
Fatty Acids Profile and the Relevance of Membranes as the Target of Nutrition-Based Strategies in Atopic Dermatitis: A Narrative Review

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
3. Epidemiology of Atopic Dermatitis
4. Genetic Aspects
5. Molecular Aspects
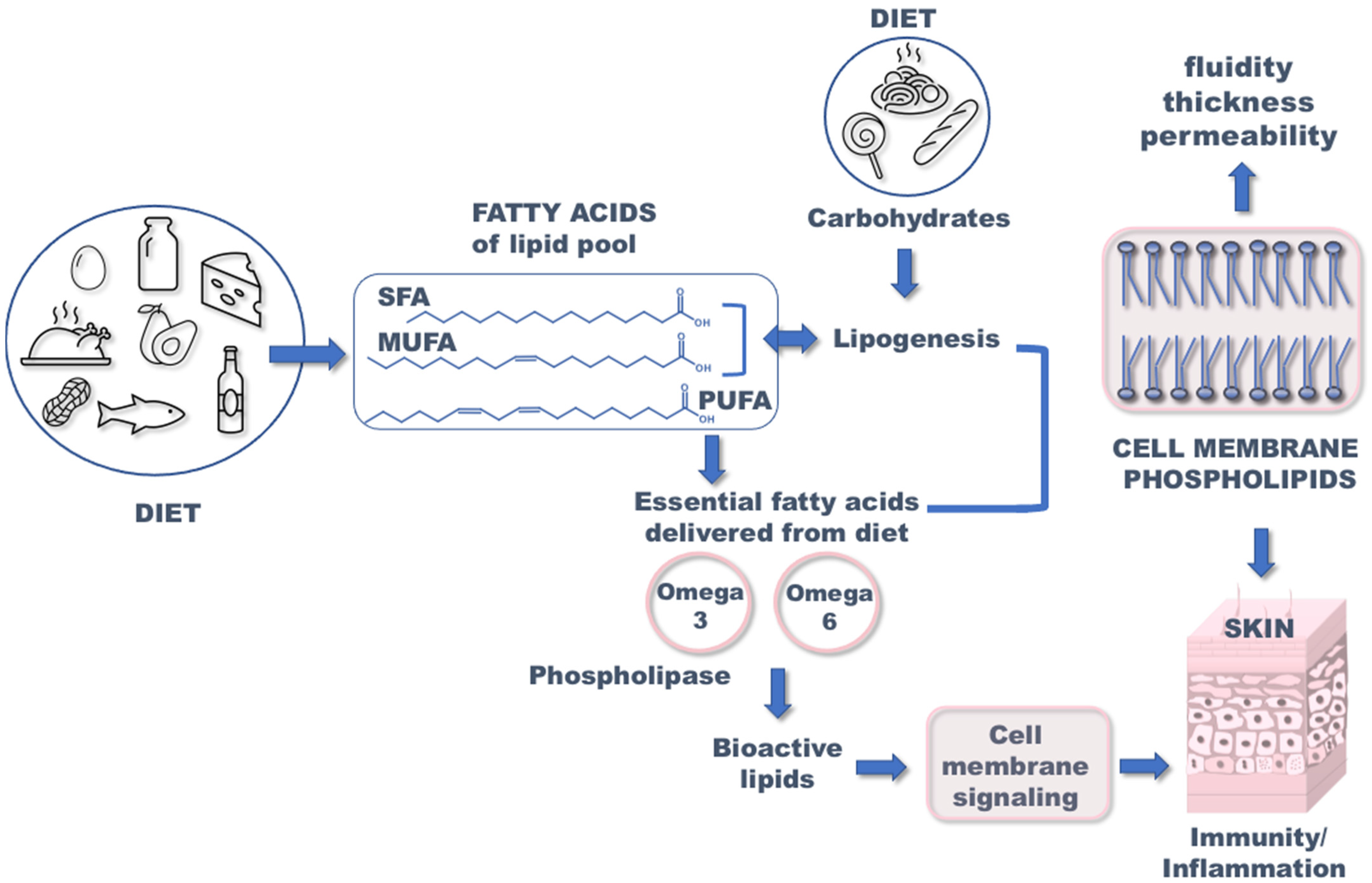
6. Diet and Atopic Dermatitis
6.1. Effect of Monounsaturated Fatty Acids on Atopic Dermatitis
6.2. Effect of Polyunsaturated Fatty Acids on Atopic Dermatitis
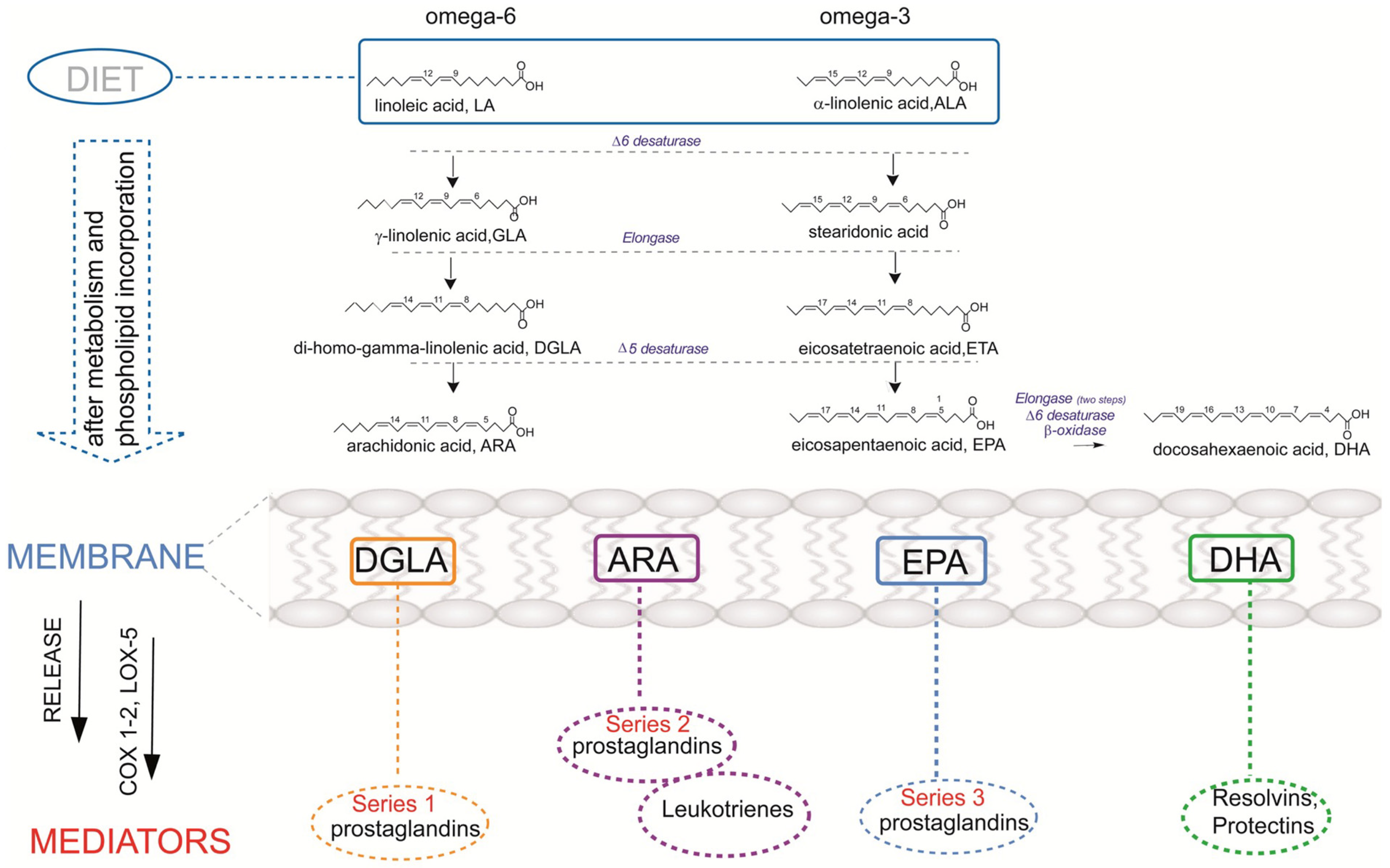
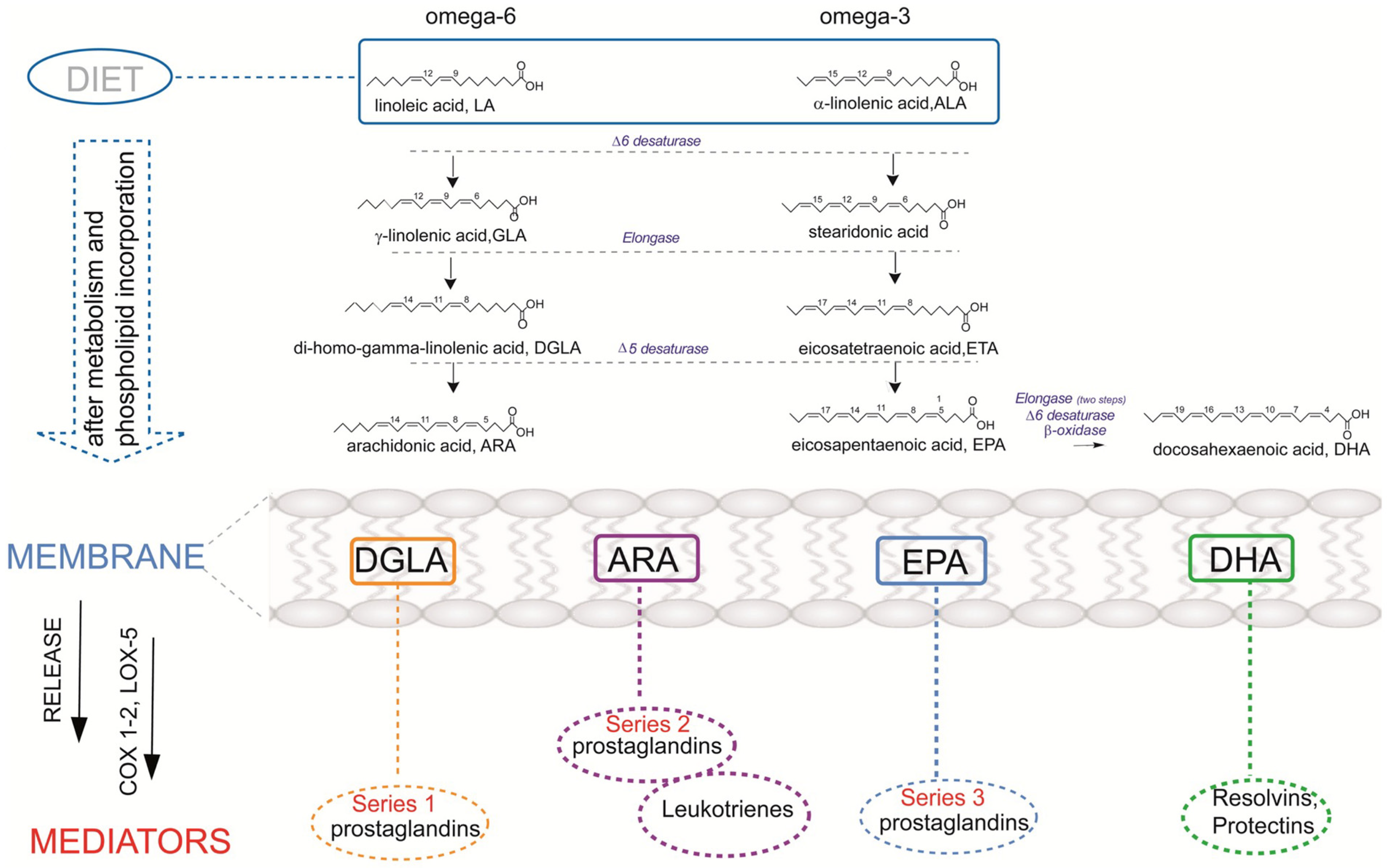
6.3. Different Dietary Sources of Omega-6 and Omega-3
- (1)
- Competition on the enzymatic cascade by omega-3 PUFAs that inhibits the omega-6 AA formation and diminishes the contribution to PGE2 formation (Figure 1);
- (2)
6.4. Effect of Trans Fatty Acids on Atopic Dermatitis
7. Fatty Acid-Based Membrane Lipidomics in Atopic Dermatitis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhattacharya, N.; Sato, W.J.; Kelly, A.; Ganguli-Indra, G.; Indra, A.K. Epidermal Lipids: Key Mediators of Atopic Dermatitis Pathogenesis. Trends. Mol. Med. 2019, 25, 551–562. [Google Scholar] [CrossRef]
- Tomczak, H.; Wróbel, J.; Jenerowicz, D.; Sadowska-Przytocka, A.; Wachal, M.; Adamski, Z.; Czarnecka-Operacz, M.M. The Role of Staphylococcus Aureus in Atopic Dermatitis: Microbiological and Immunological Implications. Postepy Dermatol. Allergol. 2019, 36, 485–491. [Google Scholar] [CrossRef]
- Barman, M.; Stråvik, M.; Broberg, K.; Sandin, A.; Wold, A.E.; Sandberg, A.-S. Proportions of Polyunsaturated Fatty Acids in Umbilical Cord Blood at Birth Are Related to Atopic Eczema Development in the First Year of Life. Nutrients 2021, 13, 3779. [Google Scholar] [CrossRef]
- Sala-Vila, A.; Miles, E.A.; Calder, P.C. Fatty Acid Composition Abnormalities in Atopic Disease: Evidence Explored and Role in the Disease Process Examined. Clin. Exp. Allergy 2008, 38, 1432–1450. [Google Scholar] [CrossRef]
- Miles, E.A.; Calder, P.C. Can Early Omega-3 Fatty Acid Exposure Reduce Risk of Childhood Allergic Disease? Nutrients 2017, 9, 784. [Google Scholar] [CrossRef]
- Kaźmierska, A.; Bolesławska, I.; Polańska, A.; Dańczak-Pazdrowska, A.; Jagielski, P.; Drzymała-Czyż, S.; Adamski, Z.; Przysławski, J. Effect of Evening Primrose Oil Supplementation on Selected Parameters of Skin Condition in a Group of Patients Treated with Isotretinoin—A Randomized Double-Blind Trial. Nutrients 2022, 14, 2980. [Google Scholar] [CrossRef]
- Spector, A.A.; Kiser, R.E.; Denning, G.M.; Koh, S.-W.; DeBault, L.E. Modification of the Fatty Acid Composition of Cultured Human Fibroblasts. J. Lipid Res. 1979, 20, 536–547. [Google Scholar] [CrossRef]
- de Carvalho, C.C.C.R.; Caramujo, M.J. The Various Roles of Fatty Acids. Molecules 2018, 23, 2583. [Google Scholar] [CrossRef]
- Ferreri, C.; Chatgilialoglu, C. Membrane Lipidomics for Personalized Health; John Wiley & Sons: Hoboken, NJ, USA, 2015; ISBN 1118540417. [Google Scholar]
- Yang, M.; Zhou, M.; Song, L. A Review of Fatty Acids Influencing Skin Condition. J. Cosmet. Dermatol. 2020, 19, 3199–3204. [Google Scholar] [CrossRef]
- Cui, L.; Jia, Y.; Cheng, Z.; Gao, Y.; Zhang, G.; Li, J.; He, C. Advancements in the Maintenance of Skin Barrier/Skin Lipid Composition and the Involvement of Metabolic Enzymes. J. Cosmet. Dermatol. 2016, 15, 549–558. [Google Scholar] [CrossRef]
- Coomans de Brachène, A.; Dif, N.; de Rocca Serra, A.; Bonnineau, C.; Velghe, A.I.; Larondelle, Y.; Tyteca, D.; Demoulin, J. PDGF-induced Fibroblast Growth Requires Monounsaturated Fatty Acid Production by Stearoyl-CoA Desaturase. FEBS Open Bio. 2017, 7, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Alatibi, K.I.; Hagenbuchner, J.; Wehbe, Z.; Karall, D.; Ausserlechner, M.J.; Vockley, J.; Spiekerkoetter, U.; Grünert, S.C.; Tucci, S. Different Lipid Signature in Fibroblasts of Long-Chain Fatty Acid Oxidation Disorders. Cells 2021, 10, 1239. [Google Scholar] [CrossRef] [PubMed]
- Kendall, A.C.; Pilkington, S.M.; Massey, K.A.; Sassano, G.; Rhodes, L.E.; Nicolaou, A. Distribution of Bioactive Lipid Mediators in Human Skin. J. Invest. Dermatol. 2015, 135, 1510–1520. [Google Scholar] [CrossRef] [PubMed]
- Kendall, A.C.; Nicolaou, A. Bioactive Lipid Mediators in Skin Inflammation and Immunity. Prog Lipid Res 2013, 52, 141–164. [Google Scholar] [CrossRef]
- Williams, H.; Flohr, C. How Epidemiology Has Challenged 3 Prevailing Concepts about Atopic Dermatitis. J. Allergy Clin. Immunol. 2006, 118, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Stewart, A.; von Mutius, E.; Cookson, W.; Anderson, H.R.; of Asthma, I.S. Is Eczema Really on the Increase Worldwide? J. Allergy Clin. Immunol. 2008, 121, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, T.; Vieluf, D.; Behrendt, H.; Kramer, U.; Ring, J. Atopic Eczema and Other Manifestations of Atopy: Results of a Study in East and West Germany. Allergy 1996, 51, 532–539. [Google Scholar] [CrossRef]
- Strachan, D.P. Hay Fever, Hygiene, and Household Size. BMJ Br. Med. J. 1989, 299, 1259. [Google Scholar] [CrossRef]
- von Kobyletzki, L.B.; Bornehag, C.G.; Breeze, E.; Larsson, M.; Lindström, C.B.; Svensson, Å. Factors Associated with Remission of Eczema in Children: A Population-Based Follow-up Study. Acta Derm. Venereol. 2014, 94, 179–184. [Google Scholar] [CrossRef]
- Kim, J.; Kim, B.E.; Leung, D.Y.M. Pathophysiology of Atopic Dermatitis: Clinical Implications. Allergy Asthma Proc. 2019, 40, 84. [Google Scholar] [CrossRef]
- Ruzicka, T.; Ring, J.; Przybilla, B. Handbook of Atopic Eczema; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013; ISBN 3662026716. [Google Scholar]
- Raimondo, A.; Lembo, S. Atopic Dermatitis: Epidemiology and Clinical Phenotypes. Dermatol Pr. Concept 2021, 11, e2021146. [Google Scholar] [CrossRef] [PubMed]
- Odhiambo, J.A.; Williams, H.C.; Clayton, T.O.; Robertson, C.F.; Asher, M.I.; Group, I.P.T.S. Global Variations in Prevalence of Eczema Symptoms in Children from ISAAC Phase Three. J. Allergy Clin. Immunol. 2009, 124, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Kiiski, V.; Salava, A.; Susitaival, P.; Barnhill, S.; Remitz, A.; Heliovaara, M. Atopic Dermatitis in Adults: A Population-based Study in Finland. Int. J. Dermatol. 2022, 61, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Mohr, N.; Naatz, M.; Zeervi, L.; Langenbruch, A.; Bieber, T.; Werfel, T.; Wollenberg, A.; Augustin, M. Cost-of-illness of Atopic Dermatitis in Germany: Data from Dermatology Routine Care. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1346–1356. [Google Scholar] [CrossRef]
- Kleyn, C.E.; Barbarot, S.; Reed, C.; Losi, S.; von Arx, L.-B.; Robert, C.; Anderson, P.; Grond, S.; Costanzo, A. Burden of Moderate to Severe Atopic Dermatitis in Adults from France, Italy, and the UK: Patient-Reported Outcomes and Treatment Patterns. Dermatol. Ther. 2022, 12, 1947–1965. [Google Scholar] [CrossRef]
- Naldi, L.; Colombo, P.; Placchesi, E.B.; Piccitto, R.; Chatenoud, L.; la Vecchia, C. Study Design and Preliminary Results from the Pilot Phase of the PraKtis Study: Self-Reported Diagnoses of Selected Skin Diseases in a Representative Sample of the Italian Population. Dermatology 2004, 208, 38–42. [Google Scholar] [CrossRef]
- Barbarot, S.; Auziere, S.; Gadkari, A.; Girolomoni, G.; Puig, L.; Simpson, E.L.; Margolis, D.J.; de Bruin-Weller, M.; Eckert, L. Epidemiology of Atopic Dermatitis in Adults: Results from an International Survey. Allergy 2018, 73, 1284–1293. [Google Scholar] [CrossRef]
- Nutten, S. Atopic Dermatitis: Global Epidemiology and Risk Factors. Ann. Nutr. Metab. 2015, 66, 8–16. [Google Scholar] [CrossRef]
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers. 2018, 4, 1. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, S.W.; Yon, D.K.; Ha, E.K.; Jee, H.M.; Sung, M.; Sim, H.J.; Yoon, J.W.; Choi, S.; Shin, Y.H. Association of Serum Lipid Parameters with the SCORAD Index and Onset of Atopic Dermatitis in Children. Pediatr. Allergy Immunol. 2021, 32, 322–330. [Google Scholar] [CrossRef]
- Chisaguano, A.M.; Montes, R.; Pérez-Berezo, T.; Castellote, A.I.; Guerendiain, M.; Bustamante, M.; Morales, E.; García-Esteban, R.; Sunyer, J.; Franch, À. Gene Expression of Desaturase (FADS1 and FADS2) and Elongase (ELOVL5) Enzymes in Peripheral Blood: Association with Polyunsaturated Fatty Acid Levels and Atopic Eczema in 4-Year-Old Children. PLoS ONE 2013, 8, e78245. [Google Scholar] [CrossRef] [PubMed]
- Al-Shobaili, H.A.; Ahmed, A.A.; Alnomair, N.; Alobead, Z.A.; Rasheed, Z. Molecular Genetic of Atopic Dermatitis: An Update. Int. J. Health Sci. (Qassim) 2016, 10, 96. [Google Scholar] [CrossRef] [PubMed]
- Nedoszytko, B.; Reszka, E.; Gutowska-Owsiak, D.; Trzeciak, M.; Lange, M.; Jarczak, J.; Niedoszytko, M.; Jablonska, E.; Romantowski, J.; Strapagiel, D. Genetic and Epigenetic Aspects of Atopic Dermatitis. Int. J. Mol. Sci. 2020, 21, 6484. [Google Scholar] [CrossRef] [PubMed]
- Margolis, D.J.; Apter, A.J.; Gupta, J.; Hoffstad, O.; Papadopoulos, M.; Campbell, L.E.; Sandilands, A.; McLean, W.H.I.; Rebbeck, T.R.; Mitra, N. The Persistence of Atopic Dermatitis and Filaggrin (FLG) Mutations in a US Longitudinal Cohort. J. Allergy Clin. Immunol. 2012, 130, 912–917. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.; Akiyama, M.; Nemoto-Hasebe, I.; Nomura, T.; Sandilands, A.; Chao, S.; Lee, J.; Sheu, H.; McLean, W.H.I.; Shimizu, H. Analysis of Taiwanese Ichthyosis Vulgaris Families Further Demonstrates Differences in FLG Mutations between European and Asian Populations. Br. J. Dermatol. 2009, 161, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.N.A.; Irvine, A.D.; Terron-Kwiatkowski, A.; Zhao, Y.; Liao, H.; Lee, S.P.; Goudie, D.R.; Sandilands, A.; Campbell, L.E.; Smith, F.J.D. Common Loss-of-Function Variants of the Epidermal Barrier Protein Filaggrin Are a Major Predisposing Factor for Atopic Dermatitis. Nat. Genet 2006, 38, 441–446. [Google Scholar] [CrossRef]
- Watson, W.; Kapur, S. Atopic Dermatitis. Allergy, Asthma & Clinical Immunology. Eczema (Atopic Dermat.) Treat. 2011, 7, 17. [Google Scholar]
- Martin, M.J.; Estravís, M.; García-Sánchez, A.; Dávila, I.; Isidoro-García, M.; Sanz, C. Genetics and Epigenetics of Atopic Dermatitis: An Updated Systematic Review. Genes 2020, 11, 442. [Google Scholar] [CrossRef]
- Stemmler, S.; Hoffjan, S. Trying to Understand the Genetics of Atopic Dermatitis. Mol. Cell Probes 2016, 30, 374–385. [Google Scholar] [CrossRef]
- Rzehak, P.; Heinrich, J.; Klopp, N.; Schaeffer, L.; Hoff, S.; Wolfram, G.; Illig, T.; Linseisen, J. Evidence for an Association between Genetic Variants of the Fatty Acid Desaturase 1 Fatty Acid Desaturase 2 (FADS1 FADS2) Gene Cluster and the Fatty Acid Composition of Erythrocyte Membranes. Br. J. Nutr. 2008, 101, 20–26. [Google Scholar] [CrossRef]
- Rzehak, P.; Thijs, C.; Standl, M.; Mommers, M.; Glaser, C.; Jansen, E.; Klopp, N.; Koppelman, G.H.; Singmann, P.; Postma, D.S. Variants of the FADS1 FADS2 Gene Cluster, Blood Levels of Polyunsaturated Fatty Acids and Eczema in Children within the First 2 Years of Life. PLoS ONE 2010, 5, e13261. [Google Scholar] [CrossRef] [PubMed]
- Tanjung, C.; Rzehak, P.; Sudoyo, H.; Mansyur, M.; Munasir, Z.; Immanuel, S.; Irawan, R.; Reischl, E.; Demmelmair, H.; Hadinegoro, S.R. The Association of Fatty Acid Desaturase Gene Polymorphisms on Long-Chain Polyunsaturated Fatty Acid Composition in Indonesian Infants. Am. J. Clin. Nutr. 2018, 108, 1135–1144. [Google Scholar] [CrossRef]
- Lattka, E.; Klopp, N.; Demmelmair, H.; Klingler, M.; Heinrich, J.; Koletzko, B. Genetic Variations in Polyunsaturated Fatty Acid Metabolism–Implications for Child Health? Ann. Nutr. Metab. 2012, 60, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Standl, M.; Sausenthaler, S.; Lattka, E.; Koletzko, S.; Bauer, C.; Wichmann, H.; von Berg, A.; Berdel, D.; Krämer, U.; Schaaf, B. FADS Gene Variants Modulate the Effect of Dietary Fatty Acid Intake on Allergic Diseases in Children. Clini. Exp. Allergy 2011, 41, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Conway, M.C.; McSorley, E.M.; Mulhern, M.S.; Strain, J.J.; van Wijngaarden, E.; Yeates, A.J. Influence of Fatty Acid Desaturase (FADS) Genotype on Maternal and Child Polyunsaturated Fatty Acids (PUFA) Status and Child Health Outcomes: A Systematic Review. Nutr. Rev. 2020, 78, 627–646. [Google Scholar] [CrossRef]
- Simon, D.; Eng, P.A.; Borelli, S.; Kägi, R.; Zimmermann, C.; Zahner, C.; Drewe, J.; Hess, L.; Ferrari, G.; Lautenschlager, S. Gamma-Linolenic Acid Levels Correlate with Clinical Efficacy of Evening Primrose Oil in Patients with Atopic Dermatitis. Adv. Ther. 2014, 31, 180–188. [Google Scholar] [CrossRef]
- Schaeffer, L.; Gohlke, H.; Müller, M.; Heid, I.M.; Palmer, L.J.; Kompauer, I.; Demmelmair, H.; Illig, T.; Koletzko, B.; Heinrich, J. Common Genetic Variants of the FADS1 FADS2 Gene Cluster and Their Reconstructed Haplotypes Are Associated with the Fatty Acid Composition in Phospholipids. Hum. Mol. Genet. 2006, 15, 1745–1756. [Google Scholar] [CrossRef]
- Singmann, P.; Rzehak, P.; Berdel, D.; Wichmann, H.E.; Heinrich, J. No Association between FADS Polymorphisms and Atopic Diseases in Children from the GINI and LISA Birth Cohorts. Allergy 2010, 65, 1627–1629. [Google Scholar] [CrossRef]
- Standl, M.; Sausenthaler, S.; Lattka, E.; Koletzko, S.; Bauer, C.; Wichmann, H.; Von Berg, A.; Berdel, D.; Krämer, U.; Schaaf, B. FADS Gene Cluster Modulates the Effect of Breastfeeding on Asthma. Results from the GINIplus and LISAplus Studies. Allergy 2012, 67, 83–90. [Google Scholar] [CrossRef]
- Barman, M.; Nilsson, S.; Torinsson Naluai, Å.; Sandin, A.; Wold, A.E.; Sandberg, A.-S. Single Nucleotide Polymorphisms in the FADS Gene Cluster but Not the ELOVL2 Gene Are Associated with Serum Polyunsaturated Fatty Acid Composition and Development of Allergy (in a Swedish Birth Cohort). Nutrients 2015, 7, 10100–10115. [Google Scholar] [CrossRef]
- Totté, J.E.E.; van der Feltz, W.T.; Hennekam, M.; van Belkum, A.; van Zuuren, E.J.; Pasmans, S. Prevalence and Odds of Staphylococcus Aureus Carriage in Atopic Dermatitis: A Systematic Review and Meta-analysis. Br. J. Dermatol. 2016, 175, 687–695. [Google Scholar] [CrossRef]
- Incorvaia, C.; Frati, F.; Verna, N.; D’Alò, S.; Motolese, A.; Pucci, S. Allergy and the Skin. Clin. Exp. Immunol. 2008, 153, 27–29. [Google Scholar] [CrossRef]
- Manti, S.; Leonardi, S.; Panasiti, I.; Arrigo, T.; Salpietro, C.; Cuppari, C. Serum IL-10, IL-17 and IL-23 Levels as “Bioumoral Bridges” between Dyslipidemia and Atopy. Cytokine 2017, 99, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Balić, A.; Vlašić, D.; Žužul, K.; Marinović, B.; Bukvić Mokos, Z. Omega-3 versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. Int. J. Mol. Sci. 2020, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.; Meyer, R.W.; Nwaru, B.I.; Roduit, C.; Untersmayr, E.; Adel-Patient, K.; Agache, I.; Agostoni, C.; Akdis, C.A.; Bischoff, S.C. EAACI Position Paper: Influence of Dietary Fatty Acids on Asthma, Food Allergy, and Atopic Dermatitis. Allergy 2019, 74, 1429–1444. [Google Scholar] [CrossRef]
- Venter, C.; Eyerich, S.; Sarin, T.; Klatt, K.C. Nutrition and the Immune System: A Complicated Tango. Nutrients 2020, 12, 818. [Google Scholar] [CrossRef]
- Horrobin, D.F. Essential Fatty Acid Metabolism and Its Modification in Atopic Eczema. Am. J. Clin. Nutr. 2000, 71, 367s–372s. [Google Scholar] [CrossRef]
- Kaur, N.; Chugh, V.; Gupta, A.K. Essential Fatty Acids as Functional Components of Foods-a Review. J. Food Sci. Technol. 2014, 51, 2289–2303. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.-M.; Chiang, B.-L.; Wang, L.-C. Maternal Nutritional Status and Development of Atopic Dermatitis in Their Offspring. Clin. Rev. Allergy Immunol. 2021, 61, 128–155. [Google Scholar] [CrossRef]
- Hoppu, U.; Kalliomäki, M.; Isolauri, E. Maternal Diet Rich in Saturated Fat during Breastfeeding Is Associated with Atopic Sensitization of the Infant. Eur. J. Clin. Nutr. 2000, 54, 702–705. [Google Scholar] [CrossRef]
- Ellwood, P.; Asher, M.I.; García-Marcos, L.; Williams, H.; Keil, U.; Robertson, C.; Nagel, G.; Group, I.P.I.I.I.S. Do Fast Foods Cause Asthma, Rhinoconjunctivitis and Eczema? Global Findings from the International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three. Thorax 2013, 68, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.S.; Wang, J.; Zhang, X.; Zhang, L.; Zhang, H.P.; Wang, L.; Wood, L.G.; Wang, G. Is the Consumption of Fast Foods Associated with Asthma or Other Allergic Diseases? Respirology 2018, 23, 901–913. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, L.; Kragballe, K. Abnormalities in Epidermal Lipid Metabolism in Patients with Atopic Dermatitis. J. Invest. Dermatol. 1991, 96, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Trak-Fellermeier, M.A.; Brasche, S.; Winkler, G.; Koletzko, B.; Heinrich, J. Food and Fatty Acid Intake and Atopic Disease in Adults. Eur. Respir. J. 2004, 23, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, J.; Hölscher, B.; Bolte, G.; Winkler, G. Allergic Sensitization and Diet: Ecological Analysis in Selected European Cities. Eur. Respir. J. 2001, 17, 395–402. [Google Scholar] [CrossRef]
- Mojumdar, E.H.; Helder, R.W.J.; Gooris, G.S.; Bouwstra, J.A. Monounsaturated Fatty Acids Reduce the Barrier of Stratum Corneum Lipid Membranes by Enhancing the Formation of a Hexagonal Lateral Packing. Langmuir 2014, 30, 6534–6543. [Google Scholar] [CrossRef]
- Agrawala, K.; Hassoun, L.A.; Foolad, N.; Borkowski, K.; Pedersen, T.L.; Sivamani, R.K.; Newman, J.W. Effects of Atopic Dermatitis and Gender on Sebum Lipid Mediator and Fatty Acid Profiles. Prostaglandins Leukot Essent Fat. Acids 2018, 134, 7–16. [Google Scholar] [CrossRef]
- Calder, P.C. Long-Chain Fatty Acids and Inflammation. Proc. Nutr. Soc. 2012, 71, 284–289. [Google Scholar] [CrossRef]
- Flohr, C.; Mann, J. New Insights into the Epidemiology of Childhood Atopic Dermatitis. Allergy 2014, 69, 3–16. [Google Scholar] [CrossRef]
- Devereux, G.; Seaton, A. Diet as a Risk Factor for Atopy and Asthma. J. Allergy Clin. Immunol. 2005, 115, 1109–1117. [Google Scholar] [CrossRef]
- Schäfer, L.; Kragballe, K. Supplementation with Evening Primrose Oil in Atopic Dermatitis: Effect on Fatty Acids in Neutrophils and Epidermis. Lipids 1991, 26, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Chatgilialoglu, C.; Ferreri, C.; Melchiorre, M.; Sansone, A.; Torreggiani, A. Lipid Geometrical Isomerism: From Chemistry to Biology and Diagnostics. Chem. Rev. 2014, 114, 255–284. [Google Scholar] [CrossRef]
- Waehler, R. Fatty Acids: Facts vs. Fiction. Int. J. Vitam. Nutr. Res. 2021, 1, 21. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Grimble, R.F. Polyunsaturated Fatty Acids, Inflammation and Immunity. Eur. J. Clin. Nutr/ 2002, 56, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Dietary Arachidonic Acid: Harmful, Harmless or Helpful? Br. J. Nutr. 2007, 98, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, H. Intake of Arachidonic Acid-Containing Lipids in Adult Humans: Dietary Surveys and Clinical Trials. Lipids. Health Dis. 2019, 18, 1–9. [Google Scholar] [CrossRef]
- Foster, R.H.; Hardy, G.; Alany, R.G. Borage Oil in the Treatment of Atopic Dermatitis. Nutrition 2010, 26, 708–718. [Google Scholar] [CrossRef]
- Barham, J.B.; Edens, M.B.; Fonteh, A.N.; Johnson, M.M.; Easter, L.; Chilton, F.H. Addition of Eicosapentaenoic Acid to γ-Linolenic Acid–Supplemented Diets Prevents Serum Arachidonic Acid Accumulation in Humans. J. Nutr. 2000, 130, 1925–1931. [Google Scholar] [CrossRef]
- Amagai, Y.; Oida, K.; Matsuda, A.; Jung, K.; Kakutani, S.; Tanaka, T.; Matsuda, K.; Jang, H.; Ahn, G.; Xia, Y. Dihomo-γ-Linolenic Acid Prevents the Development of Atopic Dermatitis through Prostaglandin D1 Production in NC/Tnd Mice. J. Dermatol. Sci. 2015, 79, 30–37. [Google Scholar] [CrossRef]
- Sertznig, P.; Reichrath, J. Peroxisome Proliferator-Activated Receptors (PPARs) in Dermatology: Challenge and Promise. Dermatoendocrinol 2011, 3, 130–135. [Google Scholar] [CrossRef]
- Blunder, S.; Pavel, P.; Minzaghi, D.; Dubrac, S. PPARdelta in Affected Atopic Dermatitis and Psoriasis: A Possible Role in Metabolic Reprograming. Int. J. Mol. Sci. 2021, 22, 7354. [Google Scholar] [CrossRef] [PubMed]
- Nagano, N.; Okada, T.; Kayama, K.; Hosono, S.; Kitamura, Y.; Takahashi, S. Delta-6 Desaturase Activity during the First Year of Life in Preterm Infants. Prostaglandins Leukot. Essent. Fatty Acids 2016, 115, 8–11. [Google Scholar] [CrossRef]
- Töröcsik, D.; Weise, C.; Gericke, J.; Szegedi, A.; Lucas, R.; Mihaly, J.; Worm, M.; Rühl, R. Transcriptomic and Lipidomic Profiling of Eicosanoid/Docosanoid Signalling in Affected and Non-affected Skin of Human Atopic Dermatitis Patients. Exp. Dermatol. 2019, 28, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Lindskou, R.; Hølmer, G. Polyunsaturated Fatty Acids in Plasma, Red Blood Cells and Mononuclear Cell Phospholipids of Patients with Atopic Dermatitis. Allergy 1992, 47, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Nagel, G.; Linseisen, J. Dietary Intake of Fatty Acids, Antioxidants and Selected Food Groups and Asthma in Adults. Eur. J. Clin. Nutr. 2005, 59, 8–15. [Google Scholar] [CrossRef]
- Welland, S.K.; Mutius, E.; Husing, A. Intake of Trans Fatty Acids and Prevalence of Childhood Asthma and Allergies in Europe. Lancet 1999, 353, 2040–2041. [Google Scholar] [CrossRef]
- Ferreri, C.; Angelini, F.; Chatgilialoglu, C.; Dellonte, S.; Moschese, V.; Rossi, P.; Chini, L. Trans Fatty Acids and Atopic Eczema/Dermatitis Syndrome: The Relationship with a Free Radical Cis-Trans Isomerization of Membrane Lipids. Lipids 2005, 40, 661–667. [Google Scholar] [CrossRef]
- Hung, W.-L.; Hwang, L.S.; Shahidi, F.; Pan, M.-H.; Wang, Y.; Ho, C.-T. Endogenous Formation of Trans Fatty Acids: Health Implications and Potential Dietary Intervention. J. Funct. Foods 2016, 25, 14–24. [Google Scholar] [CrossRef]
- Kwon, Y. Effect of Trans–Fatty Acids on Lipid Metabolism: Mechanisms for Their Adverse Health Effects. Food Rev. Int. 2016, 32, 323–339. [Google Scholar] [CrossRef]
- Rosenthal, M.D.; Whitehurst, M.C. Selective Effects of Isomeric Cis and Trans Fatty Acids on Fatty Acyl Δ9 and Δ6 Desaturation by Human Skin Fibroblasts. Biochim. Biophys. Acta (BBA)-Lipids Lipid Metab. 1983, 753, 450–459. [Google Scholar] [CrossRef]
- Sakai, T.; Ire, A.V.; Matoba, T.; Yamamoto, S. Dietary Trans Fatty Acids Suppress the Development of Spontaneous Atopic-like Dermatitis in NC/Nga Mice. J. Nutr. Sci. Vitaminol. 2009, 55, 412–416. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Meigs, J.B.; Manson, J.E.; Rifai, N.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Consumption of Trans Fatty Acids Is Related to Plasma Biomarkers of Inflammation and Endothelial Dysfunction. J. Nutr. 2005, 135, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Rimm, E.B.; King, I.B.; Lawler, R.L.; McDonald, G.B.; Levy, W.C. Trans Fatty Acids and Systemic Inflammation in Heart Failure. Am. J. Clin. Nutr. 2004, 80, 1521–1525. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Y.; Ma, L.-J.; Yuan, J.-P.; Yu, P.; Bai, B.-X. Causal Effects of Fatty Acids on Atopic Dermatitis: A Mendelian Randomization Study. Front. Nutr. 2023, 10, 1083455. [Google Scholar] [CrossRef]
- Thomsen, B.J.; Chow, E.Y.; Sapijaszko, M.J. The Potential Uses of Omega-3 Fatty Acids in Dermatology: A Review. J. Cutan. Med. Surg. 2020, 2, 481–494. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.L.; Ash, M.E. Lipid Replacement Therapy: A Natural Medicine Approach to Replacing Damaged Lipids in Cellular Membranes and Organelles and Restoring Function. Biochim. Et Biophys. Acta (BBA)-Biomembr. 2014, 1838, 1657–1679. [Google Scholar] [CrossRef]
- Liu, R.-L.; Zhang, J.; Mou, Z.-L.; Hao, S.-L.; Zhang, Z.-Q. Microwave-Assisted One-Step Extraction-Derivatization for Rapid Analysis of Fatty Acids Profile in Herbal Medicine by Gas Chromatography-Mass Spectrometry. Analyst 2012, 137, 5135–5143. [Google Scholar] [CrossRef]
- Gallego, S.F.; Hermansson, M.; Liebisch, G.; Hodson, L.; Ejsing, C.S. Total Fatty Acid Analysis of Human Blood Samples in One Minute by High-Resolution Mass Spectrometry. Biomolecules 2019, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef]
- Brenna, J.T.; Plourde, M.; Stark, K.D.; Jones, P.J.; Lin, Y.-H. Best Practices for the Design, Laboratory Analysis, and Reporting of Trials Involving Fatty Acids. Am. J. Clin. Nutr. 2018, 108, 211–227. [Google Scholar] [CrossRef]
- Paul, J.-L.; Sall, N.-D.; Soni, T.; Poignet, J.-L.; Lindenbaum, A.; Man, N.-K.; Moatti, N.; Raichvarg, D. Lipid Peroxidation Abnormalities in Hemodialyzed Patients. Nephron 1993, 64, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Nowak, E.; Wyrwicz, G.; Smoleński, O.; Spodaryk, K. Rheological Properties of Red Blood Cells (Including Reticulocytes) in Patients with Chronic Renal Disease. Clin. Hemorheol. Microcirc. 1999, 21, 87–94. [Google Scholar] [PubMed]
- Hodson, L.; Skeaff, C.M.; Fielding, B.A. Fatty Acid Composition of Adipose Tissue and Blood in Humans and Its Use as a Biomarker of Dietary Intake. Prog. Lipid Res. 2008, 47, 348–380. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, C.; Masi, A.; Sansone, A.; Giacometti, G.; Larocca, A.V.; Menounou, G.; Scanferlato, R.; Tortorella, S.; Rota, D.; Conti, M. Fatty Acids in Membranes as Homeostatic, Metabolic and Nutritional Biomarkers: Recent Advancements in Analytics and Diagnostics. Diagnostics 2017, 7, 1. [Google Scholar] [CrossRef]
- Ferreri, C.; Chatgilialoglu, C. Role of Fatty Acid-Based Functional Lipidomics in the Development of Molecular Diagnostic Tools. Expert Rev. Mol. Diagn. 2012, 12, 767–780. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Country | 1-Year Prevalence of AD in Adults | Lifetime Prevalence of AD in Adults | Ref. |
|---|---|---|---|
| United States | 4.9% | - | [24] |
| Canada | 3.5% | - | [24] |
| Finland | 10.1% | 21.9% | [25] |
| Germany | 2.2% | 2.0–4.0% | [26] |
| France | - | 3.6% | [27] |
| Italy | 8.1% | 4.7% | [27,28] |
| Japan | 3.0% | 3.3% | [29] |
| Fatty Acid | Food Source * |
|---|---|
| SFA | meat, dairy products, fast food |
| Palmitic acid (C16:0) | meat, cheese, butter, palm oil |
| MUFA | vegetable oils, dry fruits, olive, olive oil, butter |
| Oleic acid (C18:1, n-9) | vegetable oils, e.g., olive oil, margarine, avocado, olives |
| PUFA omega-6 and omega-3 | fatty fish, algae, flax seed and oil, chia seeds, hemp seeds and oil, walnuts, almonds, hazelnuts, and other nuts |
| Linoleic acid (C18:2, n-6) | sunflower, corn, and safflower oils |
| Alpha-linolenic acid (C18:3, n-3) | flaxseeds and oil, canola oil, chia seed, purslane, algae |
| Gamma-linolenic acid (C18:3, n-6) | primrose and oil, borage and oil, blackcurrant and oil |
| Arachidonic acid (ARA, C20:4, n-6) | eggs, meat |
| Eicosapentaenoic acid (EPA, C20:5, n-3) | fish and fish oil, algae |
| Docosahexaenoic acid (DHA, C22:6, n-3) | fish oil and algae |
| Trans fatty acids | meat, milk, partially hydrogenated fats in foods, e.g., margarine |
| Fatty Acid Change/Detection Site or Natural Source | Dermatological Affection | Clinical Correlation | Ref. |
|---|---|---|---|
| SFA/foods | Atopic dermatitis | Evaluated in mothers’ diet/high atopic sensitization in infants | [63,64,65] |
| Omega-6/omega-3 PUFA unbalance/ plasma phospholipids | Atopic dermatitis | Measured in mothers and infants—increased risk in the first year of life | [3] |
| MUFA increase/skin | Atopic dermatitis | Detected in atopic dermatitis lesions | [65,66,67] |
| MUFA increase/sebum | Atopic and seborrheic dermatitis | Disruption of the stratum corneum barrier | [68,69] |
| GLA/primrose or borage oil | Atopic dermatitis | Amelioration of dermatological symptoms | [6,70,79,80] |
| DGLA decrease/blood | Atopic dermatitis | Desaturase enzyme deficiency signature | [78] |
| GLA deficiency | Atopic dermatitis in infants | Amelioration of skin affection | [84] |
| PUFA omega-6 increase/blood cells and plasma | Eczema, atopic dermatitis | Inflammatory signature | [9,59,71,72,73,86] |
| Trans fatty acids/red blood cells, T-lymphocytes | Eczema, atopic dermatitis | Radical stress signature. Intakes of processed foods | [89,90,91] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olejnik, A.; Gornowicz-Porowska, J.; Jenerowicz, D.; Polańska, A.; Dobrzyńska, M.; Przysławski, J.; Sansone, A.; Ferreri, C. Fatty Acids Profile and the Relevance of Membranes as the Target of Nutrition-Based Strategies in Atopic Dermatitis: A Narrative Review. Nutrients 2023, 15, 3857. https://doi.org/10.3390/nu15173857
Olejnik A, Gornowicz-Porowska J, Jenerowicz D, Polańska A, Dobrzyńska M, Przysławski J, Sansone A, Ferreri C. Fatty Acids Profile and the Relevance of Membranes as the Target of Nutrition-Based Strategies in Atopic Dermatitis: A Narrative Review. Nutrients. 2023; 15(17):3857. https://doi.org/10.3390/nu15173857
Chicago/Turabian StyleOlejnik, Anna, Justyna Gornowicz-Porowska, Dorota Jenerowicz, Adriana Polańska, Małgorzata Dobrzyńska, Juliusz Przysławski, Anna Sansone, and Carla Ferreri. 2023. "Fatty Acids Profile and the Relevance of Membranes as the Target of Nutrition-Based Strategies in Atopic Dermatitis: A Narrative Review" Nutrients 15, no. 17: 3857. https://doi.org/10.3390/nu15173857
APA StyleOlejnik, A., Gornowicz-Porowska, J., Jenerowicz, D., Polańska, A., Dobrzyńska, M., Przysławski, J., Sansone, A., & Ferreri, C. (2023). Fatty Acids Profile and the Relevance of Membranes as the Target of Nutrition-Based Strategies in Atopic Dermatitis: A Narrative Review. Nutrients, 15(17), 3857. https://doi.org/10.3390/nu15173857