
Myoinositols Prevent Gestational Diabetes Mellitus and Related Complications: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
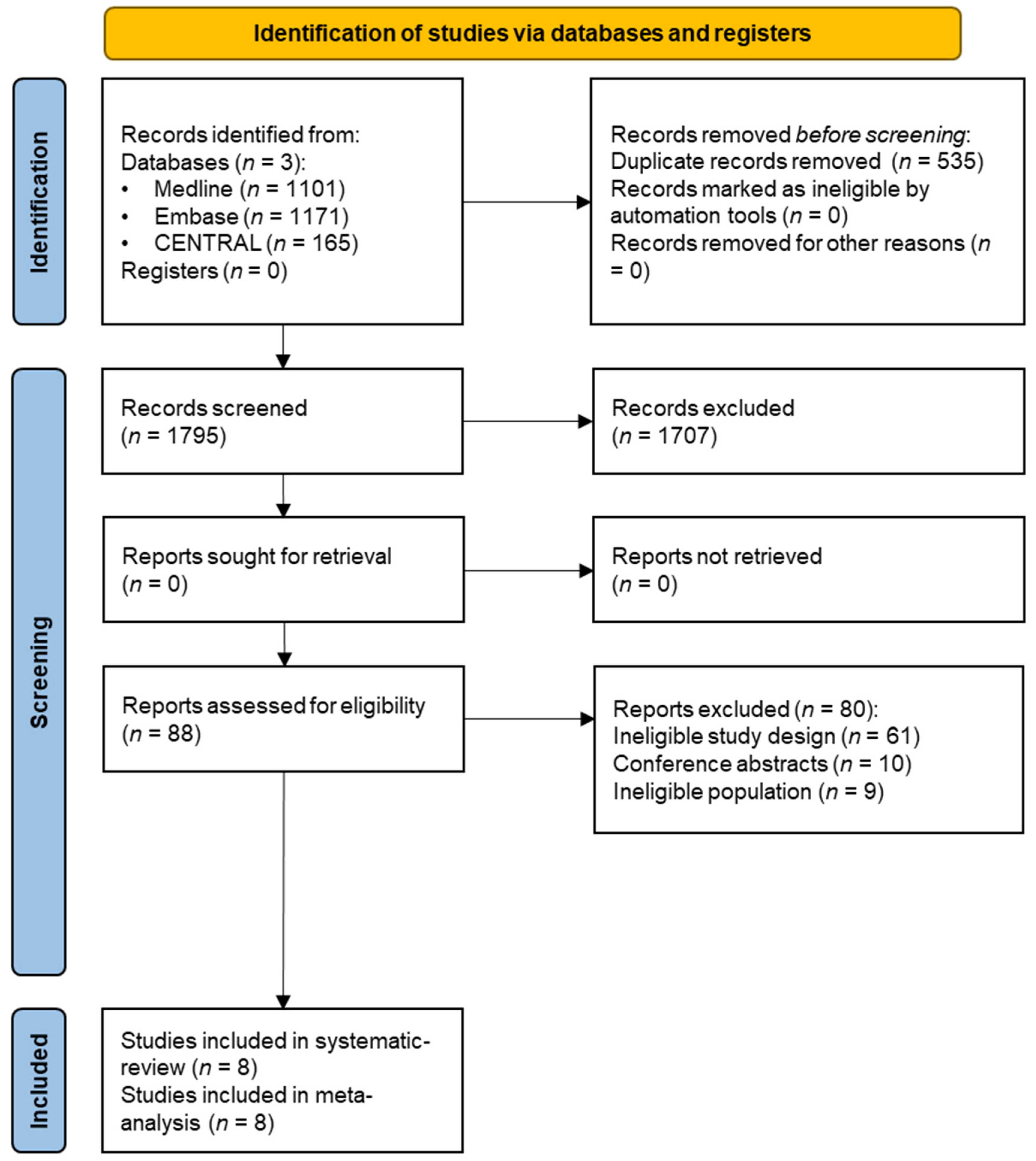
2.3. Selection Process
2.4. Data Collection Process and Data Items
2.5. Study Risk of Bias Assessment
2.6. Assessing the Level of Evidence
2.7. Synthesis Methods
3. Results
3.1. General Characteristics of the Studies
3.2. Synthesis of the Results
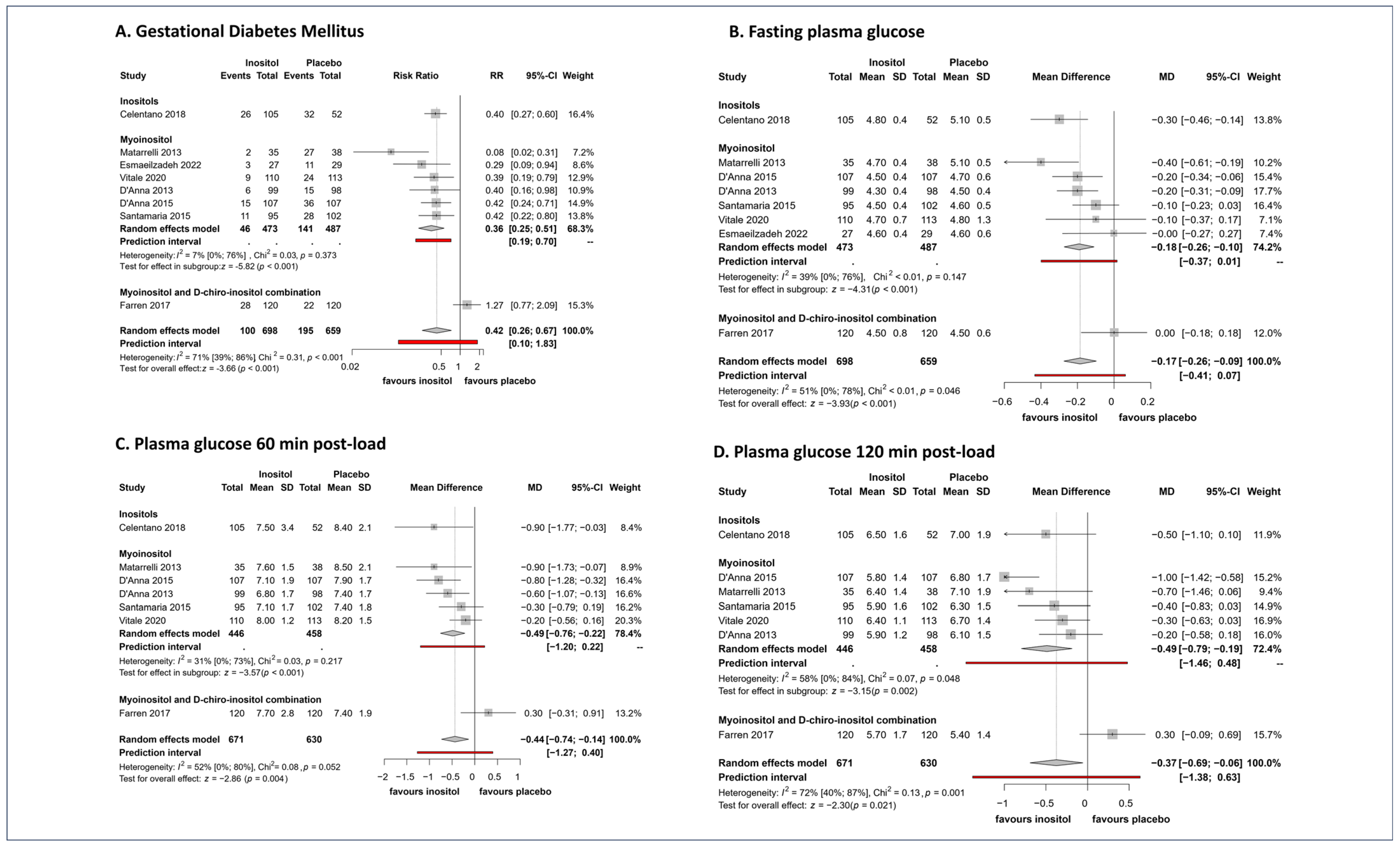
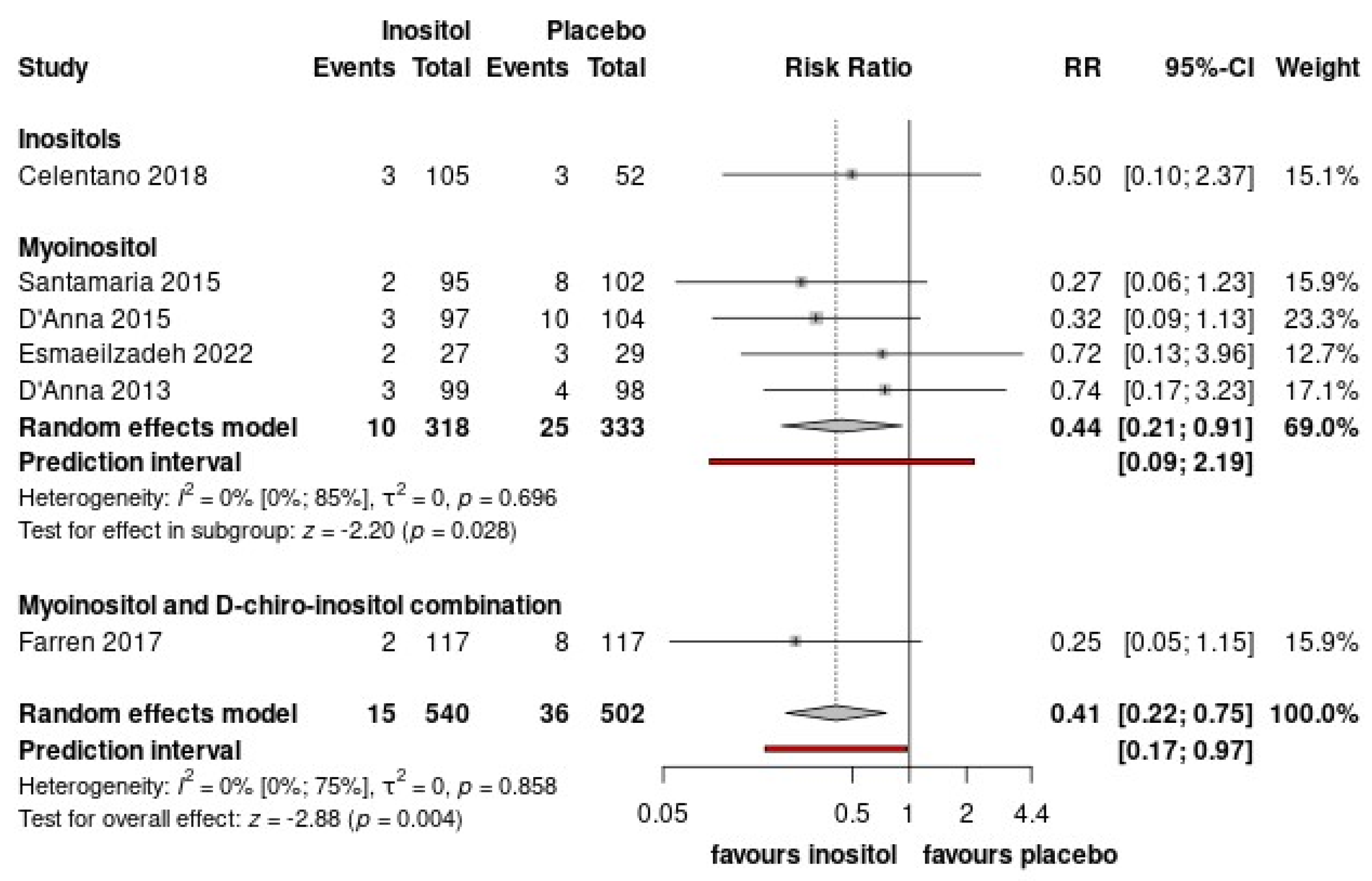
3.2.1. Inositols Decrease the Occurrence of GDM
3.2.2. Inositol Reduces Fasting, 60′, and 120′ Glucose Levels during OGTT
3.3. Delivery Outcomes
3.4. Fetal-Neonatal Health Outcomes
4. Discussion
Inositol supplementation administered from the first trimester can prevent the development of GDM by decreasing fasting, 1-h, and 2-h OGTT glucose levels.
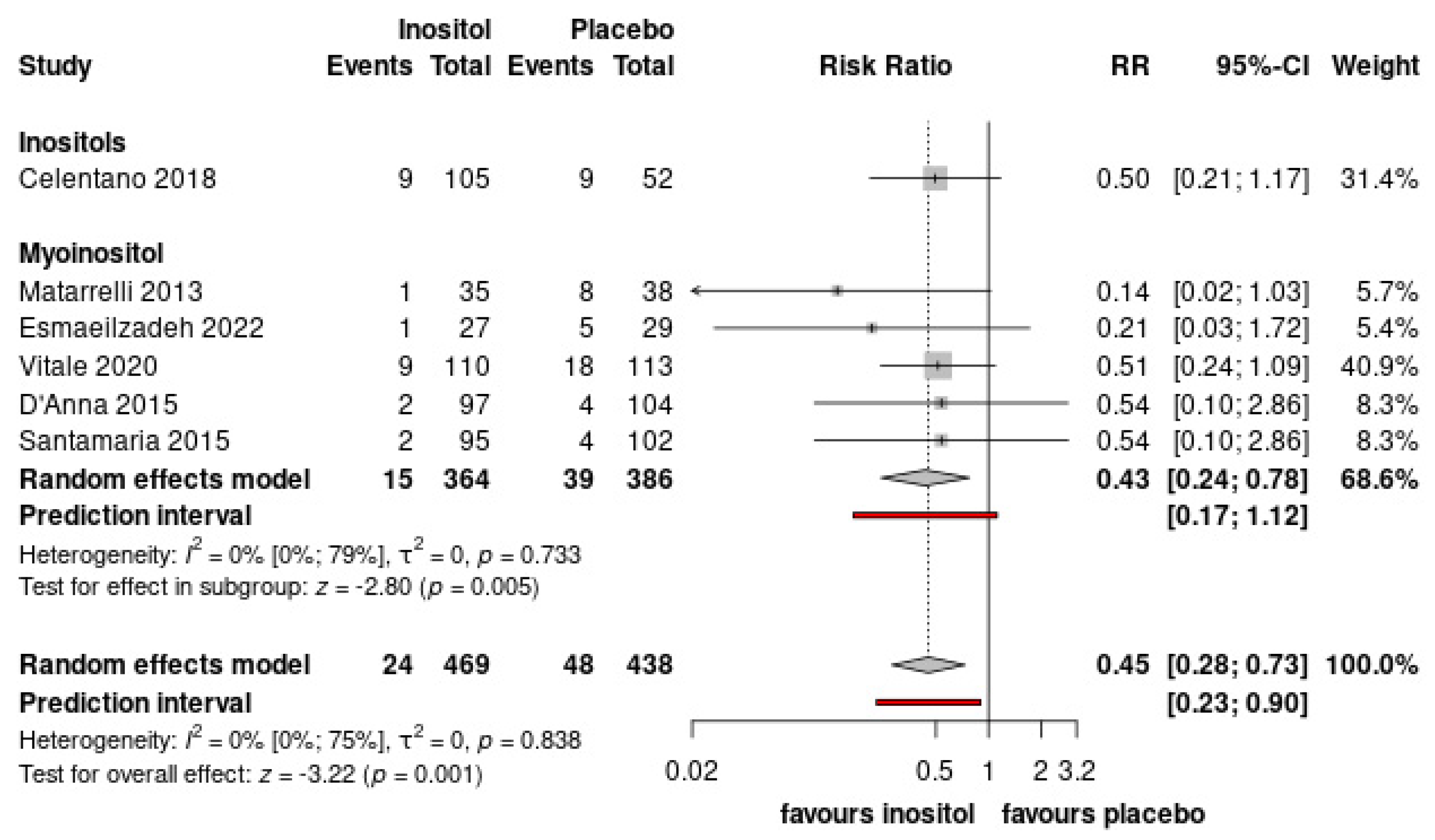
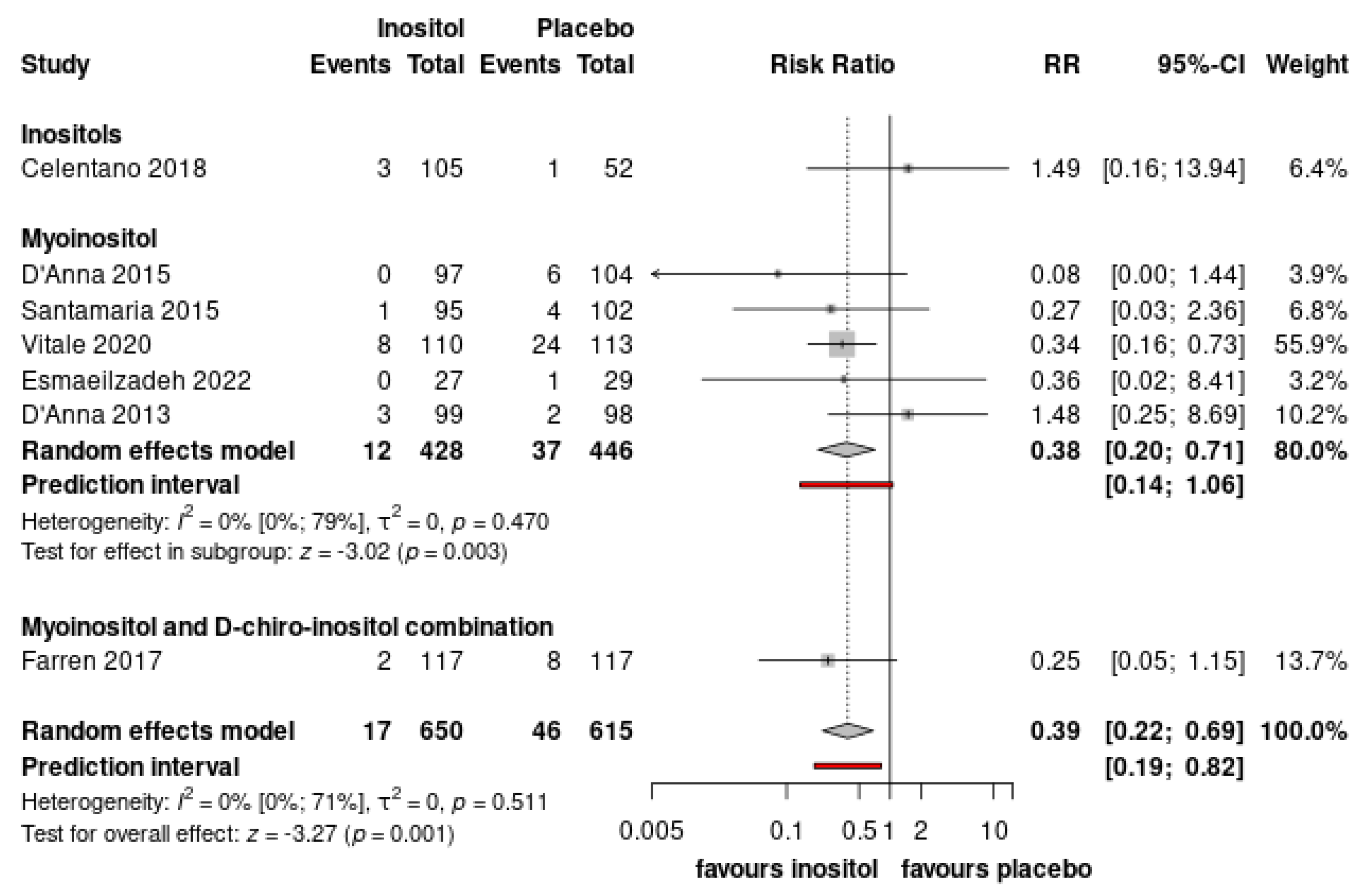
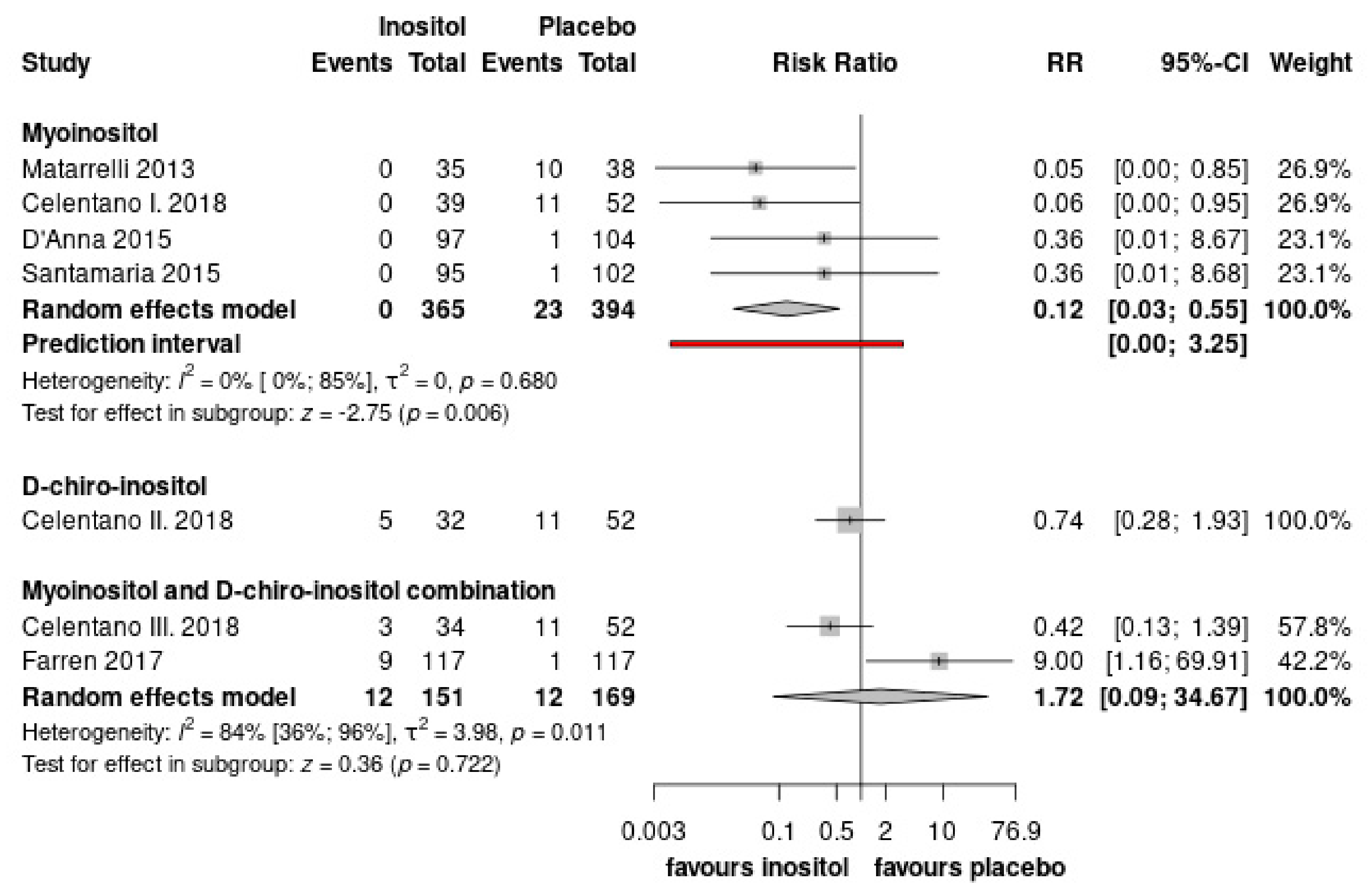
Inositol reduce the need for insulin treatment and the risk of pregnancy-induced hypertensive disorders (preeclampsia or gestational hypertension)
Inositol supplementation lowers the risk of preterm birth and neonatal hypoglycemia.
4.1. Strengths and Limitations
4.2. Implication for Practice and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GDM | gestational diabetes mellitus |
| RCT | randomized controlled trial |
| OGTT | were oral glucose tolerance test |
| RR | risk ratio |
| MD | mean difference |
| CI | confidence interval |
| T2DM | type-2 diabetes mellitus |
| MI | myoinositol |
| DCI | D-chiro-inositol |
| GLUT4 | glucose transporter type 4 |
| PICO | population: intervention, comparator, outcome |
| LGA | large for gestational age |
| IUGR | intrauterine growth restriction |
| SD | standard deviation |
| RoB2 | Risk-of-bias tool for randomized trials |
| GRADE | Grades of Recommendation, Assessment, Development, and Evaluation |
| REML | Restricted maximum likelihood |
| IADPSG | International Association of Diabetes and Pregnancy Study Groups |
| 1 h-OGTT | one-hour glucose tolerance test |
| 2 h-OGTT | two-hour glucose tolerance test |
| NICU | neonatal intensive care unit |
References
- American Diabetes Association. Gestational Diabetes Mellitus. Diabetes Care 2003, 26 (Suppl. 1), s103–s105. [Google Scholar] [CrossRef]
- Hjort, L.; Novakovic, B.; Grunnet, L.G.; Maple-Brown, L.; Damm, P.; Desoye, G.; Saffery, R. Diabetes in pregnancy and epigenetic mechanisms-how the first 9 months from conception might affect the child’s epigenome and later risk of disease. Lancet Diabetes Endocrinol. 2019, 7, 796–806. [Google Scholar] [CrossRef] [PubMed]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. 3), s173–s211. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Reynolds, C.M.; Vickers, M.H.; Baker, P.N.; Stanley, J.L. Nutritional Supplementation for the Prevention and/or Treatment of Gestational Diabetes Mellitus. Curr. Diabetes Rep. 2019, 19, 73. [Google Scholar] [CrossRef]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, P.; Saccone, G.; Pellegrino, R.; Vaccarisi, S.; Taranto, L.; Mazzulla, R.; Bernardo, S.; Venturella, R.; Di Carlo, C.; Morelli, M. Incidental diagnosis of a pancreatic adenocarcinoma in a woman affected by gestational diabetes mellitus: Case report and literature review. Am. J. Obstet. Gynecol. MFM 2021, 3, 100471. [Google Scholar] [CrossRef]
- Kamińska, K.; Stenclik, D.; Błażejewska, W.; Bogdański, P.; Moszak, M. Probiotics in the Prevention and Treatment of Gestational Diabetes Mellitus (GDM): A Review. Nutrients 2022, 14, 4303. [Google Scholar] [CrossRef]
- Zhang, D.Y.; Cheng, D.C.; Cao, Y.N.; Su, Y.; Chen, L.; Liu, W.Y.; Yu, Y.X.; Xu, X.M. The effect of dietary fiber supplement on prevention of gestational diabetes mellitus in women with pre-pregnancy overweight/obesity: A randomized controlled trial. Front. Pharmacol. 2022, 13, 922015. [Google Scholar] [CrossRef]
- Hashemi Tari, S.; Sohouli, M.H.; Lari, A.; Fatahi, S.; Rahideh, S.T. The effect of inositol supplementation on blood pressure: A systematic review and meta-analysis of randomized-controlled trials. Clin. Nutr. ESPEN 2021, 44, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Milewska, E.M.; Czyzyk, A.; Meczekalski, B.; Genazzani, A.D. Inositol and human reproduction. From cellular metabolism to clinical use. Gynecol. Endocrinol. 2016, 32, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Donnelly, R. Sex Hormone-Binding Globulin (SHBG) as an Early Biomarker and Therapeutic Target in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2020, 21, 8191. [Google Scholar] [CrossRef]
- Greff, D.; Juhász, A.E.; Váncsa, S.; Váradi, A.; Sipos, Z.; Szinte, J.; Park, S.; Hegyi, P.; Nyirády, P.; Ács, N.; et al. Inositol is an effective and safe treatment in polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Reprod. Biol. Endocrinol. 2023, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S. Inositol transport proteins. FEBS Lett. 2015, 589, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Yan, J.; Yang, H. Inositol Nutritional Supplementation for the Prevention of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 2831. [Google Scholar] [CrossRef]
- Caputo, M.; Bona, E.; Leone, I.; Samà, M.T.; Nuzzo, A.; Ferrero, A.; Aimaretti, G.; Marzullo, P.; Prodam, F. Inositols and metabolic disorders: From farm to bedside. J. Tradit. Complement. Med. 2020, 10, 252–259. [Google Scholar] [CrossRef]
- Genazzani, A.D.; Santagni, S.; Rattighieri, E.; Chierchia, E.; Despini, G.; Marini, G.; Prati, A.; Simoncini, T. Modulatory role of D-chiro-inositol (DCI) on LH and insulin secretion in obese PCOS patients. Gynecol. Endocrinol. 2014, 30, 438–443. [Google Scholar] [CrossRef]
- Dinicola, S.; Unfer, V.; Facchinetti, F.; Soulage, C.O.; Greene, N.D.; Bizzarri, M.; Laganà, A.S.; Chan, S.Y.; Bevilacqua, A.; Pkhaladze, L.; et al. Inositols: From Established Knowledge to Novel Approaches. Int. J. Mol. Sci. 2021, 22, 10575. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Iorio, A.; Spencer, F.A.; Falavigna, M.; Alba, C.; Lang, E.; Burnand, B.; McGinn, T.; Hayden, J.; Williams, K.; Shea, B.; et al. Use of GRADE for assessment of evidence about prognosis: Rating confidence in estimates of event rates in broad categories of patients. BMJ 2015, 350, h870. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. dmetar: Companion R Package For The Guide ‘Doing Meta-Analysis in R’, R Package Version 0.0.9000. 2019. [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical Aspects of the Analysis of Data From Retrospective Studies of Disease. JNCI J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [CrossRef] [PubMed]
- Paule, R.C.; Mandel, J. Consensus Values and Weighting Factors. J. Res. Natl. Bur. Stand. 1982, 87, 377–385. [Google Scholar] [CrossRef]
- Thompson, S.G.; Turner, R.M.; Warn, D.E. Multilevel models for meta-analysis, and their application to absolute risk differences. Stat. Methods Med. Res. 2001, 10, 375–392. [Google Scholar] [CrossRef]
- Viechtbauer, W. Bias and Efficiency of Meta-Analytic Variance Estimators in the Random-Effects Model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef]
- Celentano, C.; Matarrelli, B.; Pavone, G.; Vitacolonna, E.; Mattei, P.A.; Berghella, V.; Liberati, M. The influence of different inositol stereoisomers supplementation in pregnancy on maternal gestational diabetes mellitus and fetal outcomes in high-risk patients: A randomized controlled trial. J. Matern. Fetal Neonatal Med. 2020, 33, 743–751. [Google Scholar] [CrossRef] [PubMed]
- D’Anna, R.; Di Benedetto, A.; Scilipoti, A.; Santamaria, A.; Interdonato, M.L.; Petrella, E.; Neri, I.; Pintaudi, B.; Corrado, F.; Facchinetti, F. Myo-inositol Supplementation for Prevention of Gestational Diabetes in Obese Pregnant Women: A Randomized Controlled Trial. Obstet. Gynecol. 2015, 126, 310–315. [Google Scholar] [CrossRef] [PubMed]
- D’Anna, R.; Scilipoti, A.; Giordano, D.; Caruso, C.; Cannata, M.L.; Interdonato, M.L.; Corrado, F.; Di Benedetto, A. myo-Inositol supplementation and onset of gestational diabetes mellitus in pregnant women with a family history of type 2 diabetes: A prospective, randomized, placebo-controlled study. Diabetes Care 2013, 36, 854–857. [Google Scholar] [CrossRef]
- Esmaeilzadeh, S.; Ghadimi, R.; Mashayekh-Amiri, S.; Delavar, M.A.; Basirat, Z. The effect of myo-inositol supplementation on the prevention of gestational diabetes in overweight pregnant women: A randomized, double-blind, controlled trial. Minerva Obstet. Gynecol. 2022, 75, 357–364. [Google Scholar] [CrossRef]
- Farren, M.; Daly, N.; McKeating, A.; Kinsley, B.; Turner, M.J.; Daly, S. The Prevention of Gestational Diabetes Mellitus with Antenatal Oral Inositol Supplementation: A Randomized Controlled Trial. Diabetes Care 2017, 40, 759–763. [Google Scholar] [CrossRef]
- Matarrelli, B.; Vitacolonna, E.; D’Angelo, M.; Pavone, G.; Mattei, P.A.; Liberati, M.; Celentano, C. Effect of dietary myo-inositol supplementation in pregnancy on the incidence of maternal gestational diabetes mellitus and fetal outcomes: A randomized controlled trial. J. Matern. Fetal Neonatal Med. 2013, 26, 967–972. [Google Scholar] [CrossRef]
- Santamaria, A.; Di Benedetto, A.; Petrella, E.; Pintaudi, B.; Corrado, F.; D’Anna, R.; Neri, I.; Facchinetti, F. Myo-inositol may prevent gestational diabetes onset in overweight women: A randomized, controlled trial. J. Matern. Fetal Neonatal Med. 2016, 29, 3234–3237. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Corrado, F.; Caruso, S.; Di Benedetto, A.; Giunta, L.; Cianci, A.; D’Anna, R. Myo-inositol supplementation to prevent gestational diabetes in overweight non-obese women: Bioelectrical impedance analysis, metabolic aspects, obstetric and neonatal outcomes—A randomized and open-label, placebo-controlled clinical trial. Int. J. Food Sci. Nutr. 2021, 72, 670–679. [Google Scholar] [CrossRef]
- Balsells, M.; García-Patterson, A.; Gich, I.; Corcoy, R. Maternal and Fetal Outcome in Women with Type 2 versus Type 1 Diabetes Mellitus: A Systematic Review and Metaanalysis. J. Clin. Endocrinol. Metab. 2009, 94, 4284–4291. [Google Scholar] [CrossRef]
- Clausen, T.D.; Mathiesen, E.; Ekbom, P.; Hellmuth, E.; Mandrup-Poulsen, T.; Damm, P. Poor Pregnancy Outcome in Women with Type 2 Diabetes. Diabetes Care 2005, 28, 323–328. [Google Scholar] [CrossRef]
- Juan, J.; Sun, Y.; Wei, Y.; Wang, S.; Song, G.; Yan, J.; Zhou, P.; Yang, H. Progression to type 2 diabetes mellitus after gestational diabetes mellitus diagnosed by IADPSG criteria: Systematic review and meta-analysis. Front. Endocrinol. 2022, 13, 1012244. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, D.M.; Kuang, A.; Lowe, L.P.; Hamilton, J.; Lawrence, J.M.; Lebenthal, Y.; Brickman, W.J.; Clayton, P.; Ma, R.C.; McCance, D.; et al. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Glycemia and Childhood Glucose Metabolism. Diabetes Care 2019, 42, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, F.; Unfer, V.; Dewailly, D.; Kamenov, Z.A.; Diamanti-Kandarakis, E.; Laganà, A.S.; Nestler, J.E.; Soulage, C.O. Inositols in Polycystic Ovary Syndrome: An Overview on the Advances. Trends Endocrinol. Metab. 2020, 31, 435–447. [Google Scholar] [CrossRef]
- Unfer, V.; Nestler, J.E.; Kamenov, Z.A.; Prapas, N.; Facchinetti, F. Effects of Inositol(s) in Women with PCOS: A Systematic Review of Randomized Controlled Trials. Int. J. Endocrinol. 2016, 2016, 1849162. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.Y.; Wong, M.M.H.; Pang, S.S.H.; Lo, K.K.H. Dietary supplementation for gestational diabetes prevention and management: A meta-analysis of randomized controlled trials. Arch. Gynecol. Obstet. 2021, 303, 1381–1391. [Google Scholar] [CrossRef]
- Guo, X.; Guo, S.; Miao, Z.; Li, Z.; Zhang, H. Myo-inositol lowers the risk of developing gestational diabetic mellitus in pregnancies: A systematic review and meta-analysis of randomized controlled trials with trial sequential analysis. J. Diabetes Its Complicat. 2018, 32, 342–348. [Google Scholar] [CrossRef]
- Motuhifonua, S.K.; Lin, L.; Alsweiler, J.; Crawford, T.J.; Crowther, C.A. Antenatal dietary supplementation with myo-inositol for preventing gestational diabetes. Cochrane Database Syst. Rev. 2023, 2, CD011507. [Google Scholar] [CrossRef]
- Vitagliano, A.; Saccone, G.; Cosmi, E.; Visentin, S.; Dessole, F.; Ambrosini, G.; Berghella, V. Inositol for the prevention of gestational diabetes: A systematic review and meta-analysis of randomized controlled trials. Arch. Gynecol. Obstet. 2019, 299, 55–68. [Google Scholar] [CrossRef]
- Oostdam, N.; van Poppel, M.N.; Wouters, M.G.; van Mechelen, W. Interventions for preventing gestational diabetes mellitus: A systematic review and meta-analysis. J. Women’s Health 2011, 20, 1551–1563. [Google Scholar] [CrossRef]
- Dell’Edera, D.; Sarlo, F.; Allegretti, A.; Simone, F.; Lupo, M.G.; Epifania, A.A. The influence of D-chiro-inositol and D-myo-inositol in pregnant women with glucose intolerance. Biomed. Rep. 2017, 7, 169–172. [Google Scholar] [CrossRef]
- Godfrey, K.M.; Barton, S.J.; El-Heis, S.; Kenealy, T.; Nield, H.; Baker, P.N.; Chong, Y.S.; Cutfield, W.; Chan, S.-Y.; Group, N.S. Myo-Inositol, Probiotics, and Micronutrient Supplementation From Preconception for Glycemia in Pregnancy: NiPPeR International Multicenter Double-Blind Randomized Controlled Trial. Diabetes Care 2021, 44, 1091–1099. [Google Scholar] [CrossRef]
- Saravanan, P.; Sukumar, N.; Adaikalakoteswari, A.; Goljan, I.; Venkataraman, H.; Gopinath, A.; Bagias, C.; Yajnik, C.S.; Stallard, N.; Ghebremichael-Weldeselassie, Y.; et al. Association of maternal vitamin B12 and folate levels in early pregnancy with gestational diabetes: A prospective UK cohort study (PRiDE study). Diabetologia 2021, 64, 2170–2182. [Google Scholar] [CrossRef]
- D’Anna, R.; Corrado, F.; Loddo, S.; Gullo, G.; Giunta, L.; Di Benedetto, A. Myoinositol plus α-lactalbumin supplementation, insulin resistance and birth outcomes in women with gestational diabetes mellitus: A randomized, controlled study. Sci. Rep. 2021, 11, 8866. [Google Scholar] [CrossRef]
- Fraticelli, F.; Celentano, C.; Zecca, I.A.; Di Vieste, G.; Pintaudi, B.; Liberati, M.; Franzago, M.; Di Nicola, M.; Vitacolonna, E. Effect of inositol stereoisomers at different dosages in gestational diabetes: An open-label, parallel, randomized controlled trial. Acta Diabetol. 2018, 55, 805–812. [Google Scholar] [CrossRef]
- Hegyi, P.; Erőss, B.; Izbéki, F.; Párniczky, A.; Szentesi, A. Accelerating the translational medicine cycle: The Academia Europaea pilot. Nat. Med. 2021, 27, 1317–1319. [Google Scholar] [CrossRef]
- Hegyi, P.; Petersen, O.H.; Holgate, S.; Erőss, B.; Garami, A.; Szakács, Z.; Dobszai, D.; Balaskó, M.; Kemény, L.; Peng, S.; et al. Academia Europaea Position Paper on Translational Medicine: The Cycle Model for Translating Scientific Results into Community Benefits. J. Clin. Med. 2020, 9, 1532. [Google Scholar] [CrossRef]
- Tahir, F.; Majid, Z. Inositol Supplementation in the Prevention of Gestational Diabetes Mellitus. Cureus 2019, 11, e5671. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Number of Patients (I/C) | Age (Year) (I/C) ‡ | BMI (kg/m2) (I/C) ‡ | Risk Factors/Inclusion Criteria | Intervention | Outcomes | Baseline Fasting Glucose (mg/dL) ‡ |
|---|---|---|---|---|---|---|---|---|
| Celentano, 2018 [33] | Italy | 105/52 | 33.8/33.9 | 23.8/24.4 | elevated fasting glucose at first trimester blood exams. | 4 g MI + 400 mcg FA; 500 mg DCI + 400 mcg FA; 1100 mg MI + 27.6 mg DCI | GDM, OGTT, insulin therapy, preeclampsia or pregnancy-induced hypertension, C-section, preterm birth, neonatal hypoglycemia, NICU admission | 97.2/97.2 |
| D’Anna, 2013 [35] | Italy | 99/98 | 31/31.6 | 22.8/23.6 | family history of type 2 DM | 4 g MI + 40 mcg FA | GDM, gestational hypertension, C-section, shoulder dystocia, preterm delivery, gestational age at delivery, neonatal hypoglycemia. | - |
| D’Anna, 2015 [34] | Italy | 97/104 | 30.9/31.7 | 33.8/ 33.8 | prepregnancy BMI 30 or greater | 4 g MI + 40 mcg FA | GDM, OGTT, insulin treatment, gestational hypertension, C-section, shoulder dystocia, preterm birth, gestational age at delivery, macrosomia, birth weight, neonatal hypoglycemia, NICU admission | 83.1/82.3 |
| Esmaeilzadeh, 2022 [36] | Iran | 27/29 | 27.8/29.3 | 27.3/26.9 | overweight patients (prepregnancy BMI above 25 and under 30), age 18–40 | 2 g MI + 200 mcg FA | GDM, fasting blood sugar, fasting blood insulin, insulin treatment, preeclampsia or pregnancy-induced hypertension, shoulder dystocia, C-section, preterm delivery, NICU admission | 84/85.2 |
| Farren, 2017 [37] | Ireland | 120/120 | 31.1/31.5 | 26/26.2 | patients with a family history in a first-degree relative of diabetes, either type 1 or type 2. | 1100 mg MI + 27.6 mg DCI + 400 mcg FA | GDM, OGTT, preeclampsia or pregnancy-induced hypertension, C-section, shoulder dystocia, preterm delivery, gestatational age at delivery, macrosomia, birth weight, hypoglycemia, NICU admission | - |
| Matarelli, 2013 [38] | Italy | 35/38 | 33/33.8 | 23.5/24.7 | elevated fasting glucose and BMI under 35 | 4 g MI + 400 mcg FA | GDM, OGTT, insulin therapy, gestational age at delivery, birth weight, neonatal hypoglycemia | 97.2/97.2 |
| Santamaria, 2015 [39] | Italy | 95/102 | 32.1/32.7 | 26.9/27.1 | overweight patients (prepregnancy BMI above 25 and under 30) | 4 g MI + 400 mcg FA | GDM, OGTT, insulin treatment, gestational hypertension, shoulder dystocia, C-section, preterm delivery gestational age at delivery, macrosomia, neonatal hypoglycemia, NICU admission | 81.08/78.63 |
| Vitale, 2020 [40] | Italy | 110/113 | 27.18/27.95 | 27/26.68 | overweight patients (prepregnancy BMI above 25 and under 30) | 4 g MI + 400 mcg FA | GDM, OGTT, gestational hypertension | 82.2/83.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greff, D.; Váncsa, S.; Váradi, A.; Szinte, J.; Park, S.; Hegyi, P.; Nyirády, P.; Ács, N.; Horváth, E.M.; Várbíró, S. Myoinositols Prevent Gestational Diabetes Mellitus and Related Complications: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2023, 15, 4224. https://doi.org/10.3390/nu15194224
Greff D, Váncsa S, Váradi A, Szinte J, Park S, Hegyi P, Nyirády P, Ács N, Horváth EM, Várbíró S. Myoinositols Prevent Gestational Diabetes Mellitus and Related Complications: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2023; 15(19):4224. https://doi.org/10.3390/nu15194224
Chicago/Turabian StyleGreff, Dorina, Szilárd Váncsa, Alex Váradi, Julia Szinte, Sunjune Park, Péter Hegyi, Péter Nyirády, Nándor Ács, Eszter Mária Horváth, and Szabolcs Várbíró. 2023. "Myoinositols Prevent Gestational Diabetes Mellitus and Related Complications: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 15, no. 19: 4224. https://doi.org/10.3390/nu15194224
APA StyleGreff, D., Váncsa, S., Váradi, A., Szinte, J., Park, S., Hegyi, P., Nyirády, P., Ács, N., Horváth, E. M., & Várbíró, S. (2023). Myoinositols Prevent Gestational Diabetes Mellitus and Related Complications: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients, 15(19), 4224. https://doi.org/10.3390/nu15194224