
Support from a Best Friend Makes People Eat Less under Stress: Evidence from Two Experiments


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
2.3. Experimental Manipulations
2.4. Food-Related Tasks
3. Results
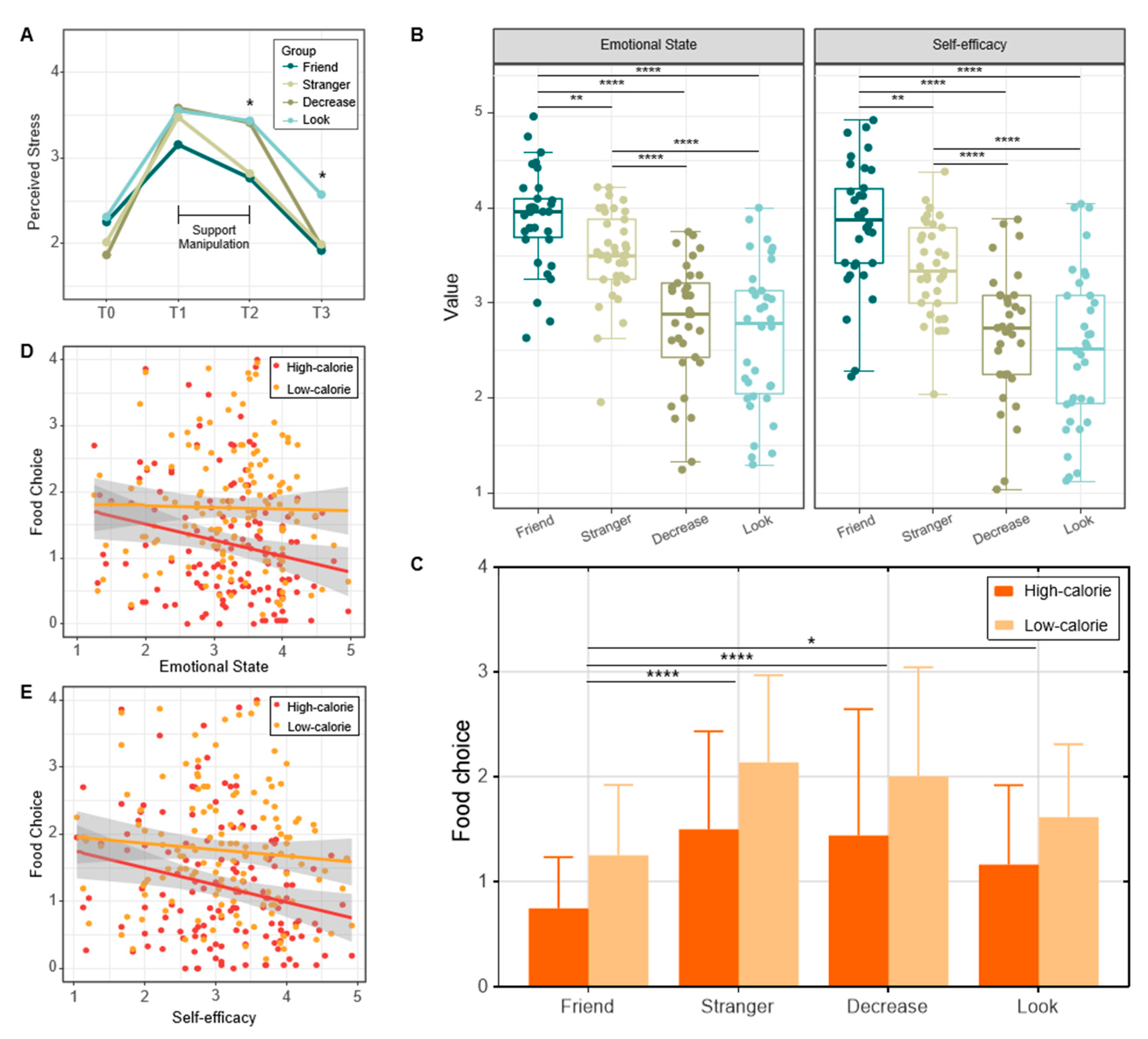
3.1. Experiment 1 Results
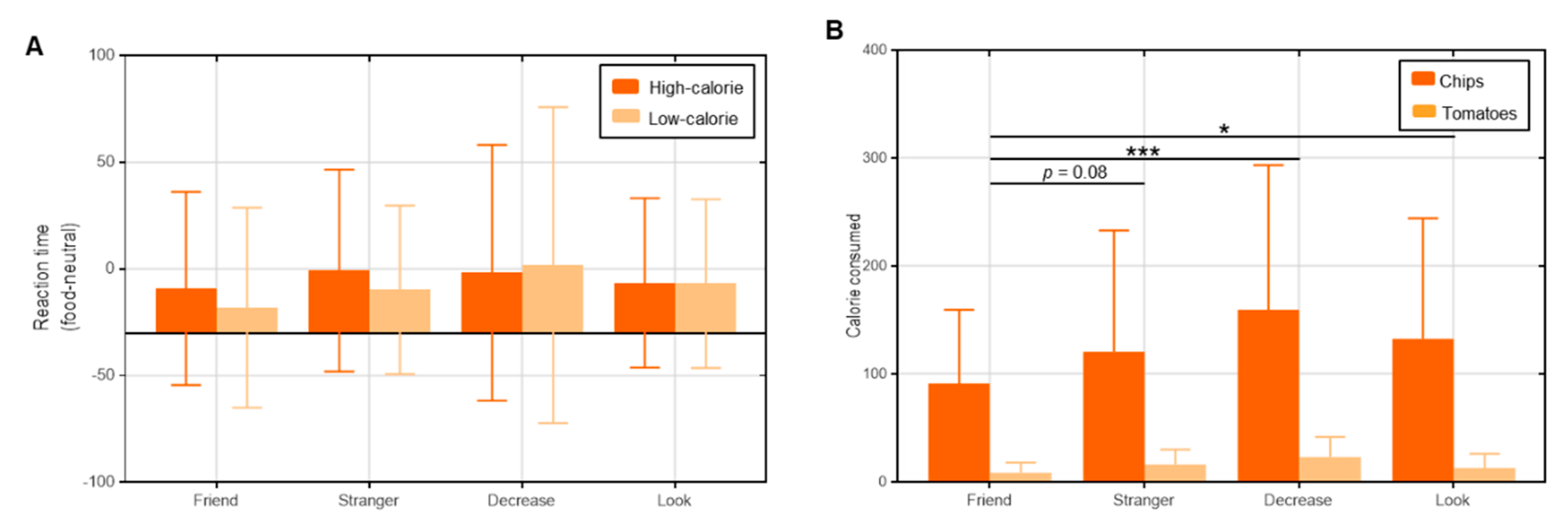
3.2. Experiment 2 Results
4. Discussion
Limitations and Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rutters, F.; Nieuwenhuizen, A.G.; Lemmens, S.G.; Born, J.M.; Westerterp-Plantenga, M.S. Acute stress-related changes in eating in the absence of hunger. Obesity 2009, 17, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.S.; Kumsta, R.; Von Dawans, B.; Monakhov, M.; Ebstein, R.P.; Heinrichs, M. Common oxytocin receptor gene (OXTR) polymorphism and social support interact to reduce stress in humans. Proc. Natl. Acad. Sci. USA 2011, 108, 19937–19942. [Google Scholar] [CrossRef]
- Finch, L.E.; Cummings, J.R.; Tomiyama, A.J. Cookie or clementine? Psychophysiological stress reactivity and recovery after eating healthy and unhealthy comfort foods. Psychoneuroendocrinology 2019, 107, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, A.J.; Dallman, M.F.; Epel, E.S. Comfort food is comforting to those most stressed: Evidence of the chronic stress response network in high stress women. Psychoneuroendocrinology 2011, 36, 1513–1519. [Google Scholar] [CrossRef]
- Geliebter, A.; Aversa, A. Emotional eating in overweight, normal weight, and underweight individuals. Eat. Behav. 2003, 3, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.L.; Byrne, S.M.; La Puma, M.; McLean, N.; Davis, E.A. The onset and course of binge eating in 8-to 13-year-old healthy weight, overweight and obese children. Eat. Behav. 2008, 9, 438–446. [Google Scholar] [CrossRef]
- Wardle, J. Eating style: A validation study of the Dutch Eating Behaviour Questionnaire in normal subjects and women with eating disorders. J. Psychosom. Res. 1987, 31, 161–169. [Google Scholar] [CrossRef]
- Cohen, A.N.; Hammen, C.; Henry, R.M.; Daley, S.E. Effects of stress and social support on recurrence in bipolar disorder. J. Affect. Disord. 2004, 82, 143–147. [Google Scholar] [CrossRef]
- Laitinen, J.; Ek, E.; Sovio, U. Stress-related eating and drinking behavior and body mass index and predictors of this behavior. Prev. Med. 2002, 34, 29–39. [Google Scholar] [CrossRef]
- Raspopow, K.; Matheson, K.; Abizaid, A.; Anisman, H. Unsupportive social interactions influence emotional eating behaviors. The role of coping styles as mediators. Appetite 2013, 62, 143–149. [Google Scholar] [CrossRef]
- Cobb, S. Social support as a moderator of life stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Wilfley, D.E.; MacKenzie, K.R.; Welch, R.R.; Weissman, M.M.; Ayres, V.E. Interpersonal Psychotherapy for Group; Basic Books: New York, NY, USA, 2000. [Google Scholar]
- Wilfley, D.E.; Pike, K.M.; Striegel-Moore, R.H. Toward an integrated model of risk for binge eating disorder. J. Gend. Cult. Health 1997, 2, 1–32. [Google Scholar]
- Ansell, E.B.; Grilo, C.M.; White, M.A. Examining the interpersonal model of binge eating and loss of control over eating in women. Int. J. Eat. Disord. 2012, 45, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.Y.; Gordon, K.H. The effects of social support and stress perception on bulimic behaviors and unhealthy food consumption. Eat. Behav. 2016, 22, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Freeman, W.H.; Lightsey, R. Self-Efficacy: The Exercise of Control; Springer: Berlin/Heidelberg, Germany, 1999. [Google Scholar]
- Chang, M.-W.; Schaffir, J.; Brown, R.; Wegener, D.T. Mediation by self-efficacy in the relation between social support and dietary intake in low-income postpartum women who were overweight or obese. Appetite 2019, 140, 248–254. [Google Scholar] [CrossRef]
- Ossewaarde, L.; Qin, S.; Van Marle, H.J.; van Wingen, G.A.; Fernández, G.; Hermans, E.J. Stress-induced reduction in reward-related prefrontal cortex function. NeuroImage 2011, 55, 345–352. [Google Scholar] [CrossRef]
- Diamond, J.; Renfrew, C. Guns, germs, and steel: The fates of human societies. Nature 1997, 386, 339. [Google Scholar]
- Lasaleta, J.D.; Sedikides, C.; Vohs, K.D. Nostalgia weakens the desire for money. J. Consum. Res. 2014, 41, 713–729. [Google Scholar] [CrossRef]
- Chang, Y.Y.-C.; Wu, P.-L.; Chiou, W.-B. Thoughts of social distancing experiences affect food intake and hypothetical binge eating: Implications for people in home quarantine during COVID-19. Soc. Sci. Med. 2021, 284, 114218. [Google Scholar] [CrossRef]
- Carver, C.S. Self-regulation of action and affect. In Handbook of Self-Regulation: Research, Theory, and Applications; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Briers, B.; Pandelaere, M.; Dewitte, S.; Warlop, L. Hungry for money: The desire for caloric resources increases the desire for financial resources and vice versa. Psychol. Sci. 2006, 17, 939–943. [Google Scholar] [CrossRef]
- Twenge, J.M.; Baumeister, R.F.; DeWall, C.N.; Ciarocco, N.J.; Bartels, J.M. Social exclusion decreases prosocial behavior. J. Pers. Soc. Psychol. 2007, 92, 56. [Google Scholar] [CrossRef]
- Morawetz, C.; Berboth, S.; Bode, S. With a little help from my friends: The effect of social proximity on emotion regulation-related brain activity. NeuroImage 2021, 230, 117817. [Google Scholar] [CrossRef]
- Pauw, L.S.; Sauter, D.A.; Van Kleef, G.A.; Fischer, A.H. Sense or sensibility? Social sharers’ evaluations of socio-affective vs. cognitive support in response to negative emotions. Cogn. Emot. 2018, 32, 1247–1264. [Google Scholar] [CrossRef] [PubMed]
- Plessow, F.; Fischer, R.; Kirschbaum, C.; Goschke, T. Inflexibly focused under stress: Acute psychosocial stress increases shielding of action goals at the expense of reduced cognitive flexibility with increasing time lag to the stressor. J. Cogn. Neurosci. 2011, 23, 3218–3227. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.L.; Miles, E.; Sheeran, P.J. Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychol. Bull. 2012, 138, 775. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Chen, X.; Zeng, W.; Xiao, M.; Liu, Y.; Gao, X.; Chen, H. Associations of harsh, unpredictable environment, amygdala connectivity and overeating for children. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2023, 120, 110644. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.J.; Skunde, M.; Wu, M.; Schnell, K.; Herpertz, S.C.; Bendszus, M.; Herzog, W.; Friederich, H.-C. Neural dissociation of food-and money-related reward processing using an abstract incentive delay task. Soc. Cogn. Affect. Neurosci. 2015, 10, 1113–1120. [Google Scholar] [CrossRef]
- Galvan, A.; Hare, T.A.; Davidson, M.; Spicer, J.; Glover, G.; Casey, B. The role of ventral frontostriatal circuitry in reward-based learning in humans. J. Neurosci. 2005, 25, 8650–8656. [Google Scholar] [CrossRef]
- O’Doherty, J.P.; Buchanan, T.W.; Seymour, B.; Dolan, R.J. Predictive neural coding of reward preference involves dissociable responses in human ventral midbrain and ventral striatum. Neuron 2006, 49, 157–166. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Verheijden, M.; Bakx, J.; Van Weel, C.; Koelen, M.; Van Staveren, W. Role of social support in lifestyle-focused weight management interventions. Eur. J. Clin. Nutr. 2005, 59, S179–S186. [Google Scholar] [CrossRef] [PubMed]
- Gruber, K.J. Social support for exercise and dietary habits among college students. Adolescence 2008, 43, 557–575. [Google Scholar] [PubMed]
- Kim, C.; McEwen, L.N.; Kieffer, E.C.; Herman, W.H.; Piette, J.D. Self-efficacy, social support, and associations with physical activity and body mass index among women with histories of gestational diabetes mellitus. Diabetes Educ. 2008, 34, 719–728. [Google Scholar] [CrossRef]
- Lasaleta, J.D.; Werle, C.O.; Yamim, A.P. Nostalgia makes people eat healthier. Appetite 2021, 162, 105187. [Google Scholar] [CrossRef] [PubMed]
- Knutson, B.; Westdorp, A.; Kaiser, E.; Hommer, D. FMRI visualization of brain activity during a monetary incentive delay task. NeuroImage 2000, 12, 20–27. [Google Scholar] [CrossRef]
- Schultz, W. Predictive reward signal of dopamine neurons. J. Neurophysiol. 1998, 80, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Balodis, I.M.; Grilo, C.M.; Kober, H.; Worhunsky, P.D.; White, M.A.; Stevens, M.C.; Pearlson, G.D.; Potenza, M.N. A pilot study linking reduced fronto–striatal recruitment during reward processing to persistent bingeing following treatment for binge-eating disorder. Int. J. Eat. Disord. 2014, 47, 376–384. [Google Scholar] [CrossRef]
- Ehrlich, S.; Geisler, D.; Ritschel, F.; King, J.A.; Seidel, M.; Boehm, I.; Breier, M.; Clas, S.; Weiss, J.; Marxen, M.; et al. Elevated cognitive control over reward processing in recovered female patients with anorexia nervosa. J. Psychiatry Neurosci. 2015, 40, 307–315. [Google Scholar] [CrossRef]
- Murao, E.; Sugihara, G.; Isobe, M.; Noda, T.; Kawabata, M.; Matsukawa, N.; Takahashi, H.; Murai, T.; Noma, S. Differences in neural responses to reward and punishment processing between anorexia nervosa subtypes: An fMRI study. Psychiatry Clin. Neurosci. 2017, 71, 647–658. [Google Scholar] [CrossRef]
- Balodis, I.M.; Kober, H.; Worhunsky, P.D.; White, M.A.; Stevens, M.C.; Pearlson, G.D.; Sinha, R.; Grilo, C.M.; Potenza, M.N. Monetary reward processing in obese individuals with and without binge eating disorder. Biol. Psychiatry 2013, 73, 877–886. [Google Scholar] [CrossRef]
- Simon, J.J.; Skunde, M.; Walther, S.; Bendszus, M.; Herzog, W.; Friederich, H.-C. Neural signature of food reward processing in bulimic-type eating disorders. Soc. Cogn. Affect. Neurosci. 2016, 11, 1393–1401. [Google Scholar] [CrossRef] [PubMed]
- Tomova, L.; Wang, K.L.; Thompson, T.; Matthews, G.A.; Takahashi, A.; Tye, K.M.; Saxe, R. Acute social isolation evokes midbrain craving responses similar to hunger. Nat. Neurosci. 2020, 23, 1597–1605. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Reynolds-Malear, J.B.; Cordero, E. Disordered Eating and the Use of Unhealthy Weight Control Methods in College Students: 1995, 2002, and 2008. Eat. Disord. 2011, 19, 323–334. [Google Scholar] [CrossRef]
- Jackson, T. Relationships between perceived close social support and health practices within community samples of American women and men. J. Psychol. 2006, 140, 229–246. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.; Persson, L.-O.; Sjöström, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. 2000, 24, 1715–1725. [Google Scholar] [CrossRef]
- Wang, X.; Wang, X.; Ma, H. Handbook of Mental Health Assessment Scale; China Mental Health Press: Beijing, China, 1999; pp. 131–133. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef]
- Luszczynska, A.; Scholz, U.; Schwarzer, R. The general self-efficacy scale: Multicultural validation studies. J. Psychol. 2005, 139, 439–457. [Google Scholar] [CrossRef]
- Torrubia, R.; Avila, C.; Moltó, J.; Caseras, X. The Sensitivity to Punishment and Sensitivity to Reward Questionnaire (SPSRQ) as a measure of Gray’s anxiety and impulsivity dimensions. Personal. Individ. Differ. 2012, 31, 837–862. [Google Scholar] [CrossRef]
- Xie, X.; Bratec, S.M.; Schmid, G.; Meng, C.; Doll, A.; Wohlschläger, A.; Finke, K.; Förstl, H.; Zimmer, C.; Pekrun, R.; et al. How do you make me feel better? Social cognitive emotion regulation and the default mode network. NeuroImage 2016, 134, 270–280. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Friend | Stranger | Decrease | Look | Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | F | p | |
| Age | 18.01–25.22 | 20.34 | 1.33 | 18.44–23.86 | 21.47 | 1.48 | 0.93–23.94 | 19.91 | 3.72 | 18.32–27.9 | 21.06 | 1.73 | 3.33 | 0.02 |
| Hunger (z-score) | 0–2.92 | −0.11 | 1 | 0–2.97 | 0.07 | 0.99 | 0–2.97 | −0.09 | 1.02 | 0–2.92 | 0.18 | 1.02 | 0.66 | 0.57 |
| BMI | 15.58–28.93 | 21.09 | 3.41 | 15.62–31.56 | 21.43 | 3.24 | 14.7–32.92 | 20.94 | 3.73 | 16.33–28.04 | 21.03 | 2.45 | 0.15 | 0.92 |
| MSPSS | 2–4 | 2.94 | 0.64 | 1.58–3.41 | 2.63 | 0.49 | 0.41–3.58 | 2.58 | 0.77 | 2–4 | 2.73 | 0.66 | 2.01 | 0.11 |
| PSS | 2.07–3.71 | 2.77 | 0.41 | 1.71–4.14 | 2.79 | 0.50 | 1.92–4.35 | 2.81 | 0.58 | 1.92–3.85 | 2.80 | 0.48 | 0.03 | 0.98 |
| NA (trait) | 1.72–3.81 | 2.58 | 0.57 | 1.36–3.81 | 2.16 | 0.61 | 1.45–4.18 | 2.31 | 0.63 | 1.27–3.81 | 2.37 | 0.60 | 2.81 | 0.04 |
| PA (trait) | 1.66–4.66 | 3.36 | 0.59 | 1.77–4.44 | 3.19 | 0.65 | 1.88–4.55 | 3.15 | 0.65 | 2–4.88 | 3.40 | 0.59 | 1.29 | 0.27 |
| NA (T0) | 1.09–3.81 | 2.11 | 0.62 | 1–3.63 | 1.77 | 0.63 | 1–3 | 1.72 | 0.48 | 1–4.09 | 2.02 | 0.73 | 3.13 | 0.02 |
| PA (T0) | 1.66–4 | 3.20 | 0.51 | 1.55–4.44 | 3 | 0.75 | 1.77–4 | 2.98 | 0.52 | 1.55–4 | 2.95 | 0.66 | 1.11 | 0.34 |
| Self-efficacy | 2.4–4.6 | 3.48 | 0.56 | 2.4–4.1 | 3.42 | 0.51 | 1.4–4.7 | 3.29 | 0.72 | 2.3–4.4 | 3.44 | 0.43 | 0.70 | 0.55 |
| EE | 1.33–3.66 | 2.17 | 0.58 | 1–4 | 2.54 | 0.65 | 1–4 | 2.37 | 0.81 | 1–4 | 2.39 | 0.74 | 1.67 | 0.17 |
| UE | 1.22–3 | 2.28 | 0.44 | 1.33–3 | 2.42 | 0.37 | 1.66–3.44 | 2.31 | 0.44 | 1.22–3.55 | 2.42 | 0.62 | 0.81 | 0.49 |
| CR | 1.28–3.42 | 2.19 | 0.45 | 1.16–3.83 | 2.58 | 0.63 | 1–3.83 | 2.45 | 0.74 | 1.28–3 | 2.35 | 0.53 | 2.58 | 0.06 |
| Characteristics | Friend | Stranger | Decrease | Look | Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | F | p | |
| Age | 18.82–23.61 | 21.20 | 1.37 | 18.44–23.86 | 21.43 | 1.51 | 18.59–23.54 | 20.37 | 1.35 | 18.57–24.36 | 21.22 | 1.52 | 3.45 | 0.02 |
| Hunger (z-score) | −1.58–1.32 | −0.26 | 0.90 | −1.18–1.79 | 0.10 | 0.99 | −1.18–1.79 | −0.13 | 1.03 | −1.58–1.32 | 0.18 | 1.05 | 1.42 | 0.24 |
| BMI | 16.73–32.49 | 21.07 | 3.47 | 15.63–31.56 | 21.48 | 3.29 | 15.63–30.12 | 21.05 | 3.19 | 17.01–24.25 | 20.10 | 1.80 | 1.26 | 0.29 |
| MSPSS | 0.83–3.67 | 2.74 | 0.56 | 1.58–3.42 | 2.63 | 0.51 | 0.42–3.58 | 2.64 | 0.79 | 1.17–3.75 | 2.57 | 0.65 | 0.46 | 0.71 |
| PSS | 1.86–3.79 | 2.79 | 0.52 | 1.71–4.14 | 2.80 | 0.52 | 1.93–4.36 | 2.74 | 0.59 | 1.93–3.57 | 2.69 | 0.44 | 0.33 | 0.80 |
| NA (trait) | 1.18–3.91 | 2.45 | 0.72 | 1.36–3.82 | 2.17 | 0.63 | 1.45–4.18 | 2.24 | 0.62 | 1.27–3.91 | 2.44 | 0.66 | 1.57 | 0.20 |
| PA (trait) | 1.67–4.22 | 3.12 | 0.60 | 1.78–4.44 | 3.18 | 0.67 | 1.89–4.56 | 3.22 | 0.66 | 2–5 | 3.30 | 0.65 | 0.49 | 0.69 |
| NA (T0) | 1–3.73 | 1.83 | 0.79 | 1–3.64 | 1.78 | 0.65 | 1–3 | 1.66 | 0.50 | 1–3.17 | 1.78 | 0.57 | 0.40 | 0.75 |
| PA (T0) | 1.44–4.44 | 2.89 | 0.80 | 1.56–4.44 | 3.02 | 0.77 | 1.78–4 | 3.01 | 0.55 | 1.33–4.33 | 3.20 | 0.68 | 1.12 | 0.34 |
| Self-efficacy | 2.1–4.4 | 3.39 | 0.55 | 2.4–4.1 | 3.44 | 0.51 | 1.4–4.7 | 3.40 | 0.71 | 2.3–4.1 | 3.43 | 0.48 | 0.05 | 0.99 |
| SR | 0.29–0.96 | 0.59 | 0.17 | 0.21–0.83 | 0.55 | 0.14 | 0.21–0.83 | 0.53 | 0.14 | 0.21–0.88 | 0.53 | 0.17 | 1.13 | 0.34 |
| EE | 1.33–4 | 2.41 | 0.66 | 1–4 | 2.52 | 0.66 | 1–4 | 2.43 | 0.79 | 1–4 | 2.17 | 0.81 | 1.40 | 0.25 |
| UE | 1.56–3.56 | 2.31 | 0.54 | 1.33–3 | 2.42 | 0.38 | 1.67–3.44 | 2.36 | 0.43 | 1.11–3.44 | 2.03 | 0.54 | 4.48 | 0.00 |
| CR | 1–3.29 | 2.10 | 0.59 | 1.17–3.83 | 2.59 | 0.65 | 1–3.83 | 2.52 | 0.69 | 0.86–2.86 | 1.81 | 0.47 | 12.49 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, M.; Luo, Y.; Zeng, W.; Chen, H. Support from a Best Friend Makes People Eat Less under Stress: Evidence from Two Experiments. Nutrients 2023, 15, 3898. https://doi.org/10.3390/nu15183898
Xiao M, Luo Y, Zeng W, Chen H. Support from a Best Friend Makes People Eat Less under Stress: Evidence from Two Experiments. Nutrients. 2023; 15(18):3898. https://doi.org/10.3390/nu15183898
Chicago/Turabian StyleXiao, Mingyue, Yijun Luo, Weiyu Zeng, and Hong Chen. 2023. "Support from a Best Friend Makes People Eat Less under Stress: Evidence from Two Experiments" Nutrients 15, no. 18: 3898. https://doi.org/10.3390/nu15183898
APA StyleXiao, M., Luo, Y., Zeng, W., & Chen, H. (2023). Support from a Best Friend Makes People Eat Less under Stress: Evidence from Two Experiments. Nutrients, 15(18), 3898. https://doi.org/10.3390/nu15183898