
Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study



Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Baseline Characteristics, Anthropometric, and Biochemical Parameters of the Participants
2.3. Definition of Hypothyroidism and Metabolic Syndrome
2.4. Estimation of Usual Food Intake by a Semi-Quantitative Food Frequency Questionnaire (SQFFQ)
2.5. Dietary Patterns by Principal Component Analysis
2.6. Quality Control of Genotyping and GWAS for Hypothyroidism Risk
2.7. Genetic Variant–Genetic Variant Interaction by a Generalized Multifactor Dimensionality Reduction (GMDR) Method
2.8. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Nutrient Intake of Participants
3.2. Anthropometric and Biochemical Measurements
3.3. Genetic Variants Associated with Hypothyroidism Risk by GWAS and SNP–SNP Interactions by GMDR
3.4. Association between Polygenic Risk Scores (PRS) and Hypothyroidism Risk
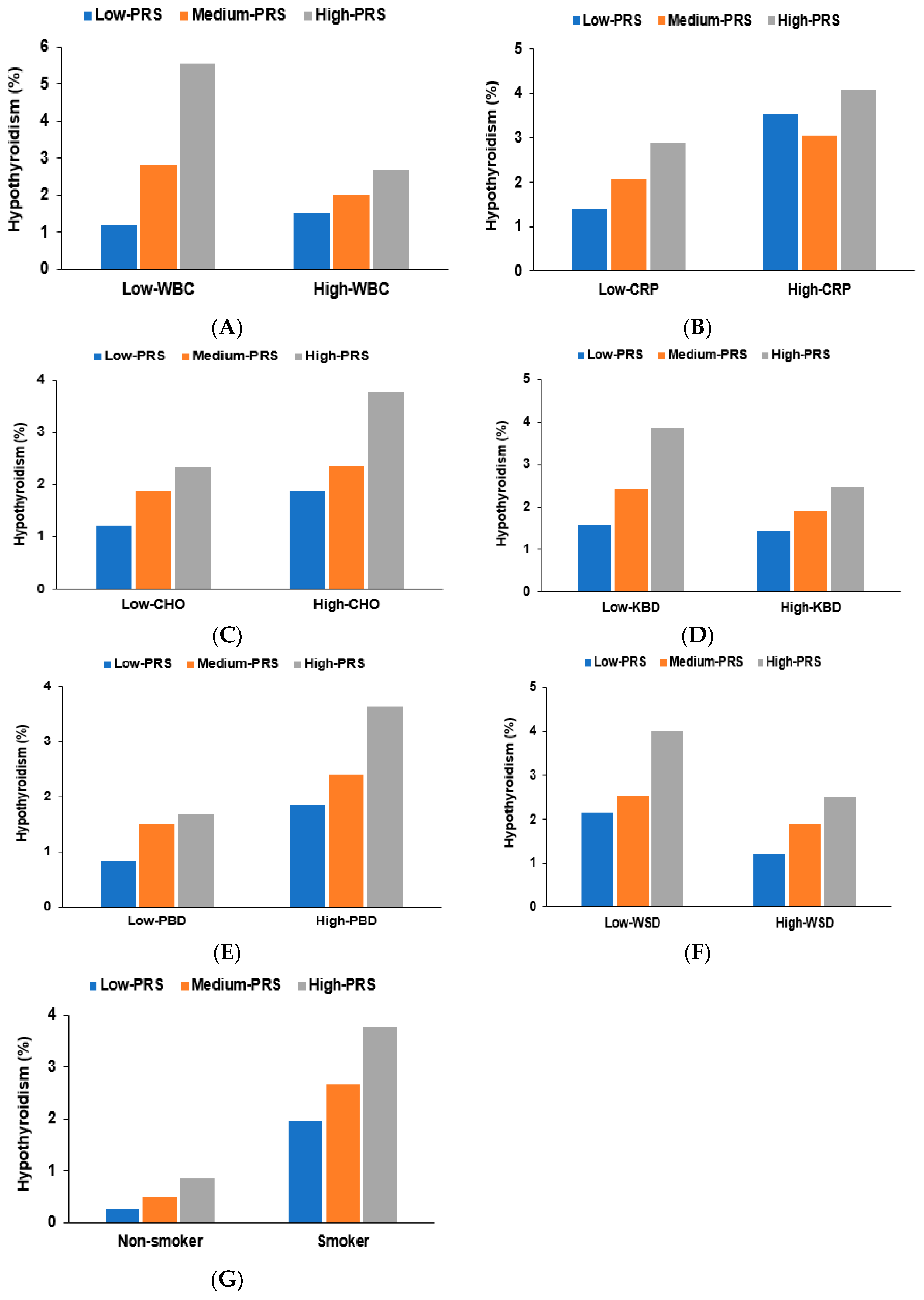
3.5. Genetic Interactions of Lifestyle Factors with Hypothyroidism Risk
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiovato, L.; Magri, F.; Carlé, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv. Ther. 2019, 36, 47–58. [Google Scholar] [CrossRef]
- Leng, O.; Razvi, S. Hypothyroidism in the older population. Thyroid. Res. 2019, 12, 2. [Google Scholar] [CrossRef]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef]
- Sawicka-Gutaj, N.; Erampamoorthy, A.; Zybek-Kocik, A.; Kyriacou, A.; Zgorzalewicz-Stachowiak, M.; Czarnywojtek, A.; Ruchała, M. The Role of Thyroid Hormones on Skeletal Muscle Thermogenesis. Metabolites 2022, 12, 336. [Google Scholar] [CrossRef]
- Su, X.; Peng, H.; Chen, X.; Wu, X.; Wang, B. Hyperlipidemia and hypothyroidism. Clin. Chim. Acta 2022, 527, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Kostopoulou, E.; Miliordos, K.; Spiliotis, B. Genetics of primary congenital hypothyroidism—A review. Hormones 2021, 20, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Kizys, M.M.L.; Louzada, R.A.; Mitne-Neto, M.; Jara, J.R.; Furuzawa, G.K.; de Carvalho, D.P.; Dias-da-Silva, M.R.; Nesi-França, S.; Dupuy, C.; Maciel, R.M.B. DUOX2 Mutations Are Associated with Congenital Hypothyroidism With Ectopic Thyroid Gland. J. Clin. Endocrinol. Metab. 2017, 102, 4060–4071. [Google Scholar] [CrossRef]
- Stoupa, A.; Kariyawasam, D.; Polak, M.; Carré, A. Genetics of congenital hypothyroidism: Modern concepts. Pediatr. Investig. 2022, 6, 123–134. [Google Scholar] [CrossRef]
- Babić Leko, M.; Gunjača, I.; Pleić, N.; Zemunik, T. Environmental Factors Affecting Thyroid-Stimulating Hormone and Thyroid Hormone Levels. Int. J. Mol. Sci. 2021, 22, 6521. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.L.; Chernock, R.D.; Mansour, M. Environmental factors and anatomic pathology of the thyroid gland: Review of literature. Diagn. Histopathol. 2020, 26, 207–215. [Google Scholar] [CrossRef]
- Bellastella, G.; Scappaticcio, L.; Caiazzo, F.; Tomasuolo, M.; Carotenuto, R.; Caputo, M.; Arena, S.; Caruso, P.; Maiorino, M.I.; Esposito, K. Mediterranean Diet and Thyroid: An Interesting Alliance. Nutrients 2022, 14, 4130. [Google Scholar] [CrossRef] [PubMed]
- Daily, J.W.; Park, S. Interaction of BDNF rs6265 variants and energy and protein intake in the risk for glucose intolerance and type 2 diabetes in middle-aged adults. Nutrition 2017, 33, 187. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Daily, J.W.; Zhang, X.; Jin, H.S.; Lee, H.J.; Lee, Y.H. Interactions with the MC4R rs17782313 variant, mental stress and energy intake and the risk of obesity in Genome Epidemiology Study. Nutr. Metab. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Ahn, J.; Lee, B.K. Self-rated Subjective Health Status Is Strongly Associated with Sociodemographic Factors, Lifestyle, Nutrient Intakes, and Biochemical Indices, but Not Smoking Status: KNHANES 2007–2012. J. Korean Med. Sci. 2015, 30, 1279–1287. [Google Scholar] [CrossRef]
- Park, S.; Kim, D.S.; Kang, S. Carrying minor allele of FADS1 and haplotype of FADS1 and FADS2 increased the risk of metabolic syndrome and moderate but not low fat diets lowered the risk in two Korean cohorts. Eur. J. Nutr. 2019, 58, 831–842. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Lee, B.K. Very-low-fat diets may be associated with increased risk of metabolic syndrome in the adult population. Clin. Nutr. 2016, 35, 1159–1167. [Google Scholar] [CrossRef]
- Park, S.; Zhang, X.; Lee, N.R.; Jin, H.S. TRPV1 Gene Polymorphisms Are Associated with Type 2 Diabetes by Their Interaction with Fat Consumption in the Korean Genome Epidemiology Study. J. Nutr. Nutr. 2016, 9, 47–61. [Google Scholar] [CrossRef]
- Hur, H.J.; Yang, H.J.; Kim, M.J.; Lee, K.H.; Kim, M.S.; Park, S. Association of Polygenic Variants with Type 2 Diabetes Risk and Their Interaction with Lifestyles in Asians. Nutrients 2022, 14, 3222. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Steel, R.G.; Torrie, J.H.; Dickey, D.A. Principles and Procedures of Statistics: A Biological Approach; McGraw-Hill: New York, NY, USA, 1997. [Google Scholar]
- Kim, J.O.; Mueller, C.W. Factor Analysis. Statistical Methods and Practical Issues; Sage publications: Thousand Oaks, CA, USA, 1978. [Google Scholar]
- Hur, H.J.; Wu, X.; Yang, H.J.; Kim, M.J.; Lee, K.-H.; Hong, M.; Park, S.; Kim, M.-S. Beneficial Effects of a Low-Glycemic Diet on Serum Metabolites and Gut Microbiota in Obese Women with Prevotella and Bacteriodes Enterotypes: A Randomized Clinical Trial. Front. Nutr. 2022, 9, 861880. [Google Scholar] [CrossRef]
- Davis, M.G.; Phillippi, J.C. Hypothyroidism: Diagnosis and Evidence-Based Treatment. J. Midwifery Womens Health 2022, 67, 394–397. [Google Scholar] [CrossRef]
- Hapon, M.B.; Simoncini, M.; Via, G.; Jahn, G.A. Effect of hypothyroidism on hormone profiles in virgin, pregnant and lactating rats, and on lactation. Reproduction 2003, 126, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Redmond, G.P. Hypothyroidism and women's health. Int. J. Fertil. Womens Med. 2002, 47, 123–127. [Google Scholar] [PubMed]
- Kaminski, J.; Junior, C.M.; Pavesi, H.; Drobrzenski, B.; Amaral, G.M.D. Effects of oral versus transdermal estradiol plus micronized progesterone on thyroid hormones, hepatic proteins, lipids, and quality of life in menopausal women with hypothyroidism: A clinical trial. Menopause 2021, 28, 1044–1052. [Google Scholar] [CrossRef]
- Frank-Raue, K.; Raue, F. Thyroid Dysfunction in Periand Postmenopausal Women-Cumulative Risks. Dtsch. Arztebl. Int. 2023, 120, 311–316. [Google Scholar]
- Kim, S.; Kwon, Y.S.; Kim, J.Y.; Hong, K.H.; Park, Y.K. Association between Iodine Nutrition Status and Thyroid Disease-Related Hormone in Korean Adults: Korean National Health and Nutrition Examination Survey VI (2013–2015). Nutrients 2019, 11, 2757. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Yeoh, Y.; Seo, M.J.; Lee, G.H.; Kim, C.-I. Estimation of Dietary Iodine Intake of Koreans through a Total Diet Study (TDS). Korean J. Community Nutr. 2021, 26, 48–55. [Google Scholar] [CrossRef]
- Katagiri, R.; Yuan, X.; Kobayashi, S.; Sasaki, S. Effect of excess iodine intake on thyroid diseases in different populations: A systematic review and meta-analyses including observational studies. PLoS ONE 2017, 12, e0173722. [Google Scholar] [CrossRef]
- Wu, K.; Zhou, Y.; Ke, S.; Huang, J.; Gao, X.; Li, B.; Lin, X.; Liu, X.; Liu, X.; Ma, L.; et al. Lifestyle is associated with thyroid function in subclinical hypothyroidism: A cross-sectional study. BMC Endocr. Disord. 2021, 21, 112. [Google Scholar] [CrossRef]
- Kim, H.I.; Oh, H.K.; Park, S.Y.; Jang, H.W.; Shin, M.H.; Han, J.M.; Bae, J.C.; Kim, S.W.; Kim, T.H.; Chung, J.H. Non-immune-related hypothyroidism and its relationship with excess iodine. Eur. J. Nutr. 2019, 58, 2851–2858. [Google Scholar] [CrossRef]
- Carlé, A.; Pedersen, I.B.; Knudsen, N.; Perrild, H.; Ovesen, L.; Rasmussen, L.B.; Jørgensen, T.; Laurberg, P. Moderate alcohol consumption may protect against overt autoimmune hypothyroidism: A population-based case-control study. Eur. J. Endocrinol. 2012, 167, 483–490. [Google Scholar] [CrossRef]
- Wiersinga, W.M. Clinical Relevance of Environmental Factors in the Pathogenesis of Autoimmune Thyroid Disease. Endocrinol. Metab. 2016, 31, 213–222. [Google Scholar] [CrossRef]
- Zhao, G.; Wang, Z.; Ji, J.; Cui, R. Effect of coffee consumption on thyroid function: NHANES 2007–2012 and Mendelian randomization. Front. Endocrinol. 2023, 14, 1188547. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Xu, M.; Wu, M.; Wang, X.; Li, F.; Zhang, J.; You, L.; Pan, X.; Feng, W.; Wu, J.; et al. Obesity is associated with subclinical hypothyroidism in the presence of thyroid autoantibodies: A cross-sectional study. BMC Endocr. Disord. 2022, 22, 94. [Google Scholar] [CrossRef] [PubMed]
- Song, R.-H.; Wang, B.; Yao, Q.-M.; Li, Q.; Jia, X.; Zhang, J.-A. The Impact of Obesity on Thyroid Autoimmunity and Dysfunction: A Systematic Review and Meta-Analysis. Front. Immunol. 2019, 10, 2349. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Aggarwal, S.; Khandelwal, D. Thyroid Dysfunction and Type 2 Diabetes Mellitus: Screening Strategies and Implications for Management. Diabetes Ther. 2019, 10, 2035–2044. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Peng, D. Update on dyslipidemia in hypothyroidism: The mechanism of dyslipidemia in hypothyroidism. J. Endocr. Connect. 2022, 11, e210002. [Google Scholar]
- Luo, Y.; Wu, F.; Huang, Z.; Gong, Y.; Zheng, Y. Assessment of the relationship between subclinical hypothyroidism and blood lipid profile: Reliable or not? Lipids Health Dis. 2022, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Izquierdo, J.; Filion, K.B.; Boivin, J.F.; Azoulay, L.; Pollak, M.; Yu, O.H.Y. Subclinical hypothyroidism and the risk of cancer incidence and cancer mortality: A systematic review. BMC Endocr. Disord. 2020, 20, 83. [Google Scholar]
- Solmunde, E.; Falstie-Jensen, A.M.; Lorenzen, E.L.; Ewertz, M.; Reinertsen, K.V.; Dekkers, O.M.; Cronin-Fenton, D.P. Breast cancer, breast cancer-directed radiation therapy and risk of hypothyroidism: A systematic review and meta-analysis. Breast 2023, 68, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Penna, G.; Rubio, I.G.S.; Brust, E.S.; Cazarin, J.; Hecht, F.; Alkmim, N.R.; Rajão, K.M.A.B.; Ramos, H.E. Congenital hypothyroidism and thyroid cancer. J. Endocr. Relat. Cancer 2021, 28, R217–R230. [Google Scholar] [CrossRef] [PubMed]
- Guastamacchia, E.; Giagulli, V.A.; Licchelli, B.; Triggiani, V. Selenium and Iodine in Autoimmune Thyroiditis. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Ates, I.; Yilmaz, F.M.; Altay, M.; Yilmaz, N.; Berker, D.; Güler, S. The relationship between oxidative stress and autoimmunity in Hashimoto's thyroiditis. Eur. J. Endocrinol. 2015, 173, 791–799. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; CampennÌ, A.; Giuffrida, G.; Casciaro, M.; Barbalace, M.C.; Hrelia, S.; Trimarchi, F.; CannavÒ, S.; Gangemi, S. Oxidative stress as a key feature of autoimmune thyroiditis: An update. Minerva Endocrinol. 2020, 45, 326–344. [Google Scholar] [CrossRef]
- Talebi, S.; Ghaedi, E.; Sadeghi, E.; Mohammadi, H.; Hadi, A.; Clark, C.C.T.; Askari, G. Trace Element Status and Hypothyroidism: A Systematic Review and Meta-analysis. Biol. Trace Elem. Res. 2020, 197, 1–14. [Google Scholar] [CrossRef]
- Rabbani, E.; Golgiri, F.; Janani, L.; Moradi, N.; Fallah, S.; Abiri, B.; Vafa, M. Randomized Study of the Effects of Zinc, Vitamin A, and Magnesium Co-supplementation on Thyroid Function, Oxidative Stress, and hs-CRP in Patients with Hypothyroidism. Biol. Trace Elem. Res. 2021, 199, 4074–4083. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.; Singh, S.; Brito, M. Thyroid, Diet, and Alternative Approaches. J. Clin. Endocrinol. Metab. 2022, 107, 2973–2981. [Google Scholar] [PubMed]
- Song, M.Y.; Park, S. Association of Polygenetic Risk Scores Related to Immunity and Inflammation with Hyperthyroidism Risk and Interactions between the Polygenetic Scores and Dietary Factors in a Large Cohort. J. Thyroid. Res. 2021, 2021, 7664641. [Google Scholar] [CrossRef] [PubMed]
- Stefan, M.; Faustino, L.C. Genetics of Thyroid-Stimulating Hormone Receptor—Relevance for Autoimmune Thyroid Disease. Front. Endocrinol. 2017, 8, 57. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Barcons, M.; Colobran, R.; Gómez-Pau, A.; Marín-Sánchez, A.; Casteràs, A.; Obiols, G.; Abella, R.; Fernández-Doblas, J.; Tonacchera, M.; Lucas-Martín, A.; et al. Graves’ Disease TSHR-Stimulating Antibodies (TSAbs) Induce the Activation of Immature Thymocytes: A Clue to the Riddle of TSAbs Generation? J. Immunol. 2015, 194, 4199–4206. [Google Scholar]
- Schoenmakers, N.; Chatterjee, V.K. TSHR mutations and subclinical congenital hypothyroidism. Nat. Rev. Endocrinol. 2015, 11, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Sun, F.; Zhang, R.J.; Zhang, C.R.; Yan, C.Y.; Zhou, Z.; Zhang, Q.Y.; Li, L.; Ying, Y.X.; Zhao, S.X.; et al. Mutation screening of the TSHR gene in 220 Chinese patients with congenital hypothyroidism. Clin. Chim. Acta 2019, 497, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.; Wang, J.; Luo, S.; Yang, Q.; Li, Q.; Zheng, H.; Hu, X.; Su, J.; Zhang, S.; Chen, R.; et al. Next-generation sequencing analysis of TSHR in 384 Chinese subclinical congenital hypothyroidism (CH) and CH patients. Clin. Chim. Acta 2016, 462, 127–132. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Men | Women | Adjusted ORs and 95% CI | |||
|---|---|---|---|---|---|
| Normal (n = 19,970) | Hypothyroidism (n = 60) | Normal (n = 35,824) | Hypothyroidism (n = 810) | ||
| Age (years) | 54.8 ± 0.07 a | 57.1 ± 1.23 a | 49.6 ± 0.24 b | 51.6 ± 1.71 a**+++ | 1.444 (1.243–1.678) |
| Gender (%) | 35.8 | 6.9 | 64.2 | 93.1 *** | 8.276 (6.294–10.88) |
| Hypothyroidism treatment (N, % treatment) | - | 49 (81.7) | - | 609 (75.2) | |
| Former+current Smoking (Number, %) | 5604 (28.1) | 14 (23.3) | 702 (1.97) | 13 (1.60) | 0.859 (0.605–1.220) |
| Drinking (>20 g/day) | 14,262 (71.6) | 39 (65.0) | 10,879 (30.5) | 191 (23.6) *** | 0.716 (0.603–0.851) |
| Coffee (>1 c/weeks) | 13,510 (67.7) | 41 (68.3) | 21,292 (59.4) | 444 (54.8) ** | 0.859 (0.74–0.990) |
| Physical activity (N, Yes%) | 8822 (45.5) | 33 (55.0) | 13,426 (38.5) | 354 (43.8) ** | 1.135 (0.986–1.306) |
| Energy (EER%) 1 | 84.6 ± 0.05 c | 84.3 ± 0.69 c | 102 ± 0.03 b | 103 ± 0.19 a+++ | 0.980 (0.853–1.127) |
| CHO (En%) 2 | 60.9 ± 0.07 b | 60.6 ± 1.09 b | 72.5 ± 0.05 a | 73.1 ± 0.29 a+++ | 1.152 (0.952-1.393) |
| Fat (En%) 3 | 11.6 ± 0.05 b | 11.4 ± 0.72 b | 15.0 ± 0.03 a | 15.0 ± 0.19 a*** | 0.516 (0.253–1.052) |
| Protein (En%) 4 | 11.1 ± 0.02 b | 11.3 ± 0.37 b | 14.1 ± 0.02 a | 14.1 ± 0.10 a+++ | 0.952 (0.779–1.164) |
| Fiber (g/day) 5 | 5.59 ± 0.02 b | 5.69 ± 0.34 ab | 6.04 ± 0.07 a | 6.08 ± 0.47 ab++ | 0.851 (0.703–1.031) |
| Iodine (ug/day) 6 | 329 ± 2.8 b | 317 ± 39.7 b | 442 ± 1.89 a | 450 ± 10.6 a+++ | 0.943 (0.809–1.100) |
| Selenium 7 | 17.3 ± 0.19 a | 11.1 ± 2.71 ab | 13.0 ± 0.13 b | 11.4 ± 0.72 b** | 0.737 (0.616–0.882) |
| Cu 8 | 0.93 ± 0.01 a | 0.80 ± 0.10 a | 0.87 ± 0.01 a | 0.79 ± 0.03 b* | 0.766 (0.642–0.914) |
| Mn 9 | 2.27 ± 0.02 a | 1.77 ± 0.21 b | 2.08 ± 0.01 a | 1.88 ± 0.06 b** | 0.743 (0.633–0.872) |
| Zn 10 | 4.74 ± 0.03 | 3.96 ± 0.40 | 4.72 ± 0.02 | 4.38 ± 0.11 ** | 0.810 (0.688–0.954) |
| Vitamin C 11 | 91.4 ± 0.52 b | 94.0 ± 7.45 b | 113 ± 0.35 a | 110 ± 1.99 a+++ | 1.053 (0.905–1.226) |
| Vitamin D 12 | 5.21 ± 0.05 b | 5.07 ± 0.66 b | 7.07 ± 0.03 a | 7.17 ± 0.18 a+++ | 1.050 (0.883–1.249) |
| Dietary inflammation index 13 | −18.5 ± 0.13 b | −19.1 ± 1.85 ab | −20.7 ± 0.09 a | −20.3+0.49 a | 0.961 (0.812–1.137) |
| Sodium 14 | 2.41 ± 0.01 | 2.39 ± 0.15 | 2.44 ± 0.01 | 2.35 ± +0.04 | 1.011 (0.871–1.174) |
| Seaweeds (g/day) 15 | 1.66 ± 0.01 b | 1.89 ± 0.27 b | 2.45 ± 0.05 a | 2.39 ± 0.37 ab++ | 0.868 (0.739–1.020) |
| Vegetables (g/day) 16 | 89.1 ± 0.81 b | 99.4 ± 11.5 ab | 114 ± 0.54 a | 115 ± 3.07 a+ | 0.973 (0.834–1.135) |
| Fruits (g/day) 17 | 167 ± 1.9 b | 165 ± 26.5 b | 243 ± 1.3 a | 240 ± 7.1 a++ | 1.080 (0.921–1.266) |
| Meats (g/day) 18 | 86.7 ± 0.88 a | 79.5 ± 12.5 ab | 83.1 ± 0.60 a | 75.0 ± 3.35 b* | 0.803 (0.674–0.956) * |
| Traditional balanced diet 19 | 14,661 (73.4) | 47 (78.3) | 22,151 (61.8) | 458 (56.5) ** | 0.848 (0.731–0.984) |
| Prudent diet 19 | 8943 (44.8) | 28 (46.7) | 26,455 (73.9) | 636 (78.5) ** | 1.242 (1.045–1.476) |
| Western-style diet 19 | 15,640 (78.3) | 45 (75.0) | 22,888 (63.9) | 493 (60.9) | 0.923 (0.794–1.073) |
| Rice-based diet 19 | 12,790 (64.1) | 37 (61.7) | 23,848 (66.6) | 513 (63.3) | 0.877 (0.756–1.018) |
| Men | Women | Adjusted ORs (95% CI) | |||
|---|---|---|---|---|---|
| Normal (n = 19,970) | Hypothyroidism (n = 60) | Normal (n = 35,824) | Hypothyroidism (n = 810) | ||
| BMI (kg/m2) 1 | 24.5 ± 0.02 a | 24.3 ± 0.45 a | 23.7 ± 0.09 b | 23.5 ± 0.62 a+# | 0.896 (0.765–1.048) |
| Waist circumference (cm) 2 | 85.7 ± 0.04 a | 86.2 ± 0.74 a | 80.5 ± 0.15 b | 79.8 ± 1.04 b+++ | 0.850 (0.680–1.063) |
| Hip circumference (cm) 3 98 | 95.7 ± 0.04 a | 97.0 ± 0.67 a | 94.4 ± 0.13 b | 93.6 ± 0.93 ab+++# | 1.007 (0.818–1.238) |
| Fasting plasma glucose (mg/dl) 4 126 | 100 ± 0.2 a | 99.0 ± 3.8 ab | 97.1 ± 0.78 b | 93.7 ± 5.33 ab | 0.981 (0.740–1.300) |
| HbA1c (%) 5 6.5 | 5.81 ± 0.01 | 5.75 ± 0.16 | 5.80 ± 0.04 | 5.61 ± 0.21 | 0.949 (0.667–1.348) |
| Total-C (mg/dl) 6 230 | 193 ± 0.3 b | 195 ± 5.8 b | 201 ± 1.2 a | 213 ± 8.1 ab+ | 1.102 (0.939–1.292) |
| LDL-C (mg/dl) 7 160 | 113 ± 0.3 b | 112 ± 4.5 b | 122 ± 0.2 a | 118 ± 1.2 ab++ | 1.142 (0.956–1.365) |
| HDL-C (mg/dl) 8 | 49.1 ± 0.1 b | 50.9 ± 1.9 b | 56.9 ± 0.4 a | 57.8 ± 0.5 ab+++ | 0.967 (0.831–1.126) |
| TG (mg/dl) 9 | 155 ± 0.9 a | 159 ± 16.9 ab | 125 ± 3.4 b | 112 ± 23.6 b++ | 1.274 (1.089–1.490) ** |
| SBP (mmHg) 10 | 125 ± 0.1 a | 123 ± 2.2 ab | 120 ± 0.4 b | 120 ± 3.1 ab+ | 0.878 (0.748–1.030) |
| DBP (mmHg) 11 | 78.3 ± 0.1 a | 77.0 ± 1.5 b | 74.1 ± 0.3 b | 71.9 ± 2.1 b+++ | 0.751 (0.530–1.002) |
| MetS (N, Yes%) | 16,430 (82.3) | 47 (78.3) | 31,433 (87.7) | 713 (88.0) | 1.078 (0.861–1.350) |
| eGFR 12 (mL/min/1.73m2) | 83.9 ± 0.14 b | 86.6 ± 2.05 ab | 87.3 ± 0.10 a | 87.9 ± 0.55 a+ | 0.862 0.693 1.074) |
| Serum ALT (U/L) 12 | 26.7 ± 0.16 a | 24.4 ± 3.0 ab | 21.8 ± 0.61 b | 22.4 ± 4.16 ab | 0.856 (0.651–1.127) |
| Serum AST (U/L) 13 | 25.7 ± 0.12 a | 23.9 ± 2.23 ab | 23.6 ± 0.46 b | 25.2 ± 3.12 ab | 1.090 (0.761–1.562) |
| Serum ALP (U/L) 14 | 186 ± 1.2 a | 172 ± 18.3 ab | 167 ± 4.2 b | 189 ± 25.3 ab*** | 2.110 (1.820–2.445) |
| WBC (×109 /L) 15 4.0 | 5.80 ± 0.02 a | 5.60 ± 0.20 a | 5.65 ± 0.01 ab | 5.55 ± 0.05 b+ | 3.151 (2.601–3.817) *** |
| Serum CRP (mg/dL) 16 0.5 | 0.17 ± 0.005 | 0.08 ± 0.10 | 0.13 ± 0.02 | 0.16 ± 0.15 | 1.355 0.959 1.914 |
| Thyroid cancer (N, %) | 35 (0.18) | 0 (0) | 336 (0.94) | 24 (2.96) *** | 3.160 2.074 4.816 |
| Cancer incidence (N, Yes%) | 536 (2.68) | 1 (1.67) | 1461 (4.08) | 64 (7.90) *** | 1.922 (1.480–2.495) |
| Asthma (N, Yes%) | 279 (1.40) | 0(0) | 643 (1.80) | 20 (2.47) | 1.346 (0.857–2.112) |
| Osteoporosis (N, Yes%) | 131 (0.66) | 0(0) | 2661 (7.43) | 92 (11.4) *** | 1.381 (1.089–1.752) |
| Arthritis (N, %) | 787 (3.94) | 3 (5.00) | 3922 (11.0) | 109 (13.5) * | 1.241 (1.005–1.534) |
| Chr 1 | SNP 2 | Position | Mi 3 | Ma 4 | OR 5 | p Value Adjusted 6 | MAF 7 | HWE 8 | Gene | Functional Consequence |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | rs144611984 | 108270345 | A | C | 1.91(1.48–2.46) | 5.05 × 10−7 | 0.0211 | 0.4238 | VAV3 | Intron |
| 6 | rs7990 | 32608077 | A | C | 1.37(1.23–1.54) | 6.04 × 10−8 | 0.19 | 0.0552 | HLA-DQA1 | Missense |
| 6 | rs28746784 | 32635140 | T | C | 1.48(1.28–1.71) | 1.22 × 10−7 | 0.0937 | 0.6098 | HLA-DQB1 | Nmd transcript |
| 6 | rs1800610 | 31543827 | A | G | 1.35(1.21–1.52) | 2.13 × 10−7 | 0.1921 | 0.6802 | TNF | Intron |
| 8 | rs11573856 | 119954995 | T | C | 0.78(0.68–0.9) | 4.74 × 10−5 | 0.1826 | 0.1248 | TNFRSF11B | Intron |
| 11 | rs11246015 | 224585 | T | C | 0.73(0.63–0.85) | 5.52 × 10−6 | 0.1482 | 0.2201 | SIRT3 | intron |
| 12 | rs7977554 | 112882859 | A | G | 1.55(1.31–1.83) | 3.12 × 10−7 | 0.0647 | 0.0878 | PTPN11 | Nmd transcript |
| 14 | rs75664963 | 81492195 | T | A | 0.77(0.68–0.86) | 7.46 × 10−6 | 0.2704 | 0.4389 | TSHR | Intron |
| 15 | rs7171366 | 45386656 | G | T | 1.45(1.21–1.74) | 4.83 × 10−6 | 0.0567 | 0.1427 | DUOX2 | Intron |
| 15 | rs117742123 | 45429332 | T | G | 1.49(1.27–1.74) | 5.82 × 10−7 | 0.0786 | 1 | DUOX1 | Nmd transcript |
| Low-PRS (N = 13,856) | Medium-PRS (N = 25,608) | High-PRS (N = 17,200) | Gene–Nutrient Interaction p Value | |
|---|---|---|---|---|
| Low WBC 1 High WBC | 1 | 2.299 (1.050–5.033) 1.249 (0.942–1.655) | 4.887 (2.186–10.93) 1.706 (1.257–2.315) | <0.0001 |
| Low CRP 2 High CRP | 1 1 | 1.515 (1.174–1.954) 0.885 (0.306–2.560) | 2.221 (1.693–2.915) 0.562 (0.209–1.510) | 0.3053 |
| Low EER 3 High EER | 1 1 | 1.248 (0.881–1.768) 1.434 (0.945–2.178) | 1.893 (1.304–2.748) 2.009 (1.281–3.149) | 0.2139 |
| Low CHO 4 High CHO | 1 1 | 1.554 (1.088–2.220) 1.238 (0.860–1.782) | 2.049 (1.396–3.009) 1.917 (1.297–2.834) | 0.0563 |
| Low protein 5 High protein | 1 1 | 1.315 (0.963–1.795) 1.449 (0.938–2.237) | 1.852 (1.324–2.590) 2.280 (1.438–3.614) | 0.2595 |
| Low fat 6 High fat 1 | 1 1 | 1.285 (0.934–1.770) 1.410 (0.865–2.297) | 1.762 (1.246–2.492) 2.367 (1.415–3.958) | 0.1768 |
| Low KBD 7 High KBD | 1 1 | 1.554 (1.034–2.335) 1.286 (0.912–1.812) | 2.654 (1.731–4.067) 1.696 (1.167–2.464) | 0.0608 |
| Low PBD 7 High PBD | 1 1 | 2.104 (1.184–3.739) 1.161 (0.865–1.558) | 2.297 (1.235–4.274) 1.859 (1.357–2.547) | 0.0140 |
| Low WSD 7 High WSD | 1 1 | 1.168 (0.797–1.712) 1.336 (0.957–1.865) | 2.042 (1.360–3.065) 1.797 (1.254–2.577) | 0.0295 |
| Low RMD 7 High RMD | 1 1 | 1.471 (0.969–2.234) 1.312 (0.944–1.824) | 2.271 (1.461–3.531) 1.855 (1.299–2.648) | 0.5219 |
| Low PA 8 High PA | 1 1 | 1.285 (0.934–1.770) 1.484 (1.020–2.159) | 1.762 (1.246–2.492) 2.227 (1.495–3.319) | 0.7276 |
| Low coffee 9 High coffee | 1 1 | 1.705 (1.088–2.671) 1.104 (0.790–1.541) | 2.415 (1.498–3.894) 1.671 (1.165–2.397) | 0.1439 |
| Low alcohol 10 High alcohol | 1 1 | 1.419 (1.043–1.931) 1.025 (0.597–1.760) | 1.962 (1.407–2.737) 1.836 (1.041–3.237) | 0.2330 |
| Non-smokers Former and current Smokers | 1 1 | 1.400 (1.089–1.800) 1.687 (0.504–5.645) | 2.073 (1.584–2.711) 3.296 (0.952–11.41) | 0.0379 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.S.; Park, S. Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study. Nutrients 2023, 15, 3850. https://doi.org/10.3390/nu15173850
Kim DS, Park S. Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study. Nutrients. 2023; 15(17):3850. https://doi.org/10.3390/nu15173850
Chicago/Turabian StyleKim, Da Sol, and Sunmin Park. 2023. "Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study" Nutrients 15, no. 17: 3850. https://doi.org/10.3390/nu15173850
APA StyleKim, D. S., & Park, S. (2023). Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study. Nutrients, 15(17), 3850. https://doi.org/10.3390/nu15173850