
Herbal Remedies for Constipation-Predominant Irritable Bowel Syndrome: A Systematic Review of Randomized Controlled Trials

 , ,
, ,  , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
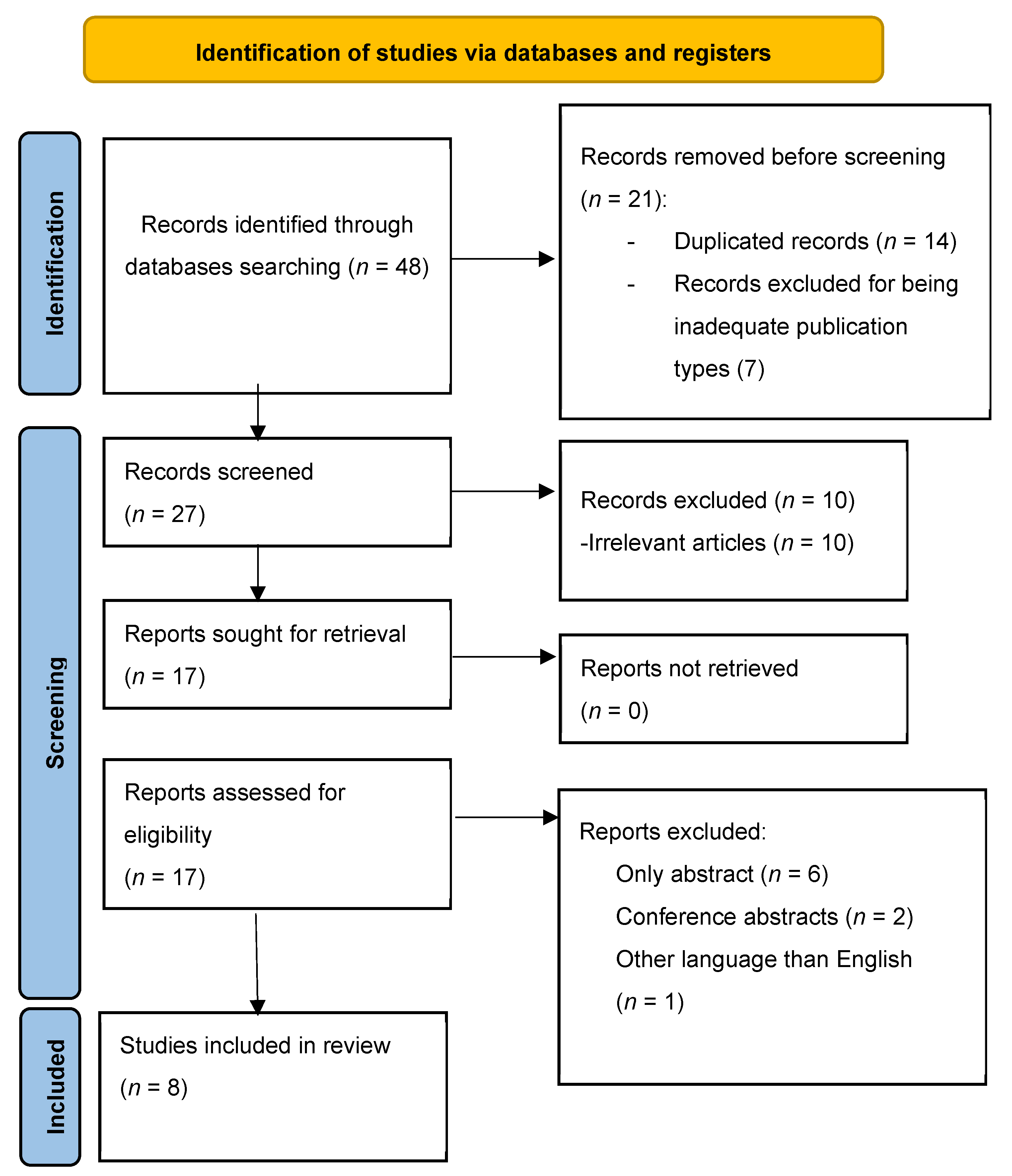
2.1. Search Strategy
2.2. Study Selection
- a)
- Study Design: Randomized controlled trials (RCTs), observational studies (cohort, case-control, cross-sectional), and clinical trials investigating the use of herbal remedies in the management of IBS-C were considered.
- b)
- Participants: Studies involving adult patients diagnosed with IBS-C according to established diagnostic criteria, such as Rome criteria, were included.
- c)
- Intervention: Studies evaluating the use of herbal remedies as the primary intervention for IBS-C management were considered eligible. Herbal remedies included botanical preparations derived from plants with potential therapeutic effects on IBS-C symptoms.
- d)
- Outcomes: Studies reporting relevant clinical outcomes related to IBS-C symptom improvement, such as changes in bowel habits, abdominal discomfort, bloating, and overall quality of life, were included.
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
2.6. Ethical Considerations
2.7. Reporting
2.8. Limitations
3. Results
3.1. Padma Lax and IBS-C
3.2. Chinese Herbal Medicine and IBS-C
3.3. Persian Herbal Syrup and IBS-C
3.4. Flixweed and Fig for IBS-C
3.5. A Combination of Quebracho, Conker Tree, and M. balsamea Willd Extract for IBS-C
3.6. Kiwifruit and IBS-C
3.7. Modified Sinisan for IBS-C
3.8. Geraniol for IBS-C
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chang, L.; Sultan, S.; Lembo, A.; Verne, G.N.; Smalley, W.; Heidelbaugh, J.J. AGA Clinical Practice Guideline on the Pharmacological Management of Irritable Bowel Syndrome with Constipation. Gastroenterology 2022, 163, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rao, S.S.C.; Kearns, K.; Orleck, K.D.; Waldman, S.A. Review article: Diagnosis, management and patient perspectives of the spectrum of constipation disorders. Aliment. Pharmacol. Ther. 2021, 53, 1250–1267. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.A.; Chang, C.-H. Burden of Constipation: Looking Beyond Bowel Movements. Am. J. Gastroenterol. 2022, 117, S2–S5. [Google Scholar] [CrossRef]
- Bellini, M.; Gambaccini, D.; Usai-Satta, P.; De Bortoli, N.; Bertani, L.; Marchi, S.; Stasi, C. Irritable bowel syndrome and chronic constipation: Fact and fiction. World J. Gastroenterol. 2015, 21, 11362–11370. [Google Scholar] [CrossRef]
- Bauer, B.A. Herbal therapy: What a clinician needs to know to counsel patients effectively. Mayo Clin. Proc. 2000, 75, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Izzo, A.A.; Borrelli, F.; Capasso, R. Herbal medicine: The dangers of drug interaction. Trends Pharmacol. Sci. 2002, 23, 358–361, author reply 359. [Google Scholar] [CrossRef]
- Ernst, E. Herbal medicines: Balancing benefits and risks. Novartis Found. Symp. 2007, 282, 154–167. [Google Scholar]
- Borins, M. The dangers of using herbs. What your patients need to know. Postgrad. Med. 1998, 104, 91–100. [Google Scholar] [CrossRef]
- Wong, W.W.; Gabriel, A.; Maxwell, G.P.; Gupta, S.C. Bleeding risks of herbal, homeopathic, and dietary supplements: A hidden nightmare for plastic surgeons? Aesthet. Surg. J. 2012, 32, 332–346. [Google Scholar] [CrossRef]
- Chambial, S.; Bhardwaj, P.; Mahdi, A.A.; Sharma, P. Lead Poisoning Due to Herbal Medications. Indian J. Clin. Biochem. 2017, 32, 246–247. [Google Scholar] [CrossRef]
- Sallon, S.; Ben-Arye, E.; Davidson, R.; Shapiro, H.; Ginsberg, G.; Ligumsky, M. A novel treatment for constipation-predominant irritable bowel syndrome using Padma Lax, a Tibetan herbal formula. Digestion 2002, 65, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Bensoussan, A.; Kellow, J.E.; Bourchier, S.J.; Fahey, P.; Shim, L.; Malcolm, A.; Boyce, P. Efficacy of a Chinese Herbal Medicine in Providing Adequate Relief of Constipation-predominant Irritable Bowel Syndrome: A Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2015, 13, 1946–1954.e1. [Google Scholar] [CrossRef] [PubMed]
- Pazhouh, H.K.; Hosseini, S.M.A.; Taghipour, A.; Hamedi, S.; Noras, M. Anti-irritable Bowel Syndrome Syrup Improves Constipation-Predominant Irritable Bowel Syndrome: A Randomized, Placebo-Controlled Trial. Chin. J. Integr. Med. 2020, 26, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Pourmasoumi, M.; Ghiasvand, R.; Darvishi, L.; Hadi, A.; Bahreini, N.; Keshavarzpour, Z. Comparison and Assessment of Flixweed and Fig Effects on Irritable Bowel Syndrome with Predominant Constipation: A Single-Blind Randomized Clinical Trial. Explore 2019, 15, 198–205. [Google Scholar] [CrossRef]
- Brown, K.; Scott-Hoy, B.; Jennings, L. Efficacy of a Quebracho, Conker Tree, and M. balsamea Willd Blended Extract in a Randomized Study in Patients with Irritable Bowel Syndrome with Constipation. J. Gastroenterol. Hepatol. Res. 2015, 4, 1762–1767. [Google Scholar] [CrossRef][Green Version]
- Chang, C.C.; Lin, Y.T.; Lu, Y.T.; Liu, Y.S.; Liu, J.F. Kiwifruit improves bowel function in patients with irritable bowel syndrome with constipation. Asia Pac. J. Clin. Nutr. 2010, 19, 451–457. [Google Scholar]
- Yu, S.P.; Ye, H.; Ha, N.L.; Ding, S.Q.; Chen, G. Effect of modified Sinisan on anorectal manometry of the constipation predominant type of irritable bowel syndrome. Chin. J. Integr. Med. 2005, 11, 27–30. [Google Scholar]
- Ricci, C.; Rizzello, F.; Valerii, M.C.; Spisni, E.; Gionchetti, P.; Turroni, S.; Candela, M.; D’Amico, F.; Spigarelli, R.; Bellocchio, I.; et al. Geraniol Treatment for Irritable Bowel Syndrome: A Double-Blind Randomized Clinical Trial. Nutrients 2022, 14, 4208. [Google Scholar] [CrossRef]
- Hęś, M.; Dziedzic, K.; Górecka, D.; Jędrusek-Golińska, A.; Gujska, E. Aloe vera (L.) Webb.: Natural Sources of Antioxidants—A Review. Plant Foods Hum. Nutr. 2019, 74, 255–265. [Google Scholar] [CrossRef]
- Kledecka, A.; Siejak, P.; Pratap-Singh, A.; Kowalczewski, P.Ł.; Fathordoobady, F.; Jarzębski, M.; Smułek, W. Extracts from Frangula alnus Mill. and Their Effects on Environmental and Probiotic Bacteria. Plants 2022, 11, 2719. [Google Scholar] [CrossRef]
- Mills, S.; Bone, K. Principles and Practice of Phytotherapy: Modern Herbal Medicine, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 17–82. [Google Scholar]
- Petkova, N.; Ivanova, L.; Filova, G.; Ivanov, I.; Denev, P. Antioxidants and carbohydrate content in infusions and microwave extracts from eight medicinal plants. J. Appl. Pharm. Sci. 2017, 7, 17–82. [Google Scholar] [CrossRef]
- Mirzaee, F.; Hosseini, A.; Jouybari, H.B.; Davoodi, A.; Azadbakht, M. Medicinal, biological and phytochemical properties of Gentiana species. J. Tradit. Complement. Med. 2017, 7, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.; Olatunde, A.; El-Mleeh, A.; Hetta, H.F.; Al-Rejaie, S.; Alghamdi, S.; Zahoor, M.; Magdy Beshbishy, A.; Murata, T.; Zaragoza-Bastida, A.; et al. Bioactive Compounds, Pharmacological Actions, and Pharmacokinetics of Wormwood (Artemisia absinthium). Antibiotics 2020, 9, 353. [Google Scholar] [CrossRef] [PubMed]
- Moradzadeh, M.; Hosseini, A.; Rakhshandeh, H.; Aghaei, A.; Sadeghnia, H.R. Cuscuta campestris induces apoptosis by increasing reactive oxygen species generation in human leukemic cells. Avicenna J. Phytomed. 2018, 8, 237–245. [Google Scholar]
- Ali, M.A. Cassia Fistula Linn: A review of phytochemical and pharmacological studies. Int. J. Pharm. Sci. Res. 2014, 5, 2125–2130. [Google Scholar]
- Patocka, J.; Navratilova, Z. Bioactivity of Echium Amoenum: A Mini Review. Biomed. J. Sci. Tech. Res. 2019, 20, 1–2. [Google Scholar] [CrossRef]
- Petrisor, G.; Motelica, L.; Craciun, L.N.; Oprea, O.C.; Ficai, D.; Ficai, A. Melissa officinalis: Composition, Pharmacological Effects and Derived Release Systems-A Review. Int. J. Mol. Sci. 2022, 23, 3591. [Google Scholar] [CrossRef]
- Nimrouzi, M.; Zarshenas, M.M. Phytochemical and pharmacological aspects of Descurainia sophia Webb ex Prantl: Modern and traditional applications. Avicenna J. Phytomed. 2016, 6, 266–272. [Google Scholar]
- Kamiloglu, S.; Akgun, B. Bioactive Compounds of Fig (Ficus carica). In Production, Processing, and Properties; Ramadan, M.F., Ed.; Springer: Cham, Switzerland, 2023; pp. 479–512. [Google Scholar]
- Rezagholizadeh, L.; Aghamohammadian, M.; Oloumi, M.; Banaei, S.; Mazani, M.; Ojarudi, M. Inhibitory effects of Ficus carica and Olea europaea on pro-inflammatory cytokines: A review. Iran. J. Basic Med. Sci. 2022, 25, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Dong, X.; Yin, X.; Wang, W.; You, L.; Ni, J. Radix Bupleuri: A Review of Traditional Uses, Botany, Phytochemistry, Pharmacology, and Toxicology. BioMed Res. Int. 2017, 2017, 7597596. [Google Scholar] [CrossRef]
- Deshmukh, N.S.; Stohs, S.J.; Magar, C.C.; Kale, A.; Sowmya, B. Bitter orange (Citrus aurantium L.) extract subchronic 90-day safety study in rats. Toxicol. Rep. 2017, 4, 598–613. [Google Scholar] [CrossRef] [PubMed]
- Jo, H.G.; Lee, G.Y.; Baek, C.Y.; Song, H.S.; Lee, D. Analgesic and Anti-Inflammatory Effects of Aucklandia lappa Root Extracts on Acetic Acid-Induced Writhing in Mice and Monosodium Iodoacetate-Induced Osteoarthritis in Rats. Plants 2020, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.J.; Zhao, Z.Y.; Chang, L.K.; Cao, Y.; Wang, S.; Kang, C.Z.; Wang, H.Y.; Zhou, L.; Huang, L.Q.; Guo, L.P. Atractylodis Rhizoma: A review of its traditional uses, phytochemistry, pharmacology, toxicology and quality control. J. Ethnopharmacol. 2021, 266, 113415. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Yu, X.; Wu, Y.; Shiraishi, F.; Kawahara, N.; Komatsu, K. Genetic and chemical characterization of white and red peony root derived from Paeonia lactiflora. J. Nat. Med. 2015, 69, 35–45. [Google Scholar] [CrossRef]
- Li, W.; Tang, Y.; Chen, Y.; Duan, J.A. Advances in the chemical analysis and biological activities of chuanxiong. Molecules 2012, 17, 10614–10651. [Google Scholar] [CrossRef]
- Chao, W.W.; Lin, B.F. Bioactivities of major constituents isolated from Angelica sinensis (Danggui). Chin. Med. 2011, 6, 29. [Google Scholar] [CrossRef]
- Mamedov, N.A.; Egamberdieva, D. Phytochemical Constituents and Pharmacological Effects of Licorice: A Review. Plant Hum. Health 2019, 3, 1–21. [Google Scholar] [CrossRef]
- Omer, A.; Quigley, E.M.M. An update on prucalopride in the treatment of chronic constipation. Therap. Adv. Gastroenterol. 2017, 10, 877–887. [Google Scholar] [CrossRef]
- National Institute of Child Health and Human Development. Drugs and Lactation Database (LactMed®); National Institute of Child Health and Human Development: Bethesda, MD, USA, 2006.
- Kim, H.W.; Li, H.; Kim, H.S.; Shin, S.E.; Jung, W.K.; Ha, K.S.; Han, E.T.; Hong, S.H.; Choi, I.W.; Park, W.S. Cisapride, a selective serotonin 5-HT4-receptor agonist, inhibits voltage-dependent K(+) channels in rabbit coronary arterial smooth muscle cells. Biochem. Biophys. Res. Commun. 2016, 478, 1423–1428. [Google Scholar] [CrossRef]
- Mączka, W.; Wińska, K.; Grabarczyk, M. One Hundred Faces of Geraniol. Molecules 2020, 25, 3303. [Google Scholar] [CrossRef]
- Currò, D.; Ianiro, G.; Pecere, S.; Bibbò, S.; Cammarota, G. Probiotics, fibre and herbal medicinal products for functional and inflammatory bowel disorders. Br. J. Pharmacol. 2017, 174, 1426–1449. [Google Scholar] [CrossRef]
- Gemcioglu, E.; Yılmaz Cakmak, N.; Baser, S.; Kocaoz, S.; Ersoy, O. Factors affecting the use of herbal products in patients with Irritable Bowel Syndrome and their results: Case-control study. BMC Gastroenterol. 2022, 22, 43. [Google Scholar] [CrossRef]
- Moayyedi, P.; Andrews, C.N.; MacQueen, G.; Korownyk, C.; Marsiglio, M.; Graff, L.; Kvern, B.; Lazarescu, A.; Liu, L.; Paterson, W.G.; et al. Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS). J. Can. Assoc. Gastroenterol. 2019, 2, 6–29. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Travica, N.; Dorairaj, R.; Sali, A. Herbal formula improves upper and lower gastrointestinal symptoms and gut health in Australian adults with digestive disorders. Nutr. Res. 2020, 76, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic-Dinic, B.; Tesic-Rajkovic, S.; Grgov, S.; Petrovic, G.; Zivkovic, V. Irritable bowel syndrome—From etiopathogenesis to therapy. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2018, 162, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Li, J.; Wang, Y.; Zhang, S. Different therapies of Chinese herbal medicine for diarrhea-predominant irritable bowel syndrome: A network meta-analysis of double-blinded, placebo-controlled trials. J. Ethnopharmacol. 2023, 317, 116672. [Google Scholar] [CrossRef] [PubMed]
- Bi, Z.; Zheng, Y.; Yuan, J.; Bian, Z. The Efficacy and Potential Mechanisms of Chinese Herbal Medicine on Irritable Bowel Syndrome. Curr. Pharm. Des. 2017, 23, 5163–5172. [Google Scholar] [CrossRef]
- Hawrelak, J.A.; Myers, S.P. Effects of two natural medicine formulations on irritable bowel syndrome symptoms: A pilot study. J. Altern. Complement. Med. 2010, 16, 1065–1071. [Google Scholar] [CrossRef]
- Hawrelak, J.A.; Wohlmuth, H.; Pattinson, M.; Myers, S.P.; Goldenberg, J.Z.; Harnett, J.; Cooley, K.; Van De Venter, C.; Reid, R.; Whitten, D.L. Western herbal medicines in the treatment of irritable bowel syndrome: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 48, 102233. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Brenner, D.M. Efficacy and Safety of Over-the-Counter Therapies for Chronic Constipation: An Updated Systematic Review. Am. J. Gastroenterol. 2021, 116, 1156–1181. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Portincasa, P.; Maes, N.; Albert, A. Efficacy of bio-optimized extracts of turmeric and essential fennel oil on the quality of life in patients with irritable bowel syndrome. Ann. Gastroenterol. 2018, 31, 685–691. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Study Design | Participants | Intervention | Main Findings |
|---|---|---|---|---|
| Sallon et al. (2002) [11] | Randomized, double-blind, placebo-controlled clinical trial | 61 patients with IBS-C | Padma Lax vs. placebo for 12 weeks 2 tablets/day or 1 tablet/day if diarrhea or loose stools occurred. 1 tablet (482 mg) contained: Aloes standardized extract (12 mg) Calumbae root (10 mg) Condurango bark (10 mg) Frangula bark (52.5 mg) Gentian root (35 mg) Elecampane rhizome (35 mg) Tropical almond fruit (35 mg) Long pepper (3.5 mg) Cascara bark (52.5 mg) Chinese rhubarb root (70 mg) Nux vomica seed (1.75 mg) Ginger root (70 mg). It also contained 3 non-herbal elements: Heavy kaolin (25 mg) Sodium bicarbonate (15 mg) Sodium sulfate (35 mg). The excipients used were: Silicium dioxide (2.4 mg) Magnesium stearate (4.6 mg). | Statistically significant improvements were found in: Constipation severity Number of daily bowel movements Abdominal pain affecting daily activities Presence of moderate or severe pain Abdominal distention severity Incomplete evacuation Flatulence. There were no significant improvements in: Abdominal distention prevalence Abdominal pain severity. 10 patients complained of mild side effects: Slight headache (1 patient) Nausea (1 patient) Hoarseness (1 patient) Diarrhea or loose stools (7 patients) with rapid resolution when lowering dose from 2 tablets/day to 1 tablet/day. |
| Bensoussan et al. (2015) [12] | Two-arm, randomized, double-blind, placebo-controlled clinical trial | 125 patients with IBS-C | CHM vs. placebo for 8 weeks 10 capsules (4.2 g)/day, 5 in the morning and 5 in the night containing: Paeonia lactiflora PALL., radix (23%) Citrus aurantium L., Fructus immaturas (20%) Magnolia officinalis REHD. and WILS., cortex (14.5%) Citrus reticulata L., pericarpi-um (14.5%) Glycyrrhiza uralensis FISCH., root (11%) Rheum palmatum L., radix (10%) Atractylodes lancea (THUNB.) DC, rhizome (7%). | There were statistically significant changes at 8 weeks in: Adequate relief (PP) Bowel habits Frequency of hard lumpy stools Bothersomeness of hard lumpy stools Straining during bowel movement Stool form Physical functioning. There were statistically significant changes at 16 weeks in: Physical functioning. There was no significant improvement at 8 weeks in: Adequate relief (ITT). There was no significant improvement at 16 weeks in: Adequate relief (PP, ITT) Bowel habits Frequency of hard lumpy stools Bothersomeness of hard lumpy stools Straining during bowel movement Stool form Abdominal pain Abdominal distension Interference with life Overall quality of life Depression Anxiety Stress Work productivity. 6 patients complained of moderate side effects: Diarrhea (3 patients) Blood in urine (1 patient) Increased bloating (1 patient) Dizziness and headaches (1 patient). |
| Pazhouh et al. (2020) [13] | Block-randomized, double-blind, placebo-controlled clinical trial | 70 patients with IBS-C | PHS vs. placebo for 6 weeks 5 mL every 8 h of the syrup prepared with: Artemisia Absinthium (100 mg) Cuscuta Campestris (100 mg) Cassia Fistula (230 mg) Echium Amoenium (270 mg) Mellisa Officinalis (190 mg) British Pharmacopoeia syrup to make the mixture 100 mL. | There was a significant improvement in: Positive responses to treatment Severity score Bristol Stool Score. There was no significant improvement in: Anxiety score Depression score. 4 patients complained of negligible side effects: Headache (2 patients) Drowsiness (1 patient) Increase in menstrual bleeding (1 patient). |
| Pourmasoumi et al. (2019) [14] | Single-blind, randomized, placebo-controlled clinical trial | 142 patients with IBS-C | Flixweed vs. fig vs. placebo for 4 months 60 g flixweed and 90 g fig/day, half before breakfast and half before lunch. | Statistically significant improvements were found in: IBS Severity Score System Quality of life Abdominal pain frequency Interference of life Dissatisfaction with bowel habits. No significant difference was found in: Abdominal pain severity C-reactive protein levels. There was no statistically significant difference between flixweed and fig. No adverse effects were reported. |
| Brown et al. (2015) [15] | Single-site, randomized, double-blind, placebo-controlled clinical trial | 16 patients with IBS-C | Blended extract of Quebracho, Conker Tree, and M. balsamea Willd vs. placebo for 2 weeks Extract consisting of: Quebracho (150 mg) Conker Tree (470 mg) M. balsamea Willd oil (0.2 mL). | There was a significant improvement in: Constipation Bloating. No side effects were reported. |
| Chang et al. (2010) [16] | Restricted randomization (3:1), placebo-controlled clinical trial | 76 patients, 60 with IBS-C and 16 healthy | Kiwifruit vs. placebo for 4 weeks 2 Hayward green kiwifruits/day. | Statistically significant improvements were found in: Defecation frequency Colon transit time. No significant improvement was found in: Fecal volume change Life stress Post-defecation feelings. No adverse effects were reported. |
| Yu et al. (2005) [17] | Randomized, placebo-controlled clinical trial | 47 patients with IBS-C | Modified Sinisan formula vs. Cisapride for 8 weeks 1 dose divided into 2 portions consisting of: Thorowax root (10 g) Immature bitter orange (10 g) Aucklandia root (10 g) Spice-bush root (10 g) Bighead atractylodes rhizome (20 g) White peony root (10 g) Ligusticum chuanxiong rhizome (10 g) Chinese angelica root (10 g) Licorice (5 g) water decocted. | Statistically significant differences were found in: Efficacy Symptom scoring Recurrence rate Rectal threshold feeling Maximal tolerance volume Rectum compliance. No significant difference was found in: Anal resting pressure Anal systolic pressure Anal diastolic pressure. No side effects are mentioned. |
| Ricci et al. (2022) [18] | interventional, prospective, multicentric, randomized, double-blinded, placebo-controlled trial | 56 patients with IBS | Geraniol vs. placebo for 4 weeks 1 capsule (470 mg)/day consisting of: Palmrose EO high geraniol (90 mg) Pulverized Zyngiber officinalis root (360 mg). The excipients used were: Vegetal magnesium stearate (10 mg) Silicon dioxide (10 mg). IBS-SSS GM composition Inflammatory markers | There was a statistically significant difference in: Abdominal Pain Days with abdominal Pain in the last 10 Bloating Satisfaction bowel habits IBS-SSS Score IBSS-SSS Score variations Responders (reduction 50 points IBS-SSS). There was no difference in: Interference with daily activities. 2 patients complained of side effects, 1 of which were unspecified gastric symptoms. Significant reduction in IBS-SSS in the geraniol group. Increase in the Ruminococcaceae and Oscillospira species and decrease in the Erysipelotrichaceae and Clostridiaceae families. No changes when it comes to inflammatory biomarkers. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiarioni, G.; Popa, S.L.; Ismaiel, A.; Pop, C.; Dumitrascu, D.I.; Brata, V.D.; Duse, T.A.; Incze, V.; Surdea-Blaga, T. Herbal Remedies for Constipation-Predominant Irritable Bowel Syndrome: A Systematic Review of Randomized Controlled Trials. Nutrients 2023, 15, 4216. https://doi.org/10.3390/nu15194216
Chiarioni G, Popa SL, Ismaiel A, Pop C, Dumitrascu DI, Brata VD, Duse TA, Incze V, Surdea-Blaga T. Herbal Remedies for Constipation-Predominant Irritable Bowel Syndrome: A Systematic Review of Randomized Controlled Trials. Nutrients. 2023; 15(19):4216. https://doi.org/10.3390/nu15194216
Chicago/Turabian StyleChiarioni, Giuseppe, Stefan Lucian Popa, Abdulrahman Ismaiel, Cristina Pop, Dinu Iuliu Dumitrascu, Vlad Dumitru Brata, Traian Adrian Duse, Victor Incze, and Teodora Surdea-Blaga. 2023. "Herbal Remedies for Constipation-Predominant Irritable Bowel Syndrome: A Systematic Review of Randomized Controlled Trials" Nutrients 15, no. 19: 4216. https://doi.org/10.3390/nu15194216
APA StyleChiarioni, G., Popa, S. L., Ismaiel, A., Pop, C., Dumitrascu, D. I., Brata, V. D., Duse, T. A., Incze, V., & Surdea-Blaga, T. (2023). Herbal Remedies for Constipation-Predominant Irritable Bowel Syndrome: A Systematic Review of Randomized Controlled Trials. Nutrients, 15(19), 4216. https://doi.org/10.3390/nu15194216