
Development, Design and Utilization of a CDSS for Refeeding Syndrome in Real Life Inpatient Care—A Feasibility Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
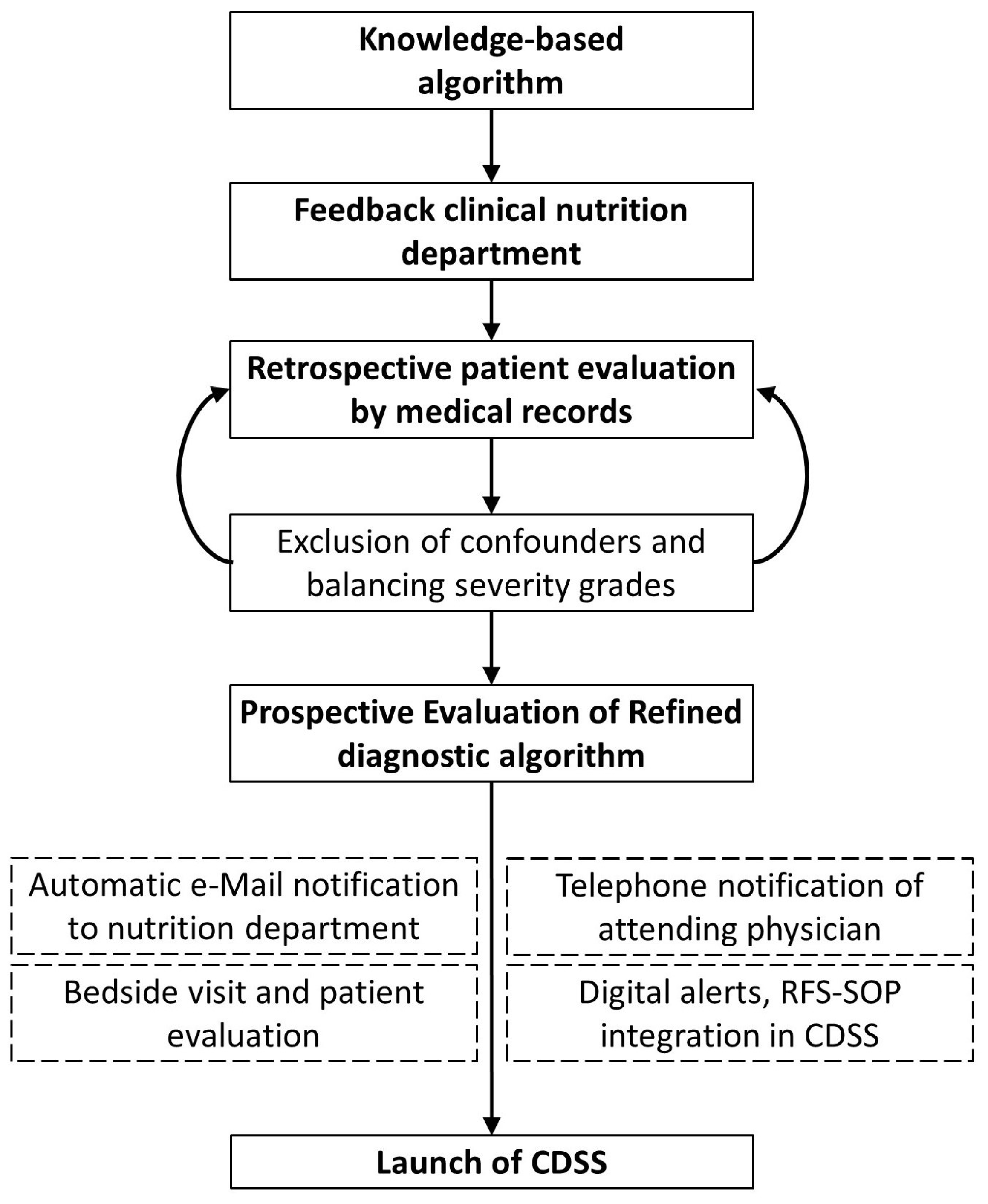
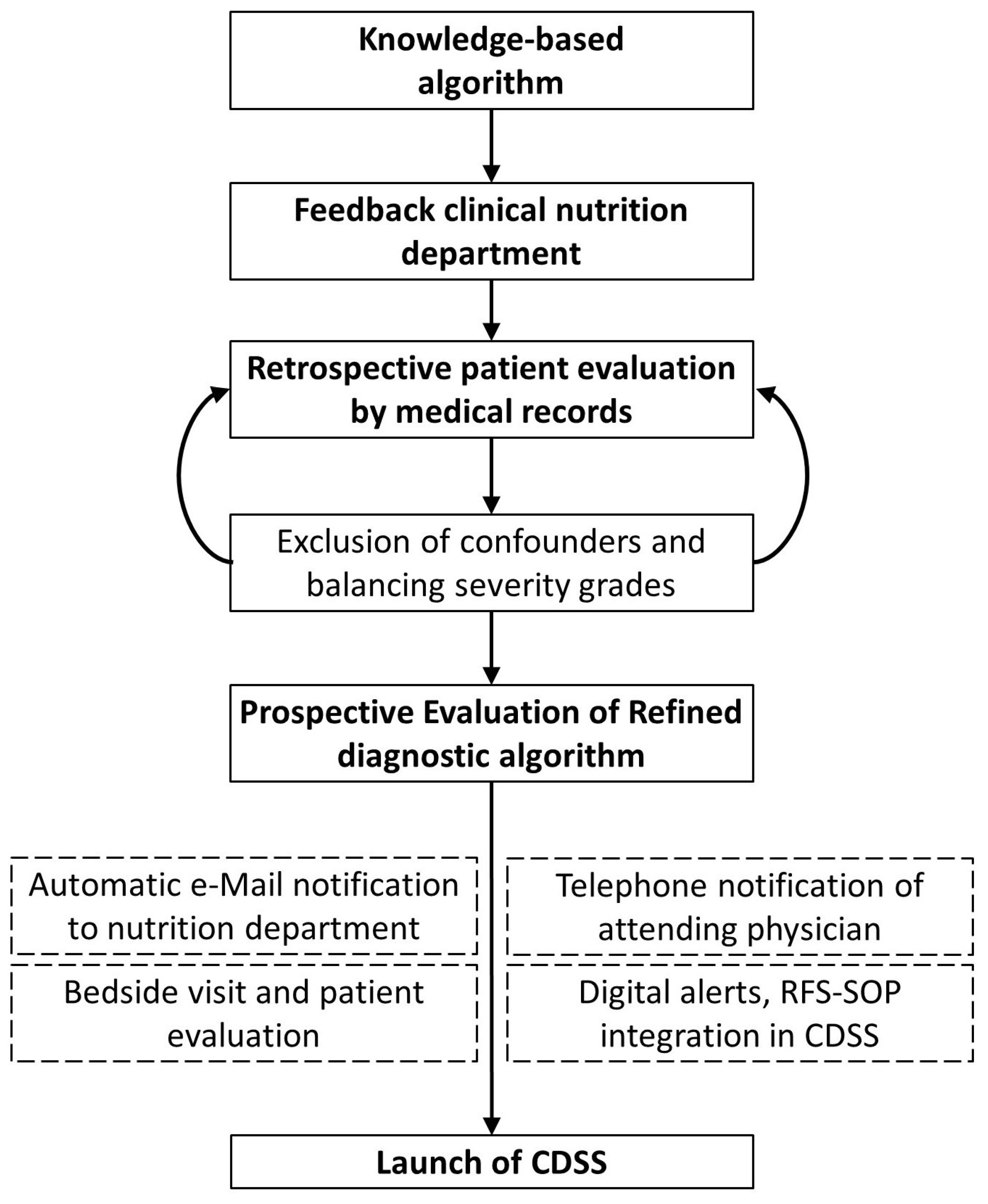
2.1. Study Design
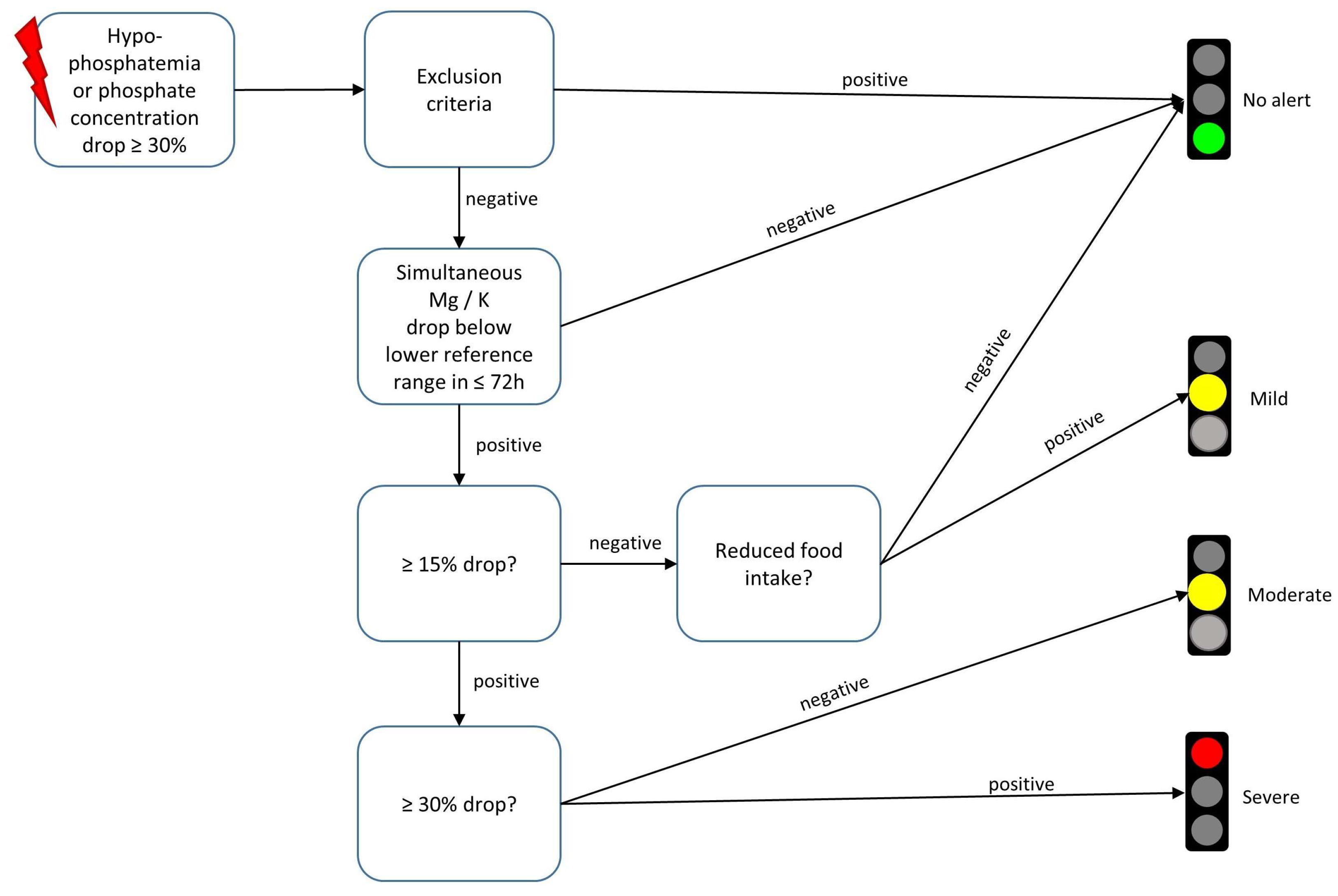
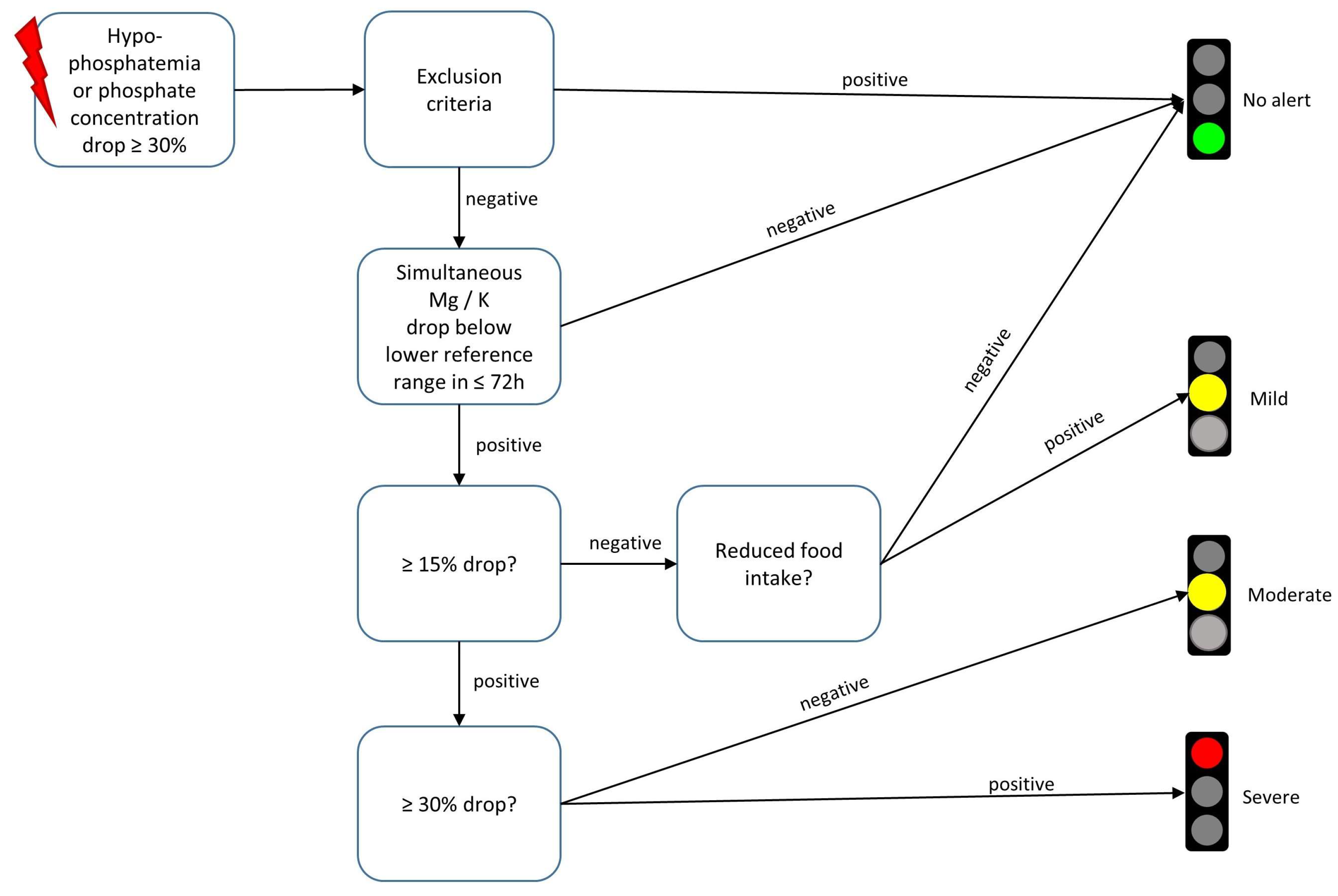
2.2. Development and Refinement of Diagnostic Algorithm
2.3. CDSS Evaluation and Clinical Workflow
- (1)
- Are you familiar with RFS?
- (2)
- Which laboratory value would you use to diagnose RFS?
- (3)
- Did the patient show a new symptom today?
- (4)
- Did you already consider a referral to the clinical nutrition department and if not, why?
2.4. Data Analysis
- -
- Laboratory data: concentrations of phosphate, potassium, magnesium, paracetamol, parathyroid hormone, parathyroid hormone-related peptide and total ketone bodies. All parameters were measured in serum or full blood samples besides for ketones, which were also measured in urine samples
- -
- Encoded items in the EHR: age, sex, reduced food intake at admission, body mass index (BMI), ward category (intensive care units vs. normal wards), OPS codes regarding dialysis, brain surgery, liver surgery, nutritional referrals and ICD-10-codes for RFS (E83.3 and E87.7)
- -
- Primary outcome in prospective evaluation: can the CDSS facilitated RFS diagnosis be confirmed by clinical experts?
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stanga, Z.; Brunner, A.; Leuenberger, M.; Grimble, R.F.; Shenkin, A.; Allison, S.P.; Lobo, D.N. Nutrition in clinical practice-the refeeding syndrome: Illustrative cases and guidelines for prevention and treatment. Eur. J. Clin. Nutr. 2008, 62, 687–694. [Google Scholar] [CrossRef]
- Nguyen, P.; Schlögl, H.; Selig, L.; Baerwald, C. Refeeding-Syndrom: Pathophysiologie, Therapie und welche rheumatologischen Patienten besonders gefährdet sind. Z. Rheumatol. 2021, 80, 263–269. [Google Scholar] [CrossRef] [PubMed]
- da Silva, J.S.V.; Seres, D.S.; Sabino, K.; Adams, S.C.; Berdahl, G.J.; Citty, S.W.; Cober, M.P.; Evans, D.C.; Greaves, J.R.; Gura, K.M.; et al. ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr. Clin. Pract. 2020, 35, 178–195. [Google Scholar] [CrossRef] [PubMed]
- Zeki, S.; Culkin, A.; Gabe, S.M.; Nightingale, J.M. Refeeding hypophosphataemia is more common in enteral than parenteral feeding in adult in patients. Clin. Nutr. 2011, 30, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Boateng, A.A.; Sriram, K.; Meguid, M.M.; Crook, M. Refeeding syndrome: Treatment considerations based on collective analysis of literature case reports. Nutrition 2010, 26, 156–167. [Google Scholar] [CrossRef]
- Wirth, R.; Diekmann, R.; Janssen, G.; Fleiter, O.; Fricke, L.; Kreilkamp, A.; Modreker, M.K.; Marburger, C.; Nels, S.; Pourhassan, M.; et al. Refeeding-Syndrom: Pathophysiologie, Risikofaktoren, Prophylaxe und Therapie. Internist 2018, 59, 326–333. [Google Scholar] [CrossRef]
- Ponzo, V.; Pellegrini, M.; Cioffi, I.; Scaglione, L.; Bo, S. The Refeeding Syndrome: A neglected but potentially serious condition for inpatients. A narrative review. Intern. Emerg. Med. 2021, 16, 49–60. [Google Scholar] [CrossRef]
- Vest, M.T.; Papas, M.A.; Shapero, M.; McGraw, P.; Capizzi, A.; Jurkovitz, C. Characteristics and Outcomes of Adult Inpatients With Malnutrition. JPEN J. Parenter. Enteral Nutr. 2018, 42, 1009–1016. [Google Scholar] [CrossRef]
- Cioffi, I.; Ponzo, V.; Pellegrini, M.; Evangelista, A.; Bioletto, F.; Ciccone, G.; Pasanisi, F.; Ghigo, E.; Bo, S. The incidence of the refeeding syndrome. A systematic review and meta-analyses of literature. Clin. Nutr. 2021, 40, 3688–3701. [Google Scholar] [CrossRef]
- Friedli, N.; Baumann, J.; Hummel, R.; Kloter, M.; Odermatt, J.; Fehr, R.; Felder, S.; Baechli, V.; Geiser, M.; Deiss, M.; et al. Refeeding syndrome is associated with increased mortality in malnourished medical inpatients: Secondary analysis of a randomized trial. Medicine 2020, 99, e18506. [Google Scholar] [CrossRef]
- Kraaijenbrink, B.; Lambers, W.M.; Mathus-Vliegen, E.; Siegert, C. Incidence of refeeding syndrome in internal medicine patients. Neth. J. Med. 2016, 74, 116–121. [Google Scholar] [PubMed]
- Bioletto, F.; Pellegrini, M.; Ponzo, V.; Cioffi, I.; de Francesco, A.; Ghigo, E.; Bo, S. Impact of Refeeding Syndrome on Short- and Medium-Term All-Cause Mortality: A Systematic Review and Meta-Analysis. Am. J. Med. 2021, 134, 1009–1018.e1. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.L.; Lo, L.; Ferguson, J.; Goldberg, H.; Diaz-Martinez, J.P.; Tomlinson, G.; Grimshaw, J.M.; Shojania, K.G. Computerised clinical decision support systems and absolute improvements in care: Meta-analysis of controlled clinical trials. BMJ 2020, 370, m3216. [Google Scholar] [CrossRef]
- Garg, A.X.; Adhikari, N.K.J.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef] [PubMed]
- Heuft, L.; Voigt, J.; Selig, L.; Stumvoll, M.; Schlögl, H.; Kaiser, T. Refeeding Syndrome—Diagnostic Challenges and the Potential of Clinical Decision Support Systems. Dtsch. Arztebl. Int. 2023, 120, 107–114. [Google Scholar] [CrossRef]
- Datta, H.K.; Malik, M.; Neely, R.D.G. Hepatic surgery-related hypophosphatemia. Clin. Chim. Acta 2007, 380, 13–23. [Google Scholar] [CrossRef]
- Leung, J.; Crook, M. Disorders of phosphate metabolism. J. Clin. Pathol. 2019, 72, 741–747. [Google Scholar] [CrossRef]
- Hong, Y.; Wang, X.-H.; Xiong, Y.-T.; Li, J.; Liu, C.-F. Association Between Admission Serum Phosphate Level and All-Cause Mortality Among Patients with Spontaneous Intracerebral Hemorrhage. Risk Manag. Healthc. Policy 2021, 14, 3739–3746. [Google Scholar] [CrossRef]
- Jiménez, J.V.; Carrillo-Pérez, D.L.; Rosado-Canto, R.; García-Juárez, I.; Torre, A.; Kershenobich, D.; Carrillo-Maravilla, E. Electrolyte and Acid-Base Disturbances in End-Stage Liver Disease: A Physiopathological Approach. Dig. Dis. Sci. 2017, 62, 1855–1871. [Google Scholar] [CrossRef]
- Nafidi, O.; Lapointe, R.W.; Lepage, R.; Kumar, R.; D’Amour, P. Mechanisms of renal phosphate loss in liver resection-associated hypophosphatemia. Ann. Surg. 2009, 249, 824–827. [Google Scholar] [CrossRef]
- Walter Costa, M.B.; Wernsdorfer, M.; Kehrer, A.; Voigt, M.; Cundius, C.; Federbusch, M.; Eckelt, F.; Remmler, J.; Schmidt, M.; Pehnke, S.; et al. The Clinical Decision Support System AMPEL for Laboratory Diagnostics: Implementation and Technical Evaluation. JMIR Med. Inform. 2021, 9, e20407. [Google Scholar] [CrossRef] [PubMed]
- Nutrition Support for Adults: Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition; National Institute for Health and Care Excellence: London, UK, 2006; ISBN 978-1-4731-1910-9.
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Polderman, K.H.; Bloemers, F.W.; Peerdeman, S.M.; Girbes, A.R. Hypomagnesemia and hypophosphatemia at admission in patients with severe head injury. Crit. Care Med. 2000, 28, 2022–2025. [Google Scholar] [CrossRef]
- Janssen, G.; Pourhassan, M.; Lenzen-Großimlinghaus, R.; Jäger, M.; Schäfer, R.; Spamer, C.; Cuvelier, I.; Volkert, D.; Wirth, R.; Janssen, G.; et al. The Refeeding Syndrome revisited: You can only diagnose what you know. Eur. J. Clin. Nutr. 2019, 73, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S. The Investigation of Parenteral Nutrition-Aotearoa (IPNA): Setting Up the 1st Phase of a Clinical Audit of the Delivery of Parenteral Nutrition (PN) in New Zealand (NZ). Master’s Thesis, Massey University, Albany, New Zealand, 2012. [Google Scholar]
- Dyson, J.K.; Thompson, N. Adult parenteral nutrition in the North of England: A region-wide audit. BMJ Open 2017, 7, e012663. [Google Scholar] [CrossRef] [PubMed]
- Friedli, N.; Stanga, Z.; Sobotka, L.; Culkin, A.; Kondrup, J.; Laviano, A.; Mueller, B.; Schuetz, P. Revisiting the refeeding syndrome: Results of a systematic review. Nutrition 2017, 35, 151–160. [Google Scholar] [CrossRef]
- Aubry, E.; Aeberhard, C.; Leuenberger, M.; Stirnimann, J.; Friedli, N.; Schütz, P.; Stanga, Z. Refeeding-Syndrom: Ein konsensusbasierter Algorithmus für stationäre Patienten. Aktuel Ernahrungsmed 2019, 44, 33–42. [Google Scholar] [CrossRef]
- Friedli, N.; Stanga, Z.; Culkin, A.; Crook, M.; Laviano, A.; Sobotka, L.; Kressig, R.W.; Kondrup, J.; Mueller, B.; Schuetz, P. Management and prevention of refeeding syndrome in medical inpatients: An evidence-based and consensus-supported algorithm. Nutrition 2018, 47, 13–20. [Google Scholar] [CrossRef]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef]
- Pirlich, M.; Schütz, T.; Norman, K.; Gastell, S.; Lübke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Güldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef]
- Volkert, D.; Weber, J.; Kiesswetter, E.; Sulz, I.; Hiesmayr, M. Ernährungssituation in Krankenhäusern und Pflegeheimen-Auswertung der nutritionDay-Daten für Deutschland. In 14 DGE Ernährungsbericht 2019; Deutsche Gesellschaft für Ernährung e. V.(DGE): Bonn, Germany, 2019; pp. V2–V669. [Google Scholar]
- Tobert, C.M.; Mott, S.L.; Nepple, K.G. Malnutrition Diagnosis during Adult Inpatient Hospitalizations: Analysis of a Multi-Institutional Collaborative Database of Academic Medical Centers. J. Acad. Nutr. Diet. 2018, 118, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.; Kleine, M.; Gessner, S.I.; Sandmann, S.; Dugas, M. Effects of computerized decision support system implementations on patient outcomes in inpatient care: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Moja, L.; Kwag, K.H.; Lytras, T.; Bertizzolo, L.; Brandt, L.; Pecoraro, V.; Rigon, G.; Vaona, A.; Ruggiero, F.; Mangia, M.; et al. Effectiveness of computerized decision support systems linked to electronic health records: A systematic review and meta-analysis. Am. J. Public Health 2014, 104, e12–e22. [Google Scholar] [CrossRef]
- Taheri Moghadam, S.; Sadoughi, F.; Velayati, F.; Ehsanzadeh, S.J.; Poursharif, S. The effects of clinical decision support system for prescribing medication on patient outcomes and physician practice performance: A systematic review and meta-analysis. BMC Med. Inform. Decis. Mak. 2021, 21, 98. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Ehrbar, N. Effects of Computerized Decision Support Systems on Practitioner Performance and Patient Outcomes: Systematic Review. JMIR Med. Inform. 2020, 8, e17283. [Google Scholar] [CrossRef]
- Ronan, C.E.; Crable, E.L.; Drainoni, M.-L.; Walkey, A.J. The impact of clinical decision support systems on provider behavior in the inpatient setting: A systematic review and meta-analysis. J. Hosp. Med. 2022, 17, 368–383. [Google Scholar] [CrossRef]
- Ettori, F.; Henin, A.; Zemmour, C.; Chow-Chine, L.; Sannini, A.; Bisbal, M.; Gonzalez, F.; Servan, L.; de Guibert, J.M.; Faucher, M.; et al. Impact of a computer-assisted decision support system (CDSS) on nutrition management in critically ill hematology patients: The NUTCHOCO study (nutritional care in hematology oncologic patients and critical outcome). Ann. Intensive Care 2019, 9, 53. [Google Scholar] [CrossRef]
- Pielmeier, U.; Rousing, M.L.; Andreassen, S.; Nielsen, B.S.; Haure, P. Decision support for optimized blood glucose control and nutrition in a neurotrauma intensive care unit: Preliminary results of clinical advice and prediction accuracy of the Glucosafe system. J. Clin. Monit. Comput. 2012, 26, 319–328. [Google Scholar] [CrossRef]
- Kouri, A.; Yamada, J.; Lam Shin Cheung, J.; van de Velde, S.; Gupta, S. Do providers use computerized clinical decision support systems? A systematic review and meta-regression of clinical decision support uptake. Implement. Sci. 2022, 17, 21. [Google Scholar] [CrossRef]
- Haase-Fielitz, A.; Elitok, S.; Schostak, M.; Ernst, M.; Isermann, B.; Albert, C.; Robra, B.-P.; Kribben, A.; Haase, M. The Effects of Intensive Versus Routine Treatment in Patients with Acute Kidney Injury. Dtsch. Arztebl. Int. 2020, 117, 289–296. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Retrospective Cohort | Prospective Cohort | |||
|---|---|---|---|---|
| True Positive (n = 100) | False Positive (n = 30) | True Positive (n = 21) | False Positive (n = 10) | |
| Sex [m/f] | 58%/42% | 46%/53% | 38%/62% | 80%/20% |
| Age [years] | 65 [58; 76] | 66 [50; 77] | 65 [56; 74] | 67 [59; 74] |
| BMI [kg/m2] | ||||
| male | 24.1 [20.8; 26.9] | 22.9 [22; 24.6] | 21.6 [17.4; 21.6] | 23.6 [21.7; 25.9] |
| female | 20.3 [18.3; 23.9] | 25 [20.9; 29.8] | 20 [19.1; 24.5] | 23.7 [23.3; 24.1] |
| Red. food intake | ||||
| Yes | 56% (56) | 40% (12) | 47% (10) | 60% (6) |
| No | 40% (40) | 53% (16) | 53% (11) | 40% (4) |
| NA | 4% (4) | 8% (2) | - | - |
| NRS-2002 | 4 [4; 5] (n = 28) | 4 [1; 5] (n = 4) | 4 [3; 5] (n = 20) | 2 [2; 2] (n = 7) |
| Positive NICE criteria | 52% (52) | 3.3% (n = 1) | 71.4% (n = 15) | 10% (n = 1) |
| Alert-severity | ||||
| mild | 46% (46) | 10% (3) | 9.5% (2) | 60% (6) |
| moderate | 30% (30) | 53% (16) | 57.5% (12) | 30% (3) |
| severe | 24% (24) | 37% (11) | 33% (7) | 10% (1) |
| Phosphate [mmol/L] | 0.53 [0.46; 0.58] | 0.55 [0.47; 0.61] | 0.48 [0.43; 0.53] | 0.66 [0.55; 0.75] |
| Potassium [mmol/L] | 3.04 [2.78; 3.31] | 2.9 [2.8; 3.3] | 3 [2.78; 3.09] | 3.09 [3.04; 3.32] |
| Magnesium [mmol/L] | 0.71 [0.6; 0.78] | 0.76 [0.63; 0.82] | 0.71 [0.63; 0.76] | 0.66 [0.6; 0.74] |
| ICD-10 | ||||
| E83.3 | 21% (21) | 26% (8) | 19% (4) | 0 |
| E87.7 | 1% (1) | 0 | 19% (4) | 0 |
| No coding | 78% (78) | 74% (22) | 81% (17) | 100% (10) |
| Ward | ||||
| ICU | 40% (40) | 50% (15) | 24% (5) | 10% (1) |
| Non-ICU | 60% (60) | 50% (15) | 76% (16) | 90% (9) |
| Nutrition referral | ||||
| yes | 33% (33) | 10% (3) | 71% (15) | 60% (6) |
| no | 67% (67) | 90% (27) | 29% (6) | 40% (4) |
| Question | Given Answers | Count |
|---|---|---|
| Are you familiar with refeeding syndrome? | yes | 16 |
| no | 8 | |
| Which laboratory value would you use to diagnose refeeding syndrome? | Unknown | 11 |
| Glucose | 1 | |
| Phosphate | 8 | |
| Electrolytes | 4 | |
| Does the patient show a new symptom today? | Diarrhea | 1 |
| Abdominal pain | 2 | |
| Weakness | 2 | |
| Weight loss | 1 | |
| Hypokalemia | 1 | |
| No new symptom | 16 | |
| Not available | 1 | |
| Did you already consider a referral the clinical nutrition department? | Yes | 3 |
| Not available | 1 | |
| No * | 20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heuft, L.; Voigt, J.; Selig, L.; Schmidt, M.; Eckelt, F.; Steinbach, D.; Federbusch, M.; Stumvoll, M.; Schlögl, H.; Isermann, B.; et al. Development, Design and Utilization of a CDSS for Refeeding Syndrome in Real Life Inpatient Care—A Feasibility Study. Nutrients 2023, 15, 3712. https://doi.org/10.3390/nu15173712
Heuft L, Voigt J, Selig L, Schmidt M, Eckelt F, Steinbach D, Federbusch M, Stumvoll M, Schlögl H, Isermann B, et al. Development, Design and Utilization of a CDSS for Refeeding Syndrome in Real Life Inpatient Care—A Feasibility Study. Nutrients. 2023; 15(17):3712. https://doi.org/10.3390/nu15173712
Chicago/Turabian StyleHeuft, Lara, Jenny Voigt, Lars Selig, Maria Schmidt, Felix Eckelt, Daniel Steinbach, Martin Federbusch, Michael Stumvoll, Haiko Schlögl, Berend Isermann, and et al. 2023. "Development, Design and Utilization of a CDSS for Refeeding Syndrome in Real Life Inpatient Care—A Feasibility Study" Nutrients 15, no. 17: 3712. https://doi.org/10.3390/nu15173712
APA StyleHeuft, L., Voigt, J., Selig, L., Schmidt, M., Eckelt, F., Steinbach, D., Federbusch, M., Stumvoll, M., Schlögl, H., Isermann, B., & Kaiser, T. (2023). Development, Design and Utilization of a CDSS for Refeeding Syndrome in Real Life Inpatient Care—A Feasibility Study. Nutrients, 15(17), 3712. https://doi.org/10.3390/nu15173712