

Weight Regain and Ingestive Behavior in Women after Metabolic Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
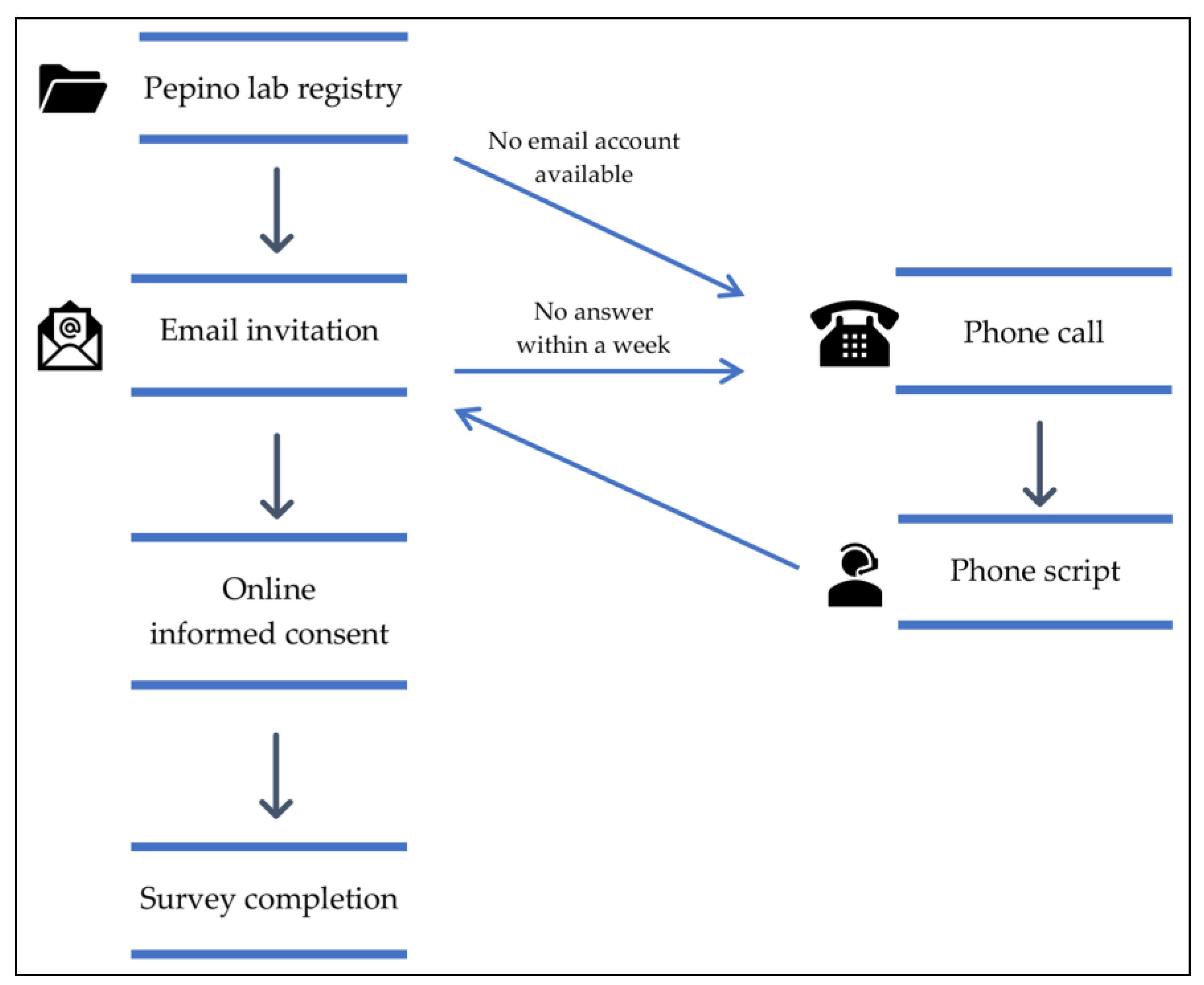
2.1. Participants
2.2. Study Procedures and Questionnaires
- Sociodemographic questionnaire. It includes personal information such as age, year of birth, sex, race, ethnicity, height, weight before surgery, current weight, lowest (nadir) weight after surgery (and date), type of bariatric surgery (and date), and pregnancy or breastfeeding status;
- Food-Craving Inventory (FCI) [23]. This validated tool measures the self-reported frequency of cravings for foods in general and specific foods. It encompasses four subscales: the frequency of cravings for high fats, carbohydrates, sweets, and fast-food fats in the past month, and it also obtains a total food craving score. Participants select their answers using a 5-point Likert scale (1 = never, 5 = always);
- Dutch Eating Behavior Questionnaire (DEBQ) [24]. This questionnaire evaluates restrained, emotional, and external eating. Restrained eating refers to consciously restricting food intake to control body weight; emotional eating considers eating in response to negative feelings such as stress or loneliness; and external eating refers to eating in response to external food cues such as sight or smell. Participants select their answers using a 5-point Likert scale (1 = never, 5 = very often);
- Eating Disorder Examination Questionnaire (EDE-Q) [25]. It assesses restraint, eating, shape, and weight concern over the past 28 days and obtains a global score that reflects the severity of eating disorder psychopathology. Participants select their answers using a 7-point Likert scale (0 = none of the time, 6 = every time);
- Additional eating disorder questions. We added questions about bariatric surgery-related eating behavior, such as loss of control when eating, grazing food between meals, and subjective overeating based on questions on the EDE-Bariatric Surgery Version (EDE-BSV) interview [26];
- Yale Food Addiction Scale (YFAS) version 2.0 [27]. This scale assesses addictive-like eating behavior in the past month according to the substance-related and addictive disorders section in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5) [28]. The scale allows the classification of participants into different categories depending on their food addiction symptoms: mild, moderate, and severe. Participants select their answers using an 8-point Likert scale (0 = never, 7 = every day);
- Alcohol Use Disorders Identification Test-Concise (AUDIT-C) [29]. This is a brief version (3 items) of the AUDIT questionnaire (10 items). Each item has five answer choices valued from 0 to 4 points. A score of 3 or more in women suggests hazardous drinking behavior or active alcohol use disorder.
2.3. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
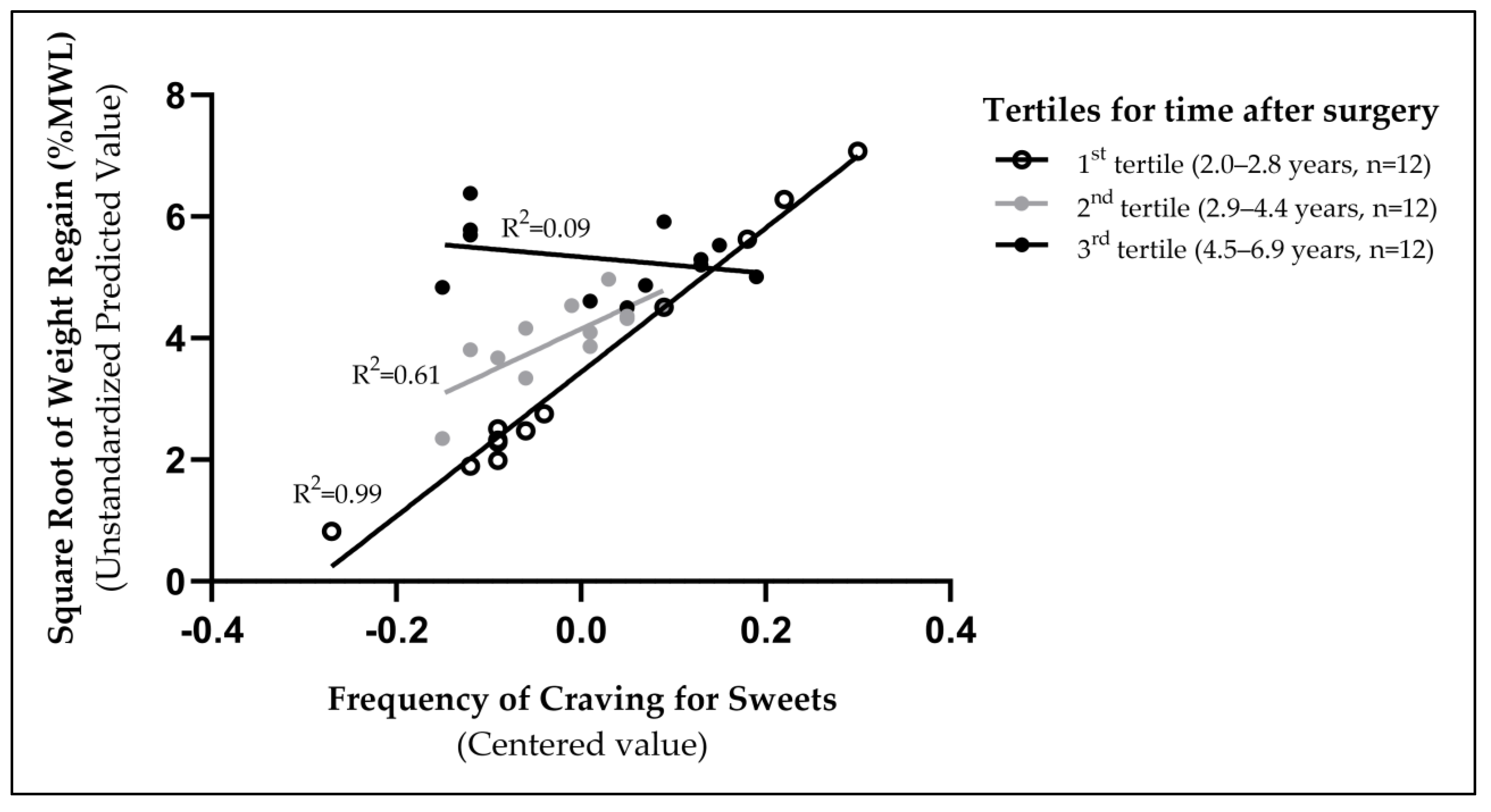
3.2. Weight Regain and Ingestive Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Timothy Garvey, W.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Non-surgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Obesity 2020, 28, O1–O58. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Adult Obesity Facts. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 7 May 2023).
- Jakobsen, G.S.; Småstuen, M.C.; Sandbu, R.; Nordstrand, N.; Hofsø, D.; Lindberg, M.; Hertel, J.K.; Hjelmesæth, J. Association of bariatric surgery vs medical obesity treatment with long-term medical complications and obesity-related comorbidities. JAMA-J. Am. Med. Assoc. 2018, 319, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef] [PubMed]
- English, W.J.; DeMaria, E.J.; Hutter, M.M.; Kothari, S.N.; Mattar, S.G.; Brethauer, S.A.; Morton, J.M. American Society for Metabolic and Bariatric Surgery 2018 estimate of metabolic and bariatric procedures performed in the United States. Surg. Obes. Relat. Dis. 2020, 16, 457–463. [Google Scholar] [CrossRef]
- O’brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes after Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef]
- English, W.J.; Williams, D.B. Metabolic and Bariatric Surgery: An Effective Treatment Option for Obesity and Cardiovascular Disease. Prog. Cardiovasc. Dis. 2018, 61, 253–269. [Google Scholar] [CrossRef]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; De Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for Metabolic and Bariatric Surgery. Surg. Obes. Relat. Dis. 2022, 18, 1345–1356. [Google Scholar] [CrossRef]
- King, W.C.; Hinerman, A.S.; Belle, S.H.; Wahed, A.S.; Courcoulas, A.P. Comparison of the Performance of Common Measures of Weight Regain After Bariatric Surgery for Association With Clinical Outcomes. JAMA 2018, 320, 1560–1569. [Google Scholar] [CrossRef]
- Athanasiadis, D.I.; Martin, A.; Kapsampelis, P.; Monfared, S.; Stefanidis, D. Factors associated with weight regain post-bariatric surgery: A systematic review. Surg. Endosc. 2021, 35, 4069–4084. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Bradley, D.; Eagon, J.C.; Sullivan, S.; Abumrad, N.A.; Klein, S. Changes in taste perception and eating behavior after bariatric surgery-induced weight loss in women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef]
- Nance, K.; Eagon, J.C.; Klein, S.; Pepino, M.Y. Effects of Sleeve Gastrectomy vs. Roux-en-Y Gastric Bypass on Eating Behavior and Sweet Taste Perception in Subjects with Obesity. Nutrients 2017, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Pepino, M.Y.; Stein, R.I.; Eagon, J.C.; Klein, S. Bariatric surgery-induced weight loss causes remission of food addiction in extreme obesity. Obesity 2014, 22, 1792–1798. [Google Scholar] [CrossRef] [PubMed]
- King, W.C.; Belle, S.H.; Hinerman, A.S.; Mitchell, J.E.; Steffen, K.J.; Courcoulas, A.P. Patient Behaviors and Characteristics Related to Weight Regain After Roux-en-Y Gastric Bypass: A Multicenter Prospective Cohort Study. Ann. Surg. 2020, 272, 1044–1052. [Google Scholar] [CrossRef]
- Bakr, A.A.; Fahmy, M.H.; Elward, A.S.; Balamoun, H.A.; Ibrahim, M.Y.; Eldahdoh, R.M. Analysis of Medium-Term Weight Regain 5 Years After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2019, 29, 3508–3513. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.C.; Simmons, E.B.; Webb, K.; Burns, J.L.; Kushner, R.F. Trends in Weight Regain Following Roux-en-Y Gastric Bypass (RYGB) Bariatric Surgery. Obes. Surg. 2015, 25, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Yanos, B.R.; Saules, K.K.; Schuh, L.M.; Sogg, S. Predictors of Lowest Weight and Long-Term Weight Regain Among Roux-en-Y Gastric Bypass Patients. Obes. Surg. 2015, 25, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- King, W.C.; Hinerman, A.S.; Courcoulas, A.P. Weight regain after bariatric surgery: A systematic literature review and comparison across studies using a large reference sample. Surg. Obes. Relat. Dis. 2020, 16, 1133–1144. [Google Scholar] [CrossRef]
- Ivezaj, V.; Benoit, S.C.; Davis, J.; Engel, S.; Lloret-Linares, C.; Mitchell, J.E.; Pepino, M.Y.; Rogers, A.M.; Steffen, K.; Sogg, S. Changes in Alcohol Use after Metabolic and Bariatric Surgery: Predictors and Mechanisms. Curr. Psychiatry Rep. 2019, 21, 85. [Google Scholar] [CrossRef]
- Acevedo, M.B.; Teran-Garcia, M.; Bucholz, K.K.; Eagon, J.C.; Bartholow, B.D.; Burd, N.A.; Khan, N.; Rowitz, B.; Pepino, M.Y. Alcohol sensitivity in women after undergoing bariatric surgery: A cross-sectional study. Surg. Obes. Relat. Dis. 2020, 16, 536–544. [Google Scholar] [CrossRef]
- Reslan, S.; Saules, K.K.; Greenwald, M.K.; Schuh, L.M. Substance misuse following Roux-en-Y gastric bypass surgery. Subst. Use Misuse 2014, 49, 405–417. [Google Scholar] [CrossRef]
- Fuchs, H.F.; Broderick, R.C.; Harnsberger, C.R.; Chang, D.C.; Sandler, B.J.; Jacobsen, G.R.; Horgan, S. Benefits of bariatric surgery do not reach obese men. J. Laparoendosc. Adv. Surg. Tech. A 2015, 25, 196–201. [Google Scholar] [CrossRef] [PubMed]
- White, M.A.; Whisenhunt, B.L.; Williamson, D.A.; Greenway, F.L.; Netemeyer, R.G. Development and validation of the food-craving inventory. Obes. Res. 2002, 10, 107–114. [Google Scholar] [CrossRef] [PubMed]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S. Eating disorder examination questionnaire. In Cognitive Behavior Therapy and Eating Disorders; Fairburn, C.G., Ed.; Guilford Press: New York, NY, USA, 2008; pp. 309–313. [Google Scholar]
- de Zwaan, M.; Hilbert, A.; Swan-Kremeier, L.; Simonich, H.; Lancaster, K.; Howell, L.M.; Monson, T.; Crosby, R.D.; Mitchell, J.E. Comprehensive interview assessment of eating behavior 18-35 months after gastric bypass surgery for morbid obesity. Surg. Obes. Relat. Dis. 2010, 6, 79–85. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef]
- Perez-Leighton, C.E.; Hamm, J.D.; Shechter, A.; Tamura, S.; Laferrère, B.; Xavier, P.-S.; Albu, J.; Greenberg, D.; Kissileff, H.R. Preoperative liking and wanting for sweet beverages as predictors of body weight loss after Roux-en-Y gastric bypass and sleeve gastrectomy. Int. J. Obes. 2020, 44, 1350–1359. [Google Scholar] [CrossRef]
- Smith, K.R.; Aghababian, A.; Papantoni, A.; Veldhuizen, M.G.; Kamath, V.; Harris, C.; Moran, T.H.; Carnell, S.; Steele, K.E. One Year Follow-Up of Taste-Related Reward Associations with Weight Loss Suggests a Critical Time to Mitigate Weight Regain Following Bariatric Surgery. Nutrients 2021, 13, 3943. [Google Scholar] [CrossRef]
- Smith, K.R.; Papantoni, A.; Veldhuizen, M.G.; Kamath, V.; Harris, C.; Moran, T.H.; Carnell, S.; Steele, K.E. Taste-related reward is associated with weight loss following bariatric surgery. J. Clin. Investig. 2020, 130, 4370–4381. [Google Scholar] [CrossRef]
- Sciamanna, C.N.; Kiernan, M.; Rolls, B.J.; Boan, J.; Stuckey, H.; Kephart, D.; Miller, C.K.; Jensen, G.; Hartmann, T.J.; Loken, E.; et al. Practices associated with weight loss versus weight-loss maintenance results of a national survey. Am. J. Prev. Med. 2011, 41, 159–166. [Google Scholar] [CrossRef]
- Brode, C.S.; Mitchell, J.E. Problematic Eating Behaviors and Eating Disorders Associated with Bariatric Surgery. Psychiatr. Clin. N. Am. 2019, 42, 287–297. [Google Scholar] [CrossRef]
- Tsouristakis, A.I.; Febres, G.; McMahon, D.J.; Tchang, B.; Conwell, I.M.; Tsang, A.J.; Ahmed, L.; Bessler, M.; Korner, J. Long-Term Modulation of Appetitive Hormones and Sweet Cravings After Adjustable Gastric Banding and Roux-en-Y Gastric Bypass. Obes. Surg. 2019, 29, 3698–3705. [Google Scholar] [CrossRef] [PubMed]
- Mack, I.; Ölschläger, S.; Sauer, H.; von Feilitzsch, M.; Weimer, K.; Junne, F.; Peeraully, R.; Enck, P.; Zipfel, S.; Teufel, M. Does Laparoscopic Sleeve Gastrectomy Improve Depression, Stress and Eating Behaviour? A 4-Year Follow-up Study. Obes. Surg. 2016, 26, 2967–2973. [Google Scholar] [CrossRef] [PubMed]
- Devlin, M.J.; King, W.C.; Kalarchian, M.A.; White, G.E.; Marcus, M.D.; Garcia, L.; Yanovski, S.Z.; Mitchell, J.E. Eating pathology and experience and weight loss in a prospective study of bariatric surgery patients: 3-year follow-up. Int. J. Eat. Disord. 2016, 49, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; Ivezaj, V.; Duffy, A.J.; Gueorguieva, R. 24-Month follow-up of randomized controlled trial of guided-self-help for loss-of-control eating after bariatric surgery. Int. J. Eat. Disord. 2022, 55, 1521–1531. [Google Scholar] [CrossRef] [PubMed]
- Devlin, M.J.; King, W.C.; Kalarchian, M.A.; Hinerman, A.; Marcus, M.D.; Yanovski, S.Z.; Mitchell, J.E. Eating pathology and associations with long-term changes in weight and quality of life in the longitudinal assessment of bariatric surgery study. Int. J. Eat. Disord. 2018, 51, 1322–1330. [Google Scholar] [CrossRef]
- Kofman, M.D.; Lent, M.R.; Swencionis, C. Maladaptive eating patterns, quality of life, and weight outcomes following gastric bypass: Results of an Internet survey. Obesity 2010, 18, 1938–1943. [Google Scholar] [CrossRef] [PubMed]
- Gero, D.; Tzafos, S.; Milos, G.; Gerber, P.A.; Vetter, D.; Bueter, M. Predictors of a Healthy Eating Disorder Examination-Questionnaire (EDE-Q) Score 1 Year After Bariatric Surgery. Obes. Surg. 2019, 29, 928–934. [Google Scholar] [CrossRef]
- Wong, E.; Fleishman, A.; Brem, A.; Jones, D.B.; Wee, C.C. High-Risk Alcohol Use and Disordered Eating Behavior Before and 1 Year After Sleeve Gastrectomy. Obes. Surg. 2022, 32, 593–598. [Google Scholar] [CrossRef]
- King, W.C.; Chen, J.Y.; Courcoulas, A.P.; Dakin, G.F.; Engel, S.G.; Flum, D.R.; Hinojosa, M.W.; Kalarchian, M.A.; Mattar, S.G.; Mitchell, J.E.; et al. Alcohol and other substance use after bariatric surgery: Prospective evidence from a U.S. multicenter cohort study. Surg. Obes. Relat. Dis. 2017, 13, 1392–1402. [Google Scholar] [CrossRef]
- Bantounou, M.A. A narrative review of the use of alcohol during the Covid-19 pandemic; effects and implications. J. Addict. Dis. 2023, 41, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Burnatowska, E.; Surma, S.; Olszanecka-Glinianowicz, M. Relationship between Mental Health and Emotional Eating during the COVID-19 Pandemic: A Systematic Review. Nutrients 2022, 14, 3989. [Google Scholar] [CrossRef] [PubMed]
- Zeigler, Z. COVID-19 Self-quarantine and Weight Gain Risk Factors in Adults. Curr. Obes. Rep. 2021, 10, 423–433. [Google Scholar] [CrossRef]
- Christian, N.J.; King, W.C.; Yanovski, S.Z.; Courcoulas, A.P.; Belle, S.H. Validity of Self-reported Weights Following Bariatric Surgery. JAMA 2013, 310, 2454–2456. [Google Scholar] [CrossRef] [PubMed]
- Faria, S.L.; Santos, A.; Magro, D.O.; Cazzo, E.; Assalin, H.B.; Guadagnini, D.; Vieira, F.T.; Dutra, E.S.; Saad, M.J.A.; Ito, M.K. Gut Microbiota Modifications and Weight Regain in Morbidly Obese Women After Roux-en-Y Gastric Bypass. Obes. Surg. 2020, 30, 4958–4966. [Google Scholar] [CrossRef] [PubMed]
- Boswell, R.G.; Sun, W.; Suzuki, S.; Kober, H. Training in cognitive strategies reduces eating and improves food choice. Proc. Natl. Acad. Sci. USA 2018, 115, E11238–E11247. [Google Scholar] [CrossRef] [PubMed]
- Myers, C.A.; Martin, C.K.; Apolzan, J.W. Food cravings and body weight: A conditioning response. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 298–302. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Participants’ Characteristics | All, N = 36 |
|---|---|
| Type of surgery (n (%)) | SG: 30 (83%) |
| RYGB: 6 (17%) | |
| Age (years) | 42.9 ± 9.5 |
| Race (n (%)) | White/Caucasian: 30 (83%) |
| Black/African American: 5 (14%) | |
| Other: 1 (3%) | |
| Ethnicity (n (%)) | Non-Hispanic: 33 (92%) |
| Hispanic: 1 (3%) | |
| Other: 2 (5%) | |
| Time after surgery (years) a | 3.3 ± 1.1 |
| Pre-surgery Body Mass Index (BMI) (kg/m2) a | 47.3 ± 3.5 |
| Current BMI (kg/m2) | 33.6 ± 7.4 |
| % Excess Weight Loss (EWL) | 66.6 ± 25.4 |
| Weight regain: % Maximum Weight Lost (MWL) a | 18.2 ± 13.6 |
| Time after surgery to reach nadir weight (years/n = 35) a | 1.2 ± 0.6 |
| Ingestive behavior-related outcomes | |
| Food-Craving Inventory | |
| High Fat | 1.9 ± 0.5 |
| Carbohydrates a | 1.7 ± 0.5 |
| Sweets a | 2.3 ± 0.5 |
| Fast Food | 2.4 ± 0.7 |
| Total Cravings | 2.1 ± 0.4 |
| Dutch Eating Behavior Questionnaire | |
| Restrained eating | 3.1 ± 0.6 |
| Emotional eating | 2.6 ± 0.9 |
| External eating | 2.8 ± 0.6 |
| Eating Disorder Examination Questionnaire | |
| Restraint | 2.2 ± 1.3 |
| Eating concern a | 0.9 ± 0.8 |
| Shape concern | 3.3 ± 1.5 |
| Weight concern | 2.7 ± 1.5 |
| Global score | 2.3 ± 1.1 |
| Yale Food Addiction Scale (n (%)) | |
| No food addiction | 27 (75%) |
| Food addiction | 9 (25%) |
| Mild | 1 (11%) |
| Moderate | 2 (22%) |
| Severe | 6 (67%) |
| Loss of control when eating (n (%)) | |
| No | 20 (56%) |
| Yes | 16 (44%) |
| At least 1/28 days (monthly) | 5 (31%) |
| At least 4/28 days (weekly) | 11 (69%) |
| Grazing (n (%)) | |
| No | 4 (11%) |
| Yes | 32 (89%) |
| At least 1/28 days (monthly) | 11 (34%) |
| At least 4/28 days (weekly) | 21 (66%) |
| Loss of control when grazing (n (%)) | |
| No | 19 (53%) |
| Yes | 17 (47%) |
| Alcohol use (n (%)) | |
| No | 5 (14%) |
| Yes | 31 (86%) |
| Non-hazardous drinking | 14 (45%) |
| Hazardous drinking | 17 (55%) |
| n | Adj. R2 | Predictor | B Coefficient | Standard Error | T | p Value | VIF |
|---|---|---|---|---|---|---|---|
| 36 | 0.31 | Frequency of cravings for sweets | 5.20 | 3.28 | 1.59 | 0.12 | 1.66 |
| EDE-Q global score | 0.13 | 0.38 | 0.35 | 0.73 | 1.76 | ||
| Time after surgery | 4.93 | 2.13 | 2.31 | 0.03 | 1.17 | ||
| Frequency of cravings for sweets × time after surgery | −44.74 | 21.15 | −2.12 | 0.04 | 2.09 | ||
| EDE-Q global score × time after surgery | 1.61 | 2.47 | 0.65 | 0.52 | 1.99 |
| Participants’ Characteristics | <20 % MWL (n = 20) | ≥20 % MWL (n = 16) | p Value |
|---|---|---|---|
| Type of surgery (n(%)) | SG: 16 (80%) | SG: 14 (88%) | 0.45 |
| RYGB: 4 (20%) | RYGB: 2 (12%) | ||
| Age (years) | 40.8 ± 8.3 | 45.6 ± 10.5 | 0.13 |
| Race (n(%)) | White/Caucasian: 18 (90%) | White/Caucasian: 12 (75%) | 0.47 |
| Black/African American: 2 (10%) | Black/African American: 3 (19%) | ||
| Other: 0 (0%) | Other: 1 (6%) | ||
| Ethnicity (n(%)) | Non-Hispanic: 18 (90%) | Non-Hispanic: 15 (94%) | 1 |
| Hispanic: 1 (5%) | Hispanic: 0 (0%) | ||
| Other: 1 (5%) | Other: 1 (6%) | ||
| Time after surgery (years) a | 3.0 ± 0.9 | 4.3 ± 1.2 | 0.09 |
| Pre-surgery Body Mass Index (BMI) (kg/m2) a | 47.8 ± 5.2 | 47.3 ± 2.5 | 0.73 |
| Current BMI (kg/m2) | 30.6 ± 5.8 | 37.5 ± 7.6 | <0.01 |
| % Excess Weight Loss (EWL) | 80.4 ± 18.5 | 49.4 ± 22.6 | <0.0001 |
| Weight regain: % Maximum Weight Lost (MWL) a | 7.3 ± 6.4 | 37.4 ± 11.9 | <0.0001 |
| Time after surgery to reach nadir weight (years/n = 35) a | 1.4 ± 0.7 | 1.2 ± 0.2 | 0.37 |
| Ingestive behavior-related outcomes | |||
| Food-Craving Inventory | |||
| High Fat | 1.8 ± 0.5 | 1.9 ± 0.4 | 0.55 |
| Carbohydrates a | 1.7 ± 0.4 | 1.9 ± 0.6 | 0.99 |
| Sweets a | 2.0 ± 0.3 | 2.8 ± 0.6 | 0.09 |
| Fast Food | 2.4 ± 0.9 | 2.5 ± 0.6 | 0.71 |
| Total Cravings | 2.1 ± 0.5 | 2.2 ± 0.4 | 0.28 |
| Dutch Eating Behavior Questionnaire | |||
| Restrained eating | 3.1 ± 0.7 | 3.2 ± 0.6 | 0.74 |
| Emotional eating | 2.4 ± 0.8 | 2.7 ± 1.1 | 0.31 |
| External eating | 2.7 ± 0.6 | 3.0 ± 0.6 | 0.09 |
| Eating Disorder Examination Questionnaire | |||
| Restraint | 2.1 ± 1.3 | 2.4 ± 1.3 | 0.58 |
| Eating concern a | 0.4 ± 0.6 | 1.6 ± 0.8 | 0.09 |
| Shape concern | 2.8 ± 1.6 | 3.8 ± 1.2 | 0.05 |
| Weight concern | 2.1 ± 1.4 | 3.4 ± 1.4 | 0.01 |
| Global score | 2.0 ± 1.1 | 2.8 ± 1.0 | 0.04 |
| Yale Food Addiction Scale (n (%)) | |||
| No food addiction | 18 (90%) | 9 (56%) | 0.03 |
| Food addiction | 2 (10%) | 7 (44%) | |
| Mild | 0 (0%) | 1 (14%) | 1 |
| Moderate | 0 (0%) | 2 (29%) | |
| Severe | 2 (100%) | 4 (57%) | |
| Loss of control when eating (n (%)) | |||
| No | 14 (70%) | 6 (38%) | 0.05 |
| Yes | 6 (30%) | 10 (63%) | |
| At least 1/28 days (monthly) | 2 (33%) | 3 (30%) | 0.65 |
| At least 4/28 days (weekly) | 4 (67%) | 7 (70%) | |
| Grazing (n (%)) | |||
| No | 4 (20%) | 0 (0%) | 0.08 |
| Yes | 16 (80%) | 16 (100%) | |
| At least 1/28 days (monthly) | 7 (44%) | 4 (25%) | 0.23 |
| At least 4/28 days (weekly) | 9 (56%) | 12 (75%) | |
| Loss of control when grazing (n (%)) | |||
| No | 12 (60%) | 7 (44%) | 0.26 |
| Yes | 8 (40%) | 9 (56%) | |
| Alcohol use (n (%)) | |||
| No | 1 (5%) | 4 (25%) | 0.11 |
| Yes | 19 (95%) | 12 (75%) | |
| Non-hazardous drinking | 6 (32%) | 8 (67%) | 0.06 |
| Hazardous drinking | 13 (68%) | 4 (33%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicanor-Carreón, J.G.; Seyedsadjadi, N.; Rowitz, B.; Pepino, M.Y. Weight Regain and Ingestive Behavior in Women after Metabolic Surgery. Nutrients 2023, 15, 3670. https://doi.org/10.3390/nu15173670
Nicanor-Carreón JG, Seyedsadjadi N, Rowitz B, Pepino MY. Weight Regain and Ingestive Behavior in Women after Metabolic Surgery. Nutrients. 2023; 15(17):3670. https://doi.org/10.3390/nu15173670
Chicago/Turabian StyleNicanor-Carreón, Jessica G., Neda Seyedsadjadi, Blair Rowitz, and Marta Yanina Pepino. 2023. "Weight Regain and Ingestive Behavior in Women after Metabolic Surgery" Nutrients 15, no. 17: 3670. https://doi.org/10.3390/nu15173670
APA StyleNicanor-Carreón, J. G., Seyedsadjadi, N., Rowitz, B., & Pepino, M. Y. (2023). Weight Regain and Ingestive Behavior in Women after Metabolic Surgery. Nutrients, 15(17), 3670. https://doi.org/10.3390/nu15173670