
Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders among Gender-Diverse Adults Assigned Male at Birth in Bangkok, Thailand



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Approval
2.2. Participants and Recruitment Procedures
2.3. Questionnaire and Data Collection
2.4. Statistical Analysis
3. Results
3.1. Descriptive Characteristics
3.2. Differences in Weight-Related Variables according to Gender Expression
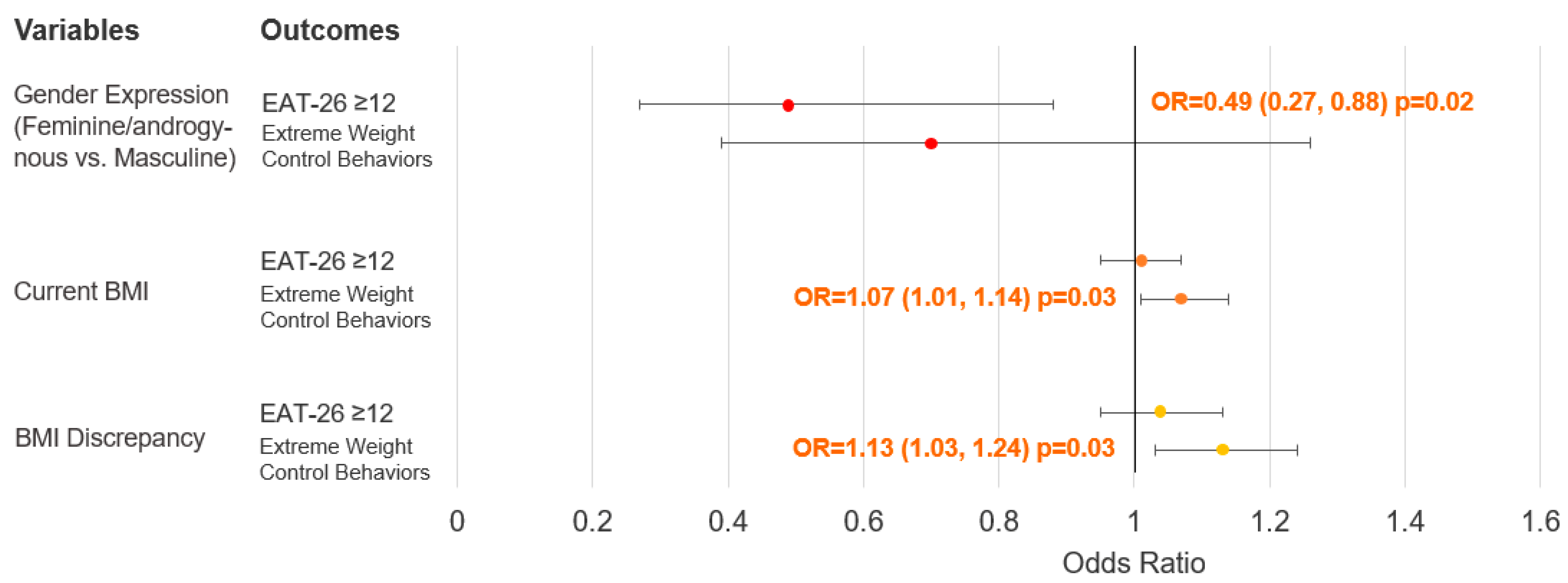
3.3. Association between Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders
4. Discussion
4.1. Association between Gender Expression and Weight Status
4.2. Association between Gender Expression and Risk of Experiencing Eating Disorders
4.3. Association between Weight Status and Risk of Experiencing Eating Disorders
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, L.L.; Harriger, J.A. Eating disorders and disordered eating behaviors in the LGBT population: A review of the literature. J. Eat. Disord. 2020, 8, 51. [Google Scholar] [CrossRef]
- McConnell, E.A.; Janulis, P.; Phillips, G., II; Truong, R.; Birkett, M. Multiple minority stress and LGBT community resilience among sexual minority men. Psychol. Sex. Orientat. Gend. Divers. 2018, 5, 1–12. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Pachankis, J.E. Stigma and Minority Stress as Social Determinants of Health Among Lesbian, Gay, Bisexual, and Transgender Youth: Research evidence and clinical implications. Pediatr. Clin. N. Am. 2016, 63, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Diemer, E.W.; Hughto, J.M.W.; Gordon, A.R.; Guss, C.; Austin, S.B.; Reisner, S.L. Beyond the Binary: Differences in Eating Disorder Prevalence by Gender Identity in a Transgender Sample. Transgend. Health 2018, 3, 17–23. [Google Scholar] [CrossRef]
- Coelho, J.S.; Lee, T.; Karnabi, P.; Burns, A.; Marshall, S.; Geller, J.; Lam, P.-Y. Eating disorders in biological males: Clinical presentation and consideration of sex differences in a pediatric sample. J. Eat. Disord. 2018, 6, 40. [Google Scholar] [CrossRef]
- Panza, E.; Fehling, K.B.; Pantalone, D.W.; Dodson, S.; Selby, E.A. Multiply marginalized: Linking minority stress due to sexual orientation, gender, and weight to dysregulated eating among sexual minority women of higher body weight. Psychol. Sex. Orientat. Gend. Divers. 2021, 8, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H. Sexual Health Determinants of Normal Weight, Overweight, and Obese Sexual Minority Men. J. Obes. 2021, 2021, 1272316. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.; Suh, Y. Stigma and Eating and Weight Disorders. Curr. Psychiatry Rep. 2015, 17, 552. [Google Scholar] [CrossRef]
- Simone, M.; Pisetsky, E.M.; Lust, K. Weight discrimination inflates psychological health risk and academic impairment in sexual minority cisgender college students relative to their heterosexual peers. Eat. Disord. 2021, 29, 685–695. [Google Scholar] [CrossRef]
- O’Brien, K.S.; Latner, J.D.; Puhl, R.M.; Vartanian, L.R.; Giles, C.; Griva, K.; Carter, A. The relationship between weight stigma and eating behavior is explained by weight bias internalization and psychological distress. Appetite 2016, 102, 70–76. [Google Scholar] [CrossRef]
- Puhl, R.M.; Himmelstein, M.S.; Pearl, R.L.; Wojtanowski, A.C.; Foster, G.D. Weight Stigma Among Sexual Minority Adults: Findings from a Matched Sample of Adults Engaged in Weight Management. Obesity 2019, 27, 1906–1915. [Google Scholar] [CrossRef]
- Meneguzzo, P.; Collantoni, E.; Meregalli, V.; Favaro, A.; Tenconi, E. Addressing Weight Bias in the Cisgender Population: Differences between Sexual Orientations. Nutrients 2022, 14, 1735. [Google Scholar] [CrossRef] [PubMed]
- Yasami, M.; Zhu, H.; Dewan, M. Poverty, Psychological Distress, and Suicidality among Gay Men and Transgender Women Sex Workers During the COVID-19 Pandemic in Phuket, Thailand. Sex. Res. Soc. Policy 2023, 20, 1203–1219. [Google Scholar] [CrossRef]
- Newman, P.A.; Reid, L.; Tepjan, S.; Akkakanjanasupar, P. LGBT+ inclusion and human rights in Thailand: A scoping review of the literature. BMC Public Health 2021, 21, 1816. [Google Scholar] [CrossRef]
- Moallef, S.; Salway, T.; Phanuphak, N.; Kivioja, K.; Pongruengphant, S.; Hayashi, K. The relationship between sexual and gender stigma and suicide attempt and ideation among LGBTQI + populations in Thailand: Findings from a national survey. Soc. Psychiatry 2022, 57, 1987–1997. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Papini, N.M.; Jung, M.; Cook, A.; Lopez, N.V.; Ptomey, L.T.; Herrmann, S.D.; Kang, M. Psychometric properties of the 26-item eating attitudes test (EAT-26): An application of rasch analysis. J. Eat. Disord. 2022, 10, 62. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.J.; Keel, P.K. Homosexuality as a specific risk factor for eating disorders in men. Int. J. Eat. Disord. 2002, 31, 300–306. [Google Scholar] [CrossRef]
- De Santis, J.P.; Layerla, D.M.; Barroso, S.; Gattamorta, K.A.; Sanchez, M.; Prado, G.J. Predictors of Eating Attitudes and Behaviors Among Gay Hispanic Men. Arch. Psychiatr. Nurs. 2012, 26, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Gulec, H.; Torun, T.; Prado, A.d.S.; Bauer, S.; Rummel-Kluge, C.; Kohls, E. Eating attitudes and depressive symptoms in a LGBTIQ sample in Turkey. Front. Psychiatry 2022, 13, 1014253. [Google Scholar] [CrossRef]
- Kaewporndawan, T.; Pariwatcharakul, P.; Pimratana, W. Criterion validity study of the eating attitudes test-26 (eat-26 thai version) among thai females. J. Psychiatr. Assoc. Thail. 2013, 58, 283–296. [Google Scholar]
- Orbitello, B.; Ciano, R.; Corsaro, M.; Rocco, P.L.; Taboga, C.; Tonutti, L.; Armellini, M.; Balestrieri, M. The EAT-26 as screening instrument for clinical nutrition unit attenders. Int. J. Obes. 2006, 30, 977–981. [Google Scholar] [CrossRef]
- Kittiteerasack, P.; Matthews, A.K.; Steffen, A. The Validity and Linguistic Testing of Translated Measures of Sexual Orientation and Gender Identity for Research in Lesbian, Gay, Bisexual, and Transgender (LGBT) Populations in Thailand. Nurs. J. 2019, 46, 122–137. [Google Scholar]
- Iyer, S.; Shriraam, V. Prevalence of Eating Disorders and Its Associated Risk Factors in Students of a Medical College Hospital in South India. Cureus 2021, 13, e12926. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Ohlsson, H.; Winkleby, M.A.; Sundquist, K.; Crump, C. School Achievement and Risk of Eating Disorders in a Swedish National Cohort. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 41–46.e1. [Google Scholar] [CrossRef] [PubMed]
- Schilder, C.M.T.; Sternheim, L.C.; Aarts, E.; Elburg, A.A.; Danner, U.N. Relationships between educational achievement, intelligence, and perfectionism in adolescents with eating disorders. Int. J. Eat. Disord. 2021, 54, 794–801. [Google Scholar] [CrossRef]
- Ancheta, A.J.; Caceres, B.A.; Jackman, K.B.; Kreuze, E.; Hughes, T.L. Sexual Identity Differences in Health Behaviors and Weight Status among Urban High School Students. Behav. Med. 2021, 47, 259–271. [Google Scholar] [CrossRef]
- Austin, S.B.; Ziyadeh, N.J.; Calzo, J.P.; Sonneville, K.R.; Kennedy, G.A.; Roberts, A.L.; Haines, J.; Scherer, E.A. Gender expression associated with BMI in a prospective cohort study of US adolescents. Obesity 2016, 24, 506–515. [Google Scholar] [CrossRef]
- Hernández-López, M.; Quiñones-Jiménez, L.; Blanco-Romero, A.L.; Rodríguez-Valverde, M. Testing the discrepancy between actual and ideal body image with the Implicit Relational Assessment Procedure (IRAP). J. Eat. Disord. 2021, 9, 82. [Google Scholar] [CrossRef]
- Rolls, B.J.; Fedoroff, I.C.; Guthrie, J.F. Gender differences in eating behavior and body weight regulation. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 1991, 10, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Breton, É.; Juster, R.; Booij, L. Gender and sex in eating disorders: A narrative review of the current state of knowledge, research gaps, and recommendations. Brain Behav. 2023, 13, e2871. [Google Scholar] [CrossRef] [PubMed]
- López-Guimerà, G.; Neumark-Sztainer, D.; Hannan, P.; Fauquet, J.; Loth, K.; Sánchez-Carracedo, D. Unhealthy Weight-control Behaviours, Dieting and Weight Status: A Cross-cultural Comparison between North American and Spanish Adolescents. Eur. Eat. Disord. Rev. 2013, 21, 276–283. [Google Scholar] [CrossRef]
- Sahasakul, Y.; Amonsusawat, N.; Phansuea, P. Lifestyles, Food Consumption Frequencies, and Eating Behaviors among Three Main Disciplines of Undergraduate Students during the Early COVID-19 Outbreak in Thailand. Nutrients 2023, 15, 2765. [Google Scholar] [CrossRef]
- da Silva, W.R.; Santana, M.d.S.; Maroco, J.; Maloa, B.F.S.; Campos, J.A.D.B. Body weight concerns: Cross-national study and identification of factors related to eating disorders. PLoS ONE 2017, 12, e0180125. [Google Scholar] [CrossRef]
- Lee, K.M.; Hunger, J.M.; Tomiyama, A.J. Weight stigma and health behaviors: Evidence from the Eating in America Study. Int. J. Obes. 2021, 45, 1499–1509. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.; Ganson, K.T.; Vittinghoff, E.; Mitchison, D.; Hay, P.; Tabler, J.; Rodgers, R.F.; Murray, S.B.; Nagata, J.M. Weight Goals, Disordered Eating Behaviors, and BMI Trajectories in US Young Adults. J. Gen. Intern. Med. 2021, 36, 2622–2630. [Google Scholar] [CrossRef]
- Lee, J.; Lee, Y. The association of body image distortion with weight control behaviors, diet behaviors, physical activity, sadness, and suicidal ideation among Korean high school students: A cross-sectional study. BMC Public Health 2016, 16, 39. [Google Scholar] [CrossRef]
- Bouzas, C.; Bibiloni, M.d.M.; Tur, J.A. Relationship between Body Image and Body Weight Control in Overweight ≥55-Year-Old Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1622. [Google Scholar] [CrossRef]
- Lantz, E.L.; Gaspar, M.E.; DiTore, R.; Piers, A.D.; Schaumberg, K. Conceptualizing body dissatisfaction in eating disorders within a self-discrepancy framework: A review of evidence. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2018, 23, 275–291. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Descriptive Characteristics | Total (n = 217) | t- or χ2 Value (df) | Gender Expression | p-Value | |
|---|---|---|---|---|---|
| Masculine (n = 137) | Feminine/Androgynous (n = 80) | ||||
| Age, years, mean (SD) | 29.9 (6.19) | 0.83 (215) | 30.2 (6.02) | 29.5 (6.49) | 0.41 ‡ |
| Birthplace, n (%) | 0.05 (1) | 0.82 § | |||
| Bangkok | 128 (59.0%) | 80 (58.4%) | 48 (60.0%) | ||
| Other provinces | 89 (41.0%) | 57 (41.6%) | 32 (40.0%) | ||
| Income per month, n (%) | 7.75 (3) | 0.05 § | |||
| Quartile 1 (THB 21,500 ¶ or less) | 54 (24.9%) | 27 (19.7%) | 27 (33.8%) | ||
| Quartile 2 (THB 21,501–33,000 ¶) | 51 (23.5%) | 30 (21.9%) | 21 (26.3%) | ||
| Quartile 3 (THB 33,001–60,000 ¶) | 61 (28.1%) | 44 (32.1%) | 17 (21.3%) | ||
| Quartile 4 (THB 60,001 ¶ or more) | 51 (23.5%) | 36 (26.3%) | 15 (18.8%) | ||
| Current Living status, n (%) | 1.09 (2) | 0.58 § | |||
| Alone | 92 (42.4%) | 59 (43.1%) | 33 (41.3%) | ||
| With Friends/Family | 92 (42.4%) | 55 (40.1%) | 37 (46.3%) | ||
| With partner/couple | 33 (15.2%) | 23 (16.8%) | 10 (12.5%) | ||
| Religion, n (%) | 1.08 (2) | 0.58 § | |||
| Atheist | 69 (31.8%) | 43 (31.4%) | 26 (32.5%) | ||
| Buddhist | 142 (65.4%) | 89 (65.0%) | 53 (66.3%) | ||
| Other religion | 6 (2.8%) | 5 (3.6%) | 1 (1.3%) | ||
| Educational attainment, n (%) | 0.62 (1) | 0.43 § | |||
| Lower than bachelor’s degree | 8 (3.7%) | 4 (2.9%) | 4 (5.0%) | ||
| Bachelor’s degree or higher | 209 (96.3%) | 133 (97.1%) | 76 (95.0%) | ||
| Relationship Status, n (%) | 4.91 (1) | 0.03 § | |||
| Single | 131 (60.4%) | 75 (54.7%) | 56 (70.0%) | ||
| Partnered/Married | 86 (39.6%) | 62 (45.3%) | 24 (30.0%) | ||
| Current Smoking Status, n (%) | 0.94 (1) | 0.33 § | |||
| Yes | 12 (5.5%) | 6 (4.4%) | 6 (7.5%) | ||
| No | 205 (94.5%) | 131 (95.6%) | 74 (92.5%) | ||
| Current Alcohol Consumption, n (%) | 2.88 (1) | 0.09 § | |||
| Yes | 74 (34.1%) | 41 (29.9%) | 33 (41.3%) | ||
| No | 143 (65.9%) | 96 (70.1%) | 47 (58.8%) | ||
| History of Mental Health Issues, n (%) | 0.03 (1) | 0.86 § | |||
| Yes | 26 (12.0%) | 16 (11.7%) | 10 (12.5%) | ||
| No/unsure | 191 (88.0%) | 121 (88.3%) | 70 (87.5%) | ||
| Weight-Related Variables | t- or χ2 Value (df) | Gender Expression | p-Value | |
|---|---|---|---|---|
| Masculine (n = 137) | Feminine/Androgynous (n = 80) | |||
| Current BMI †, kg/m2, mean (SD) | 0.19 (122.7) | 23.5 (4.01) | 23.4 (5.86) | 0.85 ‡ |
| BMI † Category, n (%) | 7.03 (4) | 0.13 § | ||
| Underweight | 4 (2.9%) | 7 (8.8%) | ||
| Normal weight | 64 (46.7%) | 43 (53.8%) | ||
| Overweight | 34 (24.8%) | 12 (15.0%) | ||
| Obesity class I | 27 (19.7%) | 12 (15.0%) | ||
| Obesity class II | 8 (5.8%) | 6 (7.5%) | ||
| Ideal BMI †, kg/m2, mean (SD) | 1.22 (215) | 22.3 (2.17) | 21.9 (2.57) | 0.22 § |
| BMI † Discrepancy ¶, kg/m2, mean (SD) | −0.52 (119.5) | 1.2 (2.65) | 1.5 (4.04) | 0.60 ‡ |
| Variables | Total EAT-26 Score | Dieting Subscale | Bulimia and Food Preoccupation Subscale | Oral Control Subscale |
|---|---|---|---|---|
| Gender Expression | ||||
| Masculine | Ref. | Ref. | Ref. | Ref. |
| Feminine/Androgynous | −2.43 (1.08) p = 0.03 | −2.43 (0.83) p = 0.004 | 0.16 (0.27) p = 0.54 | −0.15 (0.40) p = 0.70 |
| Current BMI † | 0.001 (0.11) p = 0.99 | 0.13 (0.09) p = 0.14 | 0.09 (0.03) p < 0.001 | −0.22 (0.04) p < 0.001 |
| BMI † discrepancy ‡ | 0.13 (0.16) p = 0.43 | 0.26 (0.13) p = 0.04 | 0.14 (0.04) p < 0.001 | −0.27 (0.06) p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vinitchagoon, T.; Wongpipit, W.; Phansuea, P. Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders among Gender-Diverse Adults Assigned Male at Birth in Bangkok, Thailand. Nutrients 2023, 15, 3700. https://doi.org/10.3390/nu15173700
Vinitchagoon T, Wongpipit W, Phansuea P. Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders among Gender-Diverse Adults Assigned Male at Birth in Bangkok, Thailand. Nutrients. 2023; 15(17):3700. https://doi.org/10.3390/nu15173700
Chicago/Turabian StyleVinitchagoon, Thanit, Waris Wongpipit, and Phenphop Phansuea. 2023. "Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders among Gender-Diverse Adults Assigned Male at Birth in Bangkok, Thailand" Nutrients 15, no. 17: 3700. https://doi.org/10.3390/nu15173700
APA StyleVinitchagoon, T., Wongpipit, W., & Phansuea, P. (2023). Gender Expression, Weight Status, and Risk of Experiencing Eating Disorders among Gender-Diverse Adults Assigned Male at Birth in Bangkok, Thailand. Nutrients, 15(17), 3700. https://doi.org/10.3390/nu15173700