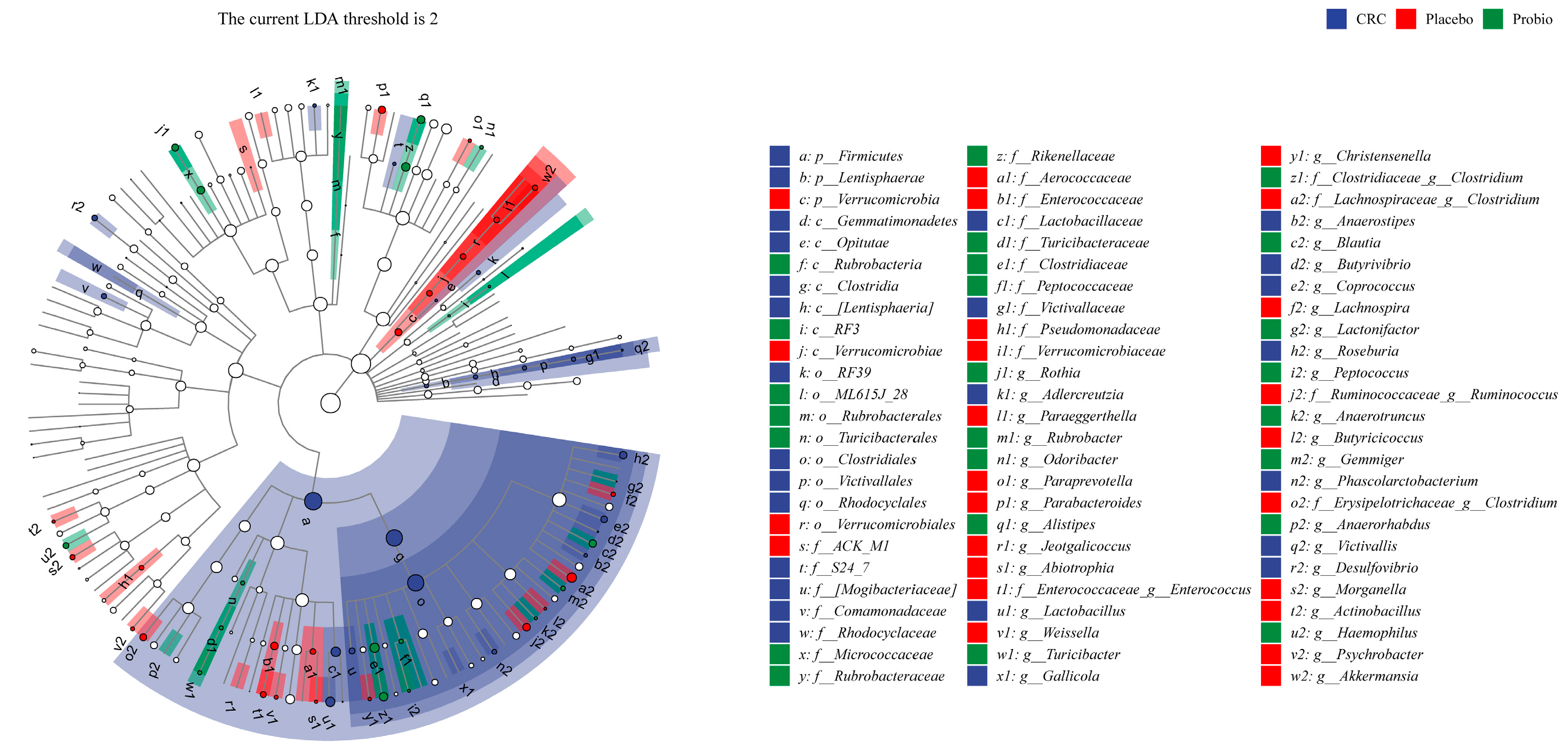
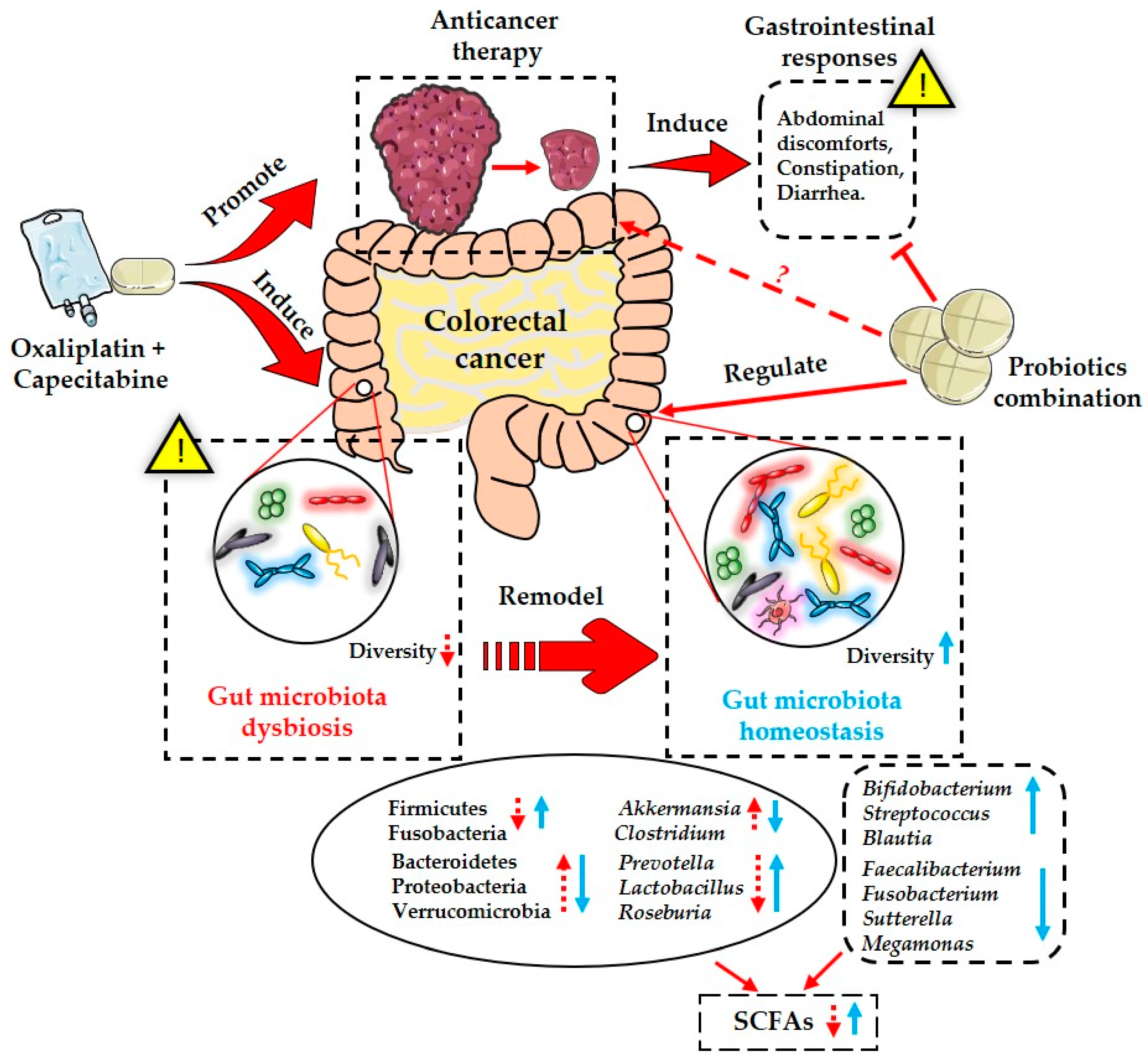
3.4. Probiotics Restore the Changed Gut Bacterial Taxa
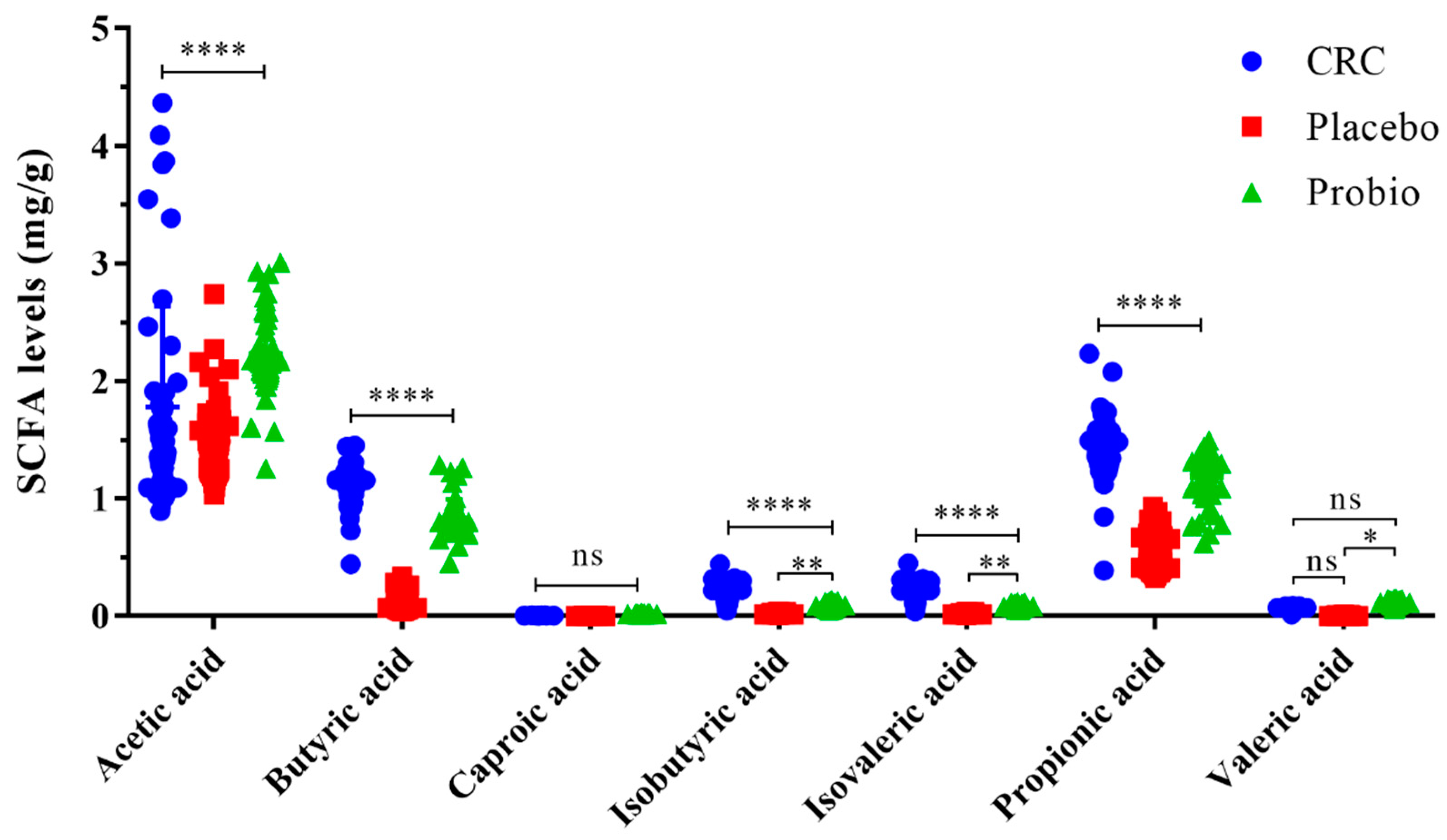
3.5. Probiotics Increase the Production of Intestinal SCFAs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Yoshino, T.; Arnold, D.; Taniguchi, H.; Pentheroudakis, G.; Yamazaki, K.; Xu, R.H.; Kim, T.W.; Ismail, F.; Tan, I.B.; Yeh, K.H.; et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: A JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann. Oncol. 2018, 29, 44–70. [Google Scholar] [CrossRef]
- Almasaudi, A.S.; McSorley, S.T.; Edwards, C.A.; McMillan, D.C. The relationship between body mass index and short term postoperative outcomes in patients undergoing potentially curative surgery for colorectal cancer: A systematic review and meta-analysis. Crit. Rev. Oncol./Hematol. 2018, 121, 68–73. [Google Scholar] [CrossRef]
- Yixia, Y.; Sripetchwandee, J.; Chattipakorn, N.; Chattipakorn, S.C. The alterations of microbiota and pathological conditions in the gut of patients with colorectal cancer undergoing chemotherapy. Anaerobe 2021, 68, 102361. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, K.; Kawai, K.; Tanaka, T.; Hata, K.; Sugihara, K.; Nozawa, H. Prognostic impact of interhospital variation in adjuvant chemotherapy for patients with Stage II/III colorectal cancer: A nationwide study. Color. Dis. 2018, 20, O162–O172. [Google Scholar] [CrossRef]
- Cunningham, D.; Morgan, R.J.; Mills, P.R.; Nelson, L.M.; Toner, P.G.; Soukop, M.; McArdle, C.S.; Russell, R.I. Functional and structural changes of the human proximal small intestine after cytotoxic therapy. J. Clin. Pathol. 1985, 38, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; He, K.; Duan, X.; Xiao, J.; Wang, H.; Xiang, G. Changes of Intestinal Microflora in Colorectal Cancer Patients after Surgical Resection and Chemotherapy. Comput. Math. Methods Med. 2022, 2022, 1940846. [Google Scholar] [CrossRef]
- Kong, C.; Gao, R.; Yan, X.; Huang, L.; He, J.; Li, H.; You, J.; Qin, H. Alterations in intestinal microbiota of colorectal cancer patients receiving radical surgery combined with adjuvant CapeOx therapy. Sci. China Life Sci. 2019, 62, 1178–1193. [Google Scholar] [CrossRef]
- Deng, X.; Li, Z.; Li, G.; Li, B.; Jin, X.; Lyu, G. Comparison of Microbiota in Patients Treated by Surgery or Chemotherapy by 16S rRNA Sequencing Reveals Potential Biomarkers for Colorectal Cancer Therapy. Front. Microbiol. 2018, 9, 1607. [Google Scholar] [CrossRef]
- Zhang, S.; Yang, Y.; Weng, W.; Guo, B.; Cai, G.; Ma, Y.; Cai, S. Fusobacterium nucleatum promotes chemoresistance to 5-fluorouracil by upregulation of BIRC3 expression in colorectal cancer. J. Exp. Clin. Cancer Res. 2019, 38, 14. [Google Scholar] [CrossRef]
- Wang, C.H.; Yang, S.X.; Gao, L.; Wang, L.L.; Cao, L. Carboxymethyl pachyman (CMP) reduces intestinal mucositis and regulates the intestinal microflora in 5-fluorouracil-treated CT26 tumour-bearing mice. Food Funct. 2018, 9, 2695–2704. [Google Scholar] [CrossRef]
- Hou, H.; Chen, D.; Zhang, K.; Zhang, W.; Liu, T.; Wang, S.; Dai, X.; Wang, B.; Zhong, W.; Cao, H. Gut microbiota-derived short-chain fatty acids and colorectal cancer: Ready for clinical translation? Cancer Lett. 2022, 526, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.H.; Chen, T.T.; Wang, Y.Q.; Gao, Y.; Kong, Y.; Liu, Z.X.; Deng, X.R. A randomised trial of probiotics to reduce severity of physiological and microbial disorders induced by partial gastrectomy for patients with gastric cancer. J. Cancer 2019, 10, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.F.; Jiang, C.L.; Li, W.Y.; Wei, J.; Hong, H.; Li, J.G.; Feng, L.; Wei, H.; Xin, H.B.; Chen, T.T. A Phase II Randomized Clinical Trial and Mechanistic Studies Using Improved Probiotics to Prevent Oral Mucositis Induced by Concurrent Radiotherapy and Chemotherapy in Nasopharyngeal Carcinoma. Front. Immunol. 2021, 12, 618150. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, K.G.; Liu, P.; Xu, X.; Zhou, Y.Y.; Gan, L.H.; Yao, L.; Li, B.; Chen, T.T.; Fang, N. Improvement Effect of Bifidobacterium animalis subsp. lactis MH-02 in Patients Receiving Resection of Colorectal Polyps: A Randomized, Double-Blind, Placebo-Controlled Trial. Front. Immunol. 2022, 13, 940500. [Google Scholar] [CrossRef]
- Jiang, C.L.; Wang, H.; Xia, C.F.; Dong, Q.; Chen, E.; Qiu, Y.; Su, Y.; Xie, H.H.; Zeng, L.; Kuang, J.; et al. A randomized, double-blind, placebo-controlled trial of probiotics to reduce the severity of oral mucositis induced by chemoradiotherapy for patients with nasopharyngeal carcinoma. Cancer-Am. Cancer Soc. 2019, 125, 1081–1090. [Google Scholar] [CrossRef]
- Zheng, C.; Chen, T.; Lu, J.; Wei, K.; Tian, H.; Liu, W.; Xu, T.; Wang, X.; Wang, S.; Yang, R.; et al. Adjuvant treatment and molecular mechanism of probiotic compounds in patients with gastric cancer after gastrectomy. Food Funct. 2021, 12, 6294–6308. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef]
- Bianchi, F.; Dall’Asta, M.; Del Rio, D.; Mangia, A.; Musci, M.; Scazzina, F. Development of a headspace solid-phase microextraction gas chromatography-mass spectrometric method for the determination of short-chain fatty acids from intestinal fermentation. Food Chem. 2011, 129, 200–205. [Google Scholar] [CrossRef]
- Zhao, G.; Nyman, M.; Jonsson, J.A. Rapid determination of short-chain fatty acids in colonic contents and faeces of humans and rats by acidified water-extraction and direct-injection gas chromatography. Biomed. Chromatogr. 2006, 20, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Chu, L.; Wang, Y.; Song, Y.; Liu, P.; Li, C.; Huang, J.; Kang, X. Application of packed-fiber solid-phase extraction coupled with GC-MS for the determination of short-chain fatty acids in children’s urine. Clin. Chim. Acta 2017, 468, 120–125. [Google Scholar] [CrossRef]
- Darbandi, A.; Mirshekar, M.; Shariati, A.; Moghadam, M.T.; Lohrasbi, V.; Asadolahi, P.; Talebi, M. The effects of probiotics on reducing the colorectal cancer surgery complications: A periodic review during 2007–2017. Clin. Nutr. 2020, 39, 2358–2367. [Google Scholar] [CrossRef]
- Tang, G.; Zhang, L. Update on Strategies of Probiotics for the Prevention and Treatment of Colorectal Cancer. Nutr. Cancer 2022, 74, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Shen, Y. The efficacy and safety of probiotics for prevention of chemoradiotherapy-induced diarrhea in people with abdominal and pelvic cancer: A systematic review and meta-analysis based on 23 randomized studies. Int. J. Surg. 2020, 84, 69–77. [Google Scholar] [CrossRef]
- Osterlund, P.; Ruotsalainen, T.; Korpela, R.; Saxelin, M.; Ollus, A.; Valta, P.; Kouri, M.; Elomaa, I.; Joensuu, H. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: A randomised study. Br. J. Cancer 2007, 97, 1028–1034. [Google Scholar] [CrossRef]
- Golkhalkhali, B.; Paliany, A.S.; Chin, K.F.; Rajandram, R. The Roles of Adjuvant Supplements in Colorectal Cancer Patients on Chemotherapy-Reaping Benefits from Metabolic Crosstalk. Nutr. Cancer 2018, 70, 184–191. [Google Scholar] [CrossRef]
- Mizuta, M.; Endo, I.; Yamamoto, S.; Inokawa, H.; Kubo, M.; Udaka, T.; Sogabe, O.; Maeda, H.; Shirakawa, K.; Okazaki, E.; et al. Perioperative supplementation with bifidobacteria improves postoperative nutritional recovery, inflammatory response, and fecal microbiota in patients undergoing colorectal surgery: A prospective, randomized clinical trial. Biosci. Microbiota Food Health 2016, 35, 77–87. [Google Scholar] [CrossRef]
- Gao, Z.; Guo, B.; Gao, R.; Zhu, Q.; Wu, W.; Qin, H. Probiotics modify human intestinal mucosa-associated microbiota in patients with colorectal cancer. Mol. Med. Rep. 2015, 12, 6119–6127. [Google Scholar] [CrossRef]
- Yuan, L.; Zhang, S.; Li, H.; Yang, F.; Mushtaq, N.; Ullah, S.; Shi, Y.; An, C.; Xu, J. The influence of gut microbiota dysbiosis to the efficacy of 5-Fluorouracil treatment on colorectal cancer. Biomed. Pharmacother. 2018, 108, 184–193. [Google Scholar] [CrossRef]
- Chang, C.W.; Liu, C.Y.; Lee, H.C.; Huang, Y.H.; Li, L.H.; Chiau, J.C.; Wang, T.E.; Chu, C.H.; Shih, S.C.; Tsai, T.H.; et al. Lactobacillus casei Variety rhamnosus Probiotic Preventively Attenuates 5-Fluorouracil/Oxaliplatin-Induced Intestinal Injury in a Syngeneic Colorectal Cancer Model. Front. Microbiol. 2018, 9, 983. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Zhao, Y.Z.; Yang, Y.; Wang, T.J.; Jin, S.Z.; Guo, J.; Liu, Z.S. The protective role of short-chain fatty acids acting as signal molecules in chemotherapy- or radiation-induced intestinal inflammation. Am. J. Cancer Res. 2020, 10, 3508–3531. [Google Scholar] [PubMed]
- Al-Qadami, G.H.; Secombe, K.R.; Subramaniam, C.B.; Wardill, H.R.; Bowen, J.M. Gut Microbiota-Derived Short-Chain Fatty Acids: Impact on Cancer Treatment Response and Toxicities. Microorganisms 2022, 10, 2048. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Placebo Group (n = 50) | Probiotics Group (n = 50) | p Value |
|---|---|---|---|
| Gender (male/female) | 29/21 | 24/26 | 0.316 |
| Age (year) | 62.1 ± 10.5 | 57.7 ± 11.9 | 0.053 |
| Tumor category | 0.326 | ||
| T0 | 0 | 0 | |
| T1 | 2 | 1 | |
| T2 | 10 | 13 | |
| T3 | 31 | 34 | |
| T4 | 7 | 2 | |
| Node category | 0.614 | ||
| N0 | 30 | 30 | |
| N1 | 10 | 13 | |
| N2 | 10 | 7 | |
| Metastasis category | |||
| M0 | 50 | 50 | / |
| TNM category | 0.891 | ||
| I | 8 | 6 | |
| II | 21 | 24 | |
| III | 21 | 20 | |
| Location of tumor | 0.603 | ||
| Right colon | 15 | 11 | |
| Left colon | 6 | 6 | |
| Sigmoid colon | 10 | 11 | |
| Rectum | 19 | 22 |
| Group | n | Nausea (%) | Acid Reflux (%) | Abdominal Pain (%) | Abdominal Distention (%) | Constipation (%) | Diarrhea (%) |
|---|---|---|---|---|---|---|---|
| Probio | 50 | 11 (22.00) | 2 (4.00) | 3 (6.00) | 5 (10.00) | 4 (8.00) | 8 (16.00) |
| Placebo | 50 | 17 (34.00) | 6 (12.00) | 12 (24.00) | 14 (28.00) | 14 (28.00) | 20 (40.00) |
| χ2 | 1.786 | 1.223 | 5.020 | 4.159 | 5.488 | 7.143 | |
| p value | 0.181 | 0.169 | 0.025 | 0.041 | 0.019 | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, F.; Li, S.; Chen, W.; Han, Y.; Yao, Y.; Yang, L.; Li, Q.; Xiao, Q.; Wei, J.; Liu, Z.; et al. Postoperative Probiotics Administration Attenuates Gastrointestinal Complications and Gut Microbiota Dysbiosis Caused by Chemotherapy in Colorectal Cancer Patients. Nutrients 2023, 15, 356. https://doi.org/10.3390/nu15020356
Huang F, Li S, Chen W, Han Y, Yao Y, Yang L, Li Q, Xiao Q, Wei J, Liu Z, et al. Postoperative Probiotics Administration Attenuates Gastrointestinal Complications and Gut Microbiota Dysbiosis Caused by Chemotherapy in Colorectal Cancer Patients. Nutrients. 2023; 15(2):356. https://doi.org/10.3390/nu15020356
Chicago/Turabian StyleHuang, Feng, Shengjie Li, Wenjie Chen, Yiyang Han, Yue Yao, Liang Yang, Qiang Li, Qun Xiao, Jing Wei, Zhaoxia Liu, and et al. 2023. "Postoperative Probiotics Administration Attenuates Gastrointestinal Complications and Gut Microbiota Dysbiosis Caused by Chemotherapy in Colorectal Cancer Patients" Nutrients 15, no. 2: 356. https://doi.org/10.3390/nu15020356
APA StyleHuang, F., Li, S., Chen, W., Han, Y., Yao, Y., Yang, L., Li, Q., Xiao, Q., Wei, J., Liu, Z., Chen, T., & Deng, X. (2023). Postoperative Probiotics Administration Attenuates Gastrointestinal Complications and Gut Microbiota Dysbiosis Caused by Chemotherapy in Colorectal Cancer Patients. Nutrients, 15(2), 356. https://doi.org/10.3390/nu15020356