
Chinese Dietary Indices and Glioma: New Insights of a Case–Control Study in the Chinese Population

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Evaluation of Dietary Indices
2.4. Other Variables
2.5. Statistical Analysis
3. Results
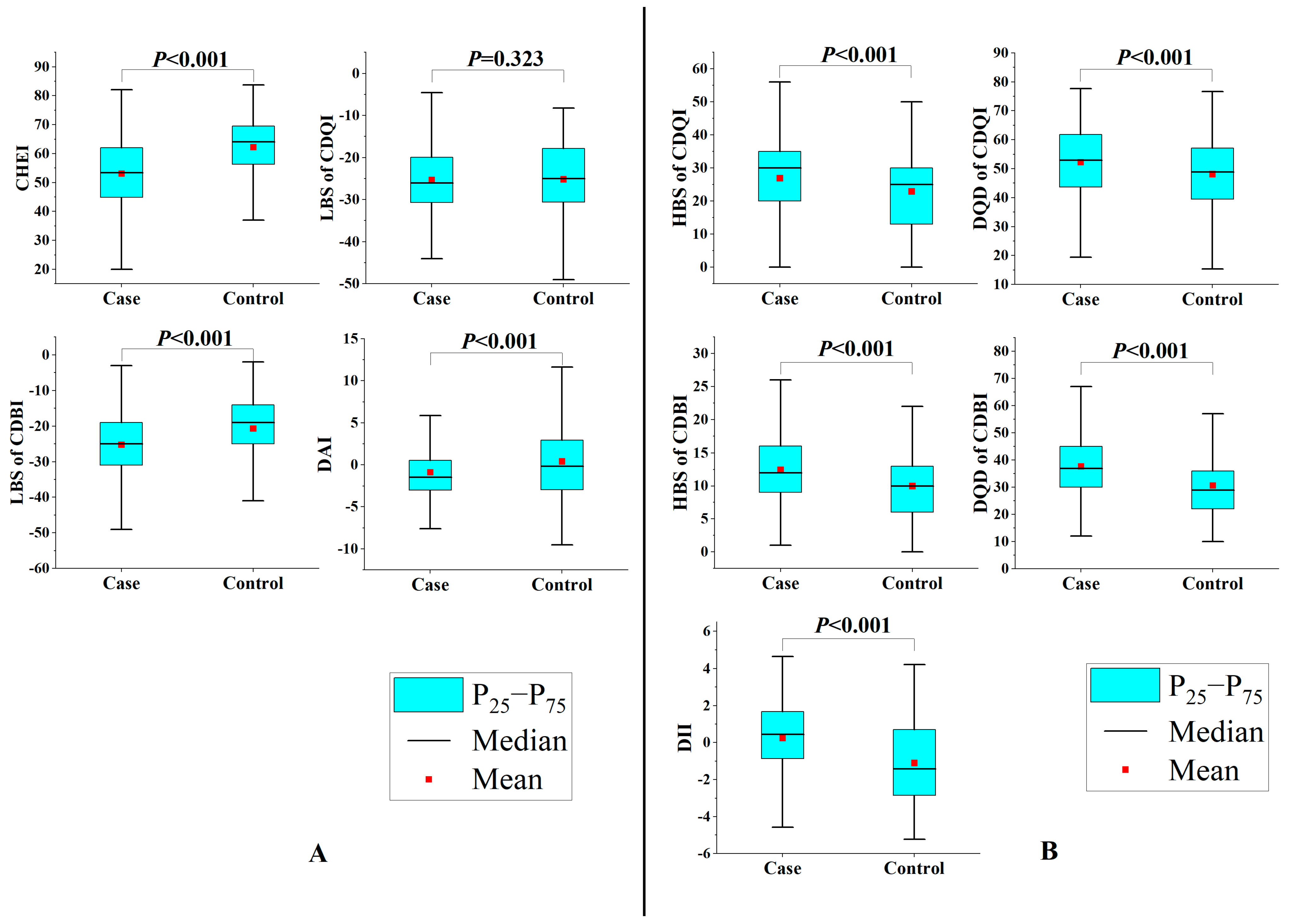
3.1. Characteristics of the Study Population and Dietary Indices
3.2. Chinese Dietary Indices and Glioma
3.3. Chinese Dietary Indices and Gliomas of Different Pathological Classifications
3.4. Chinese Dietary Indices and Glioma of Different Pathological Grades
3.5. Sensitivity Analysis
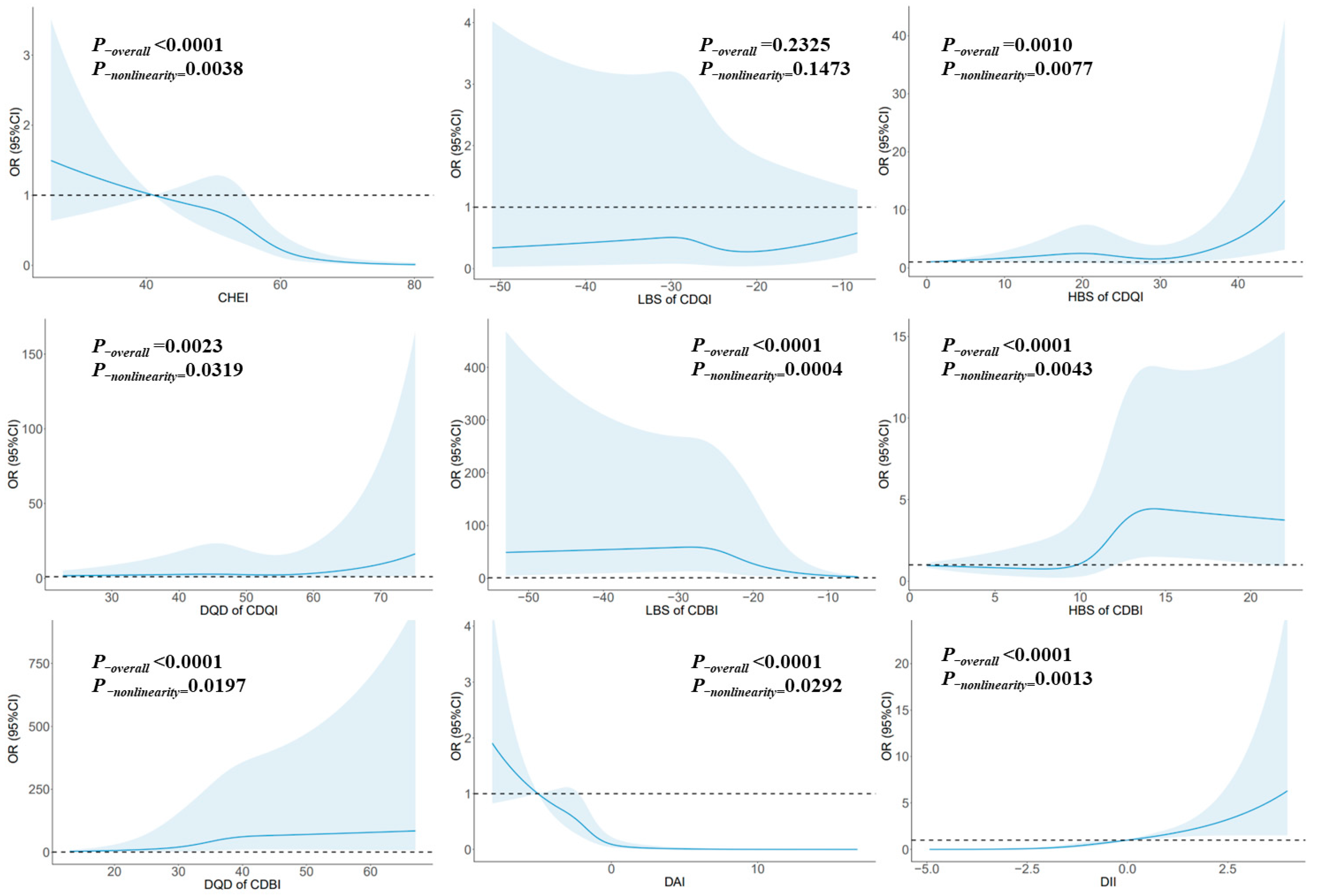
3.6. Dose–Response Relationship
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncology 2021, 23, i1–i105. [Google Scholar] [CrossRef]
- Walsh, K.M.; Claus, E.B. Diet and risk of glioma: Targets for prevention remain elusive. Neuro-Oncology 2019, 21, 832–833. [Google Scholar] [CrossRef]
- Ruder, A.M.; Carreon, T.; Butler, M.A.; Calvert, G.M.; Davis-King, K.E.; Waters, M.A.; Schulte, P.A.; Mandel, J.S.; Morton, R.F.; Reding, D.J.; et al. Exposure to farm crops, livestock, and farm tasks and risk of glioma: The Upper Midwest Health Study. Am. J. Epidemiol. 2009, 169, 1479–1491. [Google Scholar] [CrossRef]
- Turner, M.C.; Krewski, D.; Armstrong, B.K.; Chetrit, A.; Giles, G.G.; Hours, M.; McBride, M.L.; Parent, M.E.; Sadetzki, S.; Siemiatycki, J.; et al. Allergy and brain tumors in the INTERPHONE study: Pooled results from Australia, Canada, France, Israel, and New Zealand. Cancer Cause Control 2013, 24, 949–960. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Francis, S.S.; Barnholtz-Sloan, J.S. Epidemiology of Brain and Other CNS Tumors. Curr. Neurol. Neurosci. 2021, 21, 68. [Google Scholar] [CrossRef]
- Mathews, J.D.; Forsythe, A.V.; Brady, Z.; Butler, M.W.; Goergen, S.K.; Byrnes, G.B.; Giles, G.G.; Wallace, A.B.; Anderson, P.R.; Guiver, T.A.; et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: Data linkage study of 11 million Australians. Bmj-Brit. Med. J. 2013, 346, f2360. [Google Scholar] [CrossRef]
- Matsushita, M.; Fujita, K.; Nonomura, N. Influence of Diet and Nutrition on Prostate Cancer. Int. J. Mol. Sci. 2020, 21, 1447. [Google Scholar] [CrossRef] [PubMed]
- Dunneram, Y.; Greenwood, D.C.; Cade, J.E. Diet, menopause and the risk of ovarian, endometrial and breast cancer. Proc. Nutr. Soc. 2019, 78, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.W.; Li, J.W.; Fock, K.M. Diet and cancer of the esophagus and stomach. Curr. Opin. Gastroen. 2021, 37, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Terry, M.B.; Howe, G.; Pogoda, J.M.; Zhang, F.F.; Ahlbom, A.; Choi, W.; Giles, G.G.; Little, J.; Lubin, F.; Menegoz, F.; et al. An international case-control study of adult diet and brain tumor risk: A histology-specific analysis by food group. Ann. Epidemiol. 2009, 19, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Burch, J.D.; Craib, K.J.; Choi, B.C.; Miller, A.B.; Risch, H.A.; Howe, G.R. An exploratory case-control study of brain tumors in adults. JNCI-J. Natl. Cancer I 1987, 78, 601–609. [Google Scholar]
- Malmir, H.; Shayanfar, M.; Mohammad-Shirazi, M.; Sharifi, G.; Esmaillzadeh, A. Legume and Nuts Consumption in Relation to Glioma: A Case- Control Study. Nutr. Cancer 2021, 73, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Creed, J.H.; Smith-Warner, S.A.; Gerke, T.A.; Egan, K.M. A prospective study of coffee and tea consumption and the risk of glioma in the UK Biobank. Eur. J. Cancer 2020, 129, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Malmir, H.; Shayanfar, M.; Mohammad-Shirazi, M.; Tabibi, H.; Sharifi, G.; Esmaillzadeh, A. Tea and coffee consumption in relation to glioma: A case-control study. Eur. J. Nutr. 2019, 58, 103–111. [Google Scholar] [CrossRef]
- Lee, M.; Wrensch, M.; Miike, R. Dietary and tobacco risk factors for adult onset glioma in the San Francisco Bay Area (California, USA). Cancer Cause Control 1997, 8, 13–24. [Google Scholar] [CrossRef]
- Shahrestani, M.A.; Saneei, P.; Shayanfar, M.; Mohammad-Shirazi, M.; Sharifi, G.; Sadeghi, O.; Esmaillzadeh, A. The relationship between rice consumption and glioma: A case-control study in adults. Sci. Rep. 2021, 11, 6073. [Google Scholar] [CrossRef]
- Zhang, W.; Jiang, J.; Li, X.; He, Y.; Chen, F.; Li, W. Dietary Factors and Risk of Glioma in Adults: A Systematic Review and Dose-Response Meta-Analysis of Observational Studies. Front. Nutr. 2022, 9, 834258. [Google Scholar] [CrossRef]
- Dubrow, R.; Darefsky, A.S.; Park, Y.; Mayne, S.T.; Moore, S.C.; Kilfoy, B.; Cross, A.J.; Sinha, R.; Hollenbeck, A.R.; Schatzkin, A.; et al. Dietary components related to N-nitroso compound formation: A prospective study of adult glioma. Cancer Epidem. Biomar. 2010, 19, 1709–1722. [Google Scholar] [CrossRef]
- Holick, C.N.; Giovannucci, E.L.; Rosner, B.; Stampfer, M.J.; Michaud, D.S. Prospective study of intake of fruit, vegetables, and carotenoids and the risk of adult glioma. Am. J. Clin. Nutr. 2007, 85, 877–886. [Google Scholar] [CrossRef]
- Ward, H.A.; Gayle, A.; Jakszyn, P.; Merritt, M.; Melin, B.; Freisling, H.; Weiderpass, E.; Tjonneland, A.; Olsen, A.; Dahm, C.C.; et al. Meat and haem iron intake in relation to glioma in the European Prospective Investigation into Cancer and Nutrition study. Eur. J. Cancer Prev. 2018, 27, 379–383. [Google Scholar] [CrossRef]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef]
- Solans, M.; Coenders, G.; Marcos-Gragera, R.; Castello, A.; Gracia-Lavedan, E.; Benavente, Y.; Moreno, V.; Perez-Gomez, B.; Amiano, P.; Fernandez-Villa, T.; et al. Compositional analysis of dietary patterns. Stat. Methods Med. Res. 2019, 28, 2834–2847. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, Z.; Gao, Q.; Zhao, H.; Chen, S.; Huang, L.; Wang, W.; Wang, T. A review of statistical methods for dietary pattern analysis. Nutr. J. 2021, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Shayanfar, M.; Rigi, S.; Mohammad-Shirazi, M.; Sharifi, G.; Esmaillzadeh, A. Adherence to the Mediterranean dietary pattern in relation to glioma: A case-control study. Clin. Nutr. 2021, 40, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Kuan, A.S.; Green, J.; Kitahara, C.M.; Berrington, D.G.A.; Key, T.; Reeves, G.K.; Floud, S.; Balkwill, A.; Bradbury, K.; Liao, L.M.; et al. Diet and risk of glioma: Combined analysis of 3 large prospective studies in the UK and USA. Neuro-Oncology 2019, 21, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Wang, Y.; Ge, K.; Lin, H.; Popkin, B.M. Measuring diet quality in China: The INFH-UNC-CH diet quality index. Eur. J. Clin. Nutr. 2000, 54, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Zou, Z.; Li, Q.; Huang, H.; Liu, D.; Tan, R.; Xu, S. Unfavorable dietary quality and overweight or obesity in kidney transplant recipients as judged by the Chinese diet balance index 2016 (DBI-16). Asia Pac. J. Clin. Nutr. 2022, 31, 551–560. [Google Scholar] [CrossRef]
- Yuan, Y.Q.; Li, F.; Dong, R.H.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. The Development of a Chinese Healthy Eating Index and Its Application in the General Population. Nutrients 2017, 9, 977. [Google Scholar] [CrossRef]
- Vahid, F.; Rahmani, D.; Davoodi, S.H. Validation of Dietary Antioxidant Index (DAI) and investigating the relationship between DAI and the odds of gastric cancer. Nutr. Metab. 2020, 17, 102. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, O.; Shayanfar, M.; Mohammad-Shirazi, M.; Sharifi, G.; Esmaillzadeh, A. A case-control study on dietary quality indices and glioma. Brit. J. Nutr. 2019, 122, 103–110. [Google Scholar] [CrossRef]
- Zhao, W.H.; Huang, Z.P.; Zhang, X.; He, L.; Willett, W.; Wang, J.L.; Hasegawa, K.; Chen, J.S. Reproducibility and Validity of a Chinese Food Frequency Questionnaire. Biomed. Environ. Sci. 2010, 23, 1–38. [Google Scholar] [CrossRef]
- Zhang, W.; He, Y.; Kang, X.; Wang, C.; Chen, F.; Kang, Z.; Yang, S.; Zhang, R.; Peng, Y.; Li, W. Association between dietary minerals and glioma: A case-control study based on Chinese population. Front. Nutr. 2023, 10, 1118997. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.X. China Food Composition Tables; Standard Edition; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Morgan, L.L.; Miller, A.B.; Sasco, A.; Davis, D.L. Mobile phone radiation causes brain tumors and should be classified as a probable human carcinogen (2A) (review). Int. J. Oncol. 2015, 46, 1865–1871. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport Exer. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Imai, K.; Keele, L.; Tingley, D. A general approach to causal mediation analysis. Psychol. Methods 2010, 15, 309–334. [Google Scholar] [CrossRef]
- Valente, M.J.; Rijnhart, J.; Smyth, H.L.; Muniz, F.B.; MacKinnon, D.P. Causal Mediation Programs in R, Mplus, SAS, SPSS, and Stata. Struct. Equ. Model. 2020, 27, 975–984. [Google Scholar] [CrossRef]
- Zhang, W.; Du, J.; Li, H.; Yang, Y.; Cai, C.; Gao, Q.; Xing, Y.; Shao, B.; Li, G. Multiple-element exposure and metabolic syndrome in Chinese adults: A case-control study based on the Beijing population health cohort. Environ. Int. 2020, 143, 105959. [Google Scholar] [CrossRef]
- Chen, P.Y.; Fang, A.P.; Wang, X.Y.; Lan, Q.Y.; Liao, G.C.; Liu, Z.Y.; Zhang, D.M.; Zhang, Y.Y.; Chen, Y.M.; Zhu, H.L. Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study. Nutrients 2018, 10, 1113. [Google Scholar] [CrossRef]
- Luo, Y.; Zhang, Y.J.; Zhang, D.M.; Yishake, D.; Liu, Z.Y.; Chen, M.S.; Wang, F.; Zhou, Z.G.; Long, J.A.; Zhong, R.H.; et al. Association between dietary patterns and prognosis of hepatocellular carcinoma in the Guangdong liver cancer cohort study. Hepatol. Res. 2020, 50, 1164–1175. [Google Scholar] [CrossRef] [PubMed]
- Maitiniyazi, G.; Cao, X.; Chen, Y.; Zhang, R.; Liu, Y.; Li, Z.; Gu, D.; Li, T.; Xia, S. Impact of Gut Microbiota on the Association between Diet and Depressive Symptoms in Breast Cancer. Nutrients 2022, 14, 1186. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Benisi-Kohansal, S.; Shayanfar, M.; Mohammad-Shirazi, M.; Tabibi, H.; Sharifi, G.; Saneei, P.; Esmaillzadeh, A. Adherence to the Dietary Approaches to Stop Hypertension-style diet in relation to glioma: A case-control study. Br. J. Nutr. 2016, 115, 1108–1116. [Google Scholar] [CrossRef]
- Kim, S.; Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The Diet Quality Index-International (DQI-I) provides an effective tool for cross-national comparison of diet quality as illustrated by China and the United States. J. Nutr. 2003, 133, 3476–3484. [Google Scholar] [CrossRef]
- Milajerdi, A.; Namazi, N.; Larijani, B.; Azadbakht, L. The Association of Dietary Quality Indices and Cancer Mortality: A Systematic Review and Meta-analysis of Cohort Studies. Nutr. Cancer 2018, 70, 1091–1105. [Google Scholar] [CrossRef]
- Nkondjock, A.; Ghadirian, P. Diet quality and BRCA-associated breast cancer risk. Breast Cancer Res. Treat. 2007, 103, 361–369. [Google Scholar] [CrossRef]
- Shayanfar, M.; Vahid, F.; Faghfoori, Z.; Davoodi, S.H.; Goodarzi, R. The Association Between Index of Nutritional Quality (INQ) and Glioma and Evaluation of Nutrient Intakes of These Patients: A Case-Control Study. Nutr. Cancer 2018, 70, 213–220. [Google Scholar] [CrossRef]
- Saha, S.K.; Lee, S.B.; Won, J.; Choi, H.Y.; Kim, K.; Yang, G.M.; Dayem, A.A.; Cho, S.G. Correlation between Oxidative Stress, Nutrition, and Cancer Initiation. Int. J. Mol. Sci. 2017, 18, 1544. [Google Scholar] [CrossRef]
- Lutz, W.K.; Schlatter, J. Chemical carcinogens and overnutrition in diet-related cancer. Carcinogenesis 1992, 13, 2211–2216. [Google Scholar] [CrossRef]
- Key, T.J.; Spencer, E.A.; Reeves, G.K. Symposium 1: Overnutrition: Consequences and solutions. Obesity and cancer risk. Proc. Nutr. Soc. 2010, 69, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Lutz, W.K. Carcinogens in the diet vs. overnutrition. Individual dietary habits, malnutrition, and genetic susceptibility modify carcinogenic potency and cancer risk. Mutat. Res.-Fund. Mol. M 1999, 443, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Dadgostar, E.; Fallah, M.; Izadfar, F.; Heidari-Soureshjani, R.; Aschner, M.; Tamtaji, O.R.; Mirzaei, H. Therapeutic Potential of Resveratrol in the Treatment of Glioma: Insights into its Regulatory Mechanisms. Mini-Rev. Med. Chem. 2021, 21, 2835–2847. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Jiang, J.; He, Y.; Li, X.; Yin, S.; Chen, F.; Li, W. Association between vitamins and risk of brain tumors: A systematic review and dose-response meta-analysis of observational studies. Front. Nutr. 2022, 9, 935706. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovas. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Bertoia, M.L.; Triche, E.W.; Michaud, D.S.; Baylin, A.; Hogan, J.W.; Neuhouser, M.L.; Tinker, L.F.; Van Horn, L.; Waring, M.E.; Li, W.; et al. Mediterranean and Dietary Approaches to Stop Hypertension dietary patterns and risk of sudden cardiac death in postmenopausal women. Am. J. Clin. Nutr. 2014, 99, 344–351. [Google Scholar] [CrossRef]
- Tayyem, R.F.; Shehadeh, I.N.; Abumweis, S.S.; Bawadi, H.A.; Hammad, S.S.; Bani-Hani, K.E.; Al-Jaberi, T.M.; Alnusair, M.M. Physical inactivity, water intake and constipation as risk factors for colorectal cancer among adults in Jordan. Asian Pac. J. Cancer Prev. 2013, 14, 5207–5212. [Google Scholar] [CrossRef]
- Keren, Y.; Magnezi, R.; Carmon, M.; Amitai, Y. Investigation of the Association between Drinking Water Habits and the Occurrence of Women Breast Cancer. Int. J. EnvirOn. Res. Public Health 2020, 17, 7692. [Google Scholar] [CrossRef]
- Wright, M.E.; Mayne, S.T.; Stolzenberg-Solomon, R.Z.; Li, Z.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am. J. Epidemiol. 2004, 160, 68–76. [Google Scholar] [CrossRef]
- Vahid, F.; Rahmani, W.; Davoodi, S.H. The association between dietary total antioxidant capacity and quality of nutrients with odds of colorectal cancer: A hospital-based case-control study. Clin. Nutr. ESPEN 2022, 52, 277–284. [Google Scholar] [CrossRef]
- Yu, Y.C.; Paragomi, P.; Wang, R.; Jin, A.; Schoen, R.E.; Sheng, L.T.; Pan, A.; Koh, W.P.; Yuan, J.M.; Luu, H.N. Composite dietary antioxidant index and the risk of colorectal cancer: Findings from the Singapore Chinese Health Study. Int. J. Cancer 2022, 150, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Vahid, F.; Rahmani, W.; Khodabakhshi, A.; Davoodi, S.H. Associated between Dietary Antioxidant Index (DAI) and Odds of Breast Cancer and Correlation between DAI with Pathobiological Markers: Hospital-Based Incidence Case-Control Study. J. Am. Nutr. Assoc. 2022, 42, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Magnano, S.L.R.; Scalisi, A.; Agodi, A. Antioxidant and inflammatory potential of diet among women at risk of cervical cancer: Findings from a cross-sectional study in Italy. Public Health Nutr. 2022, 25, 1577–1585. [Google Scholar] [CrossRef]
- Heydari, M.; Shayanfar, M.; Sharifi, G.; Saneei, P.; Sadeghi, O.; Esmaillzadeh, A. The Association between Dietary Total Antioxidant Capacity and Glioma in Adults. Nutr. Cancer 2021, 73, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Il’Yasova, D.; Marcello, J.E.; McCoy, L.; Rice, T.; Wrensch, M. Total dietary antioxidant index and survival in patients with glioblastoma multiforme. Cancer Cause Control 2009, 20, 1255–1260. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Klaunig, J.E. Oxidative Stress and Cancer. Curr. Pharm. Design 2018, 24, 4771–4778. [Google Scholar] [CrossRef] [PubMed]
- Jelic, M.D.; Mandic, A.D.; Maricic, S.M.; Srdjenovic, B.U. Oxidative stress and its role in cancer. J. Cancer Res. Ther. 2021, 17, 22–28. [Google Scholar] [CrossRef]
- Avila-Escalante, M.L.; Coop-Gamas, F.; Cervantes-Rodriguez, M.; Mendez-Iturbide, D.; Aranda-Gonzalez, I.I. The effect of diet on oxidative stress and metabolic diseases-Clinically controlled trials. J. Food Biochem. 2020, 44, e13191. [Google Scholar] [CrossRef]
- Mirvish, S.S. Effects of vitamins C and E on N-nitroso compound formation, carcinogenesis, and cancer. Cancer-Am. Cancer Soc. 1986, 58, 1842–1850. [Google Scholar] [CrossRef]
- Dionigi, L.; Ragonese, F.; Monarca, L.; Covino, S.; de Luca, A.; Iannitti, R.G.; Bastioli, F.; Moulas, A.N.; Allegretti, M.; Fioretti, B. Focus on the Use of Resveratrol as an Adjuvant in Glioblastoma Therapy. Curr. Pharm. Des. 2020, 26, 2102–2108. [Google Scholar] [CrossRef]
- Zeng, S.; Zhao, X.; Xu, L.S.; Yang, D.; Chen, L.; Xu, M.H. Apoptosis induction effect of Apocynum venetum polyphenol on human U87 glioma cells via NF-kappaB pathway. Future Oncol. 2019, 15, 3723–3738. [Google Scholar] [CrossRef]
- Carecho, R.; Carregosa, D.; Ratilal, B.O.; Figueira, I.; Avila-Galvez, M.A.; Dos, S.C.; Loncarevic-Vasiljkovic, N. Dietary (Poly)phenols in Traumatic Brain Injury. Int. J. Mol. Sci. 2023, 24, 8908. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, Z.; Xu, Y.M.; Wu, Y.; Yu, K.K.; Zhang, C.; Ji, Y.H.; Ding, G.; Chen, F.X. Epigallocatechin-3-gallate induces apoptosis, inhibits proliferation and decreases invasion of glioma cell. Neurosci. Bull. 2014, 30, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, C.; Chen, F.; He, Y.; Yin, S.; Peng, Y.; Li, W. Phytochemicals and Glioma: Results from Dietary Mixed Exposure. Brain Sci. 2023, 13, 902. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Scott, E.; Kholghi, A.; Andreadi, C.; Rufini, A.; Karmokar, A.; Britton, R.G.; Horner-Glister, E.; Greaves, P.; Jawad, D.; et al. Cancer chemoprevention: Evidence of a nonlinear dose response for the protective effects of resveratrol in humans and mice. Sci. Transl. Med. 2015, 7, 298ra117. [Google Scholar] [CrossRef] [PubMed]
- Sasanfar, B.; Toorang, F.; Mozafari, N.M.; Salehi-Abargouei, A.; Zendehdel, K. Dietary Inflammatory Index and Breast Cancer: Report from a Large-Scale Case-Control Study. Nutr. Cancer 2022, 74, 1692–1700. [Google Scholar] [CrossRef]
- Lozano-Lorca, M.; Salcedo-Bellido, I.; Olmedo-Requena, R.; Castano-Vinyals, G.; Amiano, P.; Shivappa, N.; Hebert, J.R.; Perez-Gomez, B.; Gracia-Lavedan, E.; Gomez-Acebo, I.; et al. Dietary inflammatory index and prostate cancer risk: MCC-Spain study. Prostate Cancer Prostatic Dis. 2022, 25, 568–575. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hebert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Colorectal Cancer Risk-A Meta-Analysis. Nutrients 2017, 9, 1043. [Google Scholar] [CrossRef]
- Aminianfar, A.; Vahid, F.; Shayanfar, M.; Davoodi, S.H.; Mohammad-Shirazi, M.; Shivappa, N.; Sharifi, G.; Hebert, J.R.; Surkan, P.J.; Faghfoori, Z.; et al. The association between the dietary inflammatory index and glioma: A case-control study. Clin. Nutr. 2020, 39, 433–439. [Google Scholar] [CrossRef]
- Keibel, A.; Singh, V.; Sharma, M.C. Inflammation, microenvironment, and the immune system in cancer progression. Curr. Pharm. Des. 2009, 15, 1949–1955. [Google Scholar] [CrossRef]
- Sowers, J.L.; Johnson, K.M.; Conrad, C.; Patterson, J.T.; Sowers, L.C. The role of inflammation in brain cancer. Adv. Exp. Med. Biol. 2014, 816, 75–105. [Google Scholar] [CrossRef]
- Galvao, R.P.; Zong, H. Inflammation and Gliomagenesis: Bi-Directional Communication at Early and Late Stages of Tumor Progression. Curr. Pathobiol. Rep. 2013, 1, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Guli, C.; La Torre, D.; Tomasello, C.; Angileri, F.F.; Aguennouz, M. Role of inflammation and oxidative stress mediators in gliomas. Cancers 2010, 2, 693–712. [Google Scholar] [CrossRef] [PubMed]
- Scheurer, M.E.; El-Zein, R.; Thompson, P.A.; Aldape, K.D.; Levin, V.A.; Gilbert, M.R.; Weinberg, J.S.; Bondy, M.L. Long-term anti-inflammatory and antihistamine medication use and adult glioma risk. Cancer Epidem. Biomar. 2008, 17, 1277–1281. [Google Scholar] [CrossRef] [PubMed]
- He, Y.N.; Fang, Y.H.; Xia, J. Update of the Chinese diet balance index: DBI_16. Acta Nutr. Sin. 2018, 40, 526–530. [Google Scholar]
- Gu, J.F. Interpretation of the Report on Nutrition and Chronic Disease Status of Chinese Residents (2015). Acta Nutr. Sin. 2016, 38, 525–529. [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention. Available online: https://www.chinanutri.cn/sjnj/swsryssjg/zgjmswsrl/zgjmglswpjsrl/201512/t20151230_123992.html (accessed on 24 July 2023).



{kind=link}
{kind=link}
| Case (n = 506) | Control (n = 506) | p-Value a | |
|---|---|---|---|
| Age (years) | 42.62 ± 13.09 | 41.15 ± 12.85 | 0.072 |
| Sex, n (%) | 1.000 | ||
| Male | 284 (56.1) | 284 (56.1) | |
| Female | 222 (43.9) | 222 (43.9) | |
| BMI (kg/m2) | 24.03 ± 3.25 | 23.05 ± 3.27 | <0.001 |
| High-risk residential area, n (%) | 0.534 | ||
| Yes | 108 (21.3) | 100 (19.8) | |
| No | 398 (78.7) | 406 (80.2) | |
| Occupation, n (%) | 0.024 | ||
| Manual workers | 134 (26.5) | 103 (20.4) | |
| Mental workers | 265 (52.4) | 306 (60.5) | |
| Others | 107 (21.1) | 97 (19.1) | |
| Education level, n (%) | <0.001 | ||
| Primary school and below | 35 (6.9) | 13 (2.6) | |
| Middle school | 210 (41.5) | 127 (25.1) | |
| University and above | 261 (51.6) | 366 (72.3) | |
| Household income, n (%) | <0.001 | ||
| <3000 CNY/month | 49 (9.7) | 92 (18.2) | |
| 3000–10,000 CNY/month | 384 (75.9) | 249 (49.2) | |
| >10,000 CNY/month | 73 (14.4) | 165 (32.6) | |
| Smoking status, n (%) | 0.039 | ||
| Never smoked | 354 (70.0) | 381 (75.3) | |
| Former smoker | 65 (12.8) | 41 (8.1) | |
| Current smoker | 87 (17.2) | 84 (16.6) | |
| History of allergies, n (%) | <0.001 | ||
| Yes | 39 (7.7) | 74 (14.6) | |
| No | 467 (92.3) | 432 (85.4) | |
| History of head trauma, n (%) | 0.474 | ||
| Yes | 57 (11.3) | 50 (9.9) | |
| No | 449 (88.7) | 456 (90.1) | |
| Family history of cancer, n (%) | 0.001 | ||
| Yes | 152 (30.0) | 107 (21.1) | |
| No | 354 (70.0) | 399 (78.9) | |
| Physical activity, n (%) | <0.001 | ||
| Low | 69 (13.6) | 232 (45.8) | |
| Moderate | 209 (41.3) | 184 (36.4) | |
| High | 228 (45.1) | 90 (17.8) |
| Dietary Index | T1 | T2 | T3 | Continuous c |
|---|---|---|---|---|
| CHEI | <53.48 | 53.48–64.30 | >64.30 | |
| Case/Control | 254/84 | 160/177 | 92/245 | |
| Model 1 a | 1 | 0.30 (0.21–0.43) | 0.12 (0.08–0.18) | 0.93 (0.91–0.94) |
| Model 2 b | 1 | 0.31 (0.17–0.57) | 0.06 (0.03–0.13) | 0.90 (0.88–0.93) |
| DAI | <−2.43 | −2.43–0.60 | >0.60 | |
| Case/Control | 186/152 | 195/142 | 125/212 | |
| Model 1 a | 1 | 1.12 (0.81–1.55) | 0.50 (0.37–0.69) | 0.94 (0.91–0.97) |
| Model 2 b | 1 | 0.51 (0.27–0.97) | 0.08 (0.03–0.18) | 0.61 (0.54–0.70) |
| LBS of CDQI | <−22.08 | −22.08–−29.40 | >−29.40 | |
| Case/Control | 157/181 | 177/161 | 172/164 | |
| Model 1 a | 1 | 1.26 (0.94–1.70) | 1.21 (0.89–1.65) | 1.00 (0.99–1.02) |
| Model 2 b | 1 | 0.95 (0.53–1.68) | 1.46 (0.76–2.79) | 1.01 (0.98–1.05) |
| HBS of CDQI | <20 | 20–30 | >30 | |
| Case/Control | 156/227 | 144/157 | 206/122 | |
| Model 1 a | 1 | 1.35 (0.99–1.84) | 2.56 (1.86–3.52) | 1.03 (1.02–1.05) |
| Model 2 b | 1 | 0.86 (0.52–1.44) | 2.58 (1.52–4.40) | 1.03 (1.01–1.05) |
| DQD of CDQI | <44.71 | 44.71–56.76 | >56.76 | |
| Case/Control | 140/198 | 163/174 | 203/134 | |
| Model 1 a | 1 | 1.32 (0.97–1.79) | 2.10 (1.54–2.86) | 1.03 (1.02–1.04) |
| Model 2 b | 1 | 0.76 (0.46–1.27) | 1.93 (1.15–3.24) | 1.03 (1.01–1.05) |
| LBS of CDBI | <−18 | −18–−26 | >−26 | |
| Case/Control | 113/241 | 181/154 | 212/111 | |
| Model 1 a | 1 | 2.56 (1.83–3.59) | 3.97 (2.82–5.58) | 1.06 (1.04–1.07) |
| Model 2 b | 1 | 3.68 (2.12–6.36) | 5.75 (3.15–10.49) | 1.08 (1.06–1.12) |
| HBS of CDBI | <9 | 9–13 | >13 | |
| Case/Control | 135/243 | 158/155 | 213/108 | |
| Model 1 a | 1 | 1.72 (1.27–2.33) | 3.55 (2.55–4.96) | 1.12 (1.09–1.15) |
| Model 2 b | 1 | 3.09 (1.82–5.24) | 5.38 (2.97–9.75) | 1.14 (1.09–1.20) |
| DQD of CDBI | <28 | 28–38 | >38 | |
| Case/Control | 114/245 | 156/166 | 236/95 | |
| Model 1 a | 1 | 1.98 (1.43–2.75) | 5.19 (3.64–7.41) | 1.06 (1.04–1.07) |
| Model 2 b | 1 | 2.98 (1.72–5.16) | 7.94 (4.27–14.75) | 1.08 (1.06–1.11) |
| DII | 88/250 | 199/138 | 219/118 | |
| Case/Control | <−1.48 | −1.48–0.80 | >0.80 | |
| Model 1 a | 1 | 3.99 (2.80–5.67) | 5.45 (3.75–7.90) | 1.37 (1.28–1.47) |
| Model 2 b | 1 | 12.62 (6.09–26.16) | 31.03 (12.33–78.09) | 2.20 (1.81–2.68) |
| Pathological Classification c | Model 1 a | p | Model 2 b | p |
|---|---|---|---|---|
| Astrocytoma (n = 104) | ||||
| CHEI | 0.93 (0.90–0.96) | <0.001 | 0.89 (0.83–0.96) | 0.001 |
| DAI | 0.93 (0.87–0.99) | 0.016 | 0.01 (0.001–0.60) | 0.027 |
| LBS of CDQI | 0.99 (0.96–1.02) | 0.659 | 1.01 (0.93–1.11) | 0.798 |
| HBS of CDQI | 1.03 (1.01–1.05) | 0.020 | 1.03 (0.99–1.08) | 0.167 |
| DQD of CDQI | 1.02 (1.00–1.05) | 0.050 | 1.04 (0.99–1.09) | 0.131 |
| LBS of CDBI | 1.06 (1.02–1.09) | 0.001 | 1.16 (1.06–1.27) | 0.001 |
| HBS of CDBI | 1.16 (1.08–1.24) | <0.001 | 1.19 (1.05–1.34) | 0.005 |
| DQD of CDBI | 1.06 (1.03–1.10) | <0.001 | 1.17 (1.07–1.29) | 0.001 |
| DII | 1.40 (1.19–1.63) | <0.001 | 5.49 (1.92–15.69) | 0.001 |
| Glioblastoma (n = 237) | ||||
| CHEI | 0.93 (0.91–0.95) | <0.001 | 0.83 (0.77–0.90) | <0.001 |
| DAI | 0.94 (0.90–0.99) | 0.007 | 0.71 (0.59–0.87) | 0.001 |
| LBS of CDQI | 1.00 (0.98–1.03) | 0.731 | 1.02 (0.96–1.09) | 0.554 |
| HBS of CDQI | 1.04 (1.02–1.06) | <0.001 | 1.02 (0.98–1.05) | 0.411 |
| DQD of CDQI | 1.04 (1.02–1.05) | <0.001 | 1.02 (0.99–1.06) | 0.244 |
| LBS of CDBI | 1.05 (1.03–1.07) | <0.001 | 1.14 (1.06–1.22) | 0.001 |
| HBS of CDBI | 1.11 (1.07–1.16) | <0.001 | 1.12 (1.04–1.22) | 0.004 |
| DQD of CDBI | 1.05 (1.03–1.07) | <0.001 | 1.10 (1.05–1.15) | <0.001 |
| DII | 1.41 (1.26–1.56) | <0.001 | 2.21 (1.52–3.20) | <0.001 |
| Glioma Grading c | Model 1 a | p | Model 2 b | p |
|---|---|---|---|---|
| Low grade (n = 105) | ||||
| CHEI | 0.93 (0.90–0.96) | <0.001 | 0.91 (0.86–0.96) | 0.001 |
| DAI | 0.92 (0.87–0.99) | 0.017 | 0.27 (0.12–0.61) | 0.001 |
| LBS of CDQI | 1.01 (0.97–1.04) | 0.773 | 0.95 (0.85–1.05) | 0.313 |
| HBS of CDQI | 1.03 (1.01–1.06) | 0.017 | 1.03 (0.99–1.08) | 0.164 |
| DQD of CDQI | 1.03 (1.01–1.05) | 0.014 | 1.02 (0.98–1.07) | 0.303 |
| LBS of CDBI | 1.07 (1.03–1.10) | <0.001 | 1.12 (1.04–1.20) | 0.002 |
| HBS of CDBI | 1.15 (1.06–1.24) | <0.001 | 1.29 (1.08–1.54) | 0.005 |
| DQD of CDBI | 1.07 (1.04–1.10) | <0.001 | 1.13 (1.05–1.22) | 0.001 |
| DII | 1.37 (1.17–1.59) | <0.001 | 3.21 (1.58–6.52) | 0.001 |
| High grade (n = 328) | ||||
| CHEI | 0.93 (0.91–0.95) | <0.001 | 0.87 (0.83–0.91) | <0.001 |
| DAI | 0.95 (0.92–0.99) | 0.005 | 0.69 (0.59–0.81) | <0.001 |
| LBS of CDQI | 0.99 (0.98–1.02) | 0.829 | 1.02 (0.98–1.08) | 0.347 |
| HBS of CDQI | 1.04 (1.02–1.06) | <0.001 | 1.03 (0.99–1.06) | 0.095 |
| DQD of CDQI | 1.03 (1.02–1.05) | <0.001 | 1.03 (1.01–1.06) | 0.035 |
| LBS of CDBI | 1.04 (1.03–1.06) | <0.001 | 1.10 (1.05–1.15) | <0.001 |
| HBS of CDBI | 1.11 (1.07–1.15) | <0.001 | 1.14 (1.07–1.22) | <0.001 |
| DQD of CDBI | 1.05 (1.03–1.07) | <0.001 | 1.09 (1.05–1.13) | <0.001 |
| DII | 1.36 (1.25–1.49) | <0.001 | 2.20 (1.67–2.89) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.; He, Y.; Chen, F.; Wang, C.; Kang, X.; Peng, Y.; Li, W. Chinese Dietary Indices and Glioma: New Insights of a Case–Control Study in the Chinese Population. Nutrients 2023, 15, 3602. https://doi.org/10.3390/nu15163602
Zhang W, He Y, Chen F, Wang C, Kang X, Peng Y, Li W. Chinese Dietary Indices and Glioma: New Insights of a Case–Control Study in the Chinese Population. Nutrients. 2023; 15(16):3602. https://doi.org/10.3390/nu15163602
Chicago/Turabian StyleZhang, Weichunbai, Yongqi He, Feng Chen, Ce Wang, Xun Kang, Yue Peng, and Wenbin Li. 2023. "Chinese Dietary Indices and Glioma: New Insights of a Case–Control Study in the Chinese Population" Nutrients 15, no. 16: 3602. https://doi.org/10.3390/nu15163602
APA StyleZhang, W., He, Y., Chen, F., Wang, C., Kang, X., Peng, Y., & Li, W. (2023). Chinese Dietary Indices and Glioma: New Insights of a Case–Control Study in the Chinese Population. Nutrients, 15(16), 3602. https://doi.org/10.3390/nu15163602