
The Relationship between Depressive Symptoms, Quality of Life and miRNAs 8 Years after Bariatric Surgery

 , , ,
, , ,  , ,
, ,  , ,
, ,
Abstract
: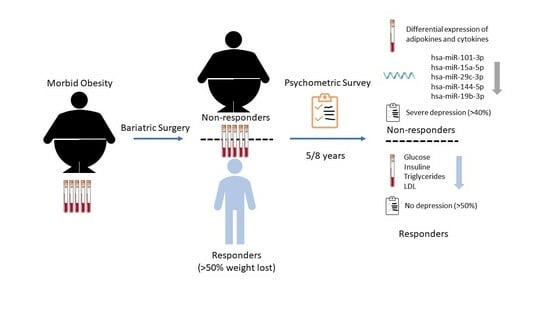
1. Introduction
2. Material and Methods
2.1. Participants
2.2. Psychometric Instruments
- -
- The 36-item Short Form Health Survey (SF-36) [38]. The SF-36 is a valid and self-administered questionnaire that assesses eight dimensions of QoL: (1) Physical functioning (PF; 10 items), (2) Role functioning—Physical (RP; 4 items), (3) Body pain (BP; 2 items), (4) General health perception (GH; 5 items), (5) Vitality (VT; 4 items), (6) Social functioning (SF; 2 items), (7) Role functioning—Emotional (RE; 3 items) and (8) Mental health (MH; 5 items). Each domain is scored from 0 to 100, with greater scores indicating better perceived QoL (physical or mental health conditions). Excellent internal consistency was found in the study sample (Cronbach’s α = 0.96 for the total scale).
- -
- Beck Depression Inventory (BD-II) [39]. This is a 21-item self-reported questionnaire that assesses the severity of depression symptoms. The total score can range from 0 to 63, with higher scores indicative of more severe depression symptoms. The clinical cut-off scores were classified as follows: no depression (0–13), mild depression (14–19), moderate depression (20–28) and severe depression (29 or more). In the current sample, total scores showed an excellent internal consistency (Cronbach’s α = 0.96).
2.3. Biochemical Data
2.4. miRNAs Sequencing
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Quality of Life and Depression at 8-Year Follow-Up after BS
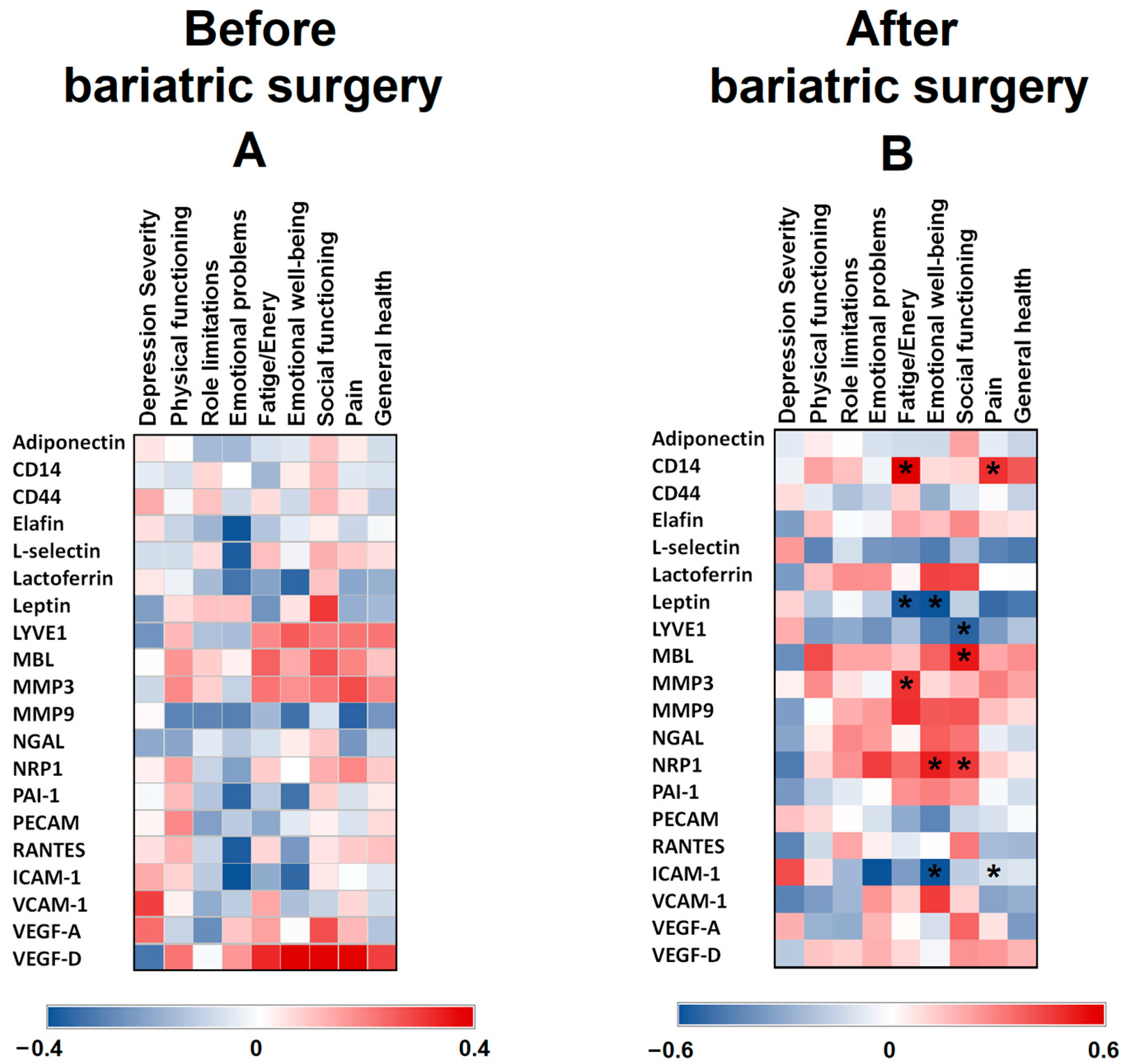
3.3. Association between Serum Protein Levels before and after Surgery vs. Psychological Variables
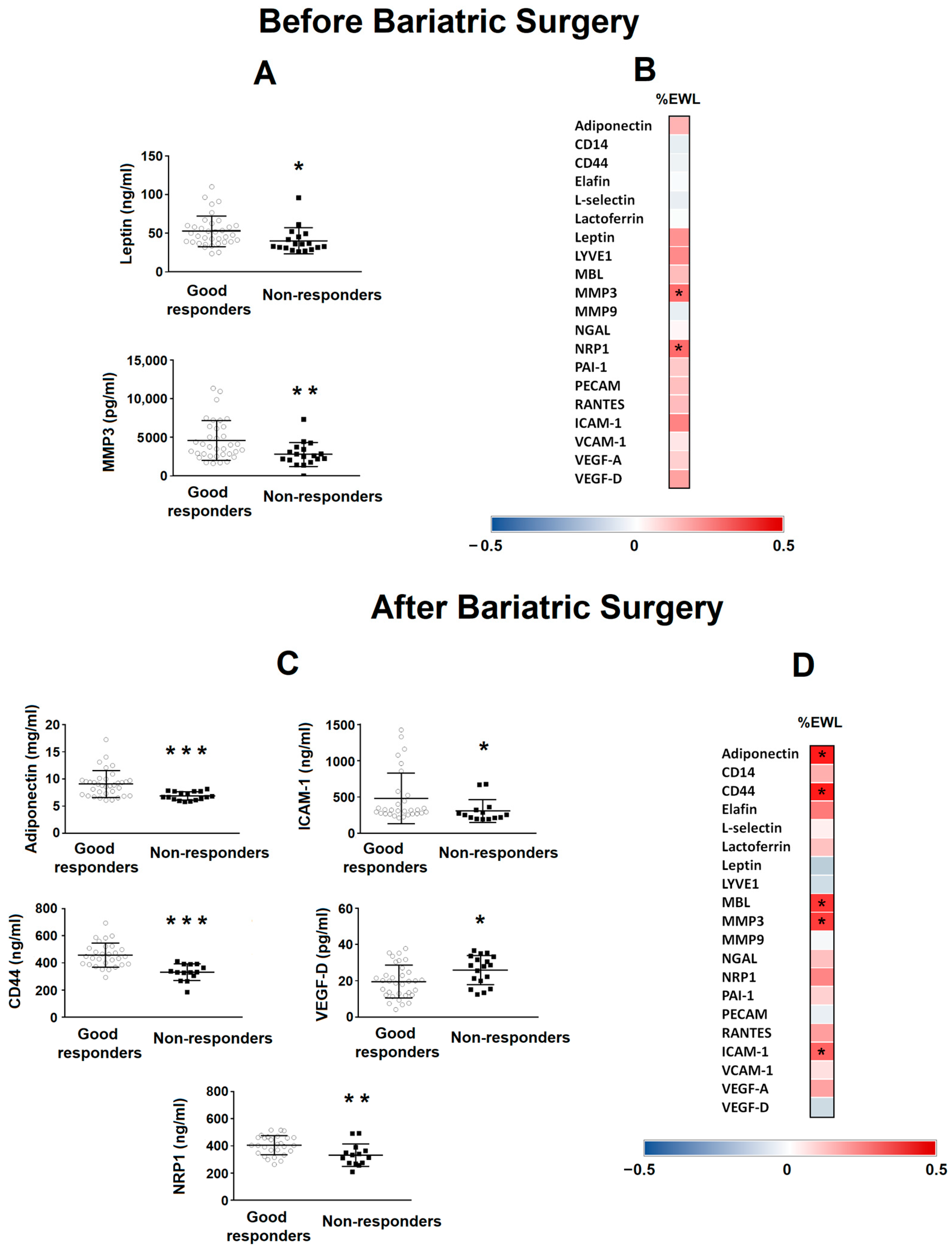
3.4. Association between Serum Protein Levels before and after Surgery vs. Bariatric Surgery Outcome
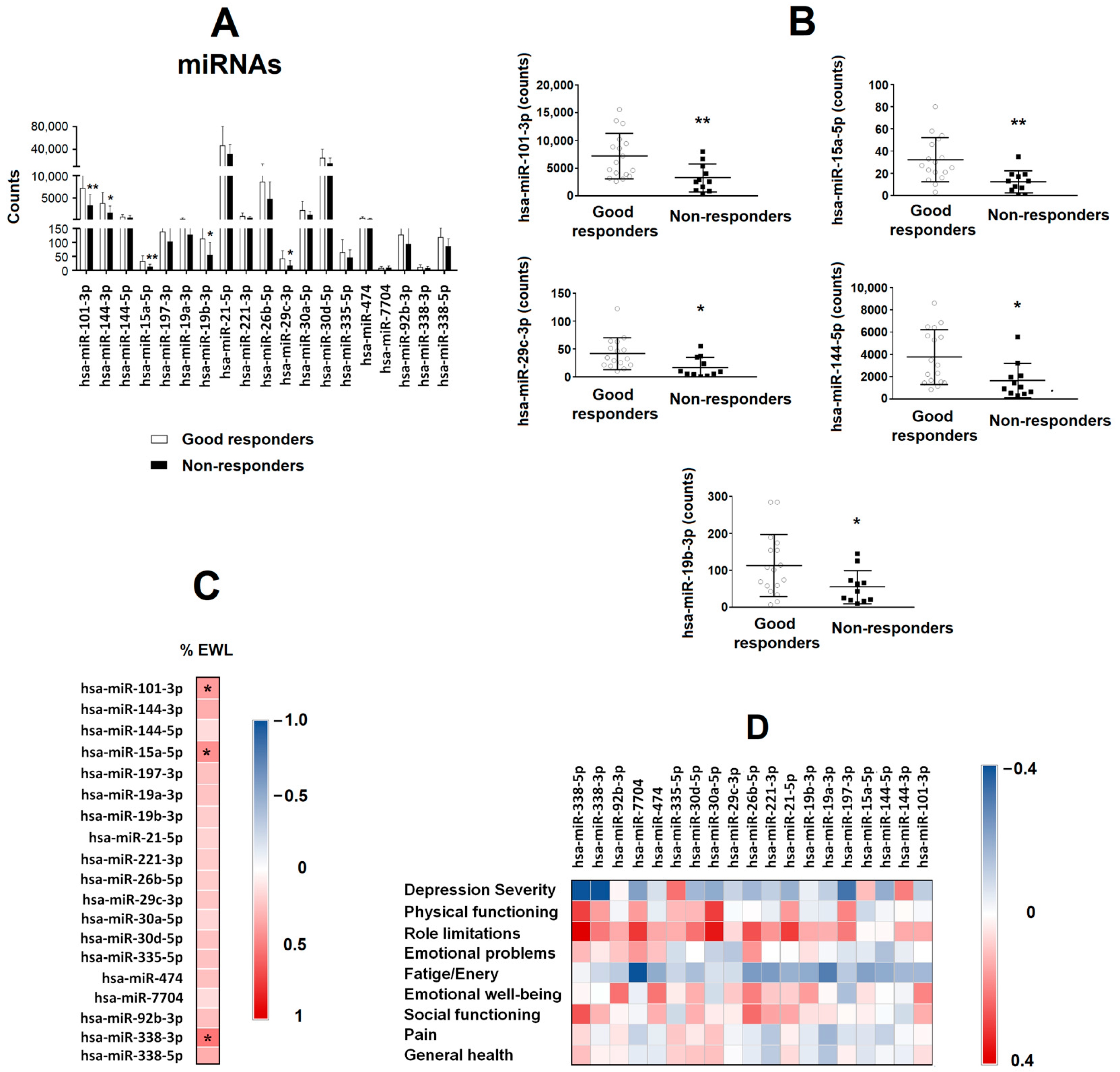
3.5. miRNA Levels as a Biomarker Predictor of Intervention Success in Patients with Class III Obesity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization, Updated 9 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 May 2022).
- Golzarand, M.; Toolabi, K.; Farid, R. The bariatric surgery and weight losing: A meta-analysis in the long- and very long-term effects of laparoscopic adjustable gastric banding, laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy on weight loss in adults. Surg. Endosc. 2017, 31, 4331–4345. [Google Scholar] [CrossRef] [PubMed]
- Closs, C.; Ackerman, M.; Masson, W.; Lobo, M.; Molinero, G.; Lavalle-Cobo, A.; Béliard, S.; Mourre, F.; Valéro, R.; Nogueira, J.P. Effectiveness of Roux-en-Y Gastric Bypass vs. Sleeve Gastrectomy on Lipid Levels in Type 2 Diabetes: A Meta-analysis. J. Gastrointest. Surg. 2022, 26, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, N.; Antoniou, S.A.; Batterham, R.L.; Busetto, L.; Godoroja, D.; Iossa, A.; Carrano, F.M.; Agresta, F.; Alarçon, I.; Azran, C.; et al. Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: Update 2020 endorsed by IFSO-EC, EASO and ESPCOP. Surg. Endosc. 2020, 34, 2332–2358. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, H.; Avidor, Y.; Braunwald, E.; Jensen, M.D.; Pories, W.; Fahrbach, K.; Schoelles, K. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef] [PubMed]
- Axer, S.; Szabo, E.; Näslund, I. Non-response After Gastric Bypass and Sleeve Gastrectomy-the Theoretical Need for Revisional Bariatric Surgery: Results from the Scandinavian Obesity Surgery Registry. Obes. Surg. 2023, 33, 2973–2980. [Google Scholar] [CrossRef] [PubMed]
- Riedel, O.; Braitmaier, M.; Dankhoff, M.; Hornschuch, M.; Klein, M.; Zachariassen, W.; Hoyer, J. Quality of life in bariatric patients up to twelve years after surgery—Results from a nationwide retrospective cohort study. Obes. Res. Clin. Pract. 2023, 17, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Lammert, M.; Medawar, E.; Hartmann, H.; Grasser, L.; Dietrich, A.; Fenske, W.; Horstmann, A. Distinct adaptations of endocrine and cognitive functions may contribute to high variability in long-term weight loss outcome after bariatric surgery. Physiol. Behav. 2023, 269, 114279. [Google Scholar] [CrossRef] [PubMed]
- Grönroos, S.; Helmiö, M.; Juuti, A.; Tiusanen, R.; Hurme, S.; Löyttyniemi, E.; Ovaska, J.; Leivonen, M.; Peromaa-Haavisto, P.; Mäklin, S.; et al. Effect of Laparoscopic Sleeve Gastrectomy vs Roux-en-Y Gastric Bypass on Weight Loss and Quality of Life at 7 Years in Patients with Morbid Obesity: The SLEEVEPASS Randomized Clinical Trial. JAMA Surg. 2021, 156, 137–146. [Google Scholar] [CrossRef]
- Askari, A.; Dai, D.; Taylor, C.; Chapple, C.; Halai, S.; Patel, K.; Mamidanna, R.; Munasinghe, A.; Rashid, F.; Al-Taan, O.; et al. Long-Term Outcomes and Quality of Life at More than 10 Years After Laparoscopic Roux-en-Y Gastric Bypass Using Bariatric Analysis and Reporting Outcome System (BAROS). Obes. Surg. 2020, 30, 3968–3973. [Google Scholar] [CrossRef]
- Hany, M.; Zidan, A.; Sabry, K.; Ibrahim, M.; Agayby, A.S.S.; Aboelsoud, M.R.; Torensma, B. How Good is Stratification and Prediction Model Analysis Between Primary and Revisional Roux-en-Y Gastric Bypass Surgery? A Multi-center Study and Narrative Review. Obes. Surg. 2023, 33, 1431–1448. [Google Scholar] [CrossRef]
- Suh, H.R.; Mui, J.; Cheng, E.; Liu, D.; Sun, S.L.; Loi, K.; Magdy, M.; Gagner, M. Outcomes of single anastomosis duodeno ileal bypass and single anastomosis stomach ileal bypass for type II diabetes: A systematic review. Expert. Rev. Endocrinol. Metab. 2023, 18, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Wang, Y.; Ji, J.; Wang, W.; Wang, D. One Anastomosis Gastric Bypass Versus Sleeve Gastrectomy for Obesity: A Systemic Review and Meta-analysis. J. Gastrointest. Surg. 2023. [Google Scholar] [CrossRef] [PubMed]
- Admiraal, W.M.; Celik, F.; Gerdes, V.E.; Dallal, R.M.; Hoekstra, J.B.; Holleman, F. Ethnic differences in weight loss and diabetes remission after bariatric surgery: A meta-analysis. Diabetes. Care. 2012, 35, 1951–1958. [Google Scholar] [CrossRef] [PubMed]
- Calderone, A.; Calabro, P.F.; Lippi, C.; Jaccheri, R.; Vitti, J.; Santini, F. Psychopathological Behaviour and Cognition in Morbid Obesity. Recent. Pat. Endocr. Metab. Immune. Drug. Discov. 2017, 10, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry. 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Sierżantowicz, R.; Ładny, J.R.; Lewko, J. Quality of Life after Bariatric Surgery-A Systematic Review. Int. J. Environ. Res. Public. Health. 2022, 19, 9078. [Google Scholar] [CrossRef] [PubMed]
- Małczak, P.; Mizera, M.; Lee, Y.; Pisarska-Adamczyk, M.; Wysocki, M.; Bała, M.M.; Witowski, J.; Rubinkiewicz, M.; Dudek, A.; Stefura, T. Quality of Life After Bariatric Surgery-a Systematic Review with Bayesian Network Meta-analysis. Obes. Surg. 2021, 31, 5213–5223. [Google Scholar] [CrossRef] [PubMed]
- Wimmelmann, C.L.; Dela, F.; Mortensen, E.L. Psychological predictors of mental health and health-related quality of life after bariatric surgery: A review of the recent research. Obes. Res. Clin. Pract. 2014, 8, e314–e324. [Google Scholar] [CrossRef]
- Averbukh, Y.; Heshka, S.; El-Shoreya, H.; Flancbaum, L.; Geliebter, A.; Kamel, S.; Pi-Sunyer, F.X.; Laferrère, B. Depression score predicts weight loss following Roux-en-Y gastric bypass. Obes. Surg. 2003, 13, 833–836. [Google Scholar] [CrossRef]
- Aguera, Z.; García-Ruiz-de-Gordejuela, A.; Vilarrasa, N.; Sanchez, I.; Baño, M.; Camacho, L.; Granero, R.; Jiménez-Murcia, S.; Virgili, N.; Lopez-Urdiales, R.; et al. Psychological and Personality Predictors of Weight Loss and Comorbid Metabolic Changes After Bariatric Surgery. Eur. Eat. Disord. Rev. 2015, 23, 509–516. [Google Scholar] [CrossRef]
- Atlantis, E.; Baker, M. Obesity effects on depression: Systematic review of epidemiological studies. Int. J. Obes. 2008, 32, 881–891. [Google Scholar] [CrossRef]
- Roberts, R.E.; Duong, H.T. Does major depression affect risk for adolescent obesity? J. Affect Disord. 2015, 186, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Patist, C.M.; Stapelberg, N.J.C.; Du Toit, E.F.; Headrick, J.P. The brain-adipocyte-gut network: Linking obesity and depression subtypes. Cogn. Affect Behav. Neurosci. 2018, 18, 1121–1144. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Capuron, L.; Miller, A.H. Cytokines sing the blues: Inflammation and the pathogenesis of depression. Trends. Immunol. 2006, 27, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Stapelberg, N.J.C.; Neumann, D.L.; Shum, D.H.K.; McConnell, H.; Hamilton-Craig, I. From physiome to pathome: A systems biology model of major depressive disorder and the psycho-immune-neuroendocrine network. Curr. Psychiatry Rev. 2015, 11, 32–62. [Google Scholar] [CrossRef]
- Elovainio, M.; Aalto, A.M.; Kivimäki, M.; Pirkola, S.; Sundvall, J.; Lönnqvist, J.; Reunanen, A. Depression and C-reactive protein: Population-based Health 2000 Study. Psychosom. Med. 2009, 71, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Gimeno, D.; Kivimäki, M.; Brunner, E.J.; Elovainio, M.; De Vogli, R.; Steptoe, A.; Kumari, M.; Lowe, G.D.; Rumley, A.; Marmot, M.G.; et al. Associations of C-reactive protein and interleukin-6 with cognitive symptoms of depression: 12-year follow-up of the Whitehall II study. Psychol. Med. 2009, 39, 413–423. [Google Scholar] [CrossRef]
- Serna-Rodríguez, M.F.; Bernal-Vega, S.; de la Barquera, J.A.O.; Camacho-Morales, A.; Pérez-Maya, A.A. The role of damage associated molecular pattern molecules (DAMPs) and permeability of the blood-brain barrier in depression and neuroinflammation. J. Neuroimmunol. 2022, 371, 577951. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, J.; Liu, Y.; Li, Z.; Li, X. TLR4-NF-κB Signal Involved in Depressive-Like Behaviors and Cytokine Expression of Frontal Cortex and Hippocampus in Stressed C57BL/6 and ob/ob Mice. Neural. Plast. 2018, 2018, 7254016. [Google Scholar] [CrossRef]
- Ouakinin, S.R.S.; Barreira, D.P.; Gois, C.J. Depression and Obesity: Integrating the Role of Stress, Neuroendocrine Dysfunction and Inflammatory Pathways. Front. Endocrinol. 2018, 9, 431. [Google Scholar] [CrossRef]
- Ferrua, C.P.; Giorgi, R.; da Rosa, L.C.; do Amaral, C.C.; Ghisleni, G.C.; Pinheiro, R.T.; Nedel, F. MicroRNAs expressed in depression and their associated pathways: A systematic review and a bioinformatics analysis. J. Chem. Neuroanat. 2019, 100, 101650. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Dosal, A.; Rodil-García, P.; Salazar-Olivo, L.A. Circulating microRNAs in human obesity: A systematic review. Biomarkers 2019, 24, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, M.; Asghar, R.; Firdoos, S.; Ahmad, N.; Nazir, A.; Ullah, K.M.; Li, N.; Zhuang, F.; Chen, Z.; Deng, Y. A Systematic Review of Circulatory microRNAs in Major Depressive Disorder: Potential Biomarkers for Disease Prognosis. Int. J. Mol. Sci. 2022, 23, 1294. [Google Scholar] [CrossRef] [PubMed]
- De Hollanda, A.; Ruiz, T.; Jimenez, A.; Flores, L.; Lacy, A.; Vidal, J. Patterns of Weight Loss Response Following Gastric Bypass and Sleeve Gastrectomy. Obes. Surg. 2015, 25, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Christou, N.V.; Look, D.; Maclean, L.D. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann. Surg. 2006, 244, 734–740. [Google Scholar] [CrossRef]
- Brethauer, S.A.; Kim, J.; el Chaar, M.; Papasavas, P.; Eisenberg, D.; Rogers, A.; Ballem, N.; Kligman, M.; Kothari, S.; ASMBS Clinical Issues Committee. Standardized outcomes reporting in metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2015, 11, 489–506. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Dwivedi, Y. MicroRNAs in depression and suicide: Recent insights and future perspectives. J. Affect Disord. 2018, 240, 146–154. [Google Scholar] [CrossRef]
- Wingo, T.S.; Yang, J.; Fan, W.; Canon, S.M.; Gerasimov, E.S.; Lori, A.; Logsdon, B.; Yao, B.; Seyfried, N.T.; Lah, J.; et al. Brain microRNAs associated with late-life depressive symptoms are also associated with cognitive trajectory and dementia. NPJ Genom. Med. 2020, 5, 6. [Google Scholar] [CrossRef]
- Lachowicz, M.J.; Preacher, K.J.; Kelley, K. A novel measure of effect size for mediation analysis. Psychol. Methods 2018, 23, 244–261. [Google Scholar] [CrossRef] [PubMed]
- Silha, J.V.; Krsek, M.; Sucharda, P.; Murphy, L.J. Angiogenic factors are elevated in overweight and obese individuals. Int. J. Obes. 2005, 29, 1308–1314. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Barajas, S.; Lammoglia, G.M.; Reyna, A.J.; Morley, T.S.; Johnson, J.A.; Scherer, P.E.; Rutkowski, J.M. Vascular Endothelial Growth Factor-D (VEGF-D) Overexpression and Lymphatic Expansion in Murine Adipose Tissue Improves Metabolism in Obesity. Am. J. Pathol. 2019, 189, 924–939. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.M.; Shao, Z.; Grenier, V.; Mawambo, G.; Daudelin, J.-F.; Dejda, A.; Pilon, F.; Popovic, N.; Boulet, S.; Parinot, C.; et al. Neuropilin-1 expression in adipose tissue macrophages protects against obesity and metabolic syndrome. Sci. Immunol. 2018, 3, eaan4626. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Bot, M.; Jansen, R.; Chan, M.K.; Cooper, J.D.; Bahn, S.; Penninx, B.W.J.H. Serum proteomic profiles of depressive subtypes. Transl. Psychiatry 2016, 6, e851. [Google Scholar] [CrossRef] [PubMed]
- Kalkman, H.O. The Association Between Vascular Inflammation and Depressive Disorder. Causality, Biomarkers and Targeted Treatment. Pharmaceuticals 2020, 13, 92. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.; Matsuda, K. How Microbes Affect Depression: Underlying Mechanisms via the Gut-Brain Axis and the Modulating Role of Probiotics. Int. J. Mol. Sci. 2022, 23, 1172. [Google Scholar] [CrossRef] [PubMed]
- Connolly, C.; Magnusson-Lind, A.; Lu, G.; Wagner, P.K.; Southwell, A.L.; Hayden, M.R.; Björkqvist, M.; Leavitt, B.R. Enhanced immune response to MMP3 stimulation in microglia expressing mutant huntingtin. Neuroscience 2016, 325, 74–88. [Google Scholar] [CrossRef]
- Fulton, S.; Décarie-Spain, L.; Fioramonti, X.; Guiard, B.; Nakajima, S. The menace of obesity to depression and anxiety prevalence. Trends. Endocrinol. Metab. 2022, 33, 18–35. [Google Scholar] [CrossRef]
- Wang, X.; Sundquist, K.; Hedelius, A.; Palmer, K.; Memon, A.A.; Sundquist, J. Circulating microRNA-144-5p is associated with depressive disorders. Clin. Epigenetics 2015, 7, 69. [Google Scholar] [CrossRef]
- Assmann, T.S.; Riezu-Boj, J.I.; Milagro, F.I.; Martínez, J.A. Circulating adiposity-related microRNAs as predictors of the response to a low-fat diet in subjects with obesity. J. Cell. Mol. Med. 2020, 24, 2956–2967. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Wang, Z.; Cheng, Y.; Ma, C.; Zhong, Y.; Xiao, Y.; Gao, X.; Li, Z. M2 macrophage-derived exosomal microRNAs inhibit cell migration and invasion in gliomas through PI3K/AKT/mTOR signaling pathway. J. Transl. Med. 2021, 19, 99. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, M.; Wei, F.Y.; Chujo, T.; Oki, S.; Yakita, M.; Kobayashi, D.; Araki, N.; Takahashi, N.; Yoshida, R.; Nakayama, H.; et al. FTO Demethylates Cyclin D1 mRNA and Controls Cell-Cycle Progression. Cell Rep. 2020, 31, 107464. [Google Scholar] [CrossRef] [PubMed]
- Langi, G.; Szczerbinski, L.; Kretowski, A. Meta-Analysis of Differential miRNA Expression after Bariatric Surgery. J. Clin. Med. 2019, 8, 1220. [Google Scholar] [CrossRef]
- Huimin, X.; Xiuwu, L.; Huaijun, N. Clinical significance of miR-19b-3p in patients with sepsis and its regulatory role in the LPS-induced inflammatory response. Eur. J. Med. Res. 2020, 25, 9. [Google Scholar]
- Liang, D.; Dapeng, D.; Wenbo, W.; Zhengming, S.; Honghai, X.; Lipeng, G.; Xuanhui, W. MiR-19b-3p attenuates IL-1β induced extracellular matrix degradation and inflammatory injury in chondrocytes by targeting GRK6. Mol. Cell Biochem. 2019, 459, 205–214. [Google Scholar]
- Lan, T.; Lim, C.; Yang, G.; Sun, Y.; Zhuang, L.; Ou, Y.; Li, H.; Wang, G.; Kisseleva, T.; Brenner, D.; et al. Sphingosine kinase 1 promotes liver fibrosis by preventing miR-19b-3p-mediated inhibition of CCR2. Hepatology 2018, 68, 1070–1086. [Google Scholar] [CrossRef]
- Van Rijswijk, A.S.; van Olst, N.; Schats, W.; van der Peet, D.L.; van de Laar, A.W. What Is Weight Loss After Bariatric Surgery Expressed in Percentage Total Weight Loss (%TWL)? A Systematic Review. Obes. Surg. 2021, 31, 3833–3847. [Google Scholar] [CrossRef]
- Ching, S.S.; Lee, P.C.; Lim, C.H.; Wong, A.S.Y.; Ng, A.Y.; Lin, J.; Lee, J. Study on weight loss outcomes after bariatric surgery to determine a metric least influenced by preoperative BMI. Int. J. Obes. 2023, 47, 993–999. [Google Scholar] [CrossRef]
- Yarigholi, F.; Bahardoust, M.; Mosavari, H.; Tehrani, F.M.; Gholizadeh, H.; Shahmiri, S.S.; Rezvani, H.; Oshidari, B.; Garakani, K.; Eghbali, F. Predictors of Weight Regain and Insufficient Weight Loss According to Different Definitions After Sleeve Gastrectomy: A Retrospective Analytical Study. Obes. Surg. 2022, 32, 4040–4046. [Google Scholar] [CrossRef]
- Saiki, A.; Yamaguchi, T.; Tanaka, S.; Sasaki, A.; Naitoh, T.; Seto, Y.; Matsubara, H.; Yokote, K.; Okazumi, S.; Ugi, S.; et al. Background characteristics and postoperative outcomes of insufficient weight loss after laparoscopic sleeve gastrectomy in Japanese patients. Ann. Gastroenterol. Surg. 2019, 3, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Van de Laar, A.W.; Nienhuijs, S.W.; Apers, J.A.; van Rijswijk, A.S.; de Zoete, J.P.; Gadiot, R.P. The Dutch bariatric weight loss chart: A multicenter tool to assess weight outcome up to 7 years after sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass. Surg. Obes. Relat. Dis. 2019, 15, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cordero, S.; Garcia Ruiz de Gordejuela, A.; Vilallonga, R.; Gonzalez, O.; Ciscar, A.; Ciudin, A.; Zabalegui, A.; Armengol, M. Analysis of the Variability in Different Criteria to Define the Success of Bariatric Surgery: Retrospective Study 5-Year Follow-Up after Sleeve Gastrectomy and Roux-en-Y Gastric Bypass. J. Clin. Med. 2022, 12, 187. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, G.; Wang, L.; Wuyun, Q.; Sang, Q.; Wang, J.; Tian, C.; Shang, M.; Wang, Z.; Du, D.; et al. Analysis of Correlation between Age and Satisfied Total Weight Loss Percentage Outcome at 1 Year after Bariatric Surgery using the Restricted Cubic Spline Function: A Retrospective Study in China. Obes. Surg. 2023, 33, 3133–3140. [Google Scholar] [CrossRef] [PubMed]
- Kapała, J.; Maroszczuk, T.; Lewandowska, J.; Lech, P.; Dowgiałło-Gornowicz, N. Weight Regain in the Second Year after Sleeve Gastrectomy Could Be a Predictor of Long-Term Outcomes? Medicina 2023, 59, 766. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Pan, Y.; Han, J.; Pan, J.; Zhang, P.; Jia, W.; Bao, Y.; Yu, H. A total weight loss of 25% shows better predictivity in evaluating the efficiency of bariatric surgery. Int. J. Obes. 2021, 45, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Holmes, C.J.; Racette, S.B. The Utility of Body Composition Assessment in Nutrition and Clinical Practice: An Overview of Current Methodology. Nutrients 2021, 13, 2493. [Google Scholar] [CrossRef]
- Salmón-Gómez, L.; Catalán, V.; Frühbeck, G.; Gómez-Ambrosi, J. Relevance of body composition in phenotyping the obesities. Rev. Endocr. Metab. Disord. 2023, 24, 809–823. [Google Scholar] [CrossRef]
- Bray, G.A. Beyond BMI. Nutrients 2023, 15, 2254. [Google Scholar] [CrossRef]
- Von Berens, Å.; Obling, S.R.; Nydahl, M.; Koochek, A.; Lissner, L.; Skoog, I.; Frändin, K.; Skoglund, E.; Rothenberg, E.; Cederholm, T. Sarcopenic obesity and associations with mortality in older women and men—A prospective observational study. BMC Geriatr. 2020, 20, 199. [Google Scholar] [CrossRef]
- Simó-Servat, A.; Ibarra, M.; Libran, M.; Quirós, C.; Puértolas, N.; Alonso, N.; Perea, V.; Simó, R.; Barahona, M.J. Usefulness of Ultrasound in Assessing the Impact of Bariatric Surgery on Body Composition: A Pilot Study. Obes. Surg. 2023, 33, 1211–1217. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RYGB/BPD | SG | p-Value | |
|---|---|---|---|
| n (male/female) | 41 (6/35) | 49 (9/40) | 0.64 |
| Age at the time of surgery (years) | 42.4 ± 9.8 | 44.3 ± 9 | 0.34 |
| %EWL | 58.5 ± 36.6 | 52.8 ± 25.7 | 0.071 |
| %TWL | 30.1 ± 13.4 | 24.7 ± 12.1 | 0.003 |
| BMI (kg/m2) | 50.1 ± 7.8 | 48.6 ± 7.6 | 0.03 |
| 34.8 ± 7.3 *** | 36.1 ± 6.1 *** | 0.66 | |
| Waist (cm) | 133.7 ± 15.5 | 130.5 ± 15.1 | 0.05 |
| 103.3 ± 18.1 *** | 104.2 ± 15.5 *** | 0.74 | |
| Hip (cm) | 145.8 ± 17.2 | 144.5 ± 12.3 | 0.17 |
| 117.4 ± 17 *** | 121.5 ± 12.5 *** | 0.27 | |
| Waist/hip ratio | 0.93 ± 0.15 | 0.9 ± 0.09 | 0.53 |
| 0.87 ± 0.09 * | 0.86 ± 0.09 * | 0.26 | |
| SBP (mmHg) | 138.5 ± 19.8 | 133 ± 17.6 | 0.23 |
| 118 ± 16.1 *** | 130.9 ± 23.6 | 0.002 | |
| DBP (mmHg) | 82.9 ± 12.4 | 80.8 ± 9 | 0.42 |
| 67.7 ± 9.3 *** | 72 ± 12.6 *** | 0.02 | |
| Glucose (mg/dl) | 111.9 ± 44.1 | 97.9 ± 27 | 0.01 |
| 81.4 ± 9.9 *** | 84.1 ± 9 *** | 0.45 | |
| Insulin (mg/dl) | 20.8 ± 11.7 | 15.9 ± 12.1 | 0.03 |
| 7.8 ± 6.1 *** | 9.9 ± 5.3 *** | 0.10 | |
| HOMA-IR | 6.2 ± 5 | 4.1 ± 3.4 | 0.003 |
| 1.65 ± 1.6 *** | 2.12 ± 1.3 *** | 0.15 | |
| Triglycerides (mg/dl) | 136.9 ± 89 | 118.6 ± 53.8 | 0.17 |
| 87.6 ± 35.4 *** | 89.8 ± 40.5 *** | 0.62 | |
| Cholesterol (mg/dl) | 190.2 ± 41.8 | 178 ± 34.7 | 0.16 |
| 164.1 ± 40.2 | 197.6 ± 39.4 | <0.001 | |
| HDL-c (mg/dl) | 46.3 ± 14.4 | 44.3 ± 13.7 | 0.47 |
| 61.9 ± 16.9 *** | 66.8 ± 16.5 *** | 0.18 | |
| LDL-c (mg/dl) | 113.5 ± 31.2 | 110.6 ± 33.6 | 0.92 |
| 84.5 ± 31.1 *** | 112.3 ± 32.6 | <0.001 |
| Good Responders | Non-Responders | p-Value | |
|---|---|---|---|
| n (male/female) | 60 (9/51) | 30 (6/24) | 0.55 |
| Type of surgery (RYGB-BPD/SG) | 60 (28/32) | 30 (12/18) | 0.35 |
| Age at the time of surgery (years) | 42.5 ± 10.2 | 45.3 ± 7.5 | 0.19 |
| %EWL | 71.0 ± 14.7 | 23.0 ± 34.8 | <0.001 |
| %TWL | 33.8 ± 7.3 | 13.8 ± 12.6 | <0.001 |
| BMI (kg/m2) | 48.8 ± 6.7 | 50 ± 9.3 | 0.55 |
| 32.2 ± 4.6 *** | 42.2 ± 4.9 *** | <0.001 | |
| Waist (cm) | 132.2 ± 15.7 | 131.6 ± 14.6 | 0.87 |
| 98.1 ± 15.9 *** | 116.3 ± 12.2 *** | <0.001 | |
| Hip (cm) | 145.9 ± 13 | 143.57 ± 17.6 | 0.49 |
| 112.8 ± 12.1 *** | 132.7931 ± 11.3 ** | <0.001 | |
| Waist/hip ratio | 0.91 ± 0.1 | 0.94 ± 0.2 | 0.34 |
| 0.85 ± 0.09 *** | 0.9 ± 0.1 | 0.48 | |
| SBP (mmHg) | 135.4 ± 19.2 | 134.6 ± 18.1 | 0.87 |
| 116.6 ± 15.7 *** | 140 ± 23.7 | <0.001 | |
| DBP (mmHg) | 81.8 ± 10.7 | 79.6 ± 9.1 | 0.38 |
| 67.1 ± 10.4 *** | 75.4 ± 11.2 | 0.005 | |
| Glucose (mg/dl) | 108.1 ± 41.7 | 97 ± 19.9 | 0.11 |
| 81 ± 6.9 *** | 87.2 ± 12.4 ** | 0.02 | |
| Insulin (mg/dl) | 20.5 ±13.8 | 14.5 ± 7.3 | 0.05 |
| 7.6 ± 5.8 *** | 11.5 ± 4.9 * | 0.003 | |
| HOMA-IR | 5.9 ± 5 | 3.6 ± 2.2 | 0.01 |
| 1.6 ± 1.5 *** | 2.5 ± 1.3 * | 0.004 | |
| Triglycerides (mg/dl) | 134.2 ± 78.7 | 112.9 ±55.4 | 0.20 |
| 79.2 ± 29.7 *** | 108.5 ± 46 ** | 0.004 | |
| Cholesterol (mg/dl) | 184.9 ± 40.9 | 180.5 ± 33.7 | 0.61 |
| 181.2 ± 44.5 | 185.6 ± 41.3 | 0.72 | |
| HDL-c (mg/dl) | 44.8 ± 13.6 | 45.3 ± 14.7 | 0.95 |
| 66.6 ± 17.9 *** | 59.9 ± 13.4 *** | 0.05 | |
| LDL-c (mg/dl) | 110.9 ± 34.4 | 113.7 ± 29.2 | 0.68 |
| 99.2 ±35.1 * | 103.6 ±33.5 * | 0.52 |
| Good Responders (n = 30) | Non-Responders (n = 23) | |||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | |d| | |
| SF-36 Physical functioning | 72.32 | 26.95 | 54.07 | 27.95 | 0.039 * | 0.66 † |
| SF-36 Role—physical | 74.71 | 40.97 | 37.52 | 42.80 | 0.008 * | 0.89 † |
| SF-36 Body pain | 59.63 | 20.80 | 43.27 | 24.48 | 0.029 * | 0.72 † |
| SF-36 General health | 70.97 | 23.29 | 59.75 | 22.15 | 0.129 | 0.51 † |
| SF-36 Vitality | 49.93 | 25.19 | 40.06 | 22.85 | 0.187 | 0.41 |
| SF-36 Social functioning | 82.04 | 23.21 | 65.12 | 28.51 | 0.054 | 0.65 † |
| SF-36 Role—emotional | 84.02 | 39.65 | 51.28 | 43.25 | 0.013 * | 0.79 † |
| SF-36 Mental health | 59.79 | 24.39 | 53.57 | 26.10 | 0.449 | 0.25 |
| SF-36 Global general health | 69.24 | 22.63 | 51.39 | 24.68 | 0.020 * | 0.75 † |
| BDI-II Total | 12.44 | 13.52 | 22.44 | 15.91 | 0.040 * | 0.68 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mela, V.; Agüera, Z.; Alvarez-Bermudez, M.D.; Martín-Reyes, F.; Granero, R.; Sánchez-García, A.; Oliva-Olivera, W.; Tomé, M.; Moreno-Ruiz, F.J.; Soler-Humanes, R.; et al. The Relationship between Depressive Symptoms, Quality of Life and miRNAs 8 Years after Bariatric Surgery. Nutrients 2023, 15, 4109. https://doi.org/10.3390/nu15194109
Mela V, Agüera Z, Alvarez-Bermudez MD, Martín-Reyes F, Granero R, Sánchez-García A, Oliva-Olivera W, Tomé M, Moreno-Ruiz FJ, Soler-Humanes R, et al. The Relationship between Depressive Symptoms, Quality of Life and miRNAs 8 Years after Bariatric Surgery. Nutrients. 2023; 15(19):4109. https://doi.org/10.3390/nu15194109
Chicago/Turabian StyleMela, Virginia, Zaida Agüera, Maria D. Alvarez-Bermudez, Flores Martín-Reyes, Roser Granero, Ana Sánchez-García, Wilfredo Oliva-Olivera, Monica Tomé, Francisco J. Moreno-Ruiz, Rocío Soler-Humanes, and et al. 2023. "The Relationship between Depressive Symptoms, Quality of Life and miRNAs 8 Years after Bariatric Surgery" Nutrients 15, no. 19: 4109. https://doi.org/10.3390/nu15194109
APA StyleMela, V., Agüera, Z., Alvarez-Bermudez, M. D., Martín-Reyes, F., Granero, R., Sánchez-García, A., Oliva-Olivera, W., Tomé, M., Moreno-Ruiz, F. J., Soler-Humanes, R., Fernández-Serrano, J. L., Sánchez-Gallegos, P., Martínez-Moreno, J. M., Sancho-Marín, R., Fernández-Aranda, F., García-Fuentes, E., Tinahones, F. J., & Garrido-Sánchez, L. (2023). The Relationship between Depressive Symptoms, Quality of Life and miRNAs 8 Years after Bariatric Surgery. Nutrients, 15(19), 4109. https://doi.org/10.3390/nu15194109