
A Potential Role Exists for Nutritional Interventions in the Chronic Phase of Mild Traumatic Brain Injury, Concussion and Sports-Related Concussion: A Systematic Review



Abstract
:1. Introduction
1.1. Traumatic Brain Injury—Definition and Diagnosing
1.2. Symptoms and Quality of Life Following mTBI
1.3. Is There a Role for Nutrition in Recovery?
2. Materials and Methods
2.1. Study Search and Selection Criteria
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
3. Synthesis of Results
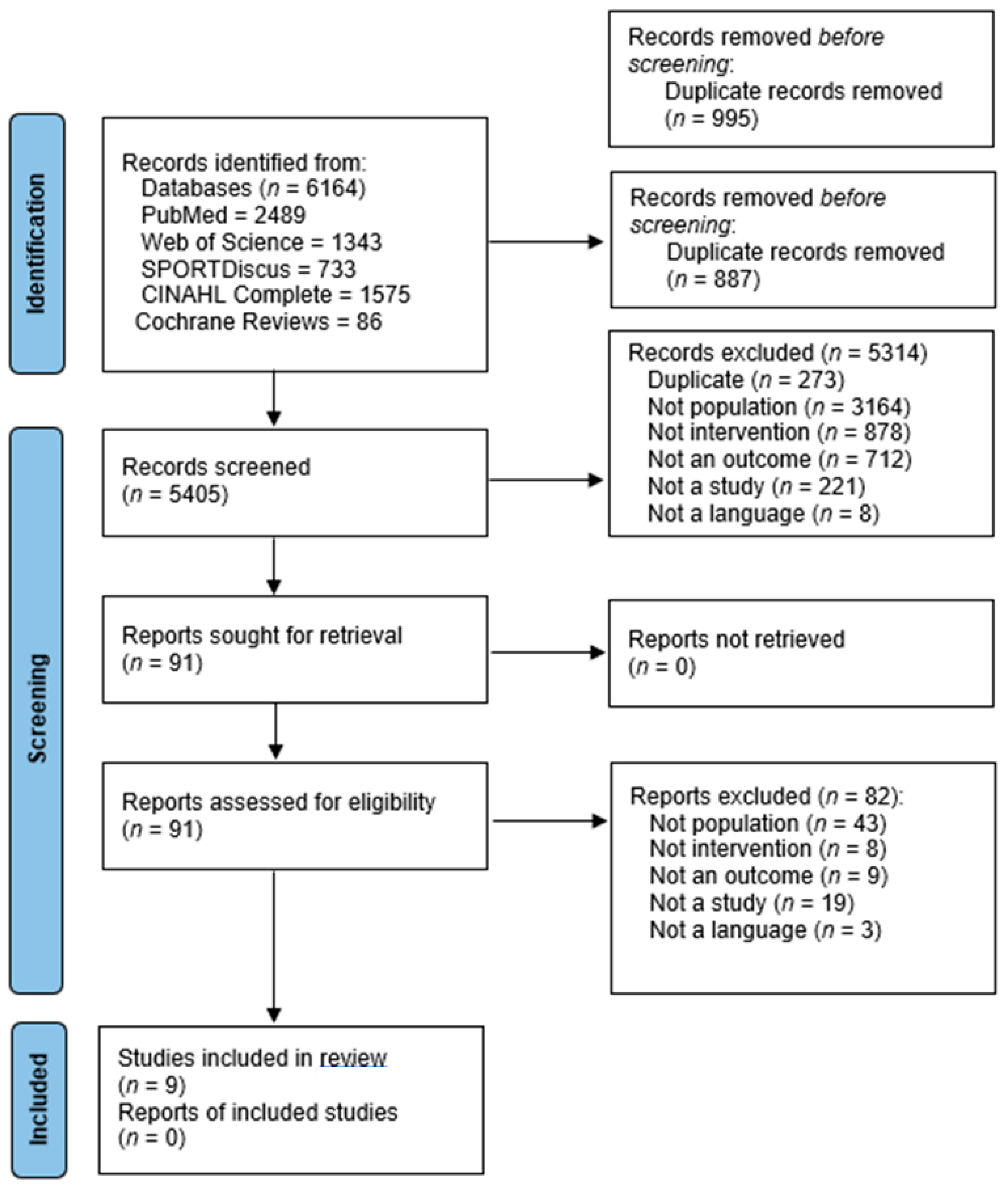
3.1. Article Selection and Quality Assessment
3.2. Details of the Included Studies and Participants
3.3. Participant Characteristics
3.4. Length of Follow-Up
3.5. Details of Interventions and Findings
3.5.1. Studies Involving Omega-3 Fatty Acids
3.5.2. Melatonin
3.5.3. Enzogenol®
3.5.4. The Ketogenic Diet (KD)
3.5.5. MLC901 Capsules
3.5.6. Phytocannabinoids
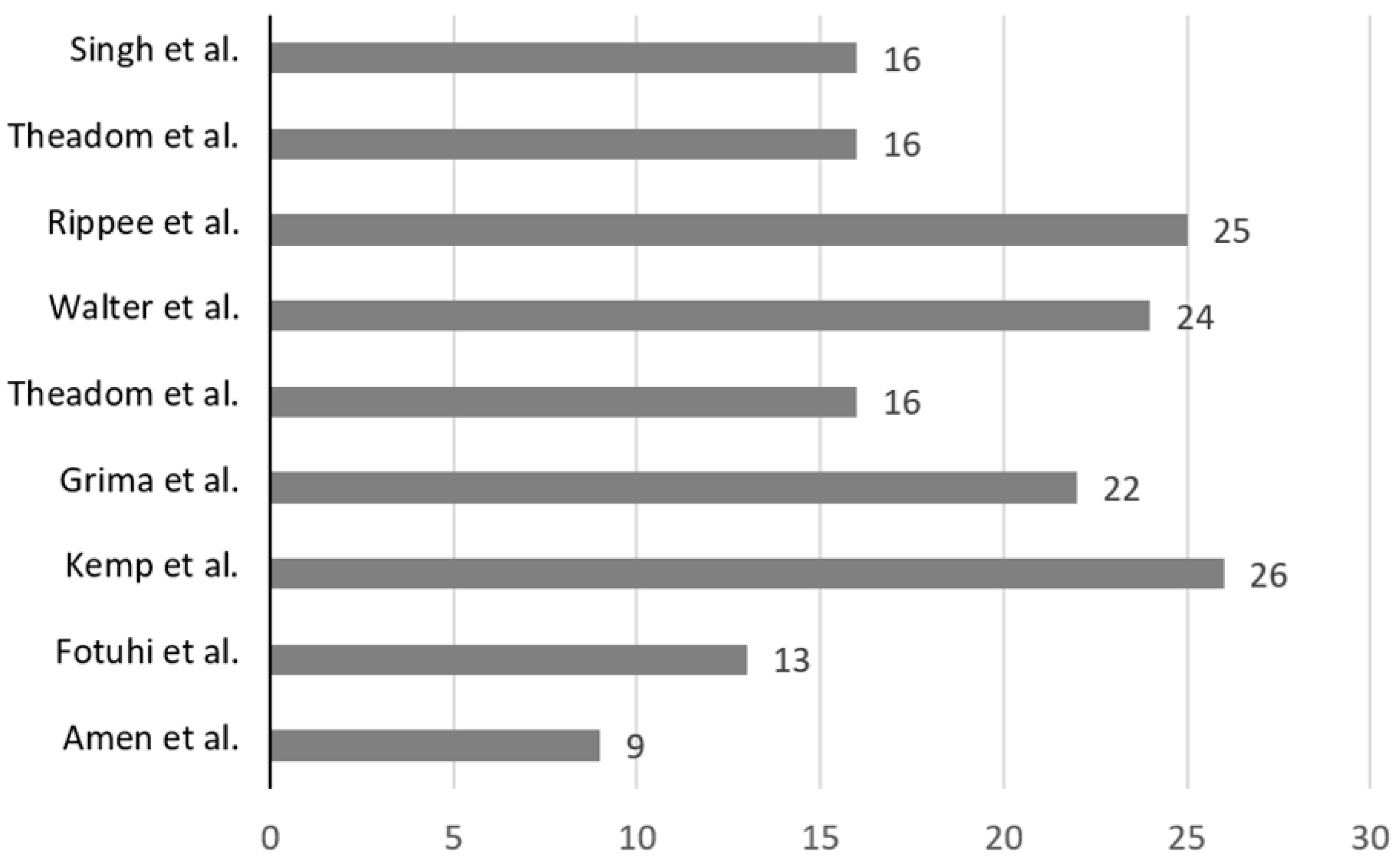
3.6. Quality and Risk of Bias Assessment
4. Discussion
4.1. Participant and Study Characteristics
4.2. The Possible Role of Nutrition in Recovery from mTBI
4.3. Limitations
4.4. Practical Applications and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Cover page |
| ABSTRACT | |||
| Abstract | 2 | See PRISMA 2020 for Abstract checklist. | P1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | P2–4 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | P4 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for syntheses. | P4–6 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | P4 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | P4–6 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of this review, including how many reviewers screened each record and each report retrieved, whether they worked independently and, if applicable, details of automation tools used in the process. | P6 |
| Data collection process | 9 | Specify the methods used to collect data from the reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators and, if applicable, details of automation tools used in the process. | P6 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses) and, if not, the methods used to decide which results to collect. | P4–6 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | P4–6 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess the risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently and, if applicable, details of automation tools used in the process. | P7 |
| Effect measures | 12 | For each outcome, specify the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | P4–6 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics or data conversions. | ||
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | ||
| 13d | Describe any methods used to synthesize the results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity and software package(s) used. | ||
| 13e | Describe any methods used to explore possible causes of heterogeneity among the study results (e.g., subgroup analysis, meta-regression). | ||
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | ||
| Reporting bias assessment | 14 | Describe any methods used to assess the risk of bias due to missing results in a synthesis (arising from reporting biases). | P7–9 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | P8 |
| 16b | Cite studies that might appear to meet the inclusion criteria but were excluded, and explain why they were excluded. | P8 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | P15–22 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | |
| Results of individual studies | 19 | For all outcomes, for each study, present: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was performed, present each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | ||
| 20c | Present results for all investigations of possible causes of heterogeneity among study results. | ||
| 20d | Present results for all sensitivity analyses conducted to assess the robustness of the synthesized results. | ||
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | P32–34 |
| 23b | Discuss any limitations of the evidence included in this review. | P34 | |
| 23c | Discuss any limitations of the review processes used. | P34 | |
| 23d | Discuss implications of the results for practice, policy and future research. | P34 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for this review, including register name and registration number or state that this review was not registered. | P4 |
| 24b | Indicate where the review protocol can be accessed or state that a protocol was not prepared. | ||
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | MA | |
| Support | 25 | Describe sources of financial or non-financial support for this review, and the role of the funders or sponsors in this review. | P35 |
| Competing interests | 26 | Declare any competing interests of the review authors. | P35 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; and any other materials used in the review. | Available upon request |
References
- Rusnak, M. Traumatic brain injury: Giving voice to a silent epidemic. Nat. Rev. Neurol. 2013, 9, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Te Ao, B.; Brown, P.; Tobias, M.; Ameratunga, S.; Barker-Collo, S.; Theadom, A.; McPherson, K.; Starkey, N.; Dowell, A.; Jones, K.; et al. Cost of traumatic brain injury in New Zealand: Evidence from a population-based study. Neurology 2014, 83, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Theadom, A.; Ellenbogen, R.G.; Bannick, M.S.; Montjoy-Venning, W.; Lucchesi, L.R.; Murray, C.J.L. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 56–87. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Theadom, A.; Barker-Collo, S.; Starkey, N.J.; McPherson, K.; Kahan, M.; Dowell, A.; Brown, P.; Parag, V.; Kydd, R.; et al. Incidence of traumatic brain injury in New Zealand: A population-based study. Lancet Neurol. 2013, 12, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Barker-Collo, S.; Theadom, A.; Jones, K.; Feigin, V.L.; Kahan, M. Accuracy of an International Classification of Diseases Code Surveillance System in the Identification of Traumatic Brain Injury. Neuroepidemiology 2016, 47, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Finch, C.F.; Clapperton, A.J.; McCrory, P. Increasing incidence of hospitalisation for sport-related concussion in Victoria, Australia. Med. J. Aust. 2013, 198, 427–430. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Kay, T.; Harrington, E.E.; Adams, R.; Anderson, T.; Berrol, S.; Cicerone, K.; Malec, J. Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87. [Google Scholar] [CrossRef]
- Dadas, A.; Janigro, D. The role and diagnostic significance of cellular barriers after concussive head trauma. Concussion 2018, 3, CNC53. [Google Scholar] [CrossRef]
- Bramlett, H.M.; Dietrich, W.D. Progressive damage after brain and spinal cord injury: Pathomechanisms and treatment strategies. Prog. Brain Res. 2007, 161, 125–141. [Google Scholar] [CrossRef]
- Saatman, K.E.; Duhaime, A.-C.; Bullock, R.; Maas, A.I.R.; Valadka, A.; Manley, G.T. Classification of traumatic brain injury for targeted therapies. J. Neurotrauma 2008, 25, 719–738. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Cui, D.; Gao, L. Traumatic brain injury: A review of characteristics, molecular basis and management. Front. Biosci. 2016, 21, 890–899. [Google Scholar] [CrossRef]
- Harmon, K.G.; Drezner, J.A.; Gammons, M.; Guskiewicz, K.M.; Halstead, M.; Herring, S.A.; Kutcher, J.S.; Pana, A.; Putukian, M.; Roberts, W.O. American Medical Society for Sports Medicine position statement: Concussion in sport. Br. J. Sports Med. 2013, 47, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.E.; Sirois, E. The possible role of hydration in concussions and long-term symptoms of concussion for athletes. A review of the evidence. J. Concussion 2020, 4, 2059700220939404. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef]
- Herring, S.; Kibler, W.B.; Putukian, M.; Solomon, G.S.; Boyajian-O’Neill, L.; Dec, K.L.; Franks, R.R.; Indelicato, P.A.; LaBella, C.R.; Leddy, J.J.; et al. Selected issues in sport-related concussion (SRC|mild traumatic brain injury) for the team physician: A consensus statement. Br. J. Sports Med. 2021, 55, 1251–1261. [Google Scholar] [CrossRef]
- McNeel, C.; Clark, G.M.; Davies, C.B.; Major, B.P.; Lum, J.A.G. Concussion incidence and time-loss in Australian football: A systematic review. J. Sci. Med. Sport 2020, 23, 125–133. [Google Scholar] [CrossRef]
- Eme, R. Neurobehavioral Outcomes of Mild Traumatic Brain Injury: A Mini Review. Brain Sci. 2017, 7, 46. [Google Scholar] [CrossRef]
- Kara, S.; Crosswell, H.; Forch, K.; Cavadino, A.; McGeown, J.; Fulcher, M. Less Than Half of Patients Recover Within 2 Weeks of Injury After a Sports-Related Mild Traumatic Brain Injury: A 2-Year Prospective Study. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2020, 30, 96–101. [Google Scholar] [CrossRef]
- Hiploylee, C.; Dufort, P.A.; Davis, H.S.; Wennberg, R.A.; Tartaglia, M.C.; Mikulis, D.; Hazrati, L.-N.; Tator, C.H. Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers. J. Neurotrauma 2017, 34, 1511–1523. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.J.; Tommerdahl, M.; King, D.A. Neurophysiological abnormalities in individuals with persistent post-concussion symptoms. Neuroscience 2019, 408, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Snell, D.; Macleod, A.; Anderson, T. Post-Concussion Syndrome after a Mild Traumatic Brain Injury: A Minefield for Clinical Practice. J. Behav. Brain Sci. 2016, 6, 227–232. [Google Scholar] [CrossRef]
- Reddy, R.P.; Rajeswaran, J.; Devi, B.I.; Kandavel, T. Cascade of Traumatic Brain Injury: A Correlational Study of Cognition, Postconcussion Symptoms, and Quality of Life. Indian J. Psychol. Med. 2017, 39, 32–39. [Google Scholar] [CrossRef]
- Alosco, M.L.; Tripodis, Y.; Baucom, Z.H.; Mez, J.; Stein, T.D.; Martin, B.; Haller, O.; Conneely, S.; McClean, M.; Nosheny, R.; et al. Late contributions of repetitive head impacts and TBI to depression symptoms and cognition. Neurology 2020, 95, e793–e804. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F. The combined effects of exercise and foods in preventing neurological and cognitive disorders. Prev. Med. 2011, 52, S75–S80. [Google Scholar] [CrossRef]
- Hadanny, A.; Efrati, S. Treatment of persistent post-concussion syndrome due to mild traumatic brain injury: Current status and future directions. Expert Rev. Neurother. 2016, 16, 875–887. [Google Scholar] [CrossRef]
- Mohamadpour, M.; Whitney, K.; Bergold, P.J. The Importance of Therapeutic Time Window in the Treatment of Traumatic Brain Injury. Front. Neurosci. 2019, 13, 7. [Google Scholar] [CrossRef]
- McGeown, J.P.; Hume, P.A.; Theadom, A.; Quarrie, K.L.; Borotkanics, R. Nutritional interventions to improve neurophysiological impairments following traumatic brain injury: A systematic review. J. Neurosci. Res. 2021, 99, 573–603. [Google Scholar] [CrossRef]
- Patch, C.S.; Hill-Yardin, E.L.; Lewis, M.; Ryan, L.; Daly, E.; Pearce, A.J. The More, the Better: High-Dose Omega-3 Fatty Acids Improve Behavioural and Molecular Outcomes in Preclinical Models in Mild Brain Injury. Curr. Neurol. Neurosci. Rep. 2021, 21, 45. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- NHMRC. A Guide to the Development, Implementation and Evaluation of Clinical Practice Guidelines; National Health and Medical Research Council: Canberra, Australia, 1990.
- Amen, D.G.; Wu, J.C.; Taylor, D.; Willeumier, K. Reversing brain damage in former NFL players: Implications for traumatic brain injury and substance abuse rehabilitation. J. Psychoact. Drugs 2011, 43, 1–5. [Google Scholar] [CrossRef]
- Fotuhi, M.; Dwivedy, P.; Yeom, L.H.; Nadeem, I.; Ebadi, A.Y.; Miles, M.; Tittle, R.K. Retrospective Analysis of a Comprehensive Concussion Recovery Program. J. Rehabil. 2020, 86, 20–31. [Google Scholar]
- Kemp, S.; Biswas, R.; Neumann, V.; Coughlan, A. The value of melatonin for sleep disorders occurring post-head injury: A pilot RCT. Brain Inj. 2004, 18, 911–919. [Google Scholar] [CrossRef]
- Grima, N.A.; Rajaratnam, S.M.W.; Mansfield, D.; Sletten, T.L.; Spitz, G.; Ponsford, J.L. Efficacy of melatonin for sleep disturbance following traumatic brain injury: A randomised controlled trial. BMC Med. 2018, 16, 8. [Google Scholar] [CrossRef]
- Theadom, A.; Mahon, S.; Barker-Collo, S.; McPherson, K.; Rush, E.; Vandal, A.C.; Feigin, V.L. Enzogenol for cognitive functioning in traumatic brain injury: A pilot placebo-controlled RCT. Eur. J. Neurol. 2013, 20, 1135–1144. [Google Scholar] [CrossRef]
- Walter, A.; Finelli, K.; Bai, X.; Arnett, P.; Bream, T.; Seidenberg, P.; Lynch, S.; Johnson, B.; Slobounov, S. Effect of Enzogenol® Supplementation on Cognitive, Executive, and Vestibular/Balance Functioning in Chronic Phase of Concussion. Dev. Neuropsychol. 2017, 42, 93–103. [Google Scholar] [CrossRef]
- Rippee, M.A.; Chen, J.; Taylor, M.K. The Ketogenic Diet in the Treatment of Post-concussion Syndrome-A Feasibility Study. Front. Nutr. 2020, 7, 160. [Google Scholar] [CrossRef]
- Walton, S.R.; Kerr, Z.Y.; Brett, B.L.; Chandran, A.; DeFreese, J.D.; Smith-Ryan, A.E.; Stoner, L.; Echemendia, R.J.; McCrea, M.; Meehan Iii, W.P.; et al. Health-promoting behaviours and concussion history are associated with cognitive function, mood-related symptoms and emotional-behavioural dyscontrol in former NFL players: An NFL-LONG Study. Br. J. Sports Med. 2021, 55, 683–690. [Google Scholar] [CrossRef]
- Singh, J.; Bhagaloo, L.; Pisorski, J.; Neary, P. Effects of phytoccannabinoids on heart rate variability and blood pressure in female post-concussion syndrome patients: Case series. Can. J. Physiol. Pharmacol. 2021, 100, 192–196. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Hooper, P.; Jutai, J.W.; Strong, G.; Russell-Minda, E. Age-related macular degeneration and low-vision rehabilitation: A systematic review. Can. J. Ophthalmol. 2008, 43, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Morton, S.; Barton, C.J.; Rice, S.; Morrissey, D. Risk factors and successful interventions for cricket-related low back pain: A systematic review. Br. J. Sports Med. 2014, 48, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Richmond, S.A.; Fukuchi, R.K.; Ezzat, A.; Schneider, K.; Schneider, G.; Emery, C.A. Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. J. Orthop. Sports Phys. Ther. 2013, 43, 515-B19. [Google Scholar] [CrossRef] [PubMed]
- Simic, M.; Hinman, R.S.; Wrigley, T.V.; Bennell, K.L.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: A systematic review. Arthr. Care Res. 2011, 63, 405–426. [Google Scholar] [CrossRef]
- Theadom, A.; Barker-Collo, S.; Jones, K.M.; Parmar, P.; Bhattacharjee, R.; Feigin, V.L. MLC 901 (NeuroAiD II™) for cognition after traumatic brain injury: A pilot randomized clinical trial. Eur. J. Neurol. 2018, 25, 1055-e82. [Google Scholar] [CrossRef]
- Noguchi, H.; Nishi, D.; Matsumura, K.; Hamazaki, K.; Hamazaki, T.; Matsuoka, Y.J. Limited effect of omega-3 fatty acids on the quality of life in survivors of traumatic injury: A randomized, placebo-controlled trial. Prostaglandins Leukot. Essent. Fat. Acids 2017, 127, 1–5. [Google Scholar] [CrossRef]
- Taylor, C.A.; Bell, J.M.; Breiding, M.J.; Xu, L. Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths—United States, 2007 and 2013. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2017, 66, 1–16. [Google Scholar] [CrossRef]
- Merritt, V.C.; Padgett, C.R.; Jak, A.J. A systematic review of sex differences in concussion outcome: What do we know? Clin. Neuropsychol. 2019, 33, 1016–1043. [Google Scholar] [CrossRef]
- Lewis, M.; Ghassemi, P.; Hibbeln, J. Therapeutic use of omega-3 fatty acids in severe head trauma. Am. J. Emerg. Med. 2013, 31, 273.e5–273.e8. [Google Scholar] [CrossRef] [PubMed]
- Bains, M.; Hall, E.D. Antioxidant therapies in traumatic brain and spinal cord injury. Biochim. Biophys. Acta 2012, 1822, 675–684. [Google Scholar] [CrossRef]
- Shen, Q.; Hiebert, J.B.; Hartwell, J.; Thimmesch, A.R.; Pierce, J.D. Systematic Review of Traumatic Brain Injury and the Impact of Antioxidant Therapy on Clinical Outcomes. Worldviews Evid.-Based Nurs. 2016, 13, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Mathias, J.L.; Alvaro, P.K. Prevalence of sleep disturbances, disorders, and problems following traumatic brain injury: A meta-analysis. Sleep Med. 2012, 13, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Kuczynski, A.; Crawford, S.; Bodell, L.; Dewey, D.; Barlow, K.M. Characteristics of post-traumatic headaches in children following mild traumatic brain injury and their response to treatment: A prospective cohort. Dev. Med. Child Neurol. 2013, 55, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Thau-Zuchman, O.; Gomes, R.N.; Dyall, S.C.; Davies, M.; Priestley, J.V.; Groenendijk, M.; De Wilde, M.C.; Tremoleda, J.L.; Michael-Titus, A.T. Brain Phospholipid Precursors Administered Post-Injury Reduce Tissue Damage and Improve Neurological Outcome in Experimental Traumatic Brain Injury. J. Neurotrauma 2019, 36, 25–42. [Google Scholar] [CrossRef]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Dietary strategy to repair plasma membrane after brain trauma: Implications for plasticity and cognition. Neurorehabil. Neural Repair 2014, 28, 75–84. [Google Scholar] [CrossRef]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Exercise facilitates the action of dietary DHA on functional recovery after brain trauma. Neuroscience 2013, 248, 655–663. [Google Scholar] [CrossRef]
- Puri, S.; Shaheen, M.; Griver, B. Nutrition and cognitive health: A life course approach. Front. Public Health 2023, 11, 1023907. [Google Scholar] [CrossRef]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between diet and sleep quality: A systematic review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef]
- Martens, L.B.; Tibeas, J.R.B.; Sanches, M.; Jakca, F.; Berk, M.; Teixeira, A.L. Nutrition-based interventions for mood disorders. Expert Rev. Neurother. 2021, 21, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Bulter, M.I.; Lackner, S. Advances in the gut microbiome and mood disorders. Curr. Opin. Psychiatry 2023, 36, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. Dietary omega-3 fatty acids normalize BDNF levels, reduce oxidative damage, and counteract learning disability after traumatic brain injury in rats. J. Neurotrauma 2004, 21, 1457–1467. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Population (P) | Adults (≥18 years and older) that have had an mTBI, concussion or SRC, single or repetitive injury and have chronic symptoms (lasting ≥1 month) | |
| Intervention (I) | Nutrition and/or dietary-related interventions administered in the post-injury chronic phase | |
| Comparator (C) | Placebo-controlled, relevant medication control or nothing | |
| Outcomes (O) | Measure of recovery following intervention such as recovery from symptoms, return to work or return to sport | |
| Group 1: Concussion terms | Group 2: Nutrition or dietary-related intervention | Group 3: Recovery terms |
| postconcussion OR “post-concussion” OR concussion OR tbi OR mtbi OR “traumatic brain injur*” OR “cortical impact” OR “fluid percussion” OR “acceleration injury” | diet* OR supplement* OR “neuroprotective agent*” OR creatine OR antioxidant* OR “anti-oxidant*” OR “fatty acid*” OR vitamin* OR nutri* OR nutraceutical OR keto* OR “amino acid*”OR “complementary and integrative medicine” OR “complementary and alternative medicine” | recovery OR “symptom resolution” OR “symptom-free” OR “symptom free” OR restoration OR “return to play” OR “return to activity” OR improvement OR rehab* OR “treatment recovery” OR “recovery of function” |
| Author (Year) Country | Study Design | Aims and Objectives | Type of Injury | Participant Characteristics | Follow-Up | Length of Chronic Symptoms | Intervention | Daily Dosage | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline n, % Male | Background, Age | Follow-Up n, % Male | Sporting Population | ||||||||
| Studies involving Omega-3 Fatty Acids | |||||||||||
| Amen et al. [34] USA | Non-randomised, open-label, single-arm study | To reverse brain damage and cognitive dysfunction in former NFL players. | SRC | n = 30, 100% | Retired NFL players who had recurrent traumatic head injuries and who had brain damage and cognitive impairment Age—NR. | NR | Yes | 2–12 months | Retired players who had head injuries during their playing career | Multifaceted intervention with a dietary component and education on “brain healthy lifestyle”, such as stopping smoking, drug abuse, nutrition and exercise. Dietary components:
|
|
| Fotuhi et al. [35] USA | Secondary analysis of a non-randomised, open-label, single-arm study | To perform a retrospective analysis of data collated from those who completed the NeuroGrow Programme (CRP) and to evaluate changes in neurocognition post intervention. | mTBI | n = 46, 35% | Those in the NeuroGrow CRP who had mTBI and experience PCS. Age (years): ≥10 Overall: 31.7 (15.9) * | NR | No | 12 weeks | At least 3 months following the patient’s relevant injury | Multifaceted rehabilitation program with a dietary component and education from a “brain coach” regarding sleep, stress management, diet and exercise. Dietary components:
| Omega-3 fatty acid containing 1000–1500 mg/day of DHA + EPA |
| Melatonin | |||||||||||
| Kemp et al. [36] UK | Randomised, double-blind, medication- controlled, crossover trial | To explore the potential of melatonin as an alternative to medications in post-TBI sleep disturbance. | Mild to severe TBI | n = 7, 100% | Community-dwelling adults with sleep disturbance following TBI. mTBI; n = 2 (29%) Age (years): 17.2–54.7 Overall: 39.6 (NR) * | n = 7, 100% | No | 10 weeks | At least 6 months post-injury. Group (months): 36.3 (NR) * | Intervention: Melatonin Control: Amitriptyline Methodology: Participants received the intervention or control treatment for 1 month, which was followed by a 2-week washout period. After this, participants swapped and received the other treatment for 1 month. | Intervention: Melatonin 5 mg Control: Amitriptyline 25 mg |
| Grima et al. [37] Australia | Randomised, double-blind placebo-controlled, crossover, clinical trial | To evaluate the effect of melatonin on those with sleep disturbance post-TBI. | Mild to severe TBI | n = 35 randomised, 67% | Community-dwelling adults with sleep complaint following TBI. mTBI; n = 2 (6%), in placebo group Age (years): 18–65 years Overall: 37 (11) * Intervention to control group: 35 (11) * Control to intervention group: 38 (10) * | n = 33, NR | No | 10 weeks | Months post-injury: Overall: 46 (13–102) ** Intervention to control group: 61 (28–115) ** Control to intervention group: 25 (10–72) ** | Intervention: Melatonin in two-piece gelatine capsule Control: Identical placebo capsule containing mannitol, acacia and pure icing sugar Methodology: Participants had a 2-week baseline run-in period, which was followed by two treatment periods lasting 4 weeks of either melatonin or the control. The initial treatment was followed by a crossover period of the alternative treatment. There was a 48 h washout period between treatments. | Intervention: Melatonin 2 mg Control: Mannitol (106 mg), acacia (11 mg) and pure icing sugar (106 mg) |
| Enzogenol® | |||||||||||
| Theadom et al. [38] NZ | Pilot, randomised, double-blind, placebo-controlled, clinical trial | To explore the safety and feasibility of the recruitment and administration of Enzogenol®, to examine efficacy of it on memory and PCS symptoms and to examine the influence of FFM and diet on outcome changes following supplementation. | mTBI | n = 60 randomised, 43% | Community-dwelling adults with persistent cognitive difficulties following mTBI. Age (years): 21–64 Intervention group: 45 (27) ** Control Group: 44 (28) ** | n = 50, NR | Partial, n = 6 (10%) sports-related injury | 16 weeks | 3–12 months post injury Months post injury: Intervention group: 71 (2.66%) * Control group: 8.04 (2.46%) * | Intervention: Enzogenol® capsule Control: Microcrystalline cellulose placebo in an identical capsule Methodology: Participants were allocated to 1. Enzogenol® (n = 30) or 2. placebo (n = 30) for 6 weeks. Then, both groups received Enzogenol® for 6 weeks, which was followed by 4 weeks of the placebo. | Intervention: Enzogenol® 1000 mg (2 × 500 mg capsules in the morning) Control: Microcrystalline cellulose 1000 mg (2 × 500 mg capsules in the morning) |
| Walter et al. [39] USA | Randomised, placebo-controlled, preclinical trial | To examine the effect of Enzogenol® on chronic concussion. | SRC | n = 42, 48% | College-aged athletes with history of SRCs (≤5 SRCs) and residual chronic symptoms. Age (years): 18–24 | n = 42, 48% | Yes | 6 weeks | Those 6 months to 3 years post-injury | Intervention: Enzogenol® capsule Control: Microcrystalline cellulose placebo in a dyed brown capsule identical to Enzogenol® Methodology: Subjects were instructed to take either the intervention or control for the study duration. | Intervention: Enzogenol® 1000 mg (2 × 500 mg capsules in the morning) Control: Microcrystalline cellulose 1000 mg (2 × 500 mg capsules in the morning) |
| The Ketogenic Diet (KD) | |||||||||||
| Rippee et al. [40] USA | Pilot, non-randomised, open-label single-arm, feasibility study | To examine the feasibility of implementing KD in those with PCS symptoms and to investigate changes in self-reported symptoms and cognitive status. | Concussion | n = 14, 14% | Community-dwelling adults with PCS symptoms. Age (years): 18–65 Overall: 45 (12.2) * | n = 11, NR n = 12 completed the study. n = 1 was non-compliant and did not reach ketosis. They were excluded from analyses. | No | 2 months | At least 4 weeks post-injury Days post-injury: 103 (56.0–217.5) ** | Nutrition counselling from a registered dietitian to consume and monitor adherence to the KD. | Participants had to consume: KD at a 1:1 ratio of g lipid to g of non-lipid, energy as 5–10% from CHO, 70–75% from fat and 20–25% from protein and MCT oil ~1–2 tbsps. |
| Studies involving MLC901 | |||||||||||
| Theadom et al. [41] NZ | Pilot, randomised, double-blind, placebo-controlled, clinical trial | To test the efficacy and safety of MLC901 on cognition and to examine its effect on mood, fatigue, physical disability, QoL and neurobehavioural sequalae. | Mild and moderate TBI | n = 78, 50% | Adults post-mild and moderate TBI with cognitive difficulties. Mild and mod TBI: (n = 2, 3% mod) Age (years): 18–65 Overall: 37.5 (14.8) * Intervention: 38.6 (14.1) * Control: 38.4 (15.7) * | n = 50, NR | No | 6 months | 1–12 months post-injury | Intervention: The MLC901 capsule contained 9 herbs known for having antioxidant and anti-inflammatory properties Control: Made from dextrin and magnesium stearate, visually indistinguishable from the intervention pills Methodology: Subjects were instructed to take either the intervention (MLC901) or placebo for the duration of the study. Participants were assessed at 9 months. | Intervention: Two × 0.4 g capsules (0.8 g), three times Control: Two × 0.4 g capsules (0.8 g), three times |
| Studies involving CBD | |||||||||||
| Singh et al. [42] | Double-blind randomised controlled trial | To investigate the responses of phytocannabinoid administration on blood pressure and heartrate variability in PCS women. | PCS | n = 4 0% | Females medically diagnosed with PCS. Age (years): 42–57 Overall: 31.7 (15.9) * | N = 4 0% | No | Every 10–28 days over a total of ≤70 days | Years | Multifaceted intervention with dietary component of self-administered CBD or a CBD:THC formula. Dietary components:
| CBD 25–400 mg or 20:1 CBD:THC formula |
| Level of Quality | Poor | Fair | Good | Excellent |
|---|---|---|---|---|
| Sum Score | ≤14 | 15–19 | 20–25 | 26–28 |
| Author (Year) Country | Level of Evidence a | Dietary Intervention Specifics | Measurements | Results | Brief Summary of Results |
|---|---|---|---|---|---|
| Studies involving Omega-3 Fatty Acids (n-3fas) | |||||
| Amen et al. [34] USA | III | Omega-3 fatty acid, high-potency multiple vitamin and brain enhancement supplement |
|
| Dietary interventions with n-3fas, multivitamin and brain enhancement supplement, in conjunction with lifestyle modifications, may improve cognitive function and cerebral blood flow in those with a history of SRC. |
| Fotuhi et al. [35] USA | III | Omega-3 fatty acid supplement and dietary advice to follow a Mediterranean diet |
|
| Dietary interventions with n-3FAs, in conjunction with other lifestyle modifications, may improve markers of neurocognition and PCS symptoms in those with chronic concussion symptomology. |
| Melatonin | |||||
| Kemp et al. [36] UK | II | Melatonin or amitriptyline |
|
| Melatonin may alleviate some sleep disorders and disturbances following TBI. |
| Grima et al. [37] Australia | II | Melatonin administered as a pill; the placebo was matched for appearance |
|
| Melatonin over a short period of time may improve sleep quality and anxiety following TBI |
| Enzogenol® | |||||
| Theadom et al. [38] NZ | II | Capsules of Enzogenol® or placebo |
|
| Enzogenol® is a well-tolerated and safe supplement for use in humans, and it may improve the frequency of self-reported cognitive failures. An RCT was recommended to examine and determine its efficacy in more detail. |
| Walter et al. [39] USA | II | Two capsules of Enzogenol® daily |
|
| In individuals with a history of SRC and residual symptoms, Enzogenol® may reduce mental fatigue and improve self-reported sleep issues. |
| The Ketogenic Diet | |||||
| Rippee et al. [40] USA | III | Nutrition counselling and KD in a ratio of 1:1 g of lipid to grams of non-lipid |
|
| The KD may be a feasible dietary treatment for PCS and help to improve some memory domains. |
| MLC901 | |||||
| Theadom et al. [41] NZ | II | Two capsules of the MLC901 three times daily |
|
| MLC901 appears to be safe and well-tolerated. It may help to improve domains of executive functioning and complex attention in individuals following mTBI or moderate TBI. |
| Phytocannabinoids | |||||
| Singh et al. [42] | III | CBD/20:1 CBD:THC formula supplement |
|
| Dietary interventions with CBD or a 20:1 CBD:THC formula supplement may improve systolic BPV but at varying doses for different individuals. |
| Study | Summary |
|---|---|
| Amen et al. [34] | Participants: Retired athletes with cognitive impairment and who experienced recurrent TBIs or SRCs during their playing career. Intervention: n-3FAs (1720 mg EPA and 1160 mg DHA), multivitamin and brain-enhancement supplement (containing antioxidants) with education for up to 1 year. Outcomes: Improvement in neurocognitive outcomes, increased brain perfusion and self-reported increases in mood, memory, motivation, sleep and attention. |
| Fotuhi et al. [35] | Participants: Community-dwelling individuals with PCS. Intervention: Multidisciplinary CRP with a dietary component (omega-3 FA containing 1000–1500 mg/day of DHA + EPA and a Mediterranean diet). Outcomes: May improve neurocognitive outcomes in those with PCS, i.e., attention, memory, psychomotor speed, reaction time, executive function, etc. |
| Kemp et al. [36] | Participants: Community-dwelling adults with post-TBI sleep disturbance. Intervention: Melatonin 5 mg daily for 10 weeks versus amitriptyline. Outcomes: Melatonin may improve daytime alertness and alleviate symptoms of anxiety and depression. |
| Grima et al. [37] | Participants: Community-dwelling adults with post-TBI sleep disturbance. Intervention: Melatonin 2 mg daily for 10 weeks. Outcomes: Melatonin may improve sleep quality and symptoms of anxiety. |
| Theadom et al. [38] | Participants: Community-dwelling adults with persistent cognitive difficulties and history of mTBI. Intervention: Enzogenol® 1000 mg daily for 16 weeks. Outcomes: Enzogenol® may reduce cognitive shortcomings associated with chronic mTBI. |
| Walter et al. [39] | Participants: College-aged athletes with a history of SRCs and residual symptoms. Intervention: Enzogenol® 1000 mg daily for 6 weeks. Outcomes: Enzogenol® may reduce mental fatigue and improve self-reported sleep problems in college-aged athletes with a history of SRCs. |
| Rippee et al. [40] | Participants: Community-dwelling adults with PCS symptoms. Intervention: KD as 1:1 ratio of g lipid to g of non-lipid, and energy as 70–75% from fat. MCT oil ~1–2 tbsps. Outcomes: The KD may help to improve PCS symptoms; however, more clinically robust studies are required to support the findings from its feasibility study. |
| Theadom et al. [41] | Participants: Adults with chronic TBI experiencing cognitive difficulties. Intervention: MLC901 capsules 0.8 g, three times daily for 6 months. Outcomes: MLC901 may contribute to improved complex attention and executive functioning in those post-TBI. |
| Singh et al. [42] | Participants: Post-menopausal females with medically diagnosed PCS. Intervention: Self-administered varying dosing of CBD or a 20:1 CBD:THC formula. Outcomes: Improvement in systolic blood pressure volume. |
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | |
| Amen et al. [34] | o | o | o | • | o | • | • | o | • | • | ? | ? | ? | |
| Fotuhi et al. [35] | • | • | • | • | ◊ | • | • | o | o | • | o | o | • | |
| Kemp et al. [36] | • | • | • | • | o | • | • | • | • | • | o | ? | • | |
| Grima et al. [37] | • | • | • | • | • | • | • | • | • | • | o | ? | • | |
| Theadom et al. [38] | • | • | • | • | • | • | • | • | • | • | o | ? | ? | |
| Walter et al. [39] | • | • | • | • | o | • | • | o | o | o | ? | ? | • | |
| Rippee et al. [40] | • | • | • | • | o | • | • | • | • | • | o | ? | • | |
| Theadom et al. [48] | • | • | • | • | • | • | • | • | • | • | • | ? | • | |
| Singh et al. [42] | • | • | • | • | • | • | • | • | • | o | ? | ? | ? | |
| Study | Q14 | Q15 | Q16 | Q17 | Q18 | Q19 | Q20 | Q21 | Q22 | Q23 | Q24 | Q25 | Q26 | Q27 |
| Amen et al. [34] | o | o | • | o | • | ? | • | ? | • | o | o | o | ? | ? |
| Fotuhi et al. [35] | o | o | • | • | • | ? | • | ? | ? | o | o | ? | ? | ? |
| Kemp et al. [36] | • | • | • | • | o | • | • | • | • | • | • | o | • | o |
| Grima et al. [37] | • | • | • | • | • | • | • | • | • | • | • | • | • | • |
| Theadom et al. [38] | • | • | • | • | • | • | • | • | • | • | • | • | • | ? |
| Walter et al. [39] | • | • | • | • | • | o | • | • | ? | • | • | o | ? | ? |
| Rippee et al. [40] | o | o | • | • | • | • | • | ? | • | o | o | o | • | ? |
| Theadom et al. [48] | • | • | • | • | • | • | • | • | ? | • | • | • | • | o |
| Singh et al. [42] | o | o | • | • | • | ? | • | • | • | o | o | ? | • | o |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan, T.; Nagle, S.; Daly, E.; Pearce, A.J.; Ryan, L. A Potential Role Exists for Nutritional Interventions in the Chronic Phase of Mild Traumatic Brain Injury, Concussion and Sports-Related Concussion: A Systematic Review. Nutrients 2023, 15, 3726. https://doi.org/10.3390/nu15173726
Ryan T, Nagle S, Daly E, Pearce AJ, Ryan L. A Potential Role Exists for Nutritional Interventions in the Chronic Phase of Mild Traumatic Brain Injury, Concussion and Sports-Related Concussion: A Systematic Review. Nutrients. 2023; 15(17):3726. https://doi.org/10.3390/nu15173726
Chicago/Turabian StyleRyan, Tansy, Sarah Nagle, Ed Daly, Alan J. Pearce, and Lisa Ryan. 2023. "A Potential Role Exists for Nutritional Interventions in the Chronic Phase of Mild Traumatic Brain Injury, Concussion and Sports-Related Concussion: A Systematic Review" Nutrients 15, no. 17: 3726. https://doi.org/10.3390/nu15173726
APA StyleRyan, T., Nagle, S., Daly, E., Pearce, A. J., & Ryan, L. (2023). A Potential Role Exists for Nutritional Interventions in the Chronic Phase of Mild Traumatic Brain Injury, Concussion and Sports-Related Concussion: A Systematic Review. Nutrients, 15(17), 3726. https://doi.org/10.3390/nu15173726