

Serum Magnesium Is Associated with Long-Term Survival of Non-ST-Elevation Myocardial Infarction Patients

 ,
,  , , ,
, , , 
Highlights
- Low serum magnesium levels are not an infrequent occurrence in hospitalized NSTEMI patients.
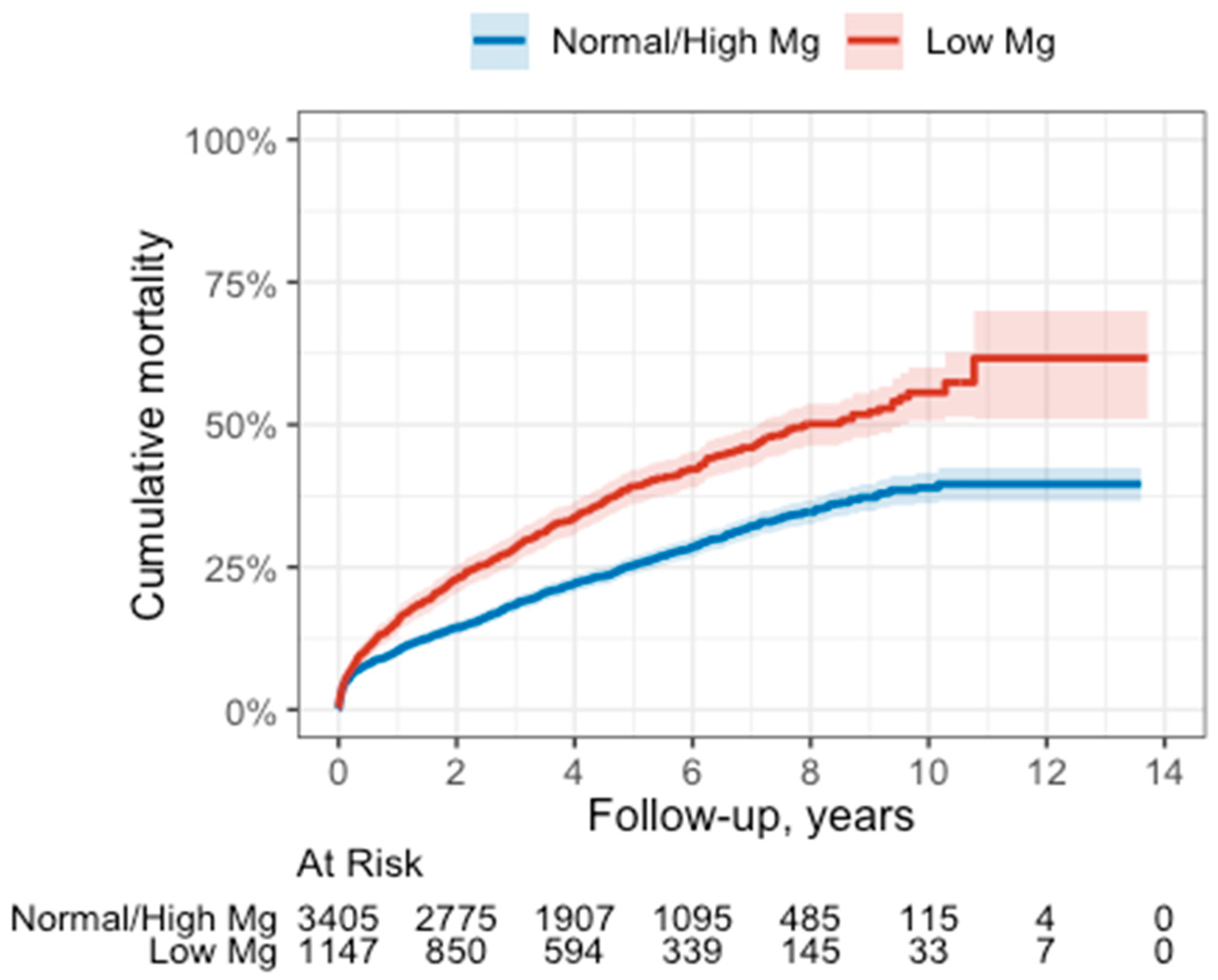
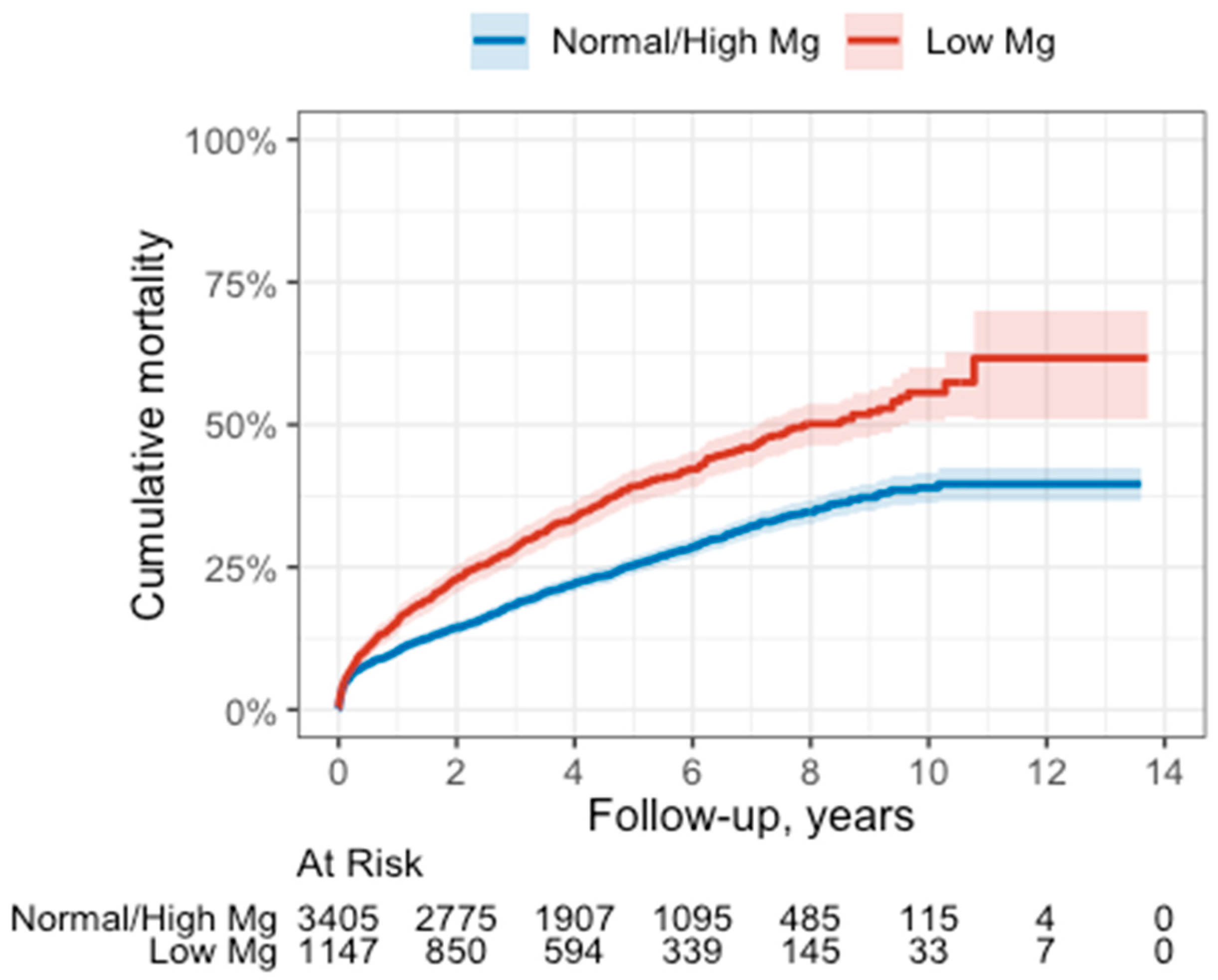
- Serum magnesium levels in NSTEMI patients upon admission were associated with long-term all-cause mortality, even after adjustments for demographic and clinical variables.
- Low serum magnesium levels upon admission may serve as an available, relatively inexpensive, and fast biomarker for poor outcomes and aid in the risk stratification of NSTEMI patients.
Abstract
:1. Introduction
2. Methods
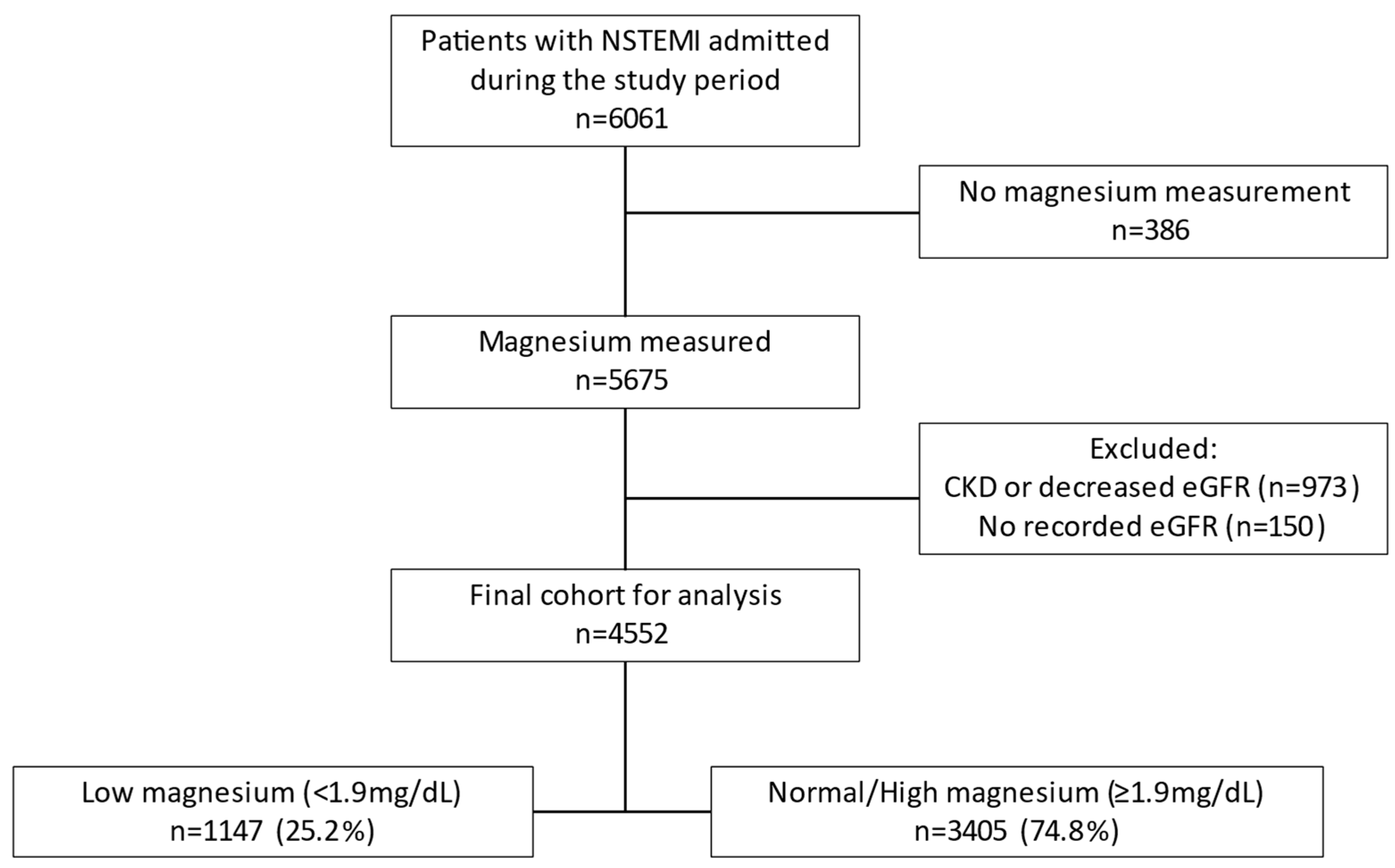
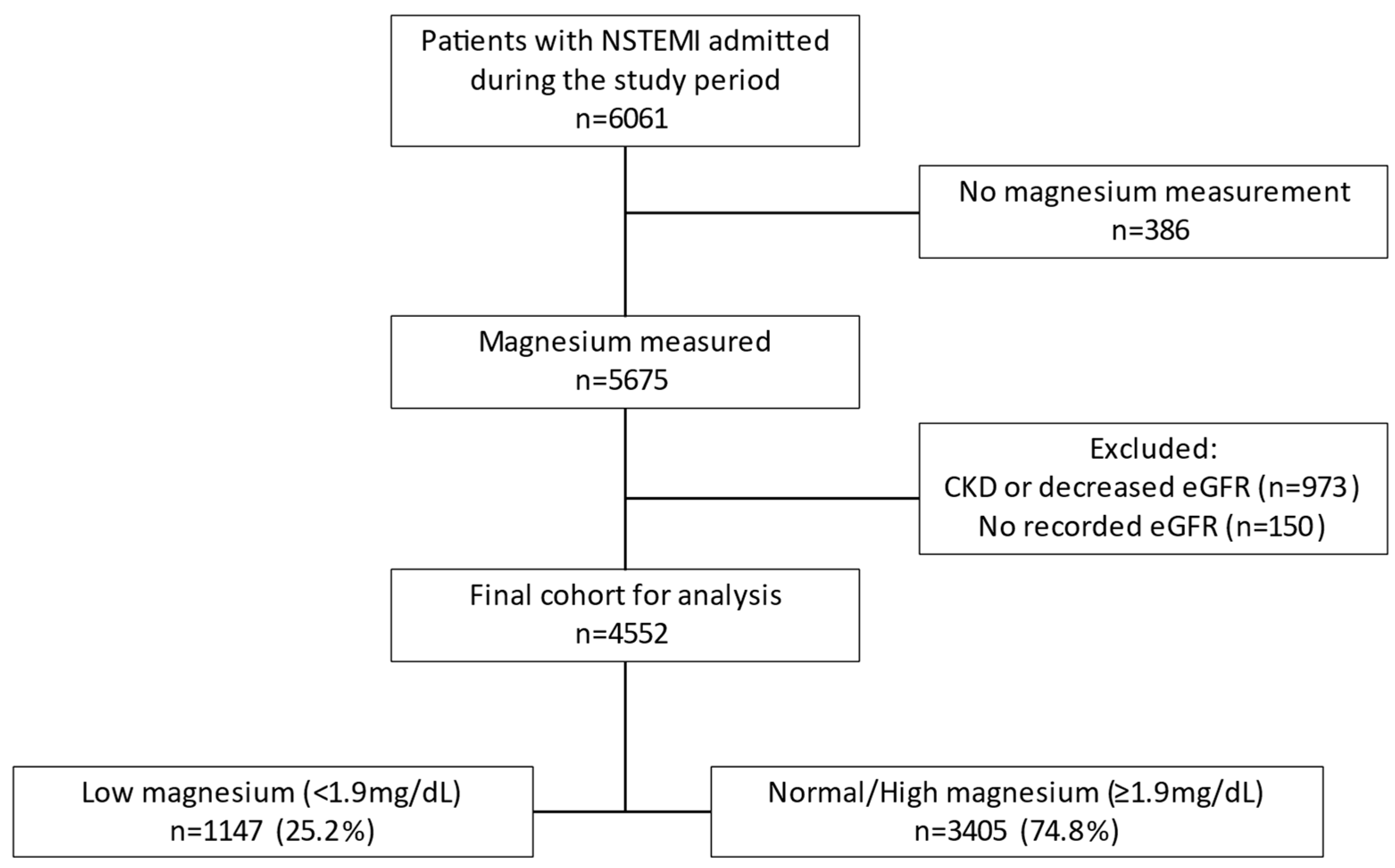
2.1. Study Population
2.2. Study Variables and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Subanalysis by Sex
3.2. Survival during Follow-Up
4. Discussion
5. Conclusions
6. Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seelig, M.S. Consequences of magnesium deficiency on the enhancement of stress reactions; preventive and therapeutic implications (a review). J. Am. Coll. Nutr. 1994, 13, 429–446. [Google Scholar] [CrossRef]
- Saris, N.-E.L.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium. Clin. Chim. Acta. 2000, 294, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Cai, D.; Zhao, S.; Li, D.; Chang, F.; Tian, X.; Huang, G.; Zhu, Z.; Liu, D.; Dou, X.; Li, S.; et al. Nutrient Intake Is Associated with Longevity Characterization by Metabolites and Element Profiles of Healthy Centenarians. Nutrients 2016, 8, 564. [Google Scholar] [CrossRef] [PubMed]
- Maier, J.A.; Malpuech-Brugère, C.; Zimowska, W.; Rayssiguier, Y.; Mazur, A. Low magnesium promotes endothelial cell dysfunction: Implications for atherosclerosis, inflammation and thrombosis. Biochim. Biophys. Acta-Mol. Basis Dis. 2004, 1689, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Pearson, P.J.; Evora, P.R.B.; Seccombe, J.F.; Schaff, H.V. Hypomagnesemia Inhibits Nitric Oxide Release From Coronary Endothelium: Protective Role of Magnesium Infusion after Cardiac Operations. Ann. Thorac. Surg. 1998, 65, 967–972. [Google Scholar] [CrossRef]
- Shechter, M.; Sharir, M.; Labrador, M.J.P.; Forrester, J.; Silver, B.; Bairey Merz, C.N. Oral Magnesium Therapy Improves Endothelial Function in Patients with Coronary Artery Disease. Circulation 2000, 102, 2353–2358. [Google Scholar] [CrossRef]
- Iseri, L.T.; French, J.H. Magnesium: Nature’s physiologic calcium blocker. Am. Heart J. 1984, 108, 188–193. [Google Scholar] [CrossRef]
- Rasmussen, H.S.; Larsen, O.G.; Meier, K.; Larsen, J. Hemodynamic effects of intravenously administered magnesium on patients with ischemic heart disease. Clin. Cardiol. 1988, 11, 824–828. [Google Scholar] [CrossRef]
- Sugiyama, A.; Xue, Y.; Hagihara, A.; Saitoh, M.; Hashimoto, K. Characterization of Magnesium Sulfate as an Antiarrhythmic Agent. J. Cardiovasc. Pharmacol. Ther. 1996, 1, 243–254. [Google Scholar] [CrossRef]
- Fiset, C.; Kargacin, M.E.; Kondo, C.S.; Lester, W.M.; Duff, H.J. Hypomagnesemia: Characterization of a model of sudden cardiac death. J. Am. Coll. Cardiol. 1996, 27, 1771–1776. [Google Scholar] [CrossRef]
- Davidenko, J.M.; Cohen, L.; Goodrow, R.; Antzelevitch, C. Quinidine-induced action potential prolongation, early afterdepolarizations, and triggered activity in canine Purkinje fibers. Effects of stimulation rate, potassium, and magnesium. Circulation 1989, 79, 674–686. [Google Scholar] [CrossRef] [PubMed]
- Verduyn, S. Role of interventricular dispersion of repolarization in acquired torsade-de-pointes arrhythmias: Reversal by magnesium. Cardiovasc. Res. 1997, 34, 453–463. [Google Scholar] [CrossRef]
- Abbott, R.D.; Ando, F.; Masaki, K.H.; Tung, K.-H.; Rodriguez, B.L.; Petrovitch, H.; Yano, K.; Curb, J.D. Dietary magnesium intake and the future risk of coronary heart disease (The Honolulu Heart Program). Am. J. Cardiol. 2003, 92, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Fishman, B.; Sharon, A.; Itelman, E.; Tsur, A.M.; Fefer, P.; Barbash, I.M.; Segev, A.; Matetzky, S.; Guetta, V.; Grossman, E.; et al. Invasive Management in Older Adults (≥80 Years) with Non-ST Elevation Myocardial Infarction. Mayo Clin. Proc. 2022, 97, 1247–1256. [Google Scholar] [CrossRef]
- Sharon, A.; Massalha, E.; Fishman, B.; Fefer, P.; Barbash, I.M.; Segev, A.; Matetzky, S.; Guetta, V.; Grossman, E.; Maor, E. Early Invasive Strategy and Outcome of Non–ST-Segment Elevation Myocardial Infarction Patients with Chronic Kidney Disease. JACC Cardiovasc. Interv. 2022, 15, 1977–1988. [Google Scholar] [CrossRef] [PubMed]
- Sharon, A.; Fishman, B.; Massalha, E.; Itelman, E.; Mouallem, M.; Fefer, P.; Barbash, I.M.; Segev, A.; Matetzky, S.; Guetta, V.; et al. Management and outcome of patients with non-ST elevation myocardial infarction and intercurrent non-coronary precipitating events. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 922–930. [Google Scholar] [CrossRef]
- Coburn, J.W.; Popovtzer, M.M.; Massry, S.G.; Kleeman, C.R. The physicochemical state and renal handling of divalent ions in chronic renal failure. Arch. Intern. Med. 1969, 124, 302–311. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Fujii, N.; Shoji, T.; Hayashi, T.; Rakugi, H.; Isaka, Y. Hypomagnesemia is a significant predictor of cardiovascular and non-cardiovascular mortality in patients undergoing hemodialysis. Kidney Int. 2014, 85, 174–181. [Google Scholar] [CrossRef]
- Van Laecke, S.; Nagler, E.V.; Verbeke, F.; Van Biesen, W.; Vanholder, R. Hypomagnesemia and the Risk of Death and GFR Decline in Chronic Kidney Disease. Am. J. Med. 2013, 126, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Segev, A.; Sagir, A.; Matetzky, S.; Segev, A.; Atar, S.; Shechter, M. Admission Serum Magnesium Levels Is Associated with Short and Long-Term Clinical Outcomes in COVID-19 Patients. Nutrients 2023, 15, 2016. [Google Scholar] [CrossRef]
- Schimatschek, H.F.; Rempis, R. Prevalence of hypomagnesemia in an unselected German population of 16,000 individuals. Magnes. Res. 2001, 14, 283–290. [Google Scholar] [PubMed]
- Rosanoff, A.; West, C.; Elin, R.J.; Micke, O.; Baniasadi, S.; Barbagallo, M.; Campbell, E.; Cheng, F.-C.; Costello, R.B.; Gamboa-Gomez, C.; et al. Recommendation on an updated standardization of serum magnesium reference ranges. Eur. J. Nutr. 2022, 61, 3697–3706. [Google Scholar] [CrossRef] [PubMed]
- Micke, O.; Vormann, J.; Kraus, A.; Kisters, K. Serum magnesium: Time for a standardized and evidence-based reference range. Magnes. Res. 2021, 34, 84–89. [Google Scholar] [PubMed]
- Elin, R.J. Status of the determination of magnesium in mononuclear blood cells in humans. Magnesium 1988, 7, 300–305. [Google Scholar] [PubMed]
- Reinhart, R.A. Magnesium metabolism. A review with special reference to the relationship between intracellular content and serum levels. Arch. Intern. Med. 1988, 148, 2415–2420. [Google Scholar] [CrossRef]
- Shechter, M. Magnesium and cardiovascular system. Magnes. Res. 2010, 23, 60–72. [Google Scholar] [PubMed]
- Fordyce, A.; Gouliouk, V.; Henkin, R. Age and gender changes in calcium and magnesium metabolism. FASEB J. 2011, 25, 768.6. [Google Scholar]
- Pham, P.-C.T.; Pham, P.-M.T.; Pham, S.V.; Miller, J.M.; Pham, P.-T.T. Hypomagnesemia in Patients with Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef]
- Larsson, S.C.; Drca, N.; Michaëlsson, K. Serum Magnesium and Calcium Levels and Risk of Atrial Fibrillation. Circ. Genom. Precis. Med. 2019, 12, e002349. [Google Scholar] [CrossRef]
- Liao, F.; Folsom, A.R.; Brancati, F.L. Is low magnesium concentration a risk factor for coronary heart disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 1998, 136, 480–490. [Google Scholar] [CrossRef]
- Gartside, P.S.; Glueck, C.J. The important role of modifiable dietary and behavioral characteristics in the causation and prevention of coronary heart disease hospitalization and mortality: The prospective NHANES I follow-up study. J. Am. Coll. Nutr. 1995, 14, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Amighi, J.; Sabeti, S.; Schlager, O.; Mlekusch, W.; Exner, M.; Lalouschek, W.; Ahmadi, R.; Minar, E.; Schillinger, M. Low Serum Magnesium Predicts Neurological Events in Patients with Advanced Atherosclerosis. Stroke 2004, 35, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Pachikian, B.D.; Neyrinck, A.M.; Deldicque, L.; De Backer, F.C.; Catry, E.; Dewulf, E.M.; Sohet, F.M.; Bindels, L.B.; Everard, A.; Francaux, M.; et al. Changes in Intestinal Bifidobacteria Levels Are Associated with the Inflammatory Response in Magnesium-Deficient Mice. J. Nutr. 2010, 140, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Tsai, P.S.; Hung, Y.C.; Huang, C.J. L-type calcium channels are involved in mediating the anti-inflammatory effects of magnesium sulphate. Br. J. Anaesth. 2010, 104, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Li, T.Y.; van Dam, R.M.; Manson, J.E.; Hu, F.B. Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am. J. Clin. Nutr. 2007, 85, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Holroyde, M.J.; Robertson, S.P.; Johnson, J.D.; Solaro, R.J.; Potter, J.D. The calcium and magnesium binding sites on cardiac troponin and their role in the regulation of myofibrillar adenosine triphosphatase. J. Biol. Chem. 1980, 255, 11688–11693. [Google Scholar] [CrossRef] [PubMed]
- Shechter, M.; Kaplinsky, E.; Rabinowitz, B. The rationale of magnesium supplementation in acute myocardial infarction. A Rev. Lit. Arch. Intern. Med. 1992, 152, 2189–2196. [Google Scholar] [CrossRef]
- Ford, E.S. Serum magnesium and ischaemic heart disease: Findings from a national sample of US adults. Int. J. Epidemiol. 1999, 28, 645–651. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Korngold, E.C.; Januzzi, J.L.; Gantzer, M.L.; Albert, C.M. Plasma and dietary magnesium and risk of sudden cardiac death in women. Am. J. Clin. Nutr. 2011, 93, 253–260. [Google Scholar] [CrossRef]
- Antman, E.M. Early administration of intravenous magnesium to high-risk patients with acute myocardial infarction in the Magnesium in Coronaries (MAGIC) Trial: A randomised controlled trial. Lancet 2002, 360, 1189–1196. [Google Scholar] [CrossRef]
- Ceremużyński, L.; Van Hao, N. Ventricular arrhythmias late after myocardial infarction are related to hypomagnesemia and magnesium loss: Preliminary trial of corrective therapy. Clin. Cardiol. 1993, 16, 493–496. [Google Scholar] [CrossRef]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef]
- Larsson, S.C.; Burgess, S.; Michaëlsson, K. Serum magnesium levels and risk of coronary artery disease: Mendelian randomisation study. BMC Med. 2018, 16, 68. [Google Scholar] [CrossRef]
- Shechter, M.; Merz, C.B.; Rude, R.K.; Labrador, M.J.P.; Meisel, S.R.; Shah, P.K.; Kaul, S. Low intracellular magnesium levels promote platelet-dependent thrombosis in patients with coronary artery disease. Am. Heart J. 2000, 140, 212–218. [Google Scholar] [CrossRef]
- Gawaz, M.; Reininger, A.; Neumann, F.-J. Platelet function and platelet-leukocyte adhesion in symptomatic coronary heart disease. effects of intravenous magnesium. Thromb. Res. 1996, 83, 341–349. [Google Scholar] [CrossRef]
- Adams, J.H.; Mitchell, J.R.A. The Effect of Agents which Modify Platelet Behaviour and of Magnesium Ions on Thrombus Formation In Vivo. Thromb. Haemost. 1979, 42, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Rukshin, V.; Santos, R.; Gheorghiu, M.; Shah, P.K.; Kar, S.; Padmanabhan, S.; Azarbal, B.; Tsang, V.T.; Makkar, R.; Samuels, B.; et al. A Prospective, Nonrandomized, Open-Labeled Pilot Study Investigating the Use of Magnesium in Patients Undergoing Nonacute Percutaneous Coronary Intervention with Stent Implantation. J. Cardiovasc. Pharmacol. Ther. 2003, 8, 193–200. [Google Scholar] [CrossRef]
- Dickens, B.; Weglicki, W.; Li, Y.-S.; Mak, I. Magnesium deficiency in vitro enhances free radical-induced intracellular oxidation and cytotoxicity in endothelial cells. FEBS Lett. 1992, 311, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Banai, S.; Haggroth, L.; Epstein, S.E.; Casscells, W. Influence of extracellular magnesium on capillary endothelial cell proliferation and migration. Circ. Res. 1990, 67, 645–650. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Low sMg (n = 1147) | Normal/High sMg (n = 3405) | Overall (n = 4552) | p-Value 1 |
|---|---|---|---|---|
| Age | 72.0 (63.5, 81.0) | 67.0 (58.0, 79.0) | 69.0 (59.0, 79.0) | <0.001 |
| Male sex | 736 (64%) | 2439 (72%) | 3175 (70%) | <0.001 |
| Atrial fibrillation | 74 (6%) | 163 (5%) | 237 (5%) | 0.028 |
| Ischemic heart disease | 672 (59%) | 2177 (64%) | 2849 (63%) | 0.001 |
| Congestive heart failure | 46 (4%) | 100 (3%) | 146 (3%) | 0.074 |
| Hypertension | 1052 (92%) | 2911 (85%) | 3963 (87%) | <0.001 |
| Diabetes mellitus | 681 (59%) | 982 (29%) | 1663 (37%) | <0.001 |
| Stroke | 93 (8%) | 189 (6%) | 282 (6%) | 0.002 |
| Dementia | 23 (2%) | 84 (2%) | 107 (2%) | 0.4 |
| Peripheral artery disease | 85 (7%) | 165 (5%) | 250 (5%) | <0.001 |
| Smoking | 353 (31%) | 1119 (33%) | 1472 (32%) | 0.2 |
| LBBB | 43 (4%) | 114 (3%) | 157 (3%) | 0.5 |
| RBBB | 117 (10%) | 293 (9%) | 410 (9%) | 0.10 |
| Minimal hemoglobin—g/dL | 11.7 (10.3, 13.2) | 13.0 (11.4, 14.2) | 12.7 (11.1, 14.0) | <0.001 |
| Creatinine clearance—mL/min/1.73 m2 | 69.5 (53.1, 86.9) | 76.9 (57.9, 92.6) | 75.2 (56.5, 91.3) | <0.001 |
| Magnesium—mg/dL | 1.7 (1.6, 1.8) | 2.0 (2.0, 2.2) | 2.0 (1.9, 2.1) | <0.001 |
| Maximal glucose—md/dL | 192.0 (145.0, 271.5) | 146.2 (120.0, 196.0) | 155.0 (124.0, 215.0) | <0.001 |
| Troponin by quartile Q1–3 Q4 | 738 (67%) 360 (33%) | 2364 (72%) 903 (28%) | 3102 (71%) 1263 (29%) | 0.001 |
| LVEF—% | 55.0 (40.0, 60.0) | 55.0 (45.0, 60.0) | 55.0 (45.0, 60.0) | <0.001 |
| RV systolic dysfunction | 46 (5%) | 118 (4%) | 164 (5%) | 0.3 |
| Catheterization | 710 (62%) | 2380 (70%) | 3090 (68%) | <0.001 |
| PCI | 446 (39%) | 1561 (46%) | 2007 (44%) | <0.001 |
| Diseased coronary vessels 0 1 2 3 | 40 (7%) 137 (23%) 171 (28%) 246 (41%) | 203 (10%) 694 (32%) 526 (25%) 682 (32%) | 243 (9%) 831 (30%) 697 (25%) 928 (34%) | <0.001 |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Characteristic | Low sMg | Normal/High sMg | p-Value 1 | Low sMg | Normal/High sMg | p-Value 1 |
| (n = 736) | (n = 3405) | (n = 411) | (n = 966) | |||
| Age | 69.0 (61.0, 78.0) | 65.0 (56.0, 75.0) | <0.001 | 78.0 (70.0, 84.0) | 74.0 (64.0, 84.0) | <0.001 |
| Hypertension | 669 (91%) | 2058 (84%) | <0.001 | 383 (93%) | 853 (88%) | 0.006 |
| Diabetes mellitus | 450 (61%) | 703 (29%) | <0.001 | 231 (56%) | 279 (29%) | <0.001 |
| Stroke | 56 (8%) | 118 (5%) | 0.004 | 37 (9%) | 71 (7%) | 0.3 |
| Peripheral artery disease | 58 (8%) | 116 (5%) | 0.001 | 27 (7%) | 49 (5%) | 0.3 |
| Creatinine clearance—mL/min/1.73 m2 | 73.2 (56.3, 89.7) | 78.8 (60.8, 93.9) | <0.001 | 63.3 (47.7, 82.0) | 69.9 (51.7, 88.8) | <0.001 |
| Minimal hemoglobin—g/dL | 12.4 (10.8, 13.7) | 13.5 (12.1, 14.6) | <0.001 | 10.9 (9.7, 12.1) | 11.9 (10.6, 12.8) | <0.001 |
| Troponin by quartile | <0.001 | 0.4 | ||||
| Q1–3 | 451 (64%) | 1652 (71%) | 287 (74%) | 712 (76%) | ||
| Q4 | 259 (36%) | 681 (29%) | 101 (26%) | 222 (24%) | ||
| LVEF—% | 50.0 (40.0, 60.0) | 55.0 (45.0, 60.0) | <0.001 | 55.0 (40.0, 60.0) | 60.0 (45.0, 60.0) | 0.008 |
| RV systolic dysfunction | 31 (5%) | 87 (4%) | 0.3 | 15 (5%) | 31 (4%) | 0.6 |
| Catheterization | 504 (68%) | 1827 (75%) | <0.001 | 206 (50%) | 553 (57%) | 0.015 |
| PCI | 326 (44%) | 1261 (52%) | <0.001 | 120 (29%) | 300 (31%) | 0.5 |
| Diseased coronary vessels | <0.001 | 0.001 | ||||
| 0 | 19 (4%) | 91 (5%) | 21 (13%) | 112 (24%) | ||
| 1 | 99 (22%) | 546 (33%) | 38 (24%) | 148 (31%) | ||
| 2 | 125 (28%) | 418 (25%) | 46 (29%) | 108 (23%) | ||
| 3 | 191 (43%) | 580 (35%) | 55 (34%) | 102 (22%) | ||
| Characteristic | HR | 95% CI | p-Value |
|---|---|---|---|
| Low serum magnesium levels | 1.24 | 1.11, 1.39 | <0.001 |
| Age | 1.07 | 1.06, 1.07 | <0.001 |
| Male sex | 1.11 | 0.99, 1.24 | 0.079 |
| Atrial fibrillation | 1.01 | 0.84, 1.21 | >0.9 |
| Congestive heart failure | 1.17 | 0.94, 1.44 | 0.2 |
| Hypertension | 1.18 | 0.97, 1.43 | 0.095 |
| Ischemic heart disease | 0.99 | 0.88, 1.11 | 0.8 |
| Diabetes mellitus | 1.25 | 1.12, 1.40 | <0.001 |
| Stroke | 1.49 | 1.27, 1.76 | <0.001 |
| Smoking | 1.37 | 1.20, 1.55 | <0.001 |
| Coronary angiography | 0.45 | 0.39, 0.52 | <0.001 |
| Percutaneous coronary intervention | 0.72 | 0.61, 0.85 | <0.001 |
| Creatinine clearance | 0.99 | 0.98, 0.99 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Segev, A.; Shechter, M.; Tsur, A.M.; Belkin, D.; Cohen, H.; Sharon, A.; Morag, N.K.; Grossman, E.; Maor, E. Serum Magnesium Is Associated with Long-Term Survival of Non-ST-Elevation Myocardial Infarction Patients. Nutrients 2023, 15, 4299. https://doi.org/10.3390/nu15194299
Segev A, Shechter M, Tsur AM, Belkin D, Cohen H, Sharon A, Morag NK, Grossman E, Maor E. Serum Magnesium Is Associated with Long-Term Survival of Non-ST-Elevation Myocardial Infarction Patients. Nutrients. 2023; 15(19):4299. https://doi.org/10.3390/nu15194299
Chicago/Turabian StyleSegev, Amitai, Michael Shechter, Avishai M. Tsur, David Belkin, Hofit Cohen, Amir Sharon, Nira Koren Morag, Ehud Grossman, and Elad Maor. 2023. "Serum Magnesium Is Associated with Long-Term Survival of Non-ST-Elevation Myocardial Infarction Patients" Nutrients 15, no. 19: 4299. https://doi.org/10.3390/nu15194299
APA StyleSegev, A., Shechter, M., Tsur, A. M., Belkin, D., Cohen, H., Sharon, A., Morag, N. K., Grossman, E., & Maor, E. (2023). Serum Magnesium Is Associated with Long-Term Survival of Non-ST-Elevation Myocardial Infarction Patients. Nutrients, 15(19), 4299. https://doi.org/10.3390/nu15194299