
Unraveling the Connection: Visceral Adipose Tissue and Vitamin D Levels in Obesity

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Methods
Patients
3. Statistical Analysis
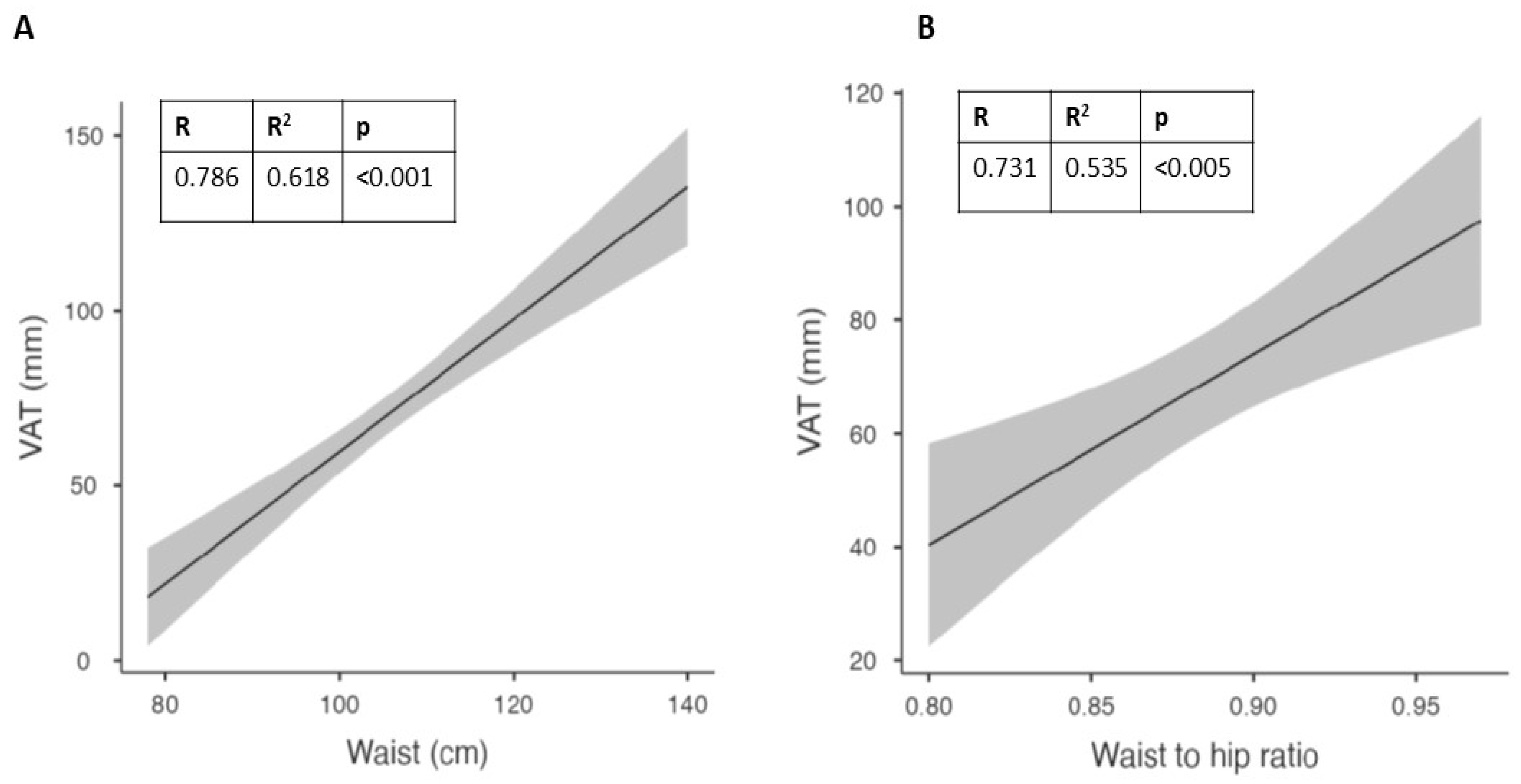
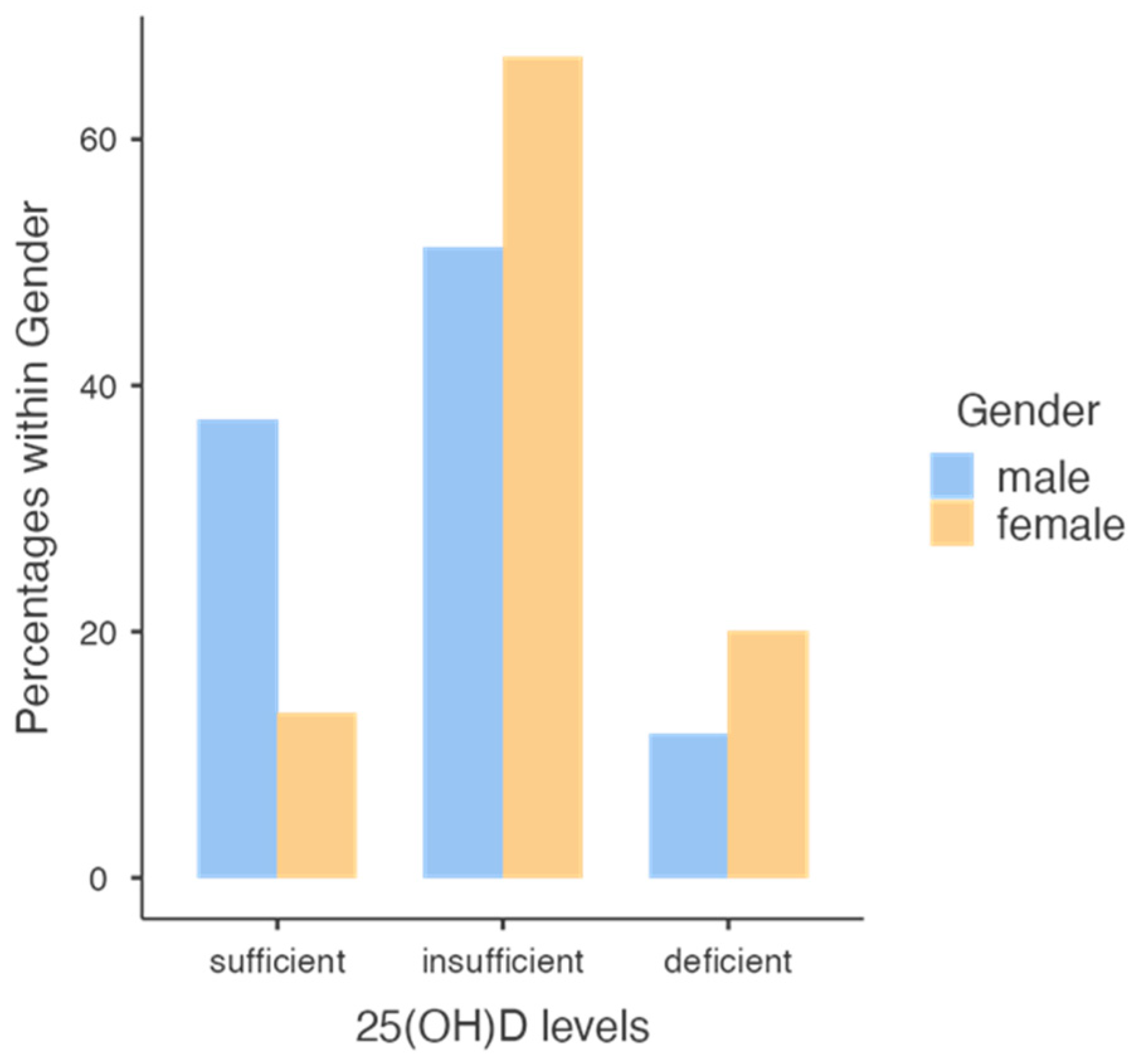
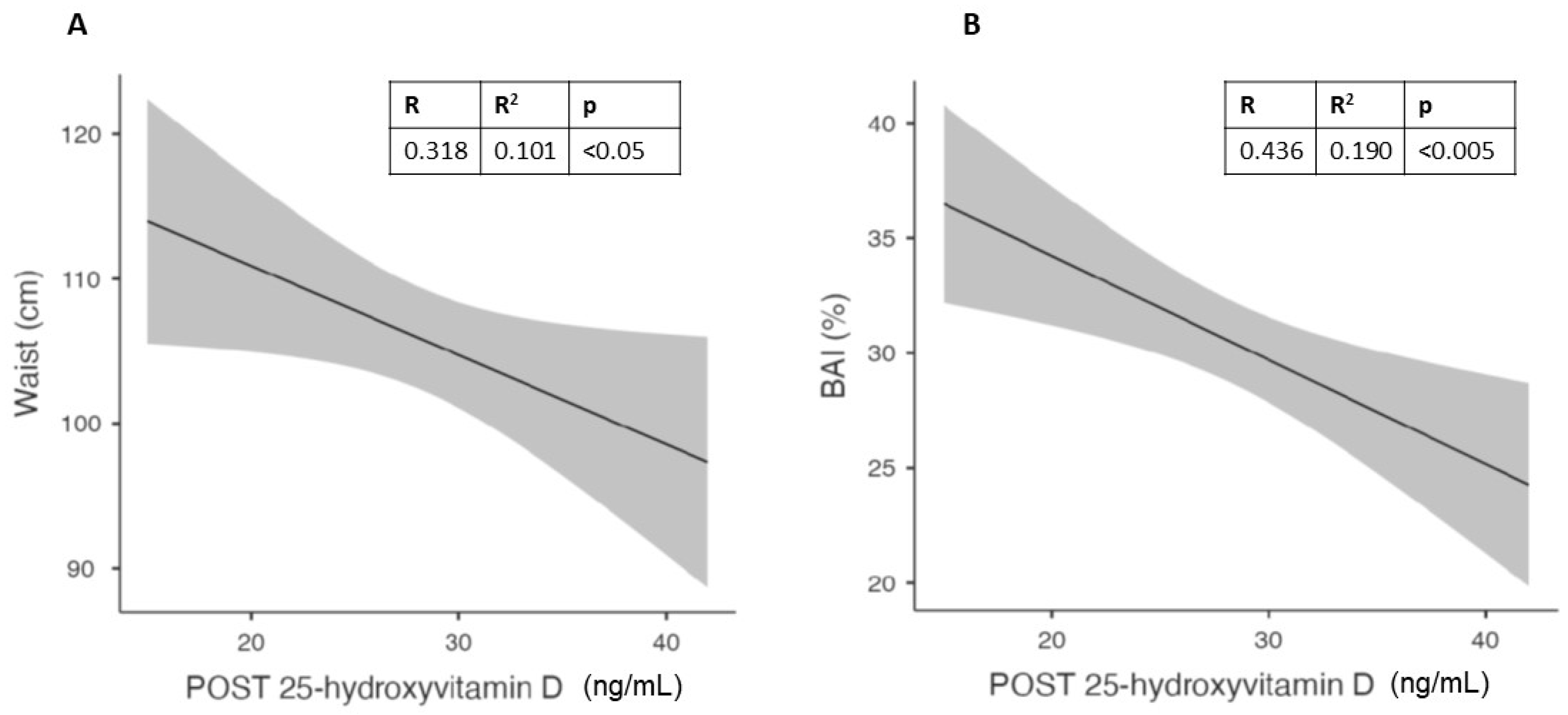
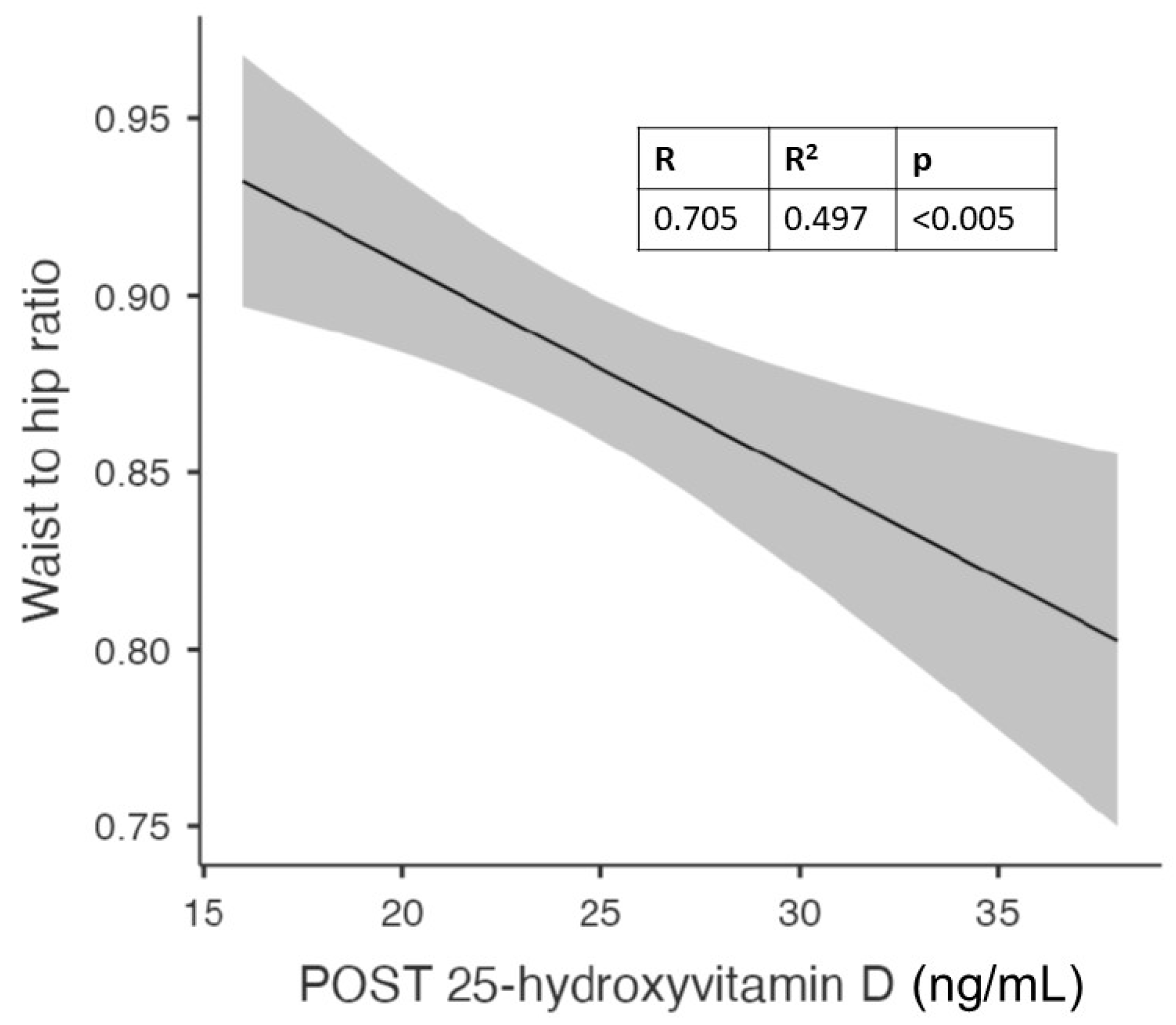
4. Results
Population of the Study
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bouillon, R.; Norman, A.W.; Lips, P. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 1980–1981. [Google Scholar] [PubMed]
- Earthman, C.; Beckman, L.; Masodkar, K.; Sibley, S. The link between obesity and low circulating 25-hydroxyvitamin D concentrations: Considerations and implications. Int. J. Obes. 2012, 36, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Brock, K.; Huang, W.-Y.; Fraser, D.; Ke, L.; Tseng, M.; Stolzenberg-Solomon, R.; Peters, U.; Ahn, J.; Purdue, M.; Mason, R. Low vitamin D status is associated with physical inactivity, obesity and low vitamin D intake in a large US sample of healthy middle-aged men and women. J. Steroid Biochem. Mol. Biol. 2010, 121, 462–466. [Google Scholar] [CrossRef] [PubMed]
- da Silva, E.M.S.; Pinho, H.S.; Rodrigues, I.G.; Pinho, C.P.S. Asociación entre los niveles séricos de vitamina D y las alteraciones cardiometabólicas. Nutr. Clínica Dietética Hosp. 2019, 39, 86–93. [Google Scholar]
- Zaki, M.; Kamal, S.; Basha, W.A.; Youness, E.; Ezzat, W.; El-Bassyouni, H.; Amr, K. Association of vitamin D receptor gene polymorphism (VDR) with vitamin D deficiency, metabolic and inflammatory markers in Egyptian obese women. Genes Dis. 2017, 4, 176–182. [Google Scholar] [CrossRef]
- Farrell, S.W.; Willis, B.L. Cardiorespiratory fitness, adiposity, and serum 25-dihydroxyvitamin D levels in women: The Cooper Center Longitudinal Study. J. Women’s Health 2012, 21, 80–86. [Google Scholar] [CrossRef]
- da Silva, S.; Maria, E.; Pinho; Sabino, H.; Rodrigues; Galvão1, I.; Pinho; Sabino, C.P. Association between serum vitamin D levels and cardiometabolic alterations. Nutr. Clín. Diet. Hosp. 2019, 39, 86–93. [Google Scholar]
- Hajhashemy, Z.; Foshati, S.; Saneei, P. Relationship between abdominal obesity (based on waist circumference) and serum vitamin D levels: A systematic review and meta-analysis of epidemiologic studies. Nutr. Rev. 2022, 80, 1105–1117. [Google Scholar] [CrossRef]
- Ritchie, S.; Connell, J. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Aggoun, Y. Obesity, metabolic syndrome, and cardiovascular disease. Pediatr. Res. 2007, 61, 653–659. [Google Scholar] [CrossRef]
- Zhong, P.; Tan, S.; Zhu, Z.; Zhu, Z.; Liang, Y.; Huang, W.; Wang, W. Normal-weight central obesity and risk of cardiovascular and microvascular events in adults with prediabetes or diabetes: Chinese and British cohorts. Diabetes/Metab. Res. Rev. 2023, e3707. [Google Scholar] [CrossRef] [PubMed]
- Hulsmans, M.; Van Dooren, E.; Mathieu, C.; Holvoet, P. Decrease of miR-146b-5p in monocytes during obesity is associated with loss of the anti-inflammatory but not insulin signaling action of adiponectin. PLoS ONE 2012, 7, e32794. [Google Scholar] [CrossRef] [PubMed]
- Kouli, G.-M.; Panagiotakos, D.B.; Kyrou, I.; Georgousopoulou, E.N.; Chrysohoou, C.; Tsigos, C.; Tousoulis, D.; Pitsavos, C. Visceral adiposity index and 10-year cardiovascular disease incidence: The ATTICA study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Piacentini, G.; Pietrobelli, A. Vitamin D daily versus monthly administration: Bone turnover and adipose tissue influences. Nutrients 2018, 10, 1934. [Google Scholar] [CrossRef]
- Pecoraro, L.; Nisi, F.; Serafin, A.; Antoniazzi, F.; Dalle Carbonare, L.; Piacentini, G.; Pietrobelli, A. Vitamin d supplementation in the assessment of cardiovascular risk factors in overweight and obese children. Med. Sci. 2022, 10, 49. [Google Scholar] [CrossRef]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A. Vitamin D insufficiency in overweight and obese children and adolescents. Front. Endocrinol. 2019, 10, 103. [Google Scholar] [CrossRef]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A. Guidelines for preventing and treating vitamin D deficiency: A 2023 update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef]
- Bilezikian, J.P.; Formenti, A.M.; Adler, R.A.; Binkley, N.; Bouillon, R.; Lazaretti-Castro, M.; Marcocci, C.; Napoli, N.; Rizzoli, R.; Giustina, A. Vitamin D: Dosing, levels, form, and route of administration: Does one approach fit all? Rev. Endocr. Metab. Disord. 2021, 22, 1201–1218. [Google Scholar] [CrossRef]
- Pludowski, P. Supplementing Vitamin D in Different Patient Groups to Reduce Deficiency. Nutrients 2023, 15, 3725. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Miazek, K.; Selmi, A.; Balcerczyk, A.; Śliwińska, A. The action of vitamin D in adipose tissue: Is there the link between vitamin D deficiency and adipose tissue-related metabolic disorders? Int. J. Mol. Sci. 2022, 23, 956. [Google Scholar] [CrossRef]
- Ding, C.; Gao, D.; Wilding, J.; Trayhurn, P.; Bing, C. Vitamin D signalling in adipose tissue. Br. J. Nutr. 2012, 108, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Carrelli, A.; Bucovsky, M.; Horst, R.; Cremers, S.; Zhang, C.; Bessler, M.; Schrope, B.; Evanko, J.; Blanco, J.; Silverberg, S.J. Vitamin D storage in adipose tissue of obese and normal weight women. J. Bone Miner. Res. 2017, 32, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Drincic, A.T.; Armas, L.A.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity 2012, 20, 1444–1448. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.; Stokholm, K.; Lund, B.; Sørensen, O. Vitamin D deficiency in obese patients and changes in circulating vitamin D metabolites following jejunoileal bypass. Int. J. Obes. 1982, 6, 473–479. [Google Scholar] [PubMed]
- Bell, N.H.; Greene, A.; Epstein, S.; Oexmann, M.J.; Shaw, S.; Shary, J. Evidence for alteration of the vitamin D-endocrine system in blacks. J. Clin. Investig. 1985, 76, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Konradsen, S.; Ag, H.; Lindberg, F.; Hexeberg, S.; Jorde, R. Serum 1, 25-dihydroxy vitamin D is inversely associated with body mass index. Eur. J. Nutr. 2008, 47, 87–91. [Google Scholar] [CrossRef]
- Moan, J.; Lagunova, Z.; Lindberg, F.A.; Porojnicu, A.C. Seasonal variation of 1, 25-dihydroxyvitamin D and its association with body mass index and age. J. Steroid Biochem. Mol. Biol. 2009, 113, 217–221. [Google Scholar] [CrossRef]
- Lagunova, Z.; Porojnicu, A.C.; Vieth, R.; Lindberg, F.A.; Hexeberg, S.; Moan, J. Serum 25-hydroxyvitamin D is a predictor of serum 1, 25-dihydroxyvitamin D in overweight and obese patients. J. Nutr. 2011, 141, 112–117. [Google Scholar] [CrossRef]
- Vlachos, I.S.; Hatziioannou, A.; Perelas, A.; Perrea, D.N. Sonographic assessment of regional adiposity. Am. J. Roentgenol. 2007, 189, 1545–1553. [Google Scholar] [CrossRef]
- Pimanov, S.; Bondarenko, V.; Makarenko, E. Visceral fat in different locations assessed by ultrasound: Correlation with computed tomography and cut-off values in patients with metabolic syndrome. Clin. Obes. 2020, 10, e12404. [Google Scholar] [CrossRef] [PubMed]
- Kotsis, V.; Tsioufis, K.; Antza, C.; Seravalle, G.; Coca, A.; Sierra, C.; Lurbe, E.; Stabouli, S.; Jelakovic, B.; Redon, J. Obesity and cardiovascular risk: A call for action from the European Society of Hypertension Working Group of Obesity, Diabetes and the High-risk Patient and European Association for the Study of Obesity: Part B: Obesity-induced cardiovascular disease, early prevention strategies and future research directions. J. Hypertens. 2018, 36, 1441–1455. [Google Scholar] [PubMed]
- Oda, E. New criteria forobesity disease’in Japan. Circ. J. 2006, 70, 150. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Fang, H.; Berg, E.; Cheng, X.; Shen, W. How to best assess abdominal obesity. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 360. [Google Scholar] [CrossRef] [PubMed]
- Boone, S.C.; Van Smeden, M.; Rosendaal, F.R.; Le Cessie, S.; Groenwold, R.H.; Jukema, J.W.; Van Dijk, K.W.; Lamb, H.J.; Greenland, P.; Neeland, I.J. Evaluation of the value of waist circumference and metabolomics in the estimation of visceral adipose tissue. Am. J. Epidemiol. 2022, 191, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Smith, U. Abdominal obesity: A marker of ectopic fat accumulation. J. Clin. Investig. 2015, 125, 1790–1792. [Google Scholar] [CrossRef] [PubMed]
- Park, C.Y.; Han, S.N. The role of vitamin D in adipose tissue biology: Adipocyte differentiation, energy metabolism, and inflammation. J. Lipid Atheroscler. 2021, 10, 130. [Google Scholar] [CrossRef]
- Yuzbashian, E.; Asghari, G.; Hedayati, M.; Zarkesh, M.; Mirmiran, P.; Khalaj, A. Determinants of vitamin D receptor gene expression in visceral and subcutaneous adipose tissue in non-obese, obese, and morbidly obese subjects. J. Steroid Biochem. Mol. Biol. 2019, 187, 82–87. [Google Scholar] [CrossRef]
- Rosenstreich, S.J.; Rich, C.; Volwiler, W. Deposition in and release of vitamin D 3 from body fat: Evidence for a storage site in the rat. J. Clin. Investig. 1971, 50, 679–687. [Google Scholar] [CrossRef]
- Mawer, E.B.; Backhouse, J.; Holman, C.A.; Lumb, G.; Stanbury, S. The distribution and storage of vitamin D and its metabolites in human tissues. Clin. Sci. 1972, 43, 413–431. [Google Scholar] [CrossRef]
- Gangloff, A.; Bergeron, J.; Lemieux, I.; Després, J.-P. Changes in circulating vitamin D levels with loss of adipose tissue. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Didriksen, A.; Burild, A.; Jakobsen, J.; Fuskevåg, O.M.; Jorde, R. Vitamin D3 increases in abdominal subcutaneous fat tissue after supplementation with vitamin D3. Eur. J. Endocrinol. 2015, 172, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Martinaityte, I.; Kamycheva, E.; Didriksen, A.; Jakobsen, J.; Jorde, R. Vitamin D stored in fat tissue during a 5-year intervention affects serum 25-hydroxyvitamin D levels the following year. J. Clin. Endocrinol. Metab. 2017, 102, 3731–3738. [Google Scholar] [CrossRef] [PubMed]
- Pourshahidi, L.K. Vitamin D and obesity: Current perspectives and future directions. Proc. Nutr. Soc. 2015, 74, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Hengist, A.; Perkin, O.; Gonzalez, J.; Betts, J.; Hewison, M.; Manolopoulos, K.; Jones, K.; Koulman, A.; Thompson, D. Mobilising vitamin D from adipose tissue: The potential impact of exercise. Nutr. Bull. 2019, 44, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Karpe, F.; Lafontan, M.; Frayn, K. Physical activity and exercise in the regulation of human adipose tissue physiology. Physiol. Rev. 2012, 92, 157–191. [Google Scholar] [CrossRef] [PubMed]
- Gangloff, A.; Bergeron, J.; Pelletier-Beaumont, E.; Nazare, J.; Smith, J.; Borel, A.; Lemieux, I.; Tremblay, A.; Poirier, P.; Alméras, N. Effect of adipose tissue volume loss on circulating 25-hydroxyvitamin D levels: Results from a 1-year lifestyle intervention in viscerally obese men. Int. J. Obes. 2015, 39, 1638–1643. [Google Scholar] [CrossRef]
- Reinehr, T.; de Sousa, G.; Alexy, U.; Kersting, M.; Andler, W. Vitamin D status and parathyroid hormone in obese children before and after weight loss. Eur. J. Endocrinol. 2007, 157, 225–232. [Google Scholar] [CrossRef]
- Chin, K.; Zhao, D.; Tibuakuu, M.; Martin, S.S.; Ndumele, C.E.; Florido, R.; Windham, B.G.; Guallar, E.; Lutsey, P.L.; Michos, E.D. Physical activity, vitamin D, and incident atherosclerotic cardiovascular disease in whites and blacks: The ARIC study. J. Clin. Endocrinol. Metab. 2017, 102, 1227–1236. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Analyses | Mean | Median | SD |
|---|---|---|---|
| Age (years) | 72.6 | 74.5 | 11.22 |
| Weight (Kg) | 85.28 | 85 | 16.74 |
| BMI (Kg/m2) | 29.13 | 28.04 | 5.22 |
| Waist circumference (cm) | 104.37 | 102.5 | 12.81 |
| Hip (cm) | 111.46 | 110 | 12.48 |
| BAI (%) | 32.07 | 31.04 | 6.76 |
| Waist-to-hip ratio | 936 | 951 | 0.04 |
| Waist-to-height ratio | 611 | 606 | 0.07 |
| SAT mean (mm) | 18.2 | 15.3 | 8.15 |
| VAT (mm) | 70.06 | 66.9 | 26.86 |
| PPAT (mm) | 14.17 | 12 | 6.86 |
| PRAT (mm) | 9.52 | 8 | 7.04 |
| 25-hydroxyvitamin D (ng/mL) | 17.59 | 18 | 5.59 |
| Calcium (mg/dL) | 9.33 | 9.35 | 0.44 |
| Group | N | Mean | SD | p | |
|---|---|---|---|---|---|
| Age (years) | males | 43 | 72.83 | 11.56 | 0.791 |
| females | 15 | 71.93 | 10.55 | ||
| Weight (Kg) | males | 43 | 88.34 | 15.98 | 0.017 |
| females | 15 | 76.53 | 16.27 | ||
| Height (m) | males | 43 | 1.74 | 0.06 | <0.001 |
| females | 15 | 1.63 | 0.07 | ||
| BMI (Kg/m2) | males | 43 | 29.26 | 5.44 | 0.74 |
| females | 15 | 28.74 | 4.7 | ||
| Waist circumference (cm) | males | 43 | 105.77 | 11.88 | 0.158 |
| females | 15 | 100.33 | 14.87 | ||
| Hip circumference (cm) | males | 43 | 110.83 | 12.3 | 0.521 |
| females | 15 | 113.26 | 13.26 | ||
| BAI (%) | males | 43 | 30.47 | 6.36 | 0.002 |
| females | 15 | 36.65 | 5.83 | ||
| Waist-to-hip ratio | males | 43 | 955 | 0.03 | < 0.001 |
| females | 15 | 883 | 0.04 | ||
| Vitamin D (ng/mL) | males | 43 | 17.9 | 5.9 | 0.46 |
| females | 15 | 16.7 | 4.8 | ||
| SAT mean (mm) | males | 43 | 16.1 | 7.53 | <0.001 |
| females | 15 | 24.1 | 7.01 | ||
| VAT (mm) | males | 43 | 70.63 | 28.53 | 0.787 |
| females | 15 | 68.43 | 22.16 | ||
| PPAT (mm) | males | 43 | 14.17 | 7.12 | 0.999 |
| females | 15 | 14.17 | 6.3 | ||
| PRAT (mm) | males | 42 | 9.03 | 7.14 | 0.384 |
| females | 15 | 10.89 | 6.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cominacini, M.; Fumaneri, A.; Ballerini, L.; Braggio, M.; Valenti, M.T.; Dalle Carbonare, L. Unraveling the Connection: Visceral Adipose Tissue and Vitamin D Levels in Obesity. Nutrients 2023, 15, 4259. https://doi.org/10.3390/nu15194259
Cominacini M, Fumaneri A, Ballerini L, Braggio M, Valenti MT, Dalle Carbonare L. Unraveling the Connection: Visceral Adipose Tissue and Vitamin D Levels in Obesity. Nutrients. 2023; 15(19):4259. https://doi.org/10.3390/nu15194259
Chicago/Turabian StyleCominacini, Mattia, Alessia Fumaneri, Linda Ballerini, Michele Braggio, Maria Teresa Valenti, and Luca Dalle Carbonare. 2023. "Unraveling the Connection: Visceral Adipose Tissue and Vitamin D Levels in Obesity" Nutrients 15, no. 19: 4259. https://doi.org/10.3390/nu15194259
APA StyleCominacini, M., Fumaneri, A., Ballerini, L., Braggio, M., Valenti, M. T., & Dalle Carbonare, L. (2023). Unraveling the Connection: Visceral Adipose Tissue and Vitamin D Levels in Obesity. Nutrients, 15(19), 4259. https://doi.org/10.3390/nu15194259