

Association of Dietary Flavonoid Intake with Serum Cotinine Levels in the General Adult Population

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Dietary Flavonoid Intake Measurement
2.3. Serum Cotinine Levels Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of Participants
3.2. Distribution and Concentration of Dietary Flavonoid Intake
3.3. The Associations of Dietary Flavonoid Intake with Serum Cotinine Levels
3.4. Subgroup Analysis
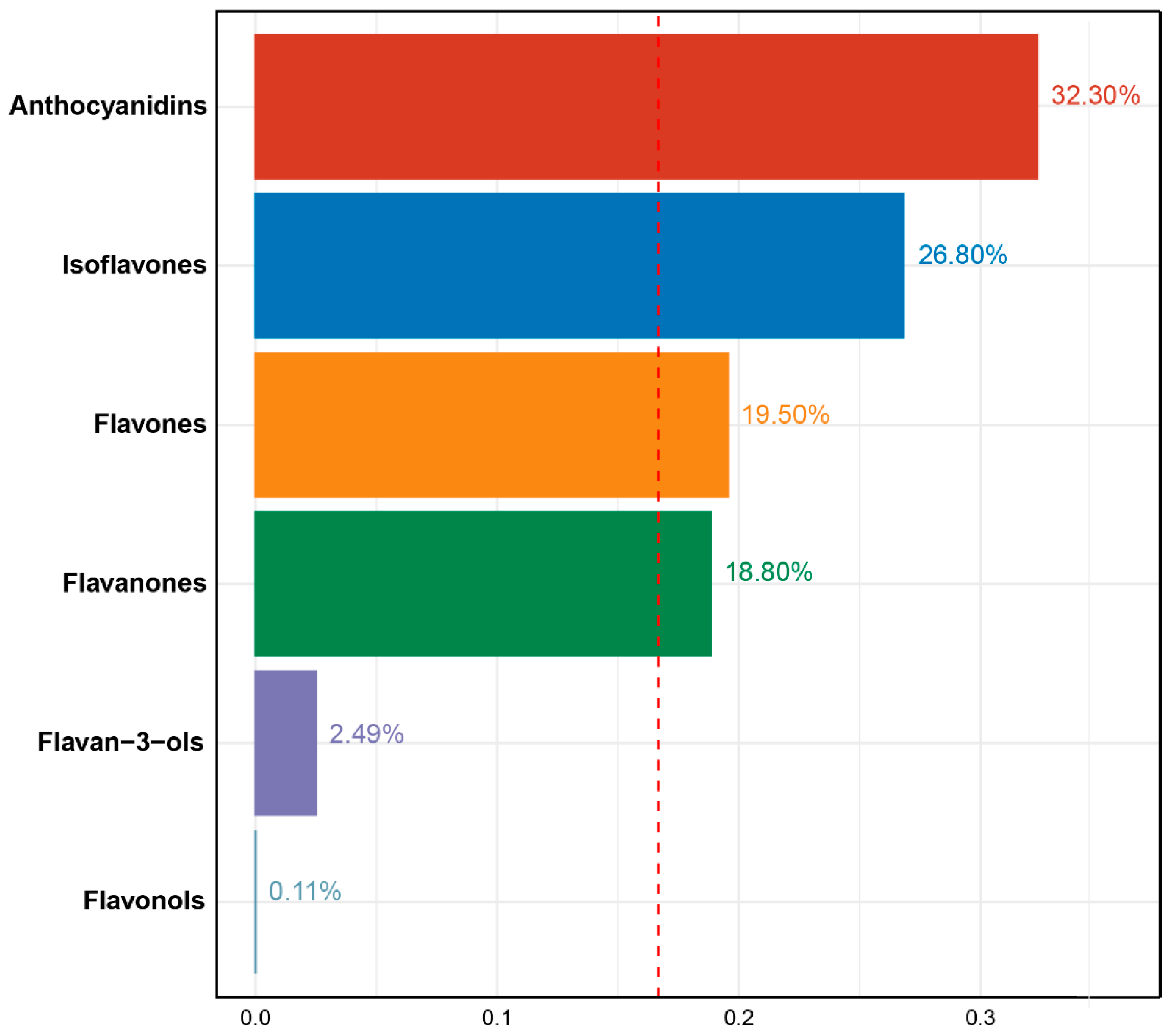
3.5. The Associations between the Mixture of Six Dietary Flavonoid Intake and the Serum Cotinine Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, M.; Eun, J.B. Flavonoids in fruits and vegetables after thermal and nonthermal processing: A review. Crit. Rev. Food Sci. Nutr. 2018, 58, 3159–3188. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Fan, Z.; Yang, Z.; Huang, T.; Tong, Y.; Yang, D.; Mao, X.; Yang, M. Flavonoids-Natural Gifts to Promote Health and Longevity. Int. J. Mol. Sci. 2022, 23, 2176. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Samtiya, M.; Dhewa, T.; Mishra, V.; Aluko, R.E. Health benefits of polyphenols: A concise review. J. Food Biochem. 2022, 46, e14264. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.S. Regulatory Roles of Flavonoids on Inflammasome Activation during Inflammatory Responses. Mol. Nutr. Food Res. 2018, 62, e1800147. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L. Cotinine as a Biomarker of Environmental Tobacco Smoke Exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef]
- List, W.; Singer, C.; Schwab, C.; Riedl, R.; Plhak, E.M.; Weger, M.; Haas, A.; Wedrich, A.; Seidel, G. Cotinine and cytokine levels in the vitreous body and blood serum of smokers and non-smokers—A pilot study. Exp. Eye Res. 2021, 212, 108773. [Google Scholar] [CrossRef]
- Grizzell, J.A.; Echeverria, V. New Insights into the Mechanisms of Action of Cotinine and its Distinctive Effects from Nicotine. Neurochem. Res. 2015, 40, 2032–2046. [Google Scholar] [CrossRef]
- Buccafusco, J.J.; Terry, A.V. The potential role of cotinine in the cognitive and neuroprotective actions of nicotine. Life Sci. 2003, 72, 2931–2942. [Google Scholar] [CrossRef]
- Jian, T.; Chen, J.; Ding, X.; Lv, H.; Li, J.; Wu, Y.; Ren, B.; Tong, B.; Zuo, Y.; Su, K.; et al. Flavonoids isolated from loquat (Eriobotrya japonica) leaves inhibit oxidative stress and inflammation induced by cigarette smoke in COPD mice: The role of TRPV1 signaling pathways. Food Funct. 2020, 11, 3516–3526. [Google Scholar] [CrossRef]
- Bondonno, N.P.; Parmenter, B.H.; Dalgaard, F.; Murray, K.; Rasmussen, D.B.; Kyrø, C.; Cassidy, A.; Bondonno, C.P.; Lewis, J.R.; Croft, K.D.; et al. Flavonoid intakes inversely associate with COPD in smokers. Eur. Respir. J. 2022, 60, 2102604. [Google Scholar] [CrossRef]
- Zhao, Z.; Gao, W.; Ding, X.; Xu, X.; Xiao, C.; Mao, G.; Xing, W. The association between dietary intake of flavonoids and its subclasses and the risk of metabolic syndrome. Front. Nutr. 2023, 10, 1195107. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, H.; Urquiza-Martínez, M.V.; Manhães-de-Castro, R.; Costa-de-Santana, B.J.R.; Villarreal, J.P.; Mercado-Camargo, R.; Torner, L.; de Souza Aquino, J.; Toscano, A.E.; Guzmán-Quevedo, O. Effects of the Treatment with Flavonoids on Metabolic Syndrome Components in Humans: A Systematic Review Focusing on Mechanisms of Action. Int. J. Mol. Sci. 2022, 23, 8344. [Google Scholar] [CrossRef] [PubMed]
- Micek, A.; Godos, J.; Del Rio, D.; Galvano, F.; Grosso, G. Dietary Flavonoids and Cardiovascular Disease: A Comprehensive Dose-Response Meta-Analysis. Mol. Nutr. Food Res. 2021, 65, e2001019. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Tu, Y.; Lao, S.; Wu, M.; Yin, H.; Wang, L.; Liao, W. The role and mechanism of citrus flavonoids in cardiovascular diseases prevention and treatment. Crit. Rev. Food Sci. Nutr. 2022, 62, 7591–7614. [Google Scholar] [CrossRef] [PubMed]
- Somerville, V.S.; Braakhuis, A.J.; Hopkins, W.G. Effect of Flavonoids on Upper Respiratory Tract Infections and Immune Function: A Systematic Review and Meta-Analysis. Adv. Nutr. 2016, 7, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Zanoaga, O.; Braicu, C.; Jurj, A.; Rusu, A.; Buiga, R.; Berindan-Neagoe, I. Progress in Research on the Role of Flavonoids in Lung Cancer. Int. J. Mol. Sci. 2019, 20, 4291. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, D.; Rajora, A.K.; Greco, F.; Osborn, H.M. Flavonoids as prospective compounds for anti-cancer therapy. Int. J. Biochem. Cell Biol. 2013, 45, 2821–2831. [Google Scholar] [CrossRef]
- Yang, N.; Jia, X.B.; Zhang, Z.H.; Sun, E.; Yan, H.M. Advance in studies on anti-cancer activity and mechanism of flavonoids. Zhongguo Zhong Yao Za Zhi (China J. Chin. Mater. Medica) 2015, 40, 373–381. [Google Scholar]
- Spagnuolo, C.; Moccia, S.; Russo, G.L. Anti-inflammatory effects of flavonoids in neurodegenerative disorders. Eur. J. Med. Chem. 2018, 153, 105–115. [Google Scholar] [CrossRef]
- Mhalhel, K.; Sicari, M.; Pansera, L.; Chen, J.; Levanti, M.; Diotel, N.; Rastegar, S.; Germanà, A.; Montalbano, G. Zebrafish: A Model Deciphering the Impact of Flavonoids on Neurodegenerative Disorders. Cells 2023, 12, 252. [Google Scholar] [CrossRef]
- Pandey, P.; Khan, F.; Seifeldin, S.A.; Alshaghdali, K.; Siddiqui, S.; Abdelwadoud, M.E.; Vyas, M.; Saeed, M.; Mazumder, A.; Saeed, A. Targeting Wnt/β-Catenin Pathway by Flavonoids: Implication for Cancer Therapeutics. Nutrients 2023, 15, 2088. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, R.S.; Wilkinson Enns, C.; Goldman, J.D.; Martin, C.L.; Steinfeldt, L.C.; Murayi, T.; Moshfegh, A.J. A New Database Facilitates Characterization of Flavonoid Intake, Sources, and Positive Associations with Diet Quality among US Adults. J. Nutr. 2015, 145, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Hukkanen, J.; Jacob, P., 3rd; Benowitz, N.L. Metabolism and disposition kinetics of nicotine. Pharmacol. Rev. 2005, 57, 79–115. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Z.; Chen, X.; Geng, T.; Wan, Z.; Lu, Q.; Li, L.; Zhu, K.; Zhang, X.; Liu, Y.; Lin, X.; et al. Associations of Serum Carotenoids With Risk of Cardiovascular Mortality Among Individuals With Type 2 Diabetes: Results from NHANES. Diabetes Care 2022, 45, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.-H.; Cui, Y.; Zhou, H.-l.; Song, W.-j.; Di, D.-S.; Zhang, R.-Y.; Huang, Q.; Liu, J.-A.; Wang, Q. Associations of multiple metals with bone mineral density: A population-based study in US adults. Chemosphere 2021, 282, 131150. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.L.; Fan, M.X.; Wu, J.L.; Li, N.; Guo, M.Q. Antioxidant and anti-inflammatory properties of flavonoids from lotus plumule. Food Chem. 2019, 277, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, X.J.; Chen, J.B.; Cao, J.P.; Li, X.; Sun, C.D. Citrus flavonoids and their antioxidant evaluation. Crit. Rev. Food Sci. Nutr. 2022, 62, 3833–3854. [Google Scholar] [CrossRef]
- Maleki, S.J.; Crespo, J.F.; Cabanillas, B. Anti-inflammatory effects of flavonoids. Food Chem. 2019, 299, 125124. [Google Scholar] [CrossRef]
- Murota, K.; Nakamura, Y.; Uehara, M. Flavonoid metabolism: The interaction of metabolites and gut microbiota. Biosci. Biotech. Bioch. 2018, 82, 600–610. [Google Scholar] [CrossRef]
- Berley, J.; Yamano, S.; Sukotjo, C. The effect of systemic nicotine on osseointegration of titanium implants in the rat femur. J. Oral. Implantol. 2010, 36, 185–193. [Google Scholar] [CrossRef]
- Hasan, F.; Khachatryan, L.; Lomnicki, S. Comparative Studies of Environmentally Persistent Free Radicals on Total Particulate Matter Collected from Electronic and Tobacco Cigarettes. Environ. Sci. Technol. 2020, 54, 5710–5718. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Jing, Z.; Shen, D.; Yang, M.; Liu, K.; Xiang, K.; Zhou, C.; Gong, X.; Deng, Y.; Li, Y.; et al. Quercetin promotes autophagy to alleviate cigarette smoke-related periodontitis. J. Periodontal. Res. 2023, 58, 1082–1095. [Google Scholar] [CrossRef] [PubMed]
- Ding, K.; Jiang, W.; Zhan, W.; Xiong, C.; Chen, J.; Wang, Y.; Jia, H.; Lei, M. The therapeutic potential of quercetin for cigarette smoking-induced chronic obstructive pulmonary disease: A narrative review. Ther. Adv. Respir. Dis. 2023, 17, 17534666231170800. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, P.A.; Barnes, P.J. Oxidative stress in COPD. Chest 2013, 144, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Bowler, R.P.; Barnes, P.J.; Crapo, J.D. The role of oxidative stress in chronic obstructive pulmonary disease. Copd 2004, 1, 255–277. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.C.; Tsai, T.Y.; Wang, C.J. The Potential Benefits of Quercetin for Brain Health: A Review of Anti-Inflammatory and Neuroprotective Mechanisms. Int. J. Mol. Sci. 2023, 24, 6328. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhao, T.; Liu, Z.; Danzengquzhen; Cisangzhuoma; Ma, J.; Li, X.; Huang, X.; Li, B. The neuromodulatory effects of flavonoids and gut Microbiota through the gut-brain axis. Front. Cell. Infect. Microbiol. 2023, 13, 1197646. [Google Scholar] [CrossRef]
- Ciumărnean, L.; Milaciu, M.V.; Runcan, O.; Vesa, Ș.C.; Răchișan, A.L.; Negrean, V.; Perné, M.G.; Donca, V.I.; Alexescu, T.G.; Para, I.; et al. The Effects of Flavonoids in Cardiovascular Diseases. Molecules 2020, 25, 4320. [Google Scholar] [CrossRef]
- Vogel, R.A. Alcohol, heart disease, and mortality: A review. Rev. Cardiovasc. Med. 2002, 3, 7–13. [Google Scholar]
- Selvakumar, P.; Badgeley, A.; Murphy, P.; Anwar, H.; Sharma, U.; Lawrence, K.; Lakshmikuttyamma, A. Flavonoids and Other Polyphenols Act as Epigenetic Modifiers in Breast Cancer. Nutrients 2020, 12, 761. [Google Scholar] [CrossRef]
- Zhou, Y.; Gu, K.; Zhou, F. Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study. Nutrients 2023, 15, 976. [Google Scholar] [CrossRef]
- Shirakami, Y.; Shimizu, M. Possible Mechanisms of Green Tea and Its Constituents against Cancer. Molecules 2018, 23, 2284. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.F.; Ruan, Y.; Li, Z.H.; Li, D. Flavonoid subclasses and type 2 diabetes mellitus risk: A meta-analysis of prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2019, 59, 2850–2862. [Google Scholar] [CrossRef]
- Al-Ishaq, R.K.; Abotaleb, M.; Kubatka, P.; Kajo, K.; Büsselberg, D. Flavonoids and Their Anti-Diabetic Effects: Cellular Mechanisms and Effects to Improve Blood Sugar Levels. Biomolecules 2019, 9, 430. [Google Scholar] [CrossRef] [PubMed]
- van der Vaart, H.; Postma, D.S.; Timens, W.; ten Hacken, N.H. Acute effects of cigarette smoke on inflammation and oxidative stress: A review. Thorax 2004, 59, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Kokkou, E.; Siasos, G.; Georgiopoulos, G.; Oikonomou, E.; Verveniotis, A.; Vavuranakis, M.; Zisimos, K.; Plastiras, A.; Kollia, M.-E.; Stefanadis, C.; et al. The impact of dietary flavonoid supplementation on smoking-induced inflammatory process and fibrinolytic impairment. Atherosclerosis 2016, 251, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Li, X.; Meng, S.; Fung, T.; Chan, A.T.; Liang, G.; Giovannucci, E.; De Vivo, I.; Lee, J.H.; Nan, H. Fruit and vegetable consumption, cigarette smoke, and leukocyte mitochondrial DNA copy number. Am. J. Clin. Nutr. 2019, 109, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Micek, A.; Raźny, U.; Paweł, K. Association between health risk factors and dietary flavonoid intake in cohort studies. Int. J. Food Sci. Nutr. 2021, 72, 1019–1034. [Google Scholar] [CrossRef] [PubMed]
- Pace, E.; Di Vincenzo, S.; Di Salvo, E.; Genovese, S.; Dino, P.; Sangiorgi, C.; Ferraro, M.; Gangemi, S. MiR-21 upregulation increases IL-8 expression and tumorigenesis program in airway epithelial cells exposed to cigarette smoke. J. Cell. Physiol. 2019, 234, 22183–22194. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Qin, L.; Ding, X.; Ma, L.; Wang, Y.; Liu, M.; Chen, H.; Yan, H.; Song, L. The regulatory effect of fermented black barley on the gut microbiota and metabolic dysbiosis in mice exposed to cigarette smoke. Food Res. Int. 2022, 157, 111465. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | Total (n = 15,752) | Serum Cotinine, ng/mL | p Value | |
|---|---|---|---|---|
| <10 ng/mL (n = 8828) | ≥10 ng/mL (n = 6924) | |||
| Age, years | <0.01 | |||
| 20–39 | 4675 (31.25) | 3175 (32.70) | 1500 (45.09) | |
| 40–59 | 4922 (32.9) | 3524 (37.36) | 1398 (39.17) | |
| ≥60 | 5365 (35.86) | 4497 (29.94) | 868 (15.74) | |
| Sex, % | <0.01 | |||
| Female | 7591 (50.74) | 6065 (54.44) | 1526 (40.83) | |
| Male | 7371 (49.26) | 5131 (45.56) | 2240 (59.17) | |
| Race/ethnicity, % | <0.01 | |||
| Mexican American | 2485 (16.61) | 2117 (9.46) | 368 (5.55) | |
| Other Hispanic | 1539 (10.29) | 1277 (5.99) | 262 (4.22) | |
| Non-Hispanic White | 6729 (44.97) | 4834 (67.65) | 1895 (68.95) | |
| Non-Hispanic Black | 2931 (19.59) | 1942 (9.19) | 989 (14.88) | |
| Other race | 1278 (8.54) | 1026 (7.71) | 252 (6.41) | |
| Education level, % | <0.01 | |||
| Below high school | 3952 (26.41) | 2746 (13.98) | 1206 (23.59) | |
| High school | 3554 (23.75) | 2407 (22.22) | 1147 (34.32) | |
| Above high school | 7456 (49.83) | 6043 (63.80) | 1413 (42.09) | |
| Family PIR, % | <0.01 | |||
| ≤1.0 | 3070 (20.52) | 1900 (10.62) | 1170 (23.39) | |
| 1.1–3.0 | 6523 (43.6) | 4849 (34.65) | 1674 (40.34) | |
| >3.0 | 5369 (35.88) | 4447 (54.74) | 922 (36.27) | |
| Smoking status, % | <0.01 | |||
| Never smoker | 8100 (54.14) | 7715 (69.67) | 385 (10.41) | |
| Former smoker | 3754 (25.09) | 3302 (28.73) | 452 (14.38) | |
| Current smoker | 3108 (20.77) | 179 (1.59) | 2929 (75.21) | |
| Drinking status, % | <0.01 | |||
| Nondrinker | 3546 (23.7) | 3034 (21.50) | 512 (12.93) | |
| Low-to-moderate drinker | 10,115 (67.6) | 7446 (71.01) | 2669 (70.49) | |
| Heavy drinker | 1301 (8.7) | 716 (7.49) | 585 (16.58) | |
| Body mass index, % | <0.01 | |||
| <25.0 kg/m2 | 4047 (27.05) | 2758 (27.22) | 1289 (34.66) | |
| 25.0–29.9 kg/m2 | 5024 (33.58) | 3831 (33.24) | 1193 (31.57) | |
| >29.9 kg/m2 | 5891 (39.37) | 4607 (39.54) | 1284 (33.77) | |
| Total energy intake, kcal/day | <0.01 | |||
| Quartile 1 | 3745 (25.03) | 2915 (22.07) | 830 (19.76) | |
| Quartile 2 | 3744 (25.02) | 2924 (25.42) | 820 (20.50) | |
| Quartile 3 | 3736 (24.97) | 2832 (26.62) | 904 (25.18) | |
| Quartile 4 | 3737 (24.98) | 2525 (25.88) | 1212 (34.56) | |
| Supplement use, % | <0.01 | |||
| No | 7477 (49.97) | 5021 (41.70) | 2456 (63.27) | |
| Yes | 7485 (50.03) | 6175 (58.30) | 1310 (36.73) | |
| Flavonoids | Category of Flavonoid Intake, mg/day | ptrend | |||
|---|---|---|---|---|---|
| Group 1 | Group 2 | Group 3 | Group 4 | ||
| Isoflavones | |||||
| Crude | Ref (0.00) | −0.7 (−0.95, −0.44) | −0.83 (−1.13, −0.53) | −1.02 (−1.28, −0.76) | <0.01 |
| Model 1 | Ref (0.00) | −0.45 (−0.68, −0.21) | −0.62 (−0.89, −0.35) | −0.68 (−0.91, −0.44) | <0.01 |
| Model 2 | Ref (0.00) | −0.17 (−0.31, −0.02) | −0.31 (−0.47, −0.14) | −0.37 (−0.51, −0.23) | <0.01 |
| Anthocyanidins | |||||
| Crude | Ref (0.00) | −1.39 (−1.61, −1.17) | −1.75 (−2.03, −1.47) | −2.3 (−2.55, −2.06) | <0.01 |
| Model 1 | Ref (0.00) | −0.89 (−1.14, −0.65) | −1.14 (−1.39, −0.89) | −1.44 (−1.69, −1.20) | <0.01 |
| Model 2 | Ref (0.00) | −0.34 (−0.52, −0.16) | −0.45 (−0.61, −0.29) | −0.55 (−0.69, −0.41) | <0.01 |
| Flavan-3-ols | |||||
| Crude | Ref (0.00) | −0.68 (−0.90, −0.47) | −1.25 (−1.52, −0.98) | −1.09 (−1.36, −0.82) | <0.01 |
| Model 1 | Ref (0.00) | −0.51 (−0.70, −0.31) | −0.92 (−1.17, −0.68) | −0.64 (−0.88, −0.41) | <0.01 |
| Model 2 | Ref (0.00) | −0.24 (−0.42, −0.06) | −0.34 (−0.51, −0.17) | −0.25 (−0.42, −0.08) | 0.01 |
| Flavanones | |||||
| Crude | Ref (0.00) | −1.11 (−1.33, −0.88) | −1.32 (−1.58, −1.06) | −1.65 (−1.92, −1.38) | <0.01 |
| Model 1 | Ref (0.00) | −0.61 (−0.79, −0.42) | −0.74 (−1.00, −0.47) | −1.03 (−1.27, −0.79) | <0.01 |
| Model 2 | Ref (0.00) | −0.29 (−0.43, −0.16) | −0.28 (−0.46, −0.10) | −0.41 (−0.58, −0.25) | <0.01 |
| Flavones | |||||
| Crude | Ref (0.00) | −1.24 (−1.52, −0.97) | −1.46 (−1.75, −1.18) | −1.74 (−2.01, −1.47) | <0.01 |
| Model 1 | Ref (0.00) | −0.87 (−1.12, −0.62) | −0.94 (−1.20, −0.68) | −1.09 (−1.33, −0.84) | <0.01 |
| Model 2 | Ref (0.00) | −0.34 (−0.51, −0.17) | −0.32 (−0.48, −0.17) | −0.42 (−0.58, −0.26) | <0.01 |
| Flavonols | |||||
| Crude | Ref (0.00) | −0.67 (−0.93, −0.42) | −0.63 (−0.90, −0.36) | −0.54 (−0.76, −0.33) | <0.01 |
| Model 1 | Ref (0.00) | −0.45 (−0.68, −0.23) | −0.47 (−0.67, −0.27) | −0.4 (−0.58, −0.21) | <0.01 |
| Model 2 | Ref (0.00) | −0.17 (−0.35, 0.00) | −0.21 (−0.34, −0.07) | −0.14 (−0.27, −0.02) | 0.04 |
| Total flavonoids | |||||
| Crude | Ref (0.00) | −0.98 (−1.24, −0.72) | −1.56 (−1.86, −1.26) | −1.37 (−1.62, −1.12) | <0.01 |
| Model 1 | Ref (0.00) | −0.76 (−1.00, −0.52) | −1.08 (−1.34, −0.81) | −0.87 (−1.08, −0.65) | <0.01 |
| Model 2 | Ref (0.00) | −0.29 (−0.44, −0.14) | −0.41 (−0.58, −0.24) | −0.32 (−0.49, −0.16) | <0.01 |
| Flavonoids | Never Smoker (n = 8100) | Former Smoker (n = 3754) | Current Smoker (n = 3108) |
|---|---|---|---|
| Isoflavones | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.08 (−0.25, 0.09) | −0.42 (−0.83, 0.00) | −0.19 (−0.49, 0.11) |
| Group 3 | −0.30 (−0.50, −0.09) | −0.49 (−0.95, −0.04) | −0.12 (−0.31, 0.07) |
| Group 4 | −0.27 (−0.43, −0.11) | −0.75 (−1.16, −0.33) | −0.32 (−0.53, −0.11) |
| p for trend | <0.01 | <0.01 | <0.01 |
| p for interaction | 0.37 | ||
| Anthocyanidins | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.25 (−0.43, −0.06) | −0.41 (−0.88, 0.05) | −0.33 (−0.53, −0.13) |
| Group 3 | −0.27 (−0.44, −0.10) | −0.73 (−1.16, −0.31) | −0.46 (−0.77, −0.14) |
| Group 4 | −0.38 (−0.53, −0.23) | −0.81 (−1.13, −0.49) | −0.54 (−0.87, −0.22) |
| p for trend | <0.01 | <0.01 | <0.01 |
| p for interaction | 0.02 | ||
| Flavan-3-ols | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.26 (−0.38, −0.13) | −0.12 (−0.80, 0.56) | −0.18 (−0.37, 0.02) |
| Group 3 | −0.24 (−0.41, −0.08) | −0.4 (−0.94, 0.13) | −0.33 (−0.61, −0.04) |
| Group 4 | −0.17 (−0.36, 0.02) | −0.31 (−0.80, 0.19) | −0.25 (−0.52, 0.01) |
| p for trend | 0.2 | 0.11 | 0.03 |
| p for interaction | 0.65 | ||
| Flavanones | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.22 (−0.38, −0.05) | −0.49 (−0.90, −0.08) | −0.19 (−0.36, −0.01) |
| Group 3 | −0.22 (−0.41, −0.04) | −0.20 (−0.77, 0.37) | −0.42 (−0.73, −0.12) |
| Group 4 | −0.34 (−0.48, −0.19) | −0.58 (−1.01, −0.15) | −0.16 (−0.38, 0.07) |
| p for trend | <0.01 | 0.05 | 0.01 |
| p for interaction | 0.17 | ||
| Flavones | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.33 (−0.55, −0.11) | −0.42 (−0.88, 0.04) | −0.33 (−0.59, −0.06) |
| Group 3 | −0.28 (−0.50, −0.06) | −0.46 (−0.84, −0.07) | −0.29 (−0.49, −0.08) |
| Group 4 | −0.32 (−0.49, −0.14) | −0.59 (−1.00, −0.17) | −0.48 (−0.77, −0.20) |
| p for trend | <0.01 | 0.01 | <0.01 |
| p for interaction | 0.38 | ||
| Flavonols | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.19 (−0.32, −0.06) | −0.19 (−0.78, 0.41) | −0.14 (−0.36, 0.09) |
| Group 3 | −0.09 (−0.31, 0.13) | −0.48 (−0.93, −0.03) | −0.13 (−0.34, 0.08) |
| Group 4 | −0.03 (−0.21, 0.15) | −0.15 (−0.58, 0.27) | −0.36 (−0.58, −0.14) |
| p for trend | 0.82 | 0.29 | 0.01 |
| p for interaction | 0.21 | ||
| Total flavonoids | |||
| Group 1 | Ref (0.00) | Ref (0.00) | Ref (0.00) |
| Group 2 | −0.22 (−0.37, −0.06) | −0.43 (−0.90, 0.03) | −0.18 (−0.41, 0.05) |
| Group 3 | −0.28 (−0.46, −0.10) | −0.58 (−1.05, −0.11) | −0.35 (−0.56, −0.13) |
| Group 4 | −0.21 (−0.41, −0.01) | −0.52 (−0.89, −0.14) | −0.31 (−0.52, −0.09) |
| p for trend | 0.07 | 0.01 | <0.01 |
| p for interaction | 0.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, N.; Lin, S.; Yu, H.; Huang, W.; Cao, C. Association of Dietary Flavonoid Intake with Serum Cotinine Levels in the General Adult Population. Nutrients 2023, 15, 4126. https://doi.org/10.3390/nu15194126
Zhu N, Lin S, Yu H, Huang W, Cao C. Association of Dietary Flavonoid Intake with Serum Cotinine Levels in the General Adult Population. Nutrients. 2023; 15(19):4126. https://doi.org/10.3390/nu15194126
Chicago/Turabian StyleZhu, Ning, Shanhong Lin, Hang Yu, Weina Huang, and Chao Cao. 2023. "Association of Dietary Flavonoid Intake with Serum Cotinine Levels in the General Adult Population" Nutrients 15, no. 19: 4126. https://doi.org/10.3390/nu15194126
APA StyleZhu, N., Lin, S., Yu, H., Huang, W., & Cao, C. (2023). Association of Dietary Flavonoid Intake with Serum Cotinine Levels in the General Adult Population. Nutrients, 15(19), 4126. https://doi.org/10.3390/nu15194126