Whole Goat Milk-Based Formula versus Whey-Based Cow Milk Formula: What Formula Do Infants Enjoy More?—A Feasibility, Double-Blind, Randomized Controlled Trial

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
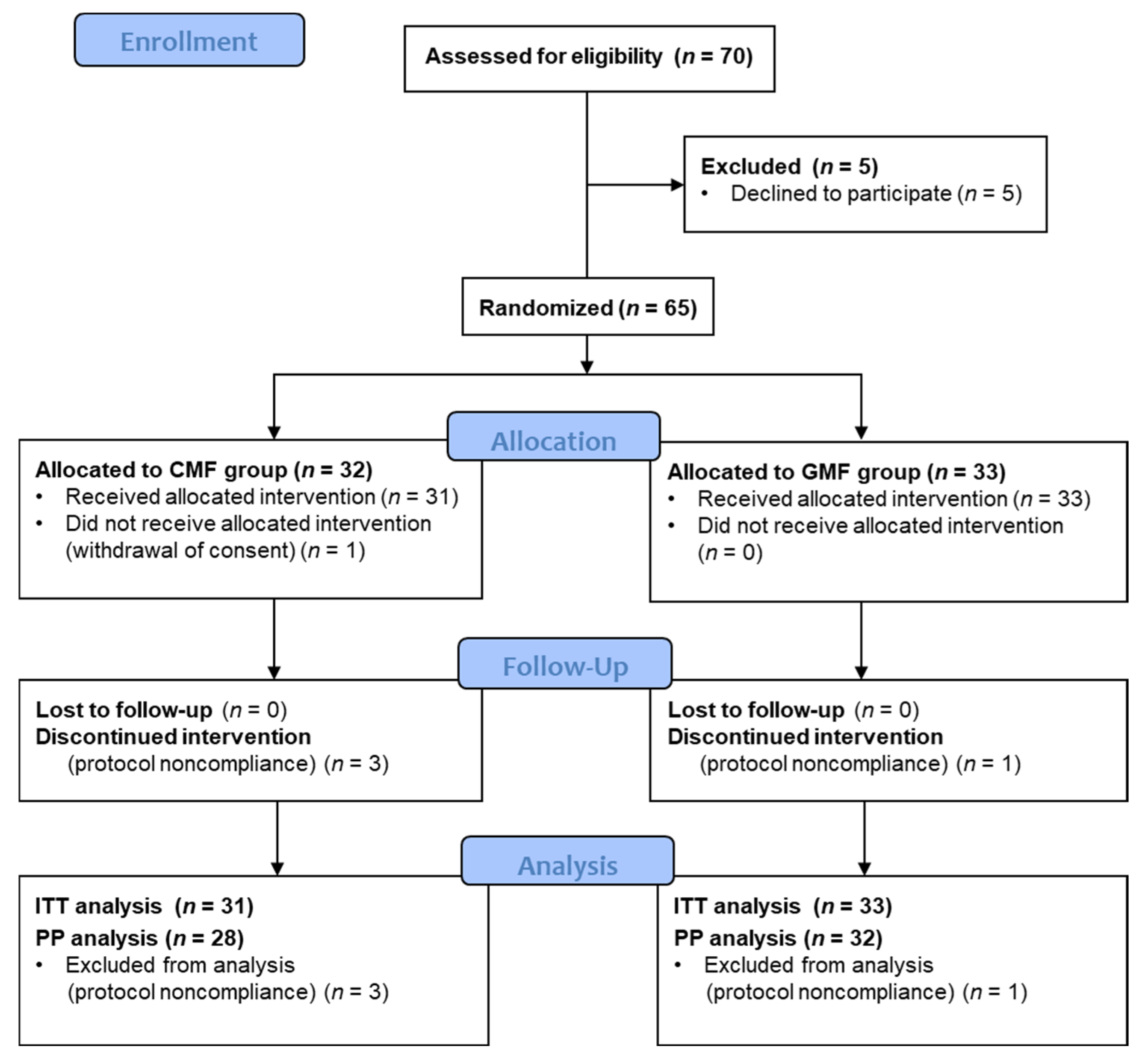
2.1. Design and Participants
2.2. Study Products
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeevenhooven, J.; Koppen, I.J.N.; Benninga, M.A. The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers. Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 1080924. [Google Scholar] [CrossRef]
- Iacono, G.; Merolla, R.; D’Amico, D.; Bonci, E.; Cavataio, F.; Di Prima, L.; Scalici, C.; Indinnimeo, L.; Averna, M.R.; Carroccio, A.; et al. Gastrointestinal symptoms in infancy: A population-based prospective study. Dig. Liver Dis. 2005, 37, 432–438. [Google Scholar] [CrossRef] [PubMed]
- van Tilburg, M.A.L.; Levy, R.L.; Walker, L.S.; Von Korff, M.; Feld, L.D.; Garner, M.; Feld, A.D.; Whitehead, W.E. Psychosocial mechanisms for the transmission of somatic symptoms from parents to children. World J. Gastroenterol. 2015, 21, 5532–5541. [Google Scholar] [CrossRef] [PubMed]
- Long, T.; Johnson, M. Living and coping with excessive infantile crying. J. Adv. Nurs. 2001, 34, 155–162. [Google Scholar] [CrossRef]
- World Health Organization; United Nations Children’s Fund (UNICEF). Implementation Guidance: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services: The Revised Baby-Friendly Hospital Initiative; World Health Organization: Geneva, Switzerland, 2018. Available online: https://apps.who.int/iris/handle/10665/272943 (accessed on 16 September 2023).
- Guajardo-Villar, A.; Demiguel, V.; Smaïli, S.; Boudet-Berquier, J.; Pilkington, H.; Blondel, B.; Salanave, B.; Regnault, N.; Pelat, C. Trends and disparities in breastfeeding initiation in France between 2010 and 2016: Results from the French National Perinatal Surveys. Matern. Child Nutr. 2022, 18, e13410. [Google Scholar] [CrossRef]
- Polack, F.P.; Khan, N.; Maisels, M.J. Changing partners: The dance of infant formula changes. Clin. Pediatr. 1999, 38, 703–708. [Google Scholar] [CrossRef]
- Nevo, N.; Rubin, L.; Tamir, A.; Levine, A.; Shaoul, R. Infant feeding patterns in the first 6 months: An assessment in full-term infants. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 234–239. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the essential composition of infant and follow-on formulae. EFSA J. 2014, 12, 3760. [CrossRef]
- Hodgkinson, A.J.; Wallace, O.A.M.; Smolenski, G.; Prosser, C.G. Gastric digestion of cow and goat milk: Peptides derived from simulated conditions of infant digestion. Food Chem. 2019, 276, 619–625. [Google Scholar] [CrossRef]
- Jiang, H.; Gallier, S.; Feng, L.; Han, J.; Liu, W. Development of the digestive system in early infancy and nutritional management of digestive problems in breastfed and formula-fed infants. Food Funct. 2022, 13, 1062–1077. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Mennella, J.A. Flavor Perception in Human Infants: Development and Functional Significance. Digestion 2011, 83, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. The Role of Dietary Experience in the Development of Eating Behavior during the First Years of Life. Ann. Nutr. Metab. 2017, 70, 241–245. [Google Scholar] [CrossRef]
- Mennella, J.A.; Beauchamp, G.K. Flavor experiences during formula feeding are related to preferences during childhood. Early Hum. Dev. 2002, 68, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Epifanio, M.; de Abreu, C.L.M.; Barros, K.; Oviedo, J.; Covic, A.; Ormenese, R.C.S. Palatability and Sensory Perception of Infant Formulas for the Treatment of Cow’s Milk Allergy According to Brazilian Mothers. Biomed. J. Sci. Tech. Res. 2020, 25, 18803–18810. [Google Scholar] [CrossRef]
- Zhou, S.J.; Sullivan, T.; Gibson, R.A.; Lönnerdal, B.; Prosser, C.G.; Lowry, D.J.; Makrides, M. Nutritional adequacy of goat milk infant formulas for term infants: A double-blind randomised controlled trial. Br. J. Nutr. 2014, 111, 1641–1651. [Google Scholar] [CrossRef]
- He, T.; Woudstra, F.; Panzer, F.; Haandrikman, A.; Verkade, H.J.; van Lee, L. Goat Milk Based Infant Formula in Newborns: A Double-Blind Randomized Controlled Trial on Growth and Safety. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 215–220. [Google Scholar] [CrossRef]
- Grant, C.; Rotherham, B.; Sharpe, S.; Scragg, R.; Thompson, J.; Andrews, J.; Wall, C.; Murphy, J.; Lowry, D. Randomized, double-blind comparison of growth in infants receiving goat milk formula versus cow milk infant formula. J. Paediatr. Child Health 2005, 41, 564–568. [Google Scholar] [CrossRef]
- Han, Y.; Chang, E.-Y.; Kim, J.; Ahn, K.; Kim, H.-Y.; Hwang, E.-M.; Lowry, D.; Prosser, C.; Lee, S.-I. Association of infant feeding practices in the general population with infant growth and stool characteristics. Nutr. Res. Pract. 2011, 5, 308–312. [Google Scholar] [CrossRef][Green Version]
- Xu, M.; Wang, Y.; Dai, Z.; Zhang, Y.; Li, Y.; Wang, J. Comparison of growth and nutritional status in infants receiving goat milk-based formula and cow milk-based formula: A randomized, double-blind study. Food Nutr. Res. 2015, 59, 28613. [Google Scholar] [CrossRef]
- Jankiewicz, M.; van Lee, L.; Biesheuvel, M.; Brouwer-Brolsma, E.M.; van der Zee, L.; Szajewska, H. The Effect of Goat-Milk-Based Infant Formulas on Growth and Safety Parameters: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2110. [Google Scholar] [CrossRef]
- European Commission Commission Directive 2006/141/EC of 22 December 2006 on Infant Formulae and Follow-On Formulae and Amending Directive 1999/21/EC (Text with EEA relevance). 2006. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:02006L0141-20130918&rid=1 (accessed on 16 September 2023).
- Llewellyn, C.H.; van Jaarsveld, C.H.M.; Johnson, L.; Carnell, S.; Wardle, J. Development and factor structure of the Baby Eating Behaviour Questionnaire in the Gemini birth cohort. Appetite 2011, 57, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, M.; Martel, C.; Porporino, M.; Zygmuntowicz, C. The Montreal Children’s Hospital Feeding Scale: A brief bilingual screening tool for identifying feeding problems. Paediatr. Child Health 2011, 16, 147-e17. [Google Scholar] [CrossRef] [PubMed]
- Manificat, S.; Dazord, A.; Langue, J.; Danjou, G.; Bauche, P.; Bovet, F.; Cubells, J.; Luchelli, R.; Tockert, E.; Conway, K. Evaluation of the quality of life of infants and very young children: Validation of a questionnaire. Multicenter European study. Arch. Pediatr. 2000, 7, 605–614. [Google Scholar] [CrossRef]
- Klockars, A.; Wood, E.L.; Gartner, S.N.; McColl, L.K.; Levine, A.S.; Carpenter, E.A.; Prosser, C.G.; Olszewski, P.K. Palatability of Goat’s versus Cow’s Milk: Insights from the Analysis of Eating Behavior and Gene Expression in the Appetite-Relevant Brain Circuit in Laboratory Animal Models. Nutrients 2019, 11, 720. [Google Scholar] [CrossRef]
- Rubio-Martín, E.; García-Escobar, E.; Ruiz de Adana, M.-S.; Lima-Rubio, F.; Peláez, L.; Caracuel, A.-M.; Bermúdez-Silva, F.-J.; Soriguer, F.; Rojo-Martínez, G.; Olveira, G. Comparison of the Effects of Goat Dairy and Cow Dairy Based Breakfasts on Satiety, Appetite Hormones, and Metabolic Profile. Nutrients 2017, 9, 877. [Google Scholar] [CrossRef] [PubMed]
- European Commission Consolidated Text: Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 Supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as Regards the Specific Compositional and Information Requirements for Infant Formula and Follow-On Formula and as Regards Requirements on Information Relating to Infant and Young Child Feeding (Text with EEA Relevance). 2021. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A02016R0127-20210408 (accessed on 17 March 2023).
- Gallier, S.; Tolenaars, L.; Prosser, C. Whole Goat Milk as a Source of Fat and Milk Fat Globule Membrane in Infant Formula. Nutrients 2020, 12, 3486. [Google Scholar] [CrossRef]
- Chen, Q.; Yin, Q.; Xie, Q.; Evivie, S.E.; Zhao, X.; Li, B.; Huo, G. Elucidating the physicochemical properties and surface composition of goat milk-based infant formula powders. Food Chem. 2022, 377, 131936. [Google Scholar] [CrossRef]
- Ye, A.; Cui, J.; Carpenter, E.; Prosser, C.; Singh, H. Dynamic in vitro gastric digestion of infant formulae made with goat milk and cow milk: Influence of protein composition. Int. Dairy J. 2019, 97, 76–85. [Google Scholar] [CrossRef]
- Dalziel, J.E.; Dunstan, K.E.; Dewhurst, H.; Van Gendt, M.; Young, W.; Carpenter, E. Goat milk increases gastric emptying and alters caecal short chain fatty acid profile compared with cow milk in healthy rats. Food Funct. 2020, 11, 8573–8582. [Google Scholar] [CrossRef]
- Hageman, J.H.J.; Danielsen, M.; Nieuwenhuizen, A.G.; Feitsma, A.L.; Dalsgaard, T.K. Comparison of bovine milk fat and vegetable fat for infant formula: Implications for infant health. Int. Dairy J. 2019, 92, 37–49. [Google Scholar] [CrossRef]
- Tannock, G.W.; Lawley, B.; Munro, K.; Gowri Pathmanathan, S.; Zhou, S.J.; Makrides, M.; Gibson, R.A.; Sullivan, T.; Prosser, C.G.; Lowry, D.; et al. Comparison of the compositions of the stool microbiotas of infants fed goat milk formula, cow milk-based formula, or breast milk. Appl. Environ. Microbiol. 2013, 79, 3040–3048. [Google Scholar] [CrossRef] [PubMed]
- Infante, D.; Prosser, C.; Tormo, R. Constipated Patients Fed Goat Milk Protein Formula: A Case Series Study. J. Nutr. Health Sci. 2018, 5, 203. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Total (n = 64) | GMF (n = 33) | CMF (n = 31) | p |
|---|---|---|---|---|
| Age, months | 2.4 ± 1.2 2(1–3) | 2.4 ± 1.2 2.5(1.5–3.5) | 2.4 ± 1.1 2(1–3.5) | 0.97 * |
| Males | 35 (54.7) | 20 (62.5) | 15 (53.5) | 0.33 ^ |
| Birth Weight, g | 3337.7 ± 700.9 3270(2997.5–3765) | 3415.8 ± 861.4 3507.5(3072.5–3877.5) | 3248.5 ± 454.0 3165(2937.5–3415) | 0.36 * |
| Length, cm | 50.2 ± 2.3 50(48.5–51) | 50.4 ± 2.6 50.3(49–51.5) | 49.9 ± 2.0 50(48–51) | 0.37 * |
| Inclusion Weight, g | 5329.2 ± 1366 5335(4595–6225) | 5540.1 ± 1213.2 5625(4650–6195) | 5104.6 ± 1500.7 4995(4100–6515) | 0.20 * |
| Length, cm | 58.8 ± 4.4 58.8(56–61.8) | 58.9 ± 4.4 58.8(56.3–61) | 58.7 ± 4.5 58.3(55.5–63.5) | 0.85 * |
| D28 ± 3 Weight, g | 6321.6 ± 1105.2 6150(5470–7130) | 6314.0 ± 1072.0 6170(5600–6790) | 6330.6 ± 1164.8 6095(5400–7200) | 0.90 µ |
| Length, cm | 62.0 ± 4.0 62(60–65) | 61.8 ± 4.1 62(59–64) | 62.3 ± 4.0 63.3(60–65) | 0.75 µ |
| Maternal age, years | 34.3 ± 4.8 35(32–36) | 34.2 ± 4.1 35(32–36) | 35.1 ± 4.9 35(32–39.5) | 0.44 * |
| Smoking during pregnancy Yes No | 10 (16.6) 50 (83.3) | 5 (15.6) 27 (84.3) | 5 (17.8) 23 (82.1) | 0.54 ^ |
| Alcohol consumption during pregnancy Yes No | 1 (1.7) 63 (98.4) | 1 (3.1) 31 (96.8) | 0 (0.0) 28 (100.0) | 1.0 ^ |
| Gestational diabetes Yes No | 7 (10.9) 57 (89.0) | 4 (12.5) 28 (87.5) | 3 (10.7) 25 (89.2) | 0.72 ^ |
| Delivery type Vaginal birth Planned cesarean Unplanned cesarean | 51 (79.7) 4 (6.7) 9 (14.0) | 25 (78.1) 3 (9.3) 4 (12.5) | 22 (78.5) 1 (3.5) 5 (17.8) | 0.64 ^ |
| BEBQ Subscales | PP Population | ITT Population | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 60) | GMF (n = 32) | CMF (n = 28) | p | Total (n = 64) | GMF (n = 33) | CMF (n = 31) | p | ||
| Enjoyment of Food | D0 | 4.4 ± 0.71 4.75(4–5) | 4.35 ± 0.85 4.63(4.25–5) | 4.47 ± 0.52 4.75(4–5) | 0.99 µ | 4.40 ± 0.71 4.75(4–5) | 4.35 ± 0.83 4.5(4.25–5) | 4.45 ± 0.57 4.75(4–5) | 0.57 µ |
| D28 | 4.58 ± 0.53 4.75(4.25–5) | 4.66 ± 0.47 4.88(4.5–5) | 4.50 ± 0.59 4.75(4–5) | 0.35 µ | 4.55 ± 0.56 4.75(4.25–5) | 4.65 ± 0.45 4.75(4.5–5) | 4.44 ± 0.65 4.55(4–5) | 0.14 µ | |
| ΔD0 − D28 | 0.15 ± 0.87 0(−0.25–0.38) | 0.30 ± 1.03 0(0–0.75) | −0.01 ± 0.61 0(−0.25–0.25) | 0.32 µ | 0.15 ± 0.82 0(−0.25–0.3) | 0.30 ± 0.98 0(0–0.5) | −0.01 ± 0.59 0(−0.25–0.25) | 0.18 µ | |
| Food Responsiveness | D0 | 2.05 ± 0.76 1.8(1.4–2.3) | 1.91 ± 0.67 1.78(1.4–2.2) | 2.19 ± 0.83 2(1.4–2.6) | 0.13 µ | 2.05 ± 0.76 1.9(1.4–2.4) | 1.91 ± 0.67 1.75(1.4–2.2) | 2.19 ± 0.83 2(1.4–2.6) | 0.13 * |
| D28 | 1.89 ± 0.91 1.6(1.2–2.4) | 2.07 ± 0.94 1.9(1.4–2.6) | 1.68 ± 0.85 1.4(1–2) | 0.04 µ | 1.90 ± 0.85 1.6(1.2–2.2) | 2.06 ± 0.89 1.89(1.4–2.4) | 1.71 ± 0.78 1.4(1–1.89) | 0.11 * | |
| ΔD0 − D28 | −0.12 ± 0.96 −0.4(−0.6–0.33) | 0.14 ± 1.05 0.1(−0.6–0.6) | −0.42 ± 0.76 −0.4(−0.8–0) | 0.04 µ | −0.16 ± 0.96 −0.4(−0.6–0.34) | 0.15 ± 1.00 0.2(−0.6–0.49) | −0.48 ± 0.81 −0.4(−1–0) | 0.010 µ | |
| Slowness in Eating | D0 | 2.53 ± 1.0 2.25(1.88–3.25) | 2.69 ± 0.98 2.5(2–3.38) | 2.36 ± 0.98 2.25(1.63–3) | 0.22 * | 2.56 ± 0.99 2.25(1.88–3.25) | 2.72 ± 0.99 2.5(2–3.5) | 2.40 ± 0.98 2.25(1.75–3.25) | 0.18 * |
| D28 | 2.13 ± 0.92 2(1.25–2.75) | 2.11 ± 0.89 2(1.25–2.75) | 2.16 ± 0.96 1.88(1.25–3) | 0.82 * | 2.16 ± 0.88 2.16(1.5–2.75) | 2.11 ± 0.84 2(1.5–2.50) | 2.21 ± 0.93 2.16(1.5–3) | 0.64 * | |
| ΔD0 − D28 | −0.41 ± 0.97 −0.25(−0.75–0.25) | −0.61 ± 1.06 −0.25(−1.25–0) | −0.17 ± 0.81 0(−0.5–0.25) | 0.11 µ | −0.40 ± 0.95 −0.25(−0.75–0.25) | −0.59 ± 1.0 −0.25(−1.25–0) | −0.17 ± 0.77 0(−0.5–0.25) | 0.08 µ | |
| Satiety Responsiveness | D0 | 2.63 ± 0.78 2.67(2–3.33) | 2.76 ± 0.78 3(2.33–3.33) | 2.49 ± 0.77 2.67(2–3) | 0.17 * | 2.64 ± 0.80 2.67(2–3.33) | 2.74 ± 0.78 3(2.33–3.33) | 2.53 ± 0.81 2.67(2–3) | 0.29 * |
| D28 | 2.70 ± 0.89 2.67(2–3.33) | 2.58 ± 0.76 2.67(2–3) | 2.83 ± 1.01 2.67(2–3.67) | 0.28 * | 2.71 ± 0.83 2.69(2.17–3.33) | 2.59 ± 0.73 2.67(2–3) | 2.83 ± 0.93 2.71(2.33–3.67) | 0.24 * | |
| ΔD0 − D28 | 0.10 ± 0.95 0(−0.34–0.84) | −0.12 ± 0.94 0(−0.67–0.34) | 0.35 ± 0.91 0.33(0–1) | 0.06 µ | 0.07 ± 0.93 0(−0.5–0.71) | −0.15 ± 0.93 0(−0.67–0.34) | 0.31 ± 0.88 0.33(0–1) | 0.049 * | |
| General Appetite | D0 | 3.85 ± 0.96 4(3–5) | 3.68 ± 1.05 4(3–4) | 4.0 ± 0.8 4(3.5–5) | 0.20 µ | 3.84 ± 0.97 4(3–5) | 3.69 ± 1.03 4(3–4) | 4.0 ± 0.90 4(3–5) | 0.21 µ |
| D28 | 3.79 ± 1.09 4(3–5) | 4.0 ± 1.08 4(4–5) | 3.54 ± 1.07 3.5(3–4) | 0.08 µ | 3.76 ± 1.04 4(3–5) | 3.98 ± 1.03 4(3.8–5) | 3.52 ± 1.02 3.8(3–4) | 0.07 µ | |
| ΔD0 − D28 | −0.07 ± 1.2 0(−1–0) | 0.31 ± 1.3 0.00(0–1) | −0.5 ± 0.95 0(−1–0) | 0.012 µ | −0.10 ± 1.13 0(−1–0) | 0.26 ± 1.23 0(−0.1–1) | −0.48 ± 0.88 0(−1–0) | 0.012 µ | |
| PP Population | ITT Population | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 60) | GMF (n = 32) | CMF (n = 28) | p | Total (n = 64) | GMF (n = 33) | CMF (n = 31) | p | ||
| Modified QUALIN score | D0 | 30.4 ± 8.4 32(25–36) | 30.4 ± 8.5 31.5(23.5–36.5) | 30.4 ± 8.4 32(26–34.5) | 0.99 * | 30.1 ± 9.2 32(25–36) | 29.4 ± 10.1 31(23–36) | 30.8 ± 8.3 32(26–35) | 0.68 * |
| D28 | 32.5 ± 7.3 33.5(26.5–38) | 34.4 ± 6.7 35.5(30–39) | 30.2 ± 7.4 31(24–36) | 0.02 * | 32.4 ± 7.3 33(26–38) | 34.5 ± 6.7 35.5(30–39) | 30.1 ± 7.3 31(24–36) | 0.02 * | |
| ΔD0 − D28 | 2.8 ± 8.9 1.5(−3.5–7) | 4.6 ± 9.4 3(−1–9) | −0.4 ± 7.6 −2.5(−6–4) | 0.03 * | 2.2 ± 8.9 1(−4–7) | 4.8 ± 9.4 3(−1–9) | −0.52 ± 7.5 −3(−6–4) | 0.02 * | |
| Skin and Gastrointestinal Symptoms | Total (n = 64) | GMF (n = 33) | CMF (n = 31) | p |
|---|---|---|---|---|
| Skin lesions | ||||
| Yes | 4 (100.0) | 2 (50.0) | 2 (50.0) | 0.85 |
| Atopic dermatitis | ||||
| Yes | 1 (25.0) | 1 (25.0) | 0 (0.0) | 0.24 |
| Rash | ||||
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Dry skin | ||||
| Yes | 3 (75.0) | 1 (25.0) | 2 (50.0) | 0.70 |
| Gastrointestinal symptoms | ||||
| Constipation | ||||
| Yes | 16 (27.6) | 12 (38.7) | 4 (14.8) | 0.042 |
| No | 42 (72.4) | 19 (61.2) | 23 (85.1) | |
| Missing data | 6 | |||
| Regurgitation | ||||
| Yes | 25 (43.1) | 11 (35.4) | 14 (51.8) | 0.20 |
| No | 33 (56.9) | 20 (64.5) | 13 (48.1) | |
| Missing data | 6 | |||
| Frequency of regurgitation | ||||
| Never | 27 (50.9) | 15 (55.5) | 12 (46.1) | 0.60 |
| <50% of feedings | 17 (32.2) | 7 (25.9) | 10 (38.5) | |
| ≥50% of feedings | 3 (5.6) | 1 (3.7) | 2 (7.7) | |
| Every feeding | 6 (11.3) | 4 (14.9) | 2 (7.7) | |
| Missing data | 11 | |||
| Crying during feeding | ||||
| Never | 44 (80.0) | 24 (82.7) | 20 (76.9) | 0.29 |
| <50% of feedings | 8 (14.5) | 3 (10.4) | 5 (19.2) | |
| ≥50% of feedings | 1 (1.8) | 0 (0.0) | 1 (3.9) | |
| Every feeding | 2 (3.7) | 2 (6.9) | 0 (0.0) | |
| Missing data | 9 | |||
| Abdominal distension | ||||
| Yes | 11 (18.9) | 8 (25.8) | 3 (11.1) | 0.15 |
| No | 47 (81.0) | 23 (74.2) | 24 (88.8) | |
| Missing data | 6 | |||
| Colic pain | ||||
| Yes | 11 (18.9) | 14 (42.4) | 11 (35.4) | 0.56 |
| No | 47 (60.9) | 19 (57.5) | 20 (64.5) | |
| Missing data | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, C.; González Serrano, A.; Batard, C.; Seror, E.; Gelwane, G.; Poidvin, A.; Lavallée, I.; Elbez, A.; Brussieux, M.; Prosser, C.; et al. Whole Goat Milk-Based Formula versus Whey-Based Cow Milk Formula: What Formula Do Infants Enjoy More?—A Feasibility, Double-Blind, Randomized Controlled Trial. Nutrients 2023, 15, 4057. https://doi.org/10.3390/nu15184057
Jung C, González Serrano A, Batard C, Seror E, Gelwane G, Poidvin A, Lavallée I, Elbez A, Brussieux M, Prosser C, et al. Whole Goat Milk-Based Formula versus Whey-Based Cow Milk Formula: What Formula Do Infants Enjoy More?—A Feasibility, Double-Blind, Randomized Controlled Trial. Nutrients. 2023; 15(18):4057. https://doi.org/10.3390/nu15184057
Chicago/Turabian StyleJung, Camille, Adolfo González Serrano, Christophe Batard, Elisa Seror, Georges Gelwane, Amélie Poidvin, Isabelle Lavallée, Annie Elbez, Maxime Brussieux, Colin Prosser, and et al. 2023. "Whole Goat Milk-Based Formula versus Whey-Based Cow Milk Formula: What Formula Do Infants Enjoy More?—A Feasibility, Double-Blind, Randomized Controlled Trial" Nutrients 15, no. 18: 4057. https://doi.org/10.3390/nu15184057
APA StyleJung, C., González Serrano, A., Batard, C., Seror, E., Gelwane, G., Poidvin, A., Lavallée, I., Elbez, A., Brussieux, M., Prosser, C., Gallier, S., & Bellaïche, M. (2023). Whole Goat Milk-Based Formula versus Whey-Based Cow Milk Formula: What Formula Do Infants Enjoy More?—A Feasibility, Double-Blind, Randomized Controlled Trial. Nutrients, 15(18), 4057. https://doi.org/10.3390/nu15184057