


Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) among Clinical vs. Non-Clinical Adolescent Israeli Females


Abstract
:1. Introduction
1.1. Eating Disorders—Past and Present
1.2. Self-Reported Screening Tools for Disordered Eating Behaviors
- A difference would be found between a clinical population and a non-clinical population in the factor structure of the EAT-26.
- The clinical group would show a factor structure that is more like the original EAT-26 (three factors) than the non-clinical group would.
- In accordance with the first hypothesis, a difference would be found between the current EAT-26 cutoff point, reflecting the presence of pathological eating preoccupations and behaviors, and the original cutoff point (20).
2. Materials and Methods
2.1. Participants and Procedure
2.2. The EAT-26 Instrument
2.3. Data Analysis
3. Results
3.1. Assessing Configural Invariance
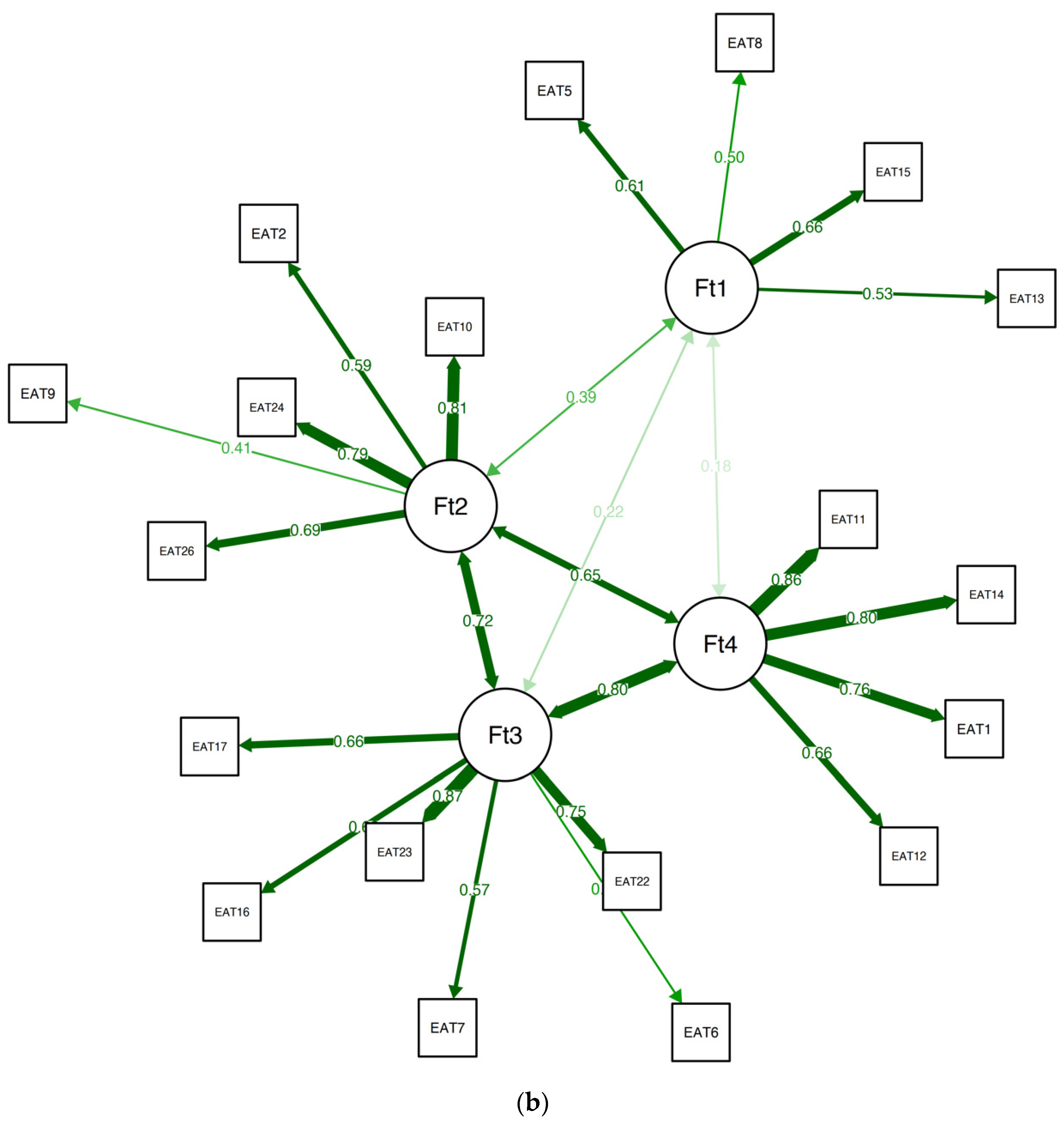
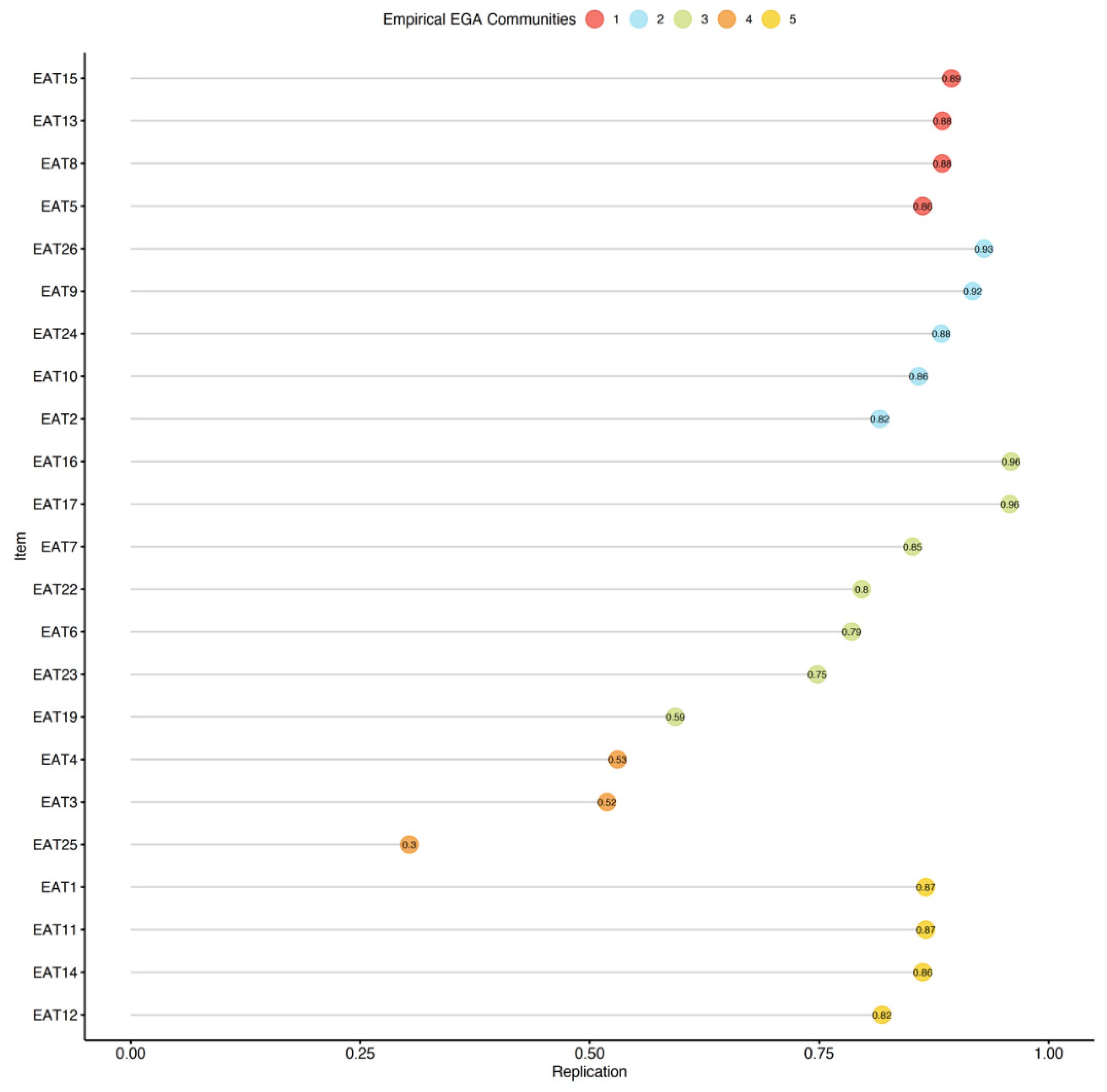
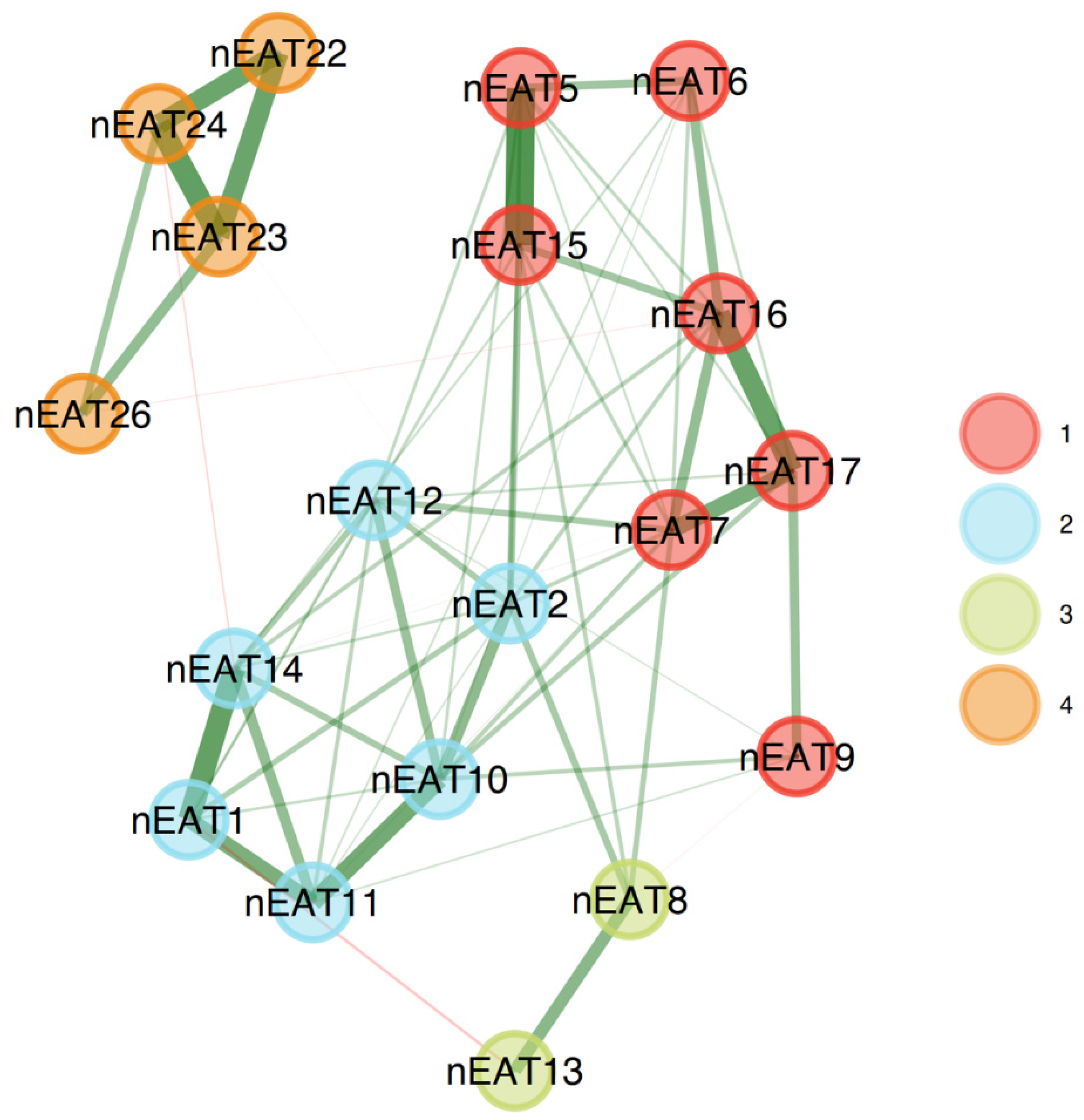
3.2. Exploratory Graph Analysis
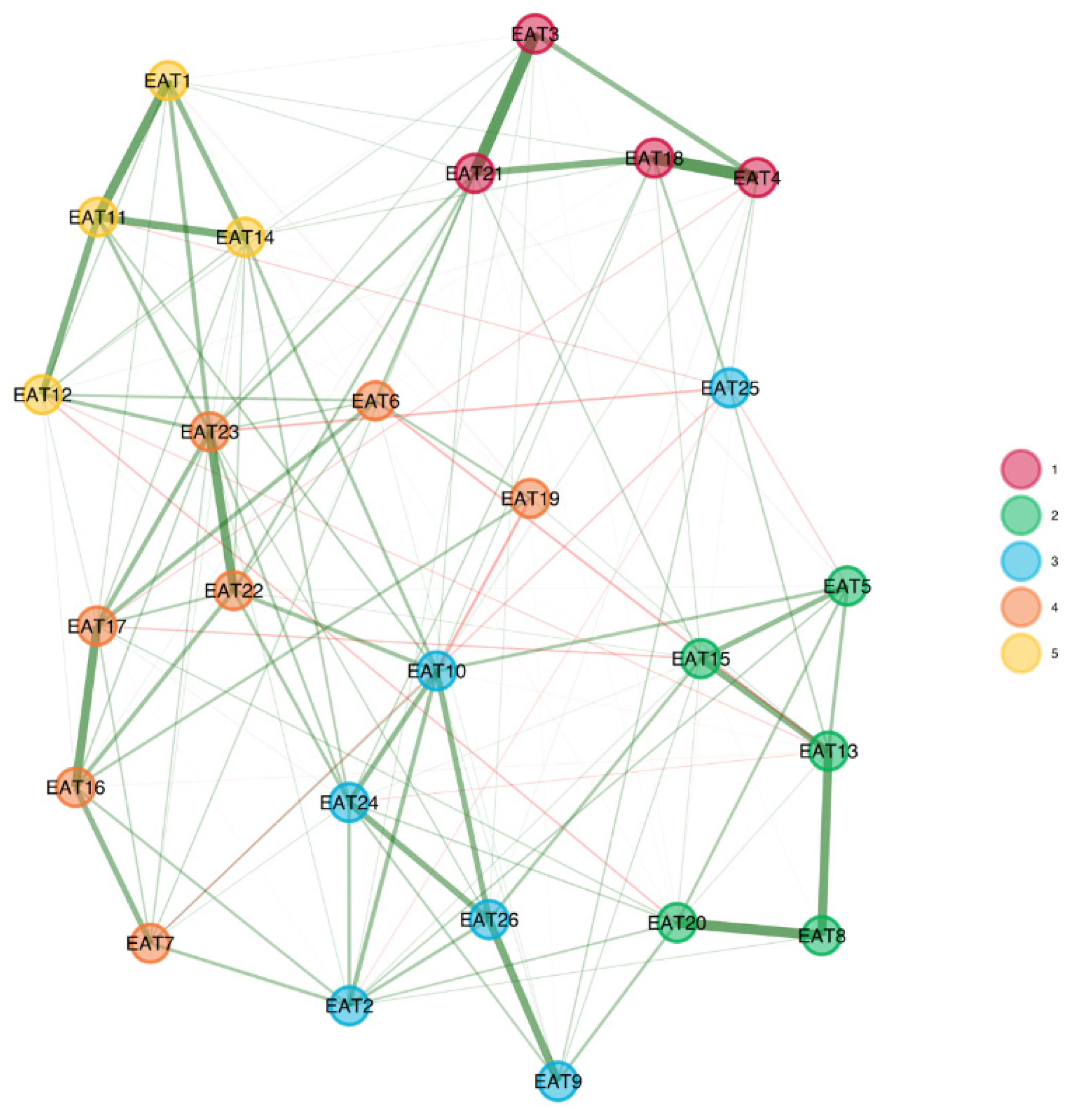
3.3. Clinical Sample
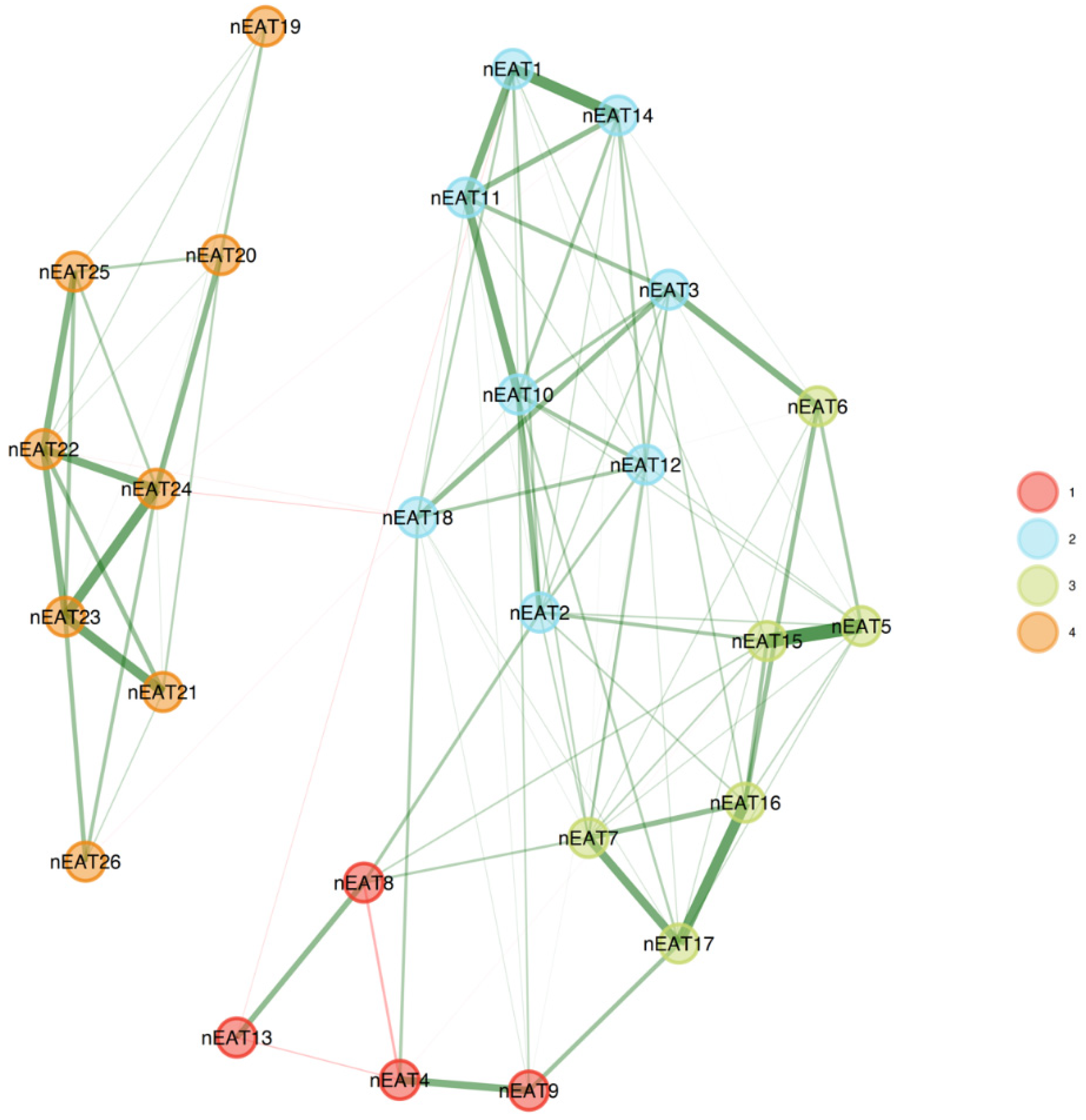
3.4. Non-Clinical Sample
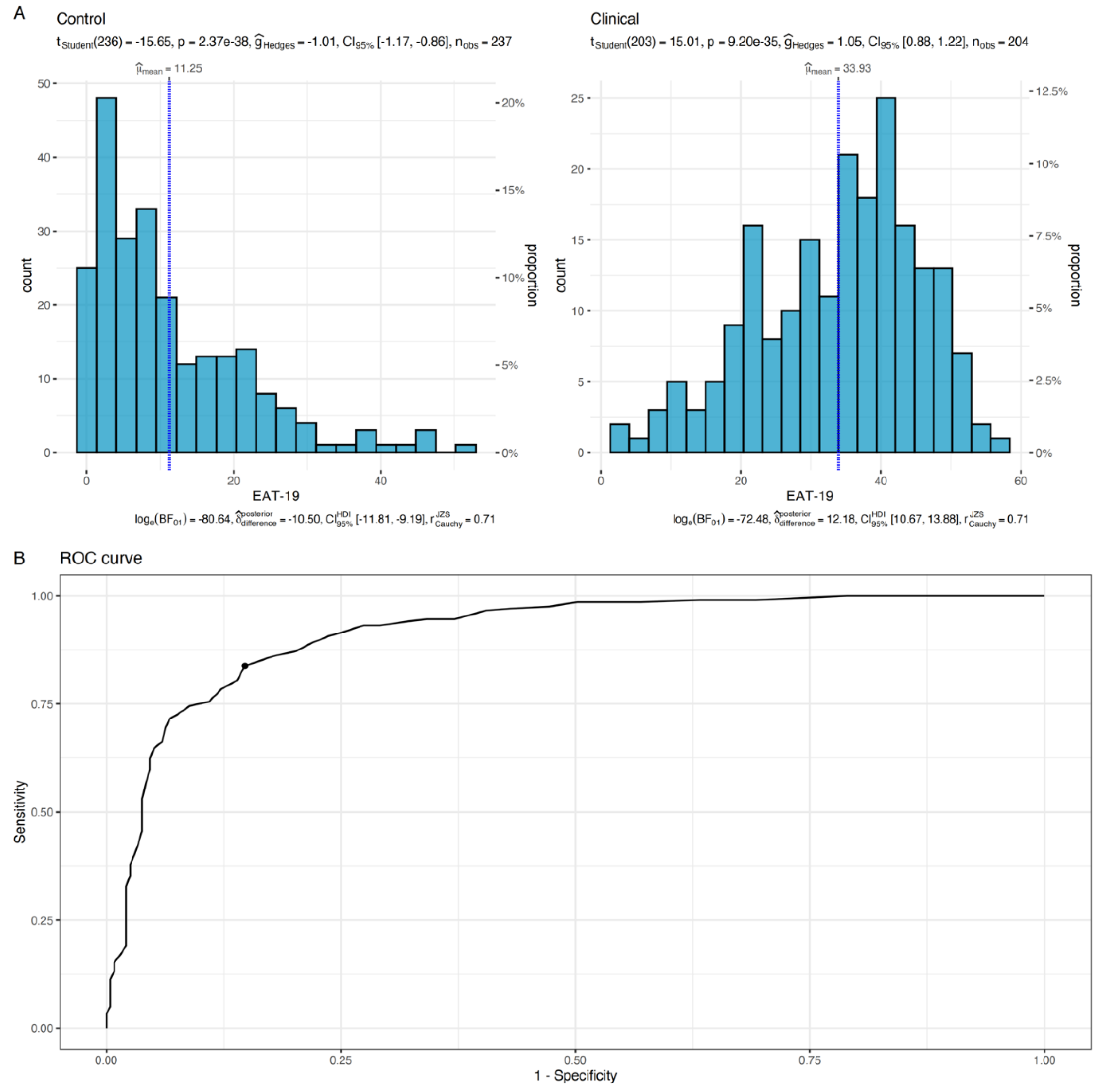
3.5. Effectiveness of Using the EAT-19 as a Diagnostic Test
4. Discussion
4.1. Limitations, Directions for Future Research, and Conclusions
4.1.1. Limitations
4.1.2. Future Research
4.1.3. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bulik, C.; Yilmaz, Z.; HArdaway, A. Genetics and Epigenetics of Eating Disorders. Adv. Genom. Genet. 2015, 5, 131–150. [Google Scholar] [CrossRef] [PubMed]
- Sharan, P.; Sundar, A.S. Eating Disorders in Women. Indian J. Psychiatry 2015, 57, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Katz, B. Gender and Disordered Eating of Adolescents in Israel. Isr. J. Psychiatry Relat. Sci. 2014, 51, 137–144. Available online: https://cdn.doctorsonly.co.il/2014/08/10_Gender-and-Disordered.pdf (accessed on 15 September 2023). [PubMed]
- Latzer, Y.; Spivak-Lavi, Z.; Katz, R. Disordered Eating and Media Exposure among Adolescent Girls: The Role of Parental Involvement and Sense of Empowerment. Int. J. Adolesc. Youth 2015, 20, 375–391. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Lindvall Dahlgren, C.; Wisting, L.; Rø, Ø. Feeding and Eating Disorders in the DSM-5 Era: A Systematic Review of Prevalence Rates in Non-Clinical Male and Female Samples. J. Eat. Disord. 2017, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Udo, T.; Grilo, C.M. Prevalence and Correlates of DSM-5–Defined Eating Disorders in a Nationally Representative Sample of US Adults. Biol. Psychiatry 2018, 84, 345–354. [Google Scholar] [CrossRef]
- Slof-Op ‘t Landt, M.C.T.; van Furth, E.F.; van Beijsterveldt, C.E.M.; Bartels, M.; Willemsen, G.; de Geus, E.J.; Ligthart, L.; Boomsma, D.I. Prevalence of Dieting and Fear of Weight Gain across Ages: A Community Sample from Adolescents to the Elderly. Int. J. Public. Health 2017, 62, 911–919. [Google Scholar] [CrossRef]
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An Update on the Prevalence of Eating Disorders in the General Population: A Systematic Review and Meta-Analysis. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2022, 27, 415–428. [Google Scholar] [CrossRef]
- Andrea, M. The Evolution of Our Understanding and Treatment of Eating Disorders over the Past 50 Years. J. Clin. Psychol. 2019, 75, 1380–1391. [Google Scholar]
- Keel, P.K.; Klump, K.L. Are Eating Disorders Culture-Bound Syndromes? Implications for Conceptualizing Their Etiology. Psychol. Bull. 2003, 129, 747–769. [Google Scholar] [CrossRef]
- Marks, R.J.; De Foe, A.; Collett, J. The Pursuit of Wellness: Social Media, Body Image and Eating Disorders. Child. Youth Serv. Rev. 2020, 119, 105659. [Google Scholar] [CrossRef]
- Hendrickse, J.; Arpan, L.M.; Clayton, R.B.; Ridgway, J.L. Instagram and College Women’s Body Image: Investigating the Roles of Appearance-Related Comparisons and Intrasexual Competition. Comput. Human. Behav. 2017, 74, 92–100. [Google Scholar] [CrossRef]
- Coelho, G.; de Abreu Soares, E.; Innocencio da Silva Gomes, A.; Goncalves Ribeiro, B. Prevention of Eating Disorders in Female Athletes. Open Access J. Sports Med. 2014, 5, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Ocker, L.B.; Lam, E.T.C.; Jensen, B.E.; Zhang, J.J. Psychometric Properties of the Eating Attitudes Test. Meas. Phys. Educ. Exerc. Sci. 2007, 11, 25–48. [Google Scholar] [CrossRef]
- Garner, D.M. EDI-2 Eating Disorder Inventory-2: Professional Manual; Psychological Assessment Resources, Inc.: Odessa, FL, USA, 1991. [Google Scholar]
- Garner, M.D. Eating Disorder Inventory-3. Professional Manual; Psychological Assessment Resources, Inc.: Lutz, FL, USA, 2004. [Google Scholar]
- Beglin, S.; Fairburn, C. Evaluation of a New Instrument for the Detection of Eating Disorders in Community Samples. Psychiatry Res. 1992, 4, 191–201. [Google Scholar] [CrossRef]
- Fairburn, C.; Belgin, S. Assessment of Eating Disorders: Interview or Self-report Questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]
- Farnill, J.; St George’, M.; O’brien, A. The SCOFF Questionnaire and Clinical Interview for Eating Disorders in General Practice: Comparative Study. Br. Med. J. 2002, 325, 755–756. [Google Scholar] [CrossRef]
- Garner, D.; Olmsted, M.; Bohr, Y.; Garfinkel, P. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. Available online: https://www.researchgate.net/profile/David_Garner4/publication/313766446_The_Eating_Attitudes_Test_Psychometric_features_and_clinical_correlates/links/5e595921299bf1bdb8443147/The-Eating-Attitudes-Test-Psychometric-features-and-clinical-correlates.pdf (accessed on 19 September 2023). [CrossRef]
- Garner, D.; Garfinkel, P. Socio-Cultural Factors in the Development of. Anorexia Nervosa. Psychol. Med. 1980, 10, 647–656. [Google Scholar] [CrossRef]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An Index of the Symptoms of Anorexia Nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef]
- Habermas, T. History of Anorexia Nervosa. In The Wiley Handbook of Eating Disorders; Levin, M.P., Smolak, L., Eds.; Wiley: New-York, NY, USA, 2015; Volume 1, pp. 1–24. ISBN 9781118573945. [Google Scholar]
- Garfinkel, P.E.; Newman, A. The Eating Attitudes Test: Twenty-Five Years Later. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2001, 6, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Button, E.; Whitehouse, A. Subclinical Anorexia Nervosa. Psychol. Med. 1981, 11, 509–516. [Google Scholar] [CrossRef]
- Gross, J.; Rosen, J.; Leitenberg, H.; Willmuth, M. Validity of the Eating Attitudes Test and the Eating Disorders Inventory in Bulimia Nervosa. J. Consult. Clin. Psychol. 1986, 54, 875. [Google Scholar] [CrossRef]
- Koslowsky, M.; Scheinberg, Z.; Bleich, A.; Mark, M.; Apter, A.; Danon, Y.; Solomon, Z. The Factor Structure and Criterion Validity of the Short Form of the Eating Attitudes Test. J. Pers. Assess. 1992, 58, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Schwartz, D. Life Adjustment of Women with Anorexia Nervosa and Anorexic-like Behavior. Int. J. Eat. Disord. 1982, 1, 47–60. [Google Scholar] [CrossRef]
- Túry, F.; Güleç, H.; Kohls, E. Assessment Methods for Eating Disorders and Body Image Disorders. J. Psychosom. Res. 2010, 69, 601–611. [Google Scholar] [CrossRef]
- Nasser, M. The EAT Speaks Many Languages: Review of the Use of the EAT in Eating Disorders Research. Eat. Weight. Disord. —Stud. Anorex. Bulim. Obes. 1997, 2, 174–181. [Google Scholar] [CrossRef]
- Mukai, T.; Crago, M.; Shisslak, C.M. Eating Attitudes and Weight Preoccupation Among Female High School Students in Japan. J. Child Psychol. Psychiatry 1994, 35, 677–688. [Google Scholar] [CrossRef]
- Dotti, A.; Lazzari, R. Validation and Reliability of the Italian EAT-26. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 1998, 3, 188–194. [Google Scholar] [CrossRef]
- Apter, A.; Shah, M.; Iancu, I.; Abramovitc, H.; Weizman, A.; Tyano, S. Cultural Effects on Eating Attitudes in Israeli Subpopulations and Hospitalized Anorectics. Genet. Soc. Gen. Psychol. Monogr. 1994, 120, 83–99. [Google Scholar]
- Spivak-Lavi, Z.; Peleg, O.; Tzischinsky, O.; Stein, D.; Latzer, Y. Differences in the Factor Structure of the Eating Attitude Test-26 (Eat-26) in Different Cultures in Israel: Jews, Muslims, and Christians. Nutrients 2021, 13, 1899. [Google Scholar] [CrossRef] [PubMed]
- NIH National Institute of Mental Health. 1999. Available online: https://www.nih.gov/ (accessed on 15 September 2023).
- Rogoza, R.; Brytek-Matera, A.; Garner, D.M. Analysis of the EAT-26 in a Non-Clinical Sample. Arch. Psychiatry Psychother. 2016, 2, 54–58. [Google Scholar] [CrossRef]
- Rutt, C.D.; Coleman, K.J. The Evaluation of a Measurement Model for the Body Image Questionnaire and the Eating Attitudes Test in a Hispanic Population. Hisp. J. Behav. Sci. 2001, 23, 153–170. [Google Scholar] [CrossRef]
- Golino, H.; Shi, D.; Christensen, A.P.; Garrido, L.E.; Nieto, M.D.; Sadana, R.; Thiyagarajan, J.A.; Martinez-Molina, A. Investigating the Performance of Exploratory Graph Analysis and Traditional Techniques to Identify the Number of Latent Factors: A Simulation and Tutorial. Psychol. Methods 2020, 25, 292. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse Inverse Covariance Estimation with the Graphical Lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef]
- Preprint, P.; Christensen, A.P.; Garrido, L.E.; Golino, H. Unique Variable Analysis: A Novel Approach for Detecting Redundant Variables in Multivariate Data. PsyArXiv 2020, 10. [Google Scholar] [CrossRef]
- Ruscio, J.; Roche, B. Determining the Number of Factors to Retain in an Exploratory Factor Analysis Using Comparison Data of Known Factorial Structure. Psychol. Assess. 2012, 24, 282–292. [Google Scholar] [CrossRef]
- Linn, S.; Grunau, P.D. New Patient-Oriented Summary Measure of Net Total Gain in Certainty for Dichotomous Diagnostic Tests. Epidemiol. Perspect. Innov. 2006, 3, 11. [Google Scholar] [CrossRef]
- Citrome, L.; Ketter, T.A. When Does a Difference Make a Difference? Interpretation of Number Needed to Treat, Number Needed to Harm, and Likelihood to Be Helped or Harmed. Int. J. Clin. Pract. 2013, 67, 407–411. [Google Scholar] [CrossRef]
- Bali, G.; Kokka, I.; Gonidakis, F.; Papakonstantinou, E.; Vlachakis, D.; Chrousos, G.P.; Kanaka-Gantenbein, C.; Bacopoulou, F. Validation of the Eating Habits Questionnaire in Greek Adults. EMBnet J. 2023, 28, e1029. [Google Scholar] [CrossRef]
- McEnery, F.; Fitzgerald, A.; McNicholas, F.; Dooley, B. Fit for Purpose, Psychometric Assessment of the Eating Attitudes Test-26 in an Irish Adolescent Sample. Eat. Behav. 2016, 23, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Serra, R.; Di Nicolantonio, C.; Di Febo, R.; De Crescenzo, F.; Vanderlinden, J.; Vrieze, E.; Bruffaerts, R.; Loriedo, C.; Pasquini, M.; Tarsitani, L. The Transition from Restrictive Anorexia Nervosa to Binging and Purging: A Systematic Review and Meta-Analysis. Eat. Weight. Disord. 2022, 27, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Kiss-Leizer, M.; Tóth-Király, I.; Rigó, A. How the Obsession to Eat Healthy Food Meets with the Willingness to Do Sports: The Motivational Background of Orthorexia Nervosa. Bulim. Obes. 2019, 24, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Aparicio-Martinez, P.; Perea-Moreno, A.-J.; Pilar Martinez-Jimenez, M.; Dolores Redel-Macías, M.; Pagliari, C.; Vaquero-Abellan, M. Social Media, Thin-Ideal, Body Dissatisfaction and Disordered Eating Attitudes: An Exploratory Analysis. Int. J. Environ. Res. Public Health Artic. 2019, 16, 4177. [Google Scholar] [CrossRef] [PubMed]
- Schuck, K.; Munsch, S.; Schneider, S. Body Image Perceptions and Symptoms of Disturbed Eating Behavior among Children and Adolescents in Germany. Child. Adolesc. Psychiatry Ment. Health 2018, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Chao, A.M.; Wadden, T.A.; Walsh, O.A.; Gruber, K.A.; Alamuddin, N.; Berkowitz, R.I.; Tronieri, J.S. Effects of Liraglutide and Behavioral Weight Loss on Food Cravings, Eating Behaviors, and Eating Disorder Psychopathology. Obesity 2019, 27, 2005–2010. [Google Scholar] [CrossRef]
- Weiss, A.L.; Miller, J.N.; Chermak, R. Adolescent Diet Culture: Where Does It Originate? In Fad Diets and Adolescents: A Guide for Clinicians, Educators, Coaches and Trainers; Springer International Publishing: Cham, Switzerland, 2022; pp. 17–24. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (N = 207) | Control Group (N = 155) | p | |
|---|---|---|---|
| Age in years (range) | 16.1 ± 1.3 (12.3–19.0) | 16.1 ± 1.6 (12–18) | 0.99 |
| BMI (range) | 17.85 ± 3.46 (10.70–33.60) | 21.07 ± 1.61 (14.53–31.64) | <0.001 |
| BMI < 15 | 35 (16.9) | 3 (1.9) | <0.001 |
| BMI > 25 | 9 (4.4) | 31 (19.9) | <0.001 |
| Diagnosis (n/p) | 94 (45.4) | N/A | |
| AN | 45 (21.7) | ||
| AN—binge/purge BN | 33 (15.95) | ||
| Atypical EDs | 22 (10.6) | ||
| Co-morbidity (n/p) | |||
| Depression | 39 (18.8) | ||
| ADHD | 25 (12.1) | ||
| Anxiety | 10 (4.8) | ||
| OCD | 9 (4.3) | ||
| PTSD | 7 (3.4) | ||
| Dysthymia | 4 (1.9) | ||
| Social phobia | 3 (1.4) | ||
| Panic disorder | 3 (1.4) | ||
| Alcohol abuse | 2 (1.0) | ||
| Bipolar disorder | 2 (1.0) | ||
| Other | 8 (3.9) |
| (a) | |||||
|---|---|---|---|---|---|
| Weight Preoccupation | Binge/Purge Behaviors and Concerns of Others | Dieting and Restricting Symptoms | Eating-Related Concerns | ||
| nEAT11 | 0.35 | ||||
| nEAT10 | 0.33 | ||||
| nEAT1 | 0.32 | ||||
| nEAT14 | 0.30 | ||||
| nEAT12 | 0.22 | ||||
| nEAT3 | 0.22 | ||||
| nEAT2 | 0.18 | ||||
| nEAT18 | 0.16 | ||||
| nEAT8 | 0.20 | ||||
| nEAT9 | 0.18 | ||||
| nEAT13 | 0.17 | ||||
| nEAT4 | −0.28 | ||||
| nEAT16 | 0.37 | ||||
| nEAT5 | 0.31 | ||||
| nEAT17 | 0.30 | ||||
| nEAT15 | 0.28 | ||||
| nEAT7 | 0.26 | ||||
| nEAT6 | 0.15 | ||||
| nEAT23 | 0.48 | ||||
| nEAT24 | 0.44 | ||||
| nEAT22 | 0.40 | ||||
| nEAT21 | 0.26 | ||||
| nEAT25 | 0.25 | ||||
| nEAT20 | 0.22 | ||||
| nEAT26 | 0.14 | ||||
| nEAT19 | 0.09 | ||||
| (b) | |||||
| Weight Concerns | Eating-Related Concerns | Food Controls One’s Life | One’s Own and Others’ Control over the Person’s Eating | Dieting | |
| EAT11 | 0.42 | ||||
| EAT1 | 0.29 | ||||
| EAT14 | 0.26 | ||||
| EAT12 | 0.19 | ||||
| EAT26 | 0.33 | ||||
| EAT24 | 0.25 | ||||
| EAT10 | 0.23 | ||||
| EAT2 | 0.17 | ||||
| EAT9 | 0.16 | ||||
| EAT25 | |||||
| EAT18 | 0.33 | ||||
| EAT21 | 0.32 | ||||
| EAT4 | 0.30 | ||||
| EAT3 | 0.29 | ||||
| EAT13 | 0.33 | ||||
| EAT8 | 0.32 | ||||
| EAT20 | 0.25 | ||||
| EAT15 | 0.22 | ||||
| EAT5 | 0.20 | ||||
| EAT16 | 0.31 | ||||
| EAT17 | 0.29 | ||||
| EAT23 | 0.22 | 0.25 | |||
| EAT22 | 0.23 | ||||
| EAT6 | 0.15 | ||||
| EAT7 | -- | ||||
| EAT19 | -- | ||||
| Fat Concerns | Eating-Related Concerns |
One’s Own and Others’
Control over the Person’s Eating | Dieting | |
|---|---|---|---|---|
| EAT11 | 0.42 | |||
| EAT1 | 0.30 | |||
| EAT14 | 0.27 | |||
| EAT12 | 0.19 | |||
| EAT26 | 0.37 | |||
| EAT24 | 0.28 | |||
| EAT10 | 0.27 | |||
| EAT9 | 0.18 | |||
| EAT2 | 0.18 | |||
| EAT13 | 0.40 | |||
| EAT15 | 0.27 | |||
| EAT8 | 0.23 | |||
| EAT5 | 0.19 | |||
| EAT17 | 0.32 | |||
| EAT23 | 0.25 | 0.30 | ||
| EAT16 | 0.30 | |||
| EAT22 | 0.27 | |||
| EAT7 | 0.15 | |||
| EAT6 | 0.15 |
| Restrictive Weight Concerns | Dieting | Concerns of Others over One’s Eating | Eating-Related Concerns | |
|---|---|---|---|---|
| nEAT11 | 0.36 | |||
| nEAT14 | 0.35 | |||
| nEAT1 | 0.35 | |||
| nEAT10 | 0.34 | |||
| nEAT2 | 0.20 | |||
| nEAT12 | 0.20 | |||
| nEAT17 | 0.37 | |||
| nEAT16 | 0.37 | |||
| nEAT5 | 0.32 | |||
| nEAT15 | 0.28 | |||
| nEAT7 | 0.26 | |||
| nEAT6 | 0.17 | |||
| nEAT9 | 0.07 | |||
| nEAT8 | 0.24 | |||
| nEAT13 | 0.24 | |||
| nEAT23 | 0.54 | |||
| nEAT24 | 0.51 | |||
| nEAT22 | 0.40 | |||
| nEAT26 | 0.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spivak-Lavi, Z.; Latzer, Y.; Stein, D.; Peleg, O.; Tzischinsky, O. Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) among Clinical vs. Non-Clinical Adolescent Israeli Females. Nutrients 2023, 15, 4168. https://doi.org/10.3390/nu15194168
Spivak-Lavi Z, Latzer Y, Stein D, Peleg O, Tzischinsky O. Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) among Clinical vs. Non-Clinical Adolescent Israeli Females. Nutrients. 2023; 15(19):4168. https://doi.org/10.3390/nu15194168
Chicago/Turabian StyleSpivak-Lavi, Zohar, Yael Latzer, Daniel Stein, Ora Peleg, and Orna Tzischinsky. 2023. "Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) among Clinical vs. Non-Clinical Adolescent Israeli Females" Nutrients 15, no. 19: 4168. https://doi.org/10.3390/nu15194168
APA StyleSpivak-Lavi, Z., Latzer, Y., Stein, D., Peleg, O., & Tzischinsky, O. (2023). Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) among Clinical vs. Non-Clinical Adolescent Israeli Females. Nutrients, 15(19), 4168. https://doi.org/10.3390/nu15194168