
The Indicator of Emotional Eating and Its Effects on Dietary Patterns among Female Students at Qassim University


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Ethical Consideration
2.3. Data Collection
2.4. Questionnaire
2.4.1. Demographic Information
2.4.2. Anthropometrics Measurements
2.4.3. Emotional Eating Scale (EES)
2.4.4. Food Frequency Questionnaire (FFQ)
2.5. Statistical Analysis
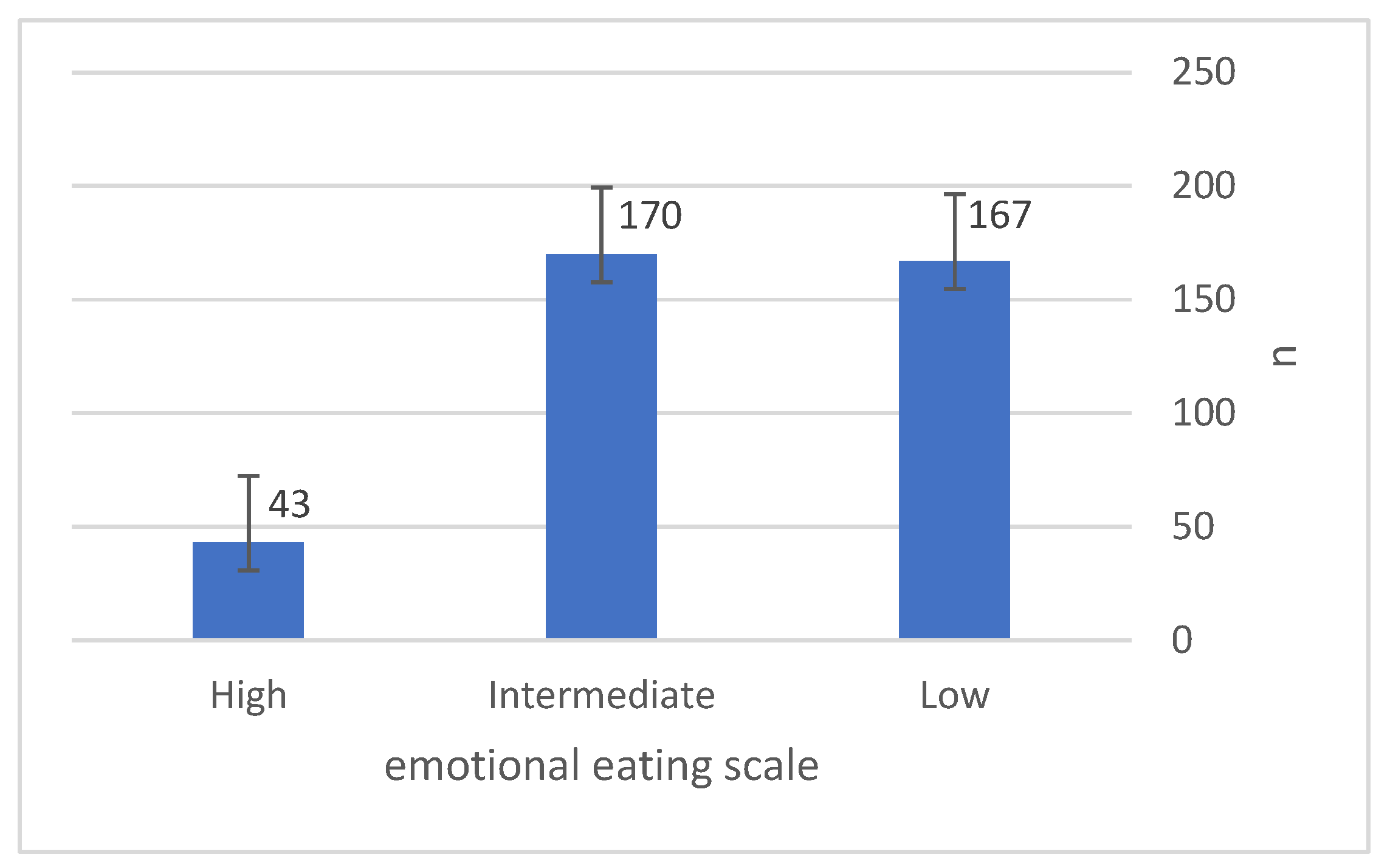
3. Results
3.1. The Associations between the Demographics and EE
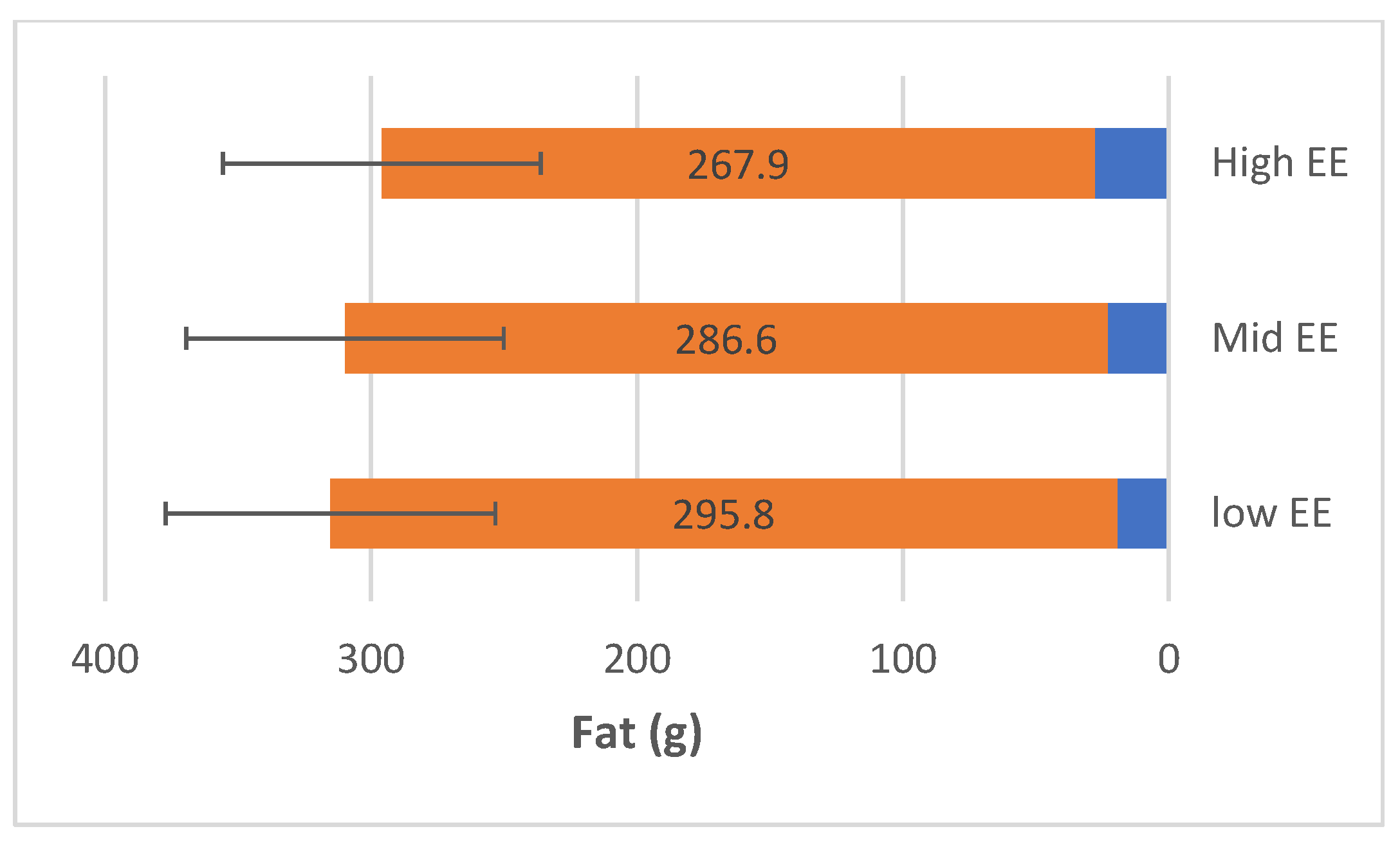
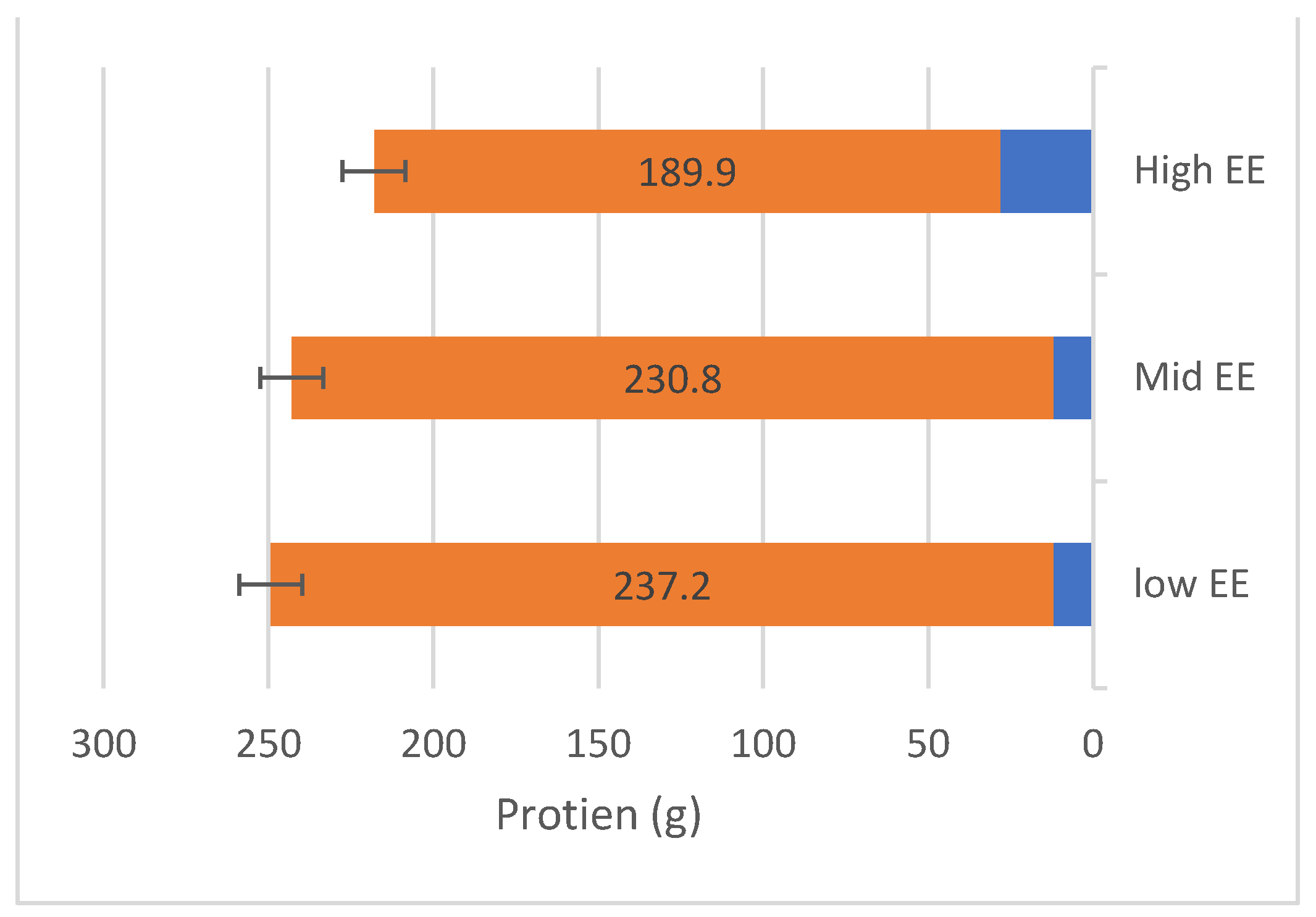
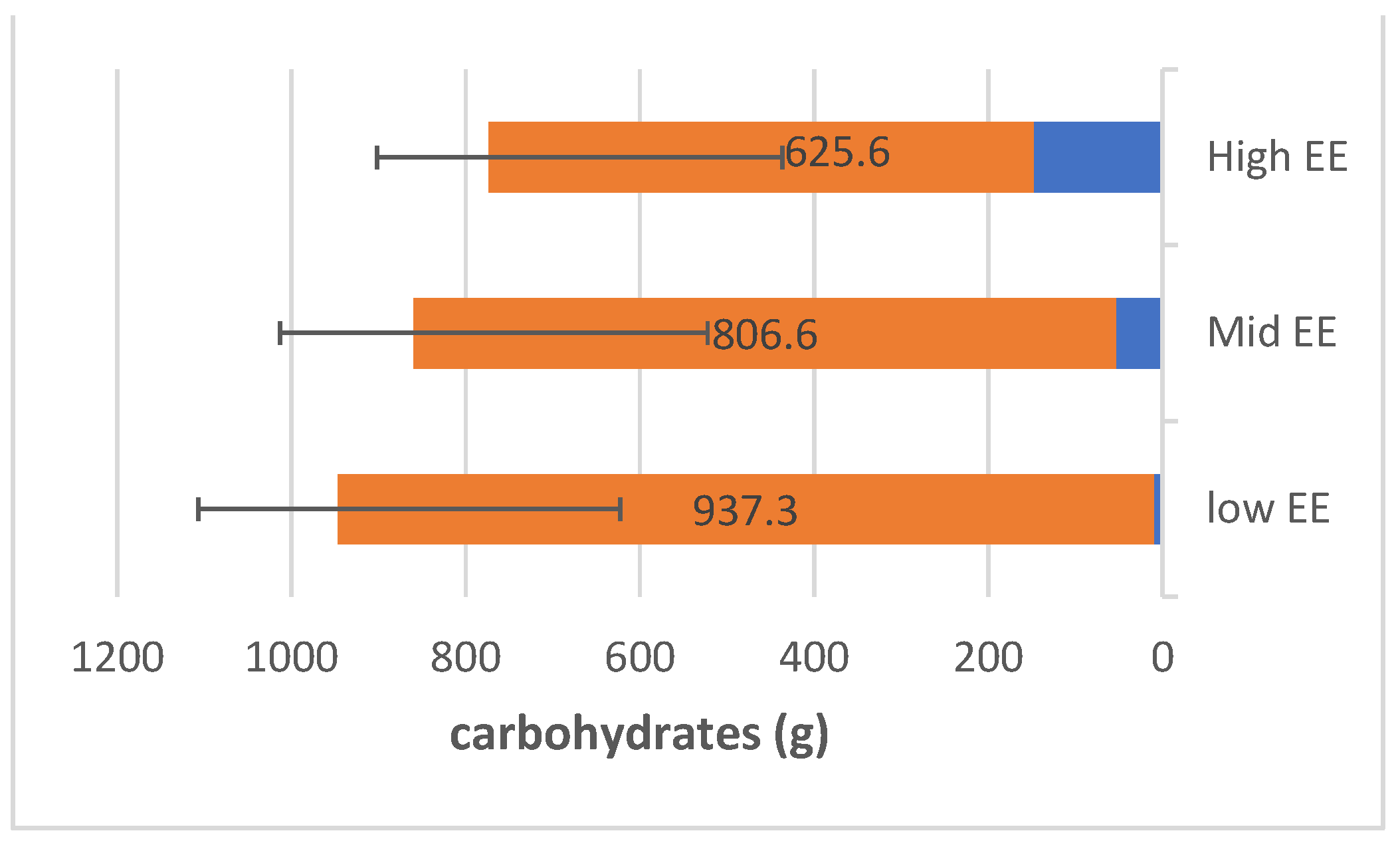
3.2. The Association between Eating Patterns and EE
Mean Macronutrient Intake
3.3. The Association between Anthropometric Measurements and Emotional Eating
3.4. The Linear Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manchón, J.; Quiles, M.J.; Quiles, Y.; López-Roig, S. Positive and Negative Emotional Eating Are Not the Same-The Spanish Version of the Positive-Negative Emotional Eating Scale (PNEES). Front. Psychol. 2021, 12, 709570. [Google Scholar] [CrossRef]
- Naja, F.; Hamadeh, R. Nutrition amid the COVID-19 Pandemic: A Multi-Level Framework for Action. Eur. J. Clin. Nutr. 2020, 74, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, H. Emotional Eating and Obesity in Adults: The Role of Depression, Sleep and Genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Ripoll, M.; Bernard, M.-C.; Vaure, C.; Bazin, E.; Commandeur, S.; Perkov, V.; Lemdani, K.; Nicolaï, M.-C.; Bonifassi, P.; Kichler, A.; et al. An Imidazole Modified Lipid Confers Enhanced MRNA-LNP Stability and Strong Immunization Properties in Mice and Non-Human Primates. Biomaterials 2022, 286, 121570. [Google Scholar] [CrossRef] [PubMed]
- Betancourt-Núñez, A.; Nava-Amante, P.A.; Bernal-Orozco, M.F.; Vizmanos, B.; Vargas-García, E.J.; Márquez-Sandoval, F.; Salas-García, M.A.; Díaz-López, A. Food Insecurity Was Negatively Associated with Adherence to the “Fruits, Vegetables, and Foods Rich in Animal Protein” Dietary Pattern among University Students’ Households: The 2018 Mexican National Household Survey. BMC Public Health 2023, 23, 854. [Google Scholar] [CrossRef]
- Betancourt-Núñez, A.; Torres-Castillo, N.; Martínez-López, E.; De Loera-Rodríguez, C.O.; Durán-Barajas, E.; Márquez-Sandoval, F.; Bernal-Orozco, M.F.; Garaulet, M.; Vizmanos, B. Emotional Eating and Dietary Patterns: Reflecting Food Choices in People with and without Abdominal Obesity. Nutrients 2022, 14, 1371. [Google Scholar] [CrossRef]
- Fuente González, C.E.; Chávez-Servín, J.L.; de la Torre-Carbot, K.; Ronquillo González, D.; de los Ángeles Aguilera Barreiro, M.; Ojeda Navarro, L.R. Relationship between Emotional Eating, Consumption of Hyperpalatable Energy-Dense Foods, and Indicators of Nutritional Status: A Systematic Review. J. Obes. 2022, 2022, 4243868. [Google Scholar] [CrossRef]
- Frayn, M.; Livshits, S.; Knäuper, B. Emotional Eating and Weight Regulation: A Qualitative Study of Compensatory Behaviors and Concerns. J. Eat. Disord. 2018, 6, 23. [Google Scholar] [CrossRef]
- Stok, F.M.; Renner, B.; Clarys, P.; Lien, N.; Lakerveld, J.; Deliens, T. Understanding Eating Behavior during the Transition from Adolescence to Young Adulthood: A Literature Review and Perspective on Future Research Directions. Nutrients 2018, 10, 667. [Google Scholar] [CrossRef]
- Nieves, G.L.; Cordobés, E.S.; Fernández, A.G.; González, G.T.; Padilla, F.M.G. Habits, Preferences and Culinary Skills of First-Year Students at the University of Huelva TT—Hábitos, Preferencias y Habilidades Culinarias de Estudiantes de Primer Curso de La Universidad de Huelva. Enferm. Glob. 2019, 18, 142–156. [Google Scholar]
- Sogari, G.; Velez-Argumedo, C.; Gómez, M.I.; Mora, C. College Students and Eating Habits: A Study Using an Ecological Model for Healthy Behavior. Nutrients 2018, 10, 1823. [Google Scholar] [CrossRef] [PubMed]
- Ganasegeran, K.; Al-Dubai, S.A.R.; Qureshi, A.M.; Al-Abed, A.-A.A.A.; Am, R.; Aljunid, S.M. Social and Psychological Factors Affecting Eating Habits among University Students in a Malaysian Medical School: A Cross-Sectional Study. Nutr. J. 2012, 11, 48. [Google Scholar] [CrossRef]
- Cheung, D.K.; Tam, D.K.Y.; Tsang, M.H.; Zhang, D.L.W.; Lit, D.S.W. Depression, Anxiety and Stress in Different Subgroups of First-Year University Students from 4-Year Cohort Data. J. Affect. Disord. 2020, 274, 305–314. [Google Scholar] [CrossRef]
- Almogbel, E.; Aladhadh, A.M.; Almotyri, B.H.; Alhumaid, A.F.; Rasheed, N. Stress Associated Alterations in Dietary Behaviours of Undergraduate Students of Qassim University, Saudi Arabia. Open Access Maced. J. Med. Sci. 2019, 7, 2182–2188. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Rodríguez, C.; Soto-López, T.; Cuesta, M. Needs and Demands for Psychological Care in University Students. Psicothema 2019, 31, 414–421. [Google Scholar] [CrossRef]
- Constant, A.; Gautier, Y.; Coquery, N.; Thibault, R.; Moirand, R.; Val-Laillet, D. Emotional Overeating Is Common and Negatively Associated with Alcohol Use in Normal-Weight Female University Students. Appetite 2018, 129, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Deliens, T.; Clarys, P.; De Bourdeaudhuij, I.; Deforche, B. Determinants of Eating Behaviour in University Students: A Qualitative Study Using Focus Group Discussions. BMC Public Health 2014, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Bongers, P.; Jansen, A.; Houben, K.; Roefs, A. Happy Eating: The Single Target Implicit Association Test Predicts Overeating after Positive Emotions. Eat. Behav. 2013, 14, 348–355. [Google Scholar] [CrossRef]
- Bennett, P.N.; Miller, M.D.; Woodman, R.J.; Hill, K.; Murray, S.; Gleadle, J.M. Nutrition Screening by Nurses in Dialysis. J. Clin. Nurs. 2013, 22, 723–732. [Google Scholar] [CrossRef]
- Alalwan, T.A.; Hilal, S.J.; Mahdi, A.M.; Ahmed, M.A.; Mandeel, Q.A. Emotional Eating Behavior among University of Bahrain Students: A Cross-Sectional Study. Arab. J. Basic Appl. Sci. 2019, 26, 424–432. [Google Scholar] [CrossRef]
- Abraham, S.; Noriega, B.R.; Shin, J.Y. College Students Eating Habits and Knowledge of Nutritional Requirements. J. Nutr. Hum. Health 2018, 2, 13–17. [Google Scholar] [CrossRef]
- Butler, S.M.; Black, D.R.; Blue, C.L.; Gretebeck, R.J. Change in Diet, Physical Activity, and Body Weight in Female College Freshman. Am. J. Health Behav. 2004, 28, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Choi, J. Impact of Stress Levels on Eating Behaviors among College Students. Nutrients 2020, 12, 1241. [Google Scholar] [CrossRef]
- Crombie, D.; Lombard, C.; Noakes, T. Emotional Intelligence Scores Predict Team Sports Performance in a National Cricket Competition. Int. J. Sports Sci. Coach. 2009, 4, 209–224. [Google Scholar] [CrossRef]
- Arnow, B.; Kenardy, J.; Agras, W.S. The Emotional Eating Scale: The Development of a Measure to Assess Coping with Negative Affect by Eating. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). WHO|Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation, Geneva, Switzerland, 8–11 December 2008; WHO: Geneva, Switzerland, 2018; pp. 8–11. [Google Scholar]
- Deliens, T.; Deforche, B.; Chapelle, L.; Clarys, P. Changes in Weight and Body Composition across Five Years at University: A Prospective Observational Study. PLoS ONE 2019, 14, e0225187. [Google Scholar] [CrossRef]
- Jaremków, A.; Markiewicz-Górka, I.; Pawlas, K. Assessment of Health Condition as Related to Lifestyle among Students in the Examination Period. Int. J. Occup. Med. Environ. Health 2020, 33, 339–351. [Google Scholar] [CrossRef]
- Saade, S.; Hallit, S.; Haddad, C.; Hallit, R.; Akel, M.; Honein, K.; Akiki, M.; Kheir, N.; Obeid, S. Factors Associated with Restrained Eating and Validation of the Arabic Version of the Restrained Eating Scale among an Adult Representative Sample of the Lebanese Population: A Cross-Sectional Study. J. Eat. Disord. 2019, 7, 24. [Google Scholar] [CrossRef]
- Waller, G.; Osman, S. Emotional Eating and Eating Psychopathology among Non-Eating-Disordered Women. Int. J. Eat. Disord. 1998, 23, 419–424. [Google Scholar] [CrossRef]
- Al-Musharaf, S. Prevalence Awend Predictors of Emotional Eating among Healthy Young Saudi Women during the COVID-19 Pandemic. Nutrients 2020, 12, 2923. [Google Scholar] [CrossRef]
- Alkhalaf, M.M.; Edwards, C.A.; Combet, E. Validation of a Food Frequency Questionnaire Specific for Salt Intake in Saudi Arabian Adults Using Urinary Biomarker and Repeated Multiple Pass 24-Hour Dietary Recall. Proc. Nutr. Soc. 2015, 74, E337. [Google Scholar] [CrossRef]
- Almutairi, A.; Jahan, S. Prevalence of Anxiety among Qassim University Female Medical Students during COVID-19 Pandemic in Saudi Arabia. Health Psychol. Res. 2022, 10, 1–8. [Google Scholar] [CrossRef]
- Herle, M.; Fildes, A.; Rijsdijk, F.; Steinsbekk, S.; Llewellyn, C. The Home Environment Shapes Emotional Eating. Child Dev. 2017, 89, 1423–1434. [Google Scholar] [CrossRef]
- Aloudah, M.A. Exploring Saudi Adolescents’ Perceptions of Emotional Eating with the Purpose of Informing the Design of an Online Health Awareness Programme; University of Reading: London, UK, 2021. [Google Scholar]
- Alafif, N.O.; Abdelfattah, E.H.; Al Hadi, R.A.; Alanazi, S.B.; Alkabaa, R.I.; Alsalem, F.A.; Aljeldah, T.M.; Aldriweesh, K.K.; Albati, A.A. Effect of Quarantine on Eating Behaviors and Weight Change among King Saud University Students in Riyadh. J. King Saud Univ. Sci. 2021, 33, 101609. [Google Scholar] [CrossRef]
- Işik, K.; Cengïz, Z. The Effect of Sociodemographic Characteristics of University Students on Emotional Eating Behavior. Perspect. Psychiatr. Care 2021, 57, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Hasan, H.A.; Ismat, H.; Hakim, H.; Khalid, H.; Al-Fityani, L.; Mohammed, R.; Ayman, A. Body Mass Index Perception, Body Image Dissatisfaction and Their Relations with Weight-Related Behaviors among University Students. Int. J. Environ. Res. Public Health 2019, 16, 1541. [Google Scholar] [CrossRef]
- Ferrer-Cascales, R.; Sánchez-SanSegundo, M.; Ruiz-Robledillo, N.; Albaladejo-Blázquez, N.; Laguna-Pérez, A.; Zaragoza-Martí, A. Eat or Skip Breakfast? The Important Role of Breakfast Quality for Health-Related Quality of Life, Stress and Depression in Spanish Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 1781. [Google Scholar] [CrossRef]
- Wallis, D.J.; Hetherington, M.M. Stress and Eating: The Effects of Ego-Threat and Cognitive Demand on Food Intake in Restrained and Emotional Eaters. Appetite 2004, 43, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Toledo, E.; De Irala, J.; Ruiz-Canela, M.; Pla-Vidal, J.; Martínez-González, M.A. Fast-Food and Commercial Baked Goods Consumption and the Risk of Depression. Public Health Nutr. 2012, 15, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Veselska, Z.D.; Husarova, D.; Kosticova, M. Energy Drinks Consumption Associated with Emotional and Behavioural Problems via Lack of Sleep and Skipped Breakfast among Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 6055. [Google Scholar] [CrossRef]
- Perveen, A.; Hamzah, H.B.; Ramlee, F.; Morgul, E.; Govindasamy, P. Skipping Breakfast and Lack of Physical Activity; Contributing Factors of Depressive Symptoms among University Students. Int. J. Acad. Res. Bus. Soc. Sci. 2018, 8, 12–23. [Google Scholar] [CrossRef]
- Jahrami, H.; Al-Mutarid, M.; Penson, P.E.; Al-Islam Faris, M.; Saif, Z.; Hammad, L. Intake of Caffeine and Its Association with Physical and Mental Health Status among University Students in Bahrain. Foods 2020, 9, 473. [Google Scholar] [CrossRef]
- Kharaba, Z.; Sammani, N.; Ashour, S.; Ghemrawi, R.; Al Meslamani, A.Z.; Al-Azayzih, A.; Buabeid, M.A.; Alfoteih, Y. Caffeine Consumption among Various University Students in the UAE, Exploring the Frequencies, Different Sources and Reporting Adverse Effects and Withdrawal Symptoms. J. Nutr. Metab. 2022, 2022, 5762299. [Google Scholar] [CrossRef]
- Salem, V.; AlHusseini, N.; Abdul Razack, H.I.; Naoum, A.; Sims, O.T.; Alqahtani, S.A. Prevalence, Risk Factors, and Interventions for Obesity in Saudi Arabia: A Systematic Review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2022, 23, e13448. [Google Scholar] [CrossRef]
- Alshibani, K. World Health Survey Saudi Arabia; Saudi Arabia Ministry of Health: Riyadh, Saudi Arabia, 2019; Volume 1, pp. 5–24. [Google Scholar]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Tuffaha, M.; Daoud, F.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Mazroa, M.A.; Al Rabeeah, A.A.; Mokdad, A.H. The Health of Saudi Youths: Current Challenges and Future Opportunities. BMC Fam. Pract. 2016, 17, 26. [Google Scholar] [CrossRef]
- ALAhmari, T.; Alomar, A.Z.; ALBeeybe, J.; Asiri, N.; ALAjaji, R.; ALMasoud, R.; Al-Hazzaa, H.M. Associations of Self-Esteem with Body Mass Index and Body Image among Saudi College-Age Females. Eat. Weight Disord. 2019, 24, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Alhazmi, A.; Aziz, F.; Hawash, M.M. Association of BMI, Physical Activity with Academic Performance among Female Students of Health Colleges of King Khalid University, Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 10912. [Google Scholar] [CrossRef]
- El Azab, E.F.; Elwasefy, S.A.; Shaban, H.E.; Mohamed, F.A.M.; Alsharari, A.H. Obesity Related Risk Factors among the Saudi Female Students in Jouf University. J. Health Med. Nurs. 2019, 4, 38–49. [Google Scholar]
- Balgoon, M.J.; Al-Zahrani, M.H.; Alkhattabi, N.A.; Alzahrani, N.A. The Correlation between Obesity and Metabolic Syndrome in Young Female University Students in the Kingdom of Saudi Arabia. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2399–2402. [Google Scholar] [CrossRef] [PubMed]
- Alowfi, A.; Binladen, S.; Irqsous, S.; Khashoggi, A.; Khan, M.A.; Calacattawi, R. Metabolic Syndrome: Prevalence and Risk Factors among Adolescent Female Intermediate and Secondary Students in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 2142. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y. Relationship between Eating Style and Food Intake of Healthy Female College Students during Chuseok Holidays. Korean J. Community Nutr. 2016, 21, 131. [Google Scholar] [CrossRef]
- van Strien, T.; Donker, M.H.; Ouwens, M.A. Is Desire to Eat in Response to Positive Emotions an “obese” Eating Style: Is Kummerspeck for Some People a Misnomer? Appetite 2016, 100, 225–235. [Google Scholar] [CrossRef] [PubMed]
- van Strien, T.; Herman, C.P.; Verheijden, M.W. Eating Style, Overeating and Weight Gain. A Prospective 2-Year Follow-up Study in a Representative Dutch Sample. Appetite 2012, 59, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Kauffman, B.Y.; Rosenfield, D.; Smits, J.A.J.; Zvolensky, M.J. Emotion Dysregulation and Body Mass Index: The Explanatory Role of Emotional Eating among Adult Smokers. Eat. Behav. 2019, 33, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Bui, C.; Lin, L.-Y.; Wu, C.-Y.; Chiu, Y.-W.; Chiou, H.-Y. Association between Emotional Eating and Frequency of Unhealthy Food Consumption among Taiwanese Adolescents. Nutrients 2021, 13, 2739. [Google Scholar] [CrossRef] [PubMed]
- Heath, G.; Dorrian, J.; Coates, A. Associations between Shift Type, Sleep, Mood, and Diet in a Group of Shift Working Nurses. Scand. J. Work Environ. Health 2019, 45, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Saleh-Ghadimi, S.; Dehghan, P.; Abbasalizad Farhangi, M.; Asghari-Jafarabadi, M.; Jafari-Vayghan, H. Could Emotional Eating Act as a Mediator between Sleep Quality and Food Intake in Female Students? Biopsychosoc. Med. 2019, 13, 15. [Google Scholar] [CrossRef]
- Abdella, H.M.; El Farssi, H.O.; Broom, D.R.; Hadden, D.A.; Dalton, C.F. Eating Behaviours and Food Cravings; Influence of Age, Sex, BMI and FTO Genotype. Nutrients 2019, 11, 377. [Google Scholar] [CrossRef]
- Bilici, S.; Ayhan, B.; Karabudak, E.; Koksal, E. Factors Affecting Emotional Eating and Eating Palatable Food in Adults. Nutr. Res. Pract. 2020, 14, 70–75. [Google Scholar] [CrossRef]
- Poelman, M.P.; Gillebaart, M.; Schlinkert, C.; Dijkstra, S.C.; Derksen, E.; Mensink, F.; Hermans, R.C.J.; Aardening, P.; de Ridder, D.; de Vet, E. Eating Behavior and Food Purchases during the COVID-19 Lockdown: A Cross-Sectional Study among Adults in the Netherlands. Appetite 2021, 157, 105002. [Google Scholar] [CrossRef]
- Zysberg, L.; Rubanov, A. Emotional Intelligence and Emotional Eating Patterns: A New Insight into the Antecedents of Eating Disorders? J. Nutr. Educ. Behav. 2010, 42, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Okumus, B.; Chaulagain, S.; Giritlioglu, I. The Effects of Demographics and Nutritional Knowledge on Hotel Employees’ External and Emotional Eating. J. Culin. Sci. Technol. 2022, 20, 266–277. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Item | EES n (%) | p-Value | ||
|---|---|---|---|---|---|
| Low | Moderate | High | |||
| Age | 18–22 | 137 (82) | 148 (87.1) | 35 (81.4) | 0.259 |
| 23–25 | 24 (14.4) | 16 (9.4) | 4 (9.3) | ||
| 26–29 | 6 (3.6) | 6 (3.5) | 4 (9.3) | ||
| Marital status | Single | 158 (94.6) | 158 (92.9) | 42 (97.7) | 0.473 |
| Married | 9 (5.4) | 12 (7.1) | 1 (2.3) | ||
| Education level | Bachelor | 162 (97) | 163 (95.9) | 38 (88.4) | 0.023 * |
| Residency | 0 (0) | 0 (0) | 1 (2.3) | ||
| Master | 5 (3) | 7 (4.1) | 4 (9.3) | ||
| GPA | Fresh students | 11 (6.6) | 15 (8.8) | 3 (7) | 0.585 |
| <2.5 | 1 (0.6) | 0 (0) | 0 (0) | ||
| 2.5–3.5 | 15 (9) | 21 (12.4) | 5 (11.6) | ||
| 3.5–4.5 | 69 (41.3) | 51 (30) | 15 (34.9) | ||
| 4.5–5 | 71 (42.5) | 83 (48.8) | 20 (46.5) | ||
| Family income level | <5 K SR | 20 (12) | 19 (11.2) | 2 (4.7) | 0.767 |
| 5–10 K SR | 44 (26.3) | 50 (29.4) | 16 (37.2) | ||
| 10–15 K SR | 48 (28.7) | 46 (27.1) | 12 (27.9) | ||
| >15 K SR | 55 (32.9) | 55 (32.4) | 13 (30.2) | ||
| Number of family members | 2–4 | 12 (7.2) | 14 (8.2) | 3 (7) | 0.03 * |
| 5–7 | 42 (25.1) | 64 (37.6) | 20 (46.5) | ||
| 8–10 | 98 (58.7) | 71 (41.8) | 17 (39.5) | ||
| >10 | 15 (9) | 21 (12.4) | 3 (7) | ||
| Variables | Items | EES n (%) | p-Value | ||
|---|---|---|---|---|---|
| Low | Moderate | High | |||
| Following a healthy eating pattern at home | Yes | 38 (22.8) | 37 (21.8) | 12 (27.9) | 0.341 |
| No | 88 (52.7) | 77 (45.3) | 22 (51.2) | ||
| Sometimes | 41 (24.6) | 56 (32.9) | 9 (20.9) | ||
| Number of meals/day | One meal | 28 (16.8) | 21 (12.4) | 8 (18.6) | 0.846 |
| Two meals | 83 (49.7) | 93 (54.7) | 22 (51.2) | ||
| Three meals | 47 (28.1) | 44 (25.9) | 10 (23.3) | ||
| Four or more meals | 9 (5.4) | 12 (7.1) | 3 (7) | ||
| Main meal/day | Breakfast | 42 (25.1) | 50 (29.4) | 19 (44.2) | 0.043 * |
| Lunch | 54 (32.3) | 65 (38.2) | 9 (20.9) | ||
| Dinner | 71 (42.5) | 55 (32.4) | 15 (34.9) | ||
| Having breakfast | Yes | 67 (40.1) | 80 (47.1) | 24 (55.8) | 0.409 |
| No | 34 (20.4) | 31 (18.2) | 6 (14) | ||
| Sometimes | 66 (39.5) | 59 (34.7) | 13 (30.2) | ||
| Cravings for sugary foods (cookies/chocolate/ice cream, etc.) | Rare | 32 (19.2) | 28 (16.5) | 6 (14) | 0.691 |
| Sometimes | 93 (55.7) | 91 (53.5) | 22 (51.2) | ||
| Always | 42 (25.1) | 51 (30) | 15 (34.9) | ||
| Craving for tea | Rare | 85 (50.9) | 90 (52.9) | 21 (48.8) | 0.990 |
| Sometimes | 53 (31.7) | 52 (30.6) | 14 (32.6) | ||
| Always | 29 (17.4) | 28 (16.5) | 8 (18.6) | ||
| Craving for coffee | Rare | 24 (14.4) | 23 (13.5) | 7 (16.3) | 0.675 |
| Sometimes | 49 (29.3) | 40 (23.5) | 13 (30.2) | ||
| Always | 94 (56.3) | 107 (62.9) | 23 (53.5) | ||
| Fast food consumption/week | Once | 82 (49.1) | 78 (45.9) | 15 (34.9) | 0.303 |
| Twice | 28 (16.8) | 42 (24.7) | 13 (30.2) | ||
| Three times | 20 (12) | 15 (8.8) | 7 (16.3) | ||
| Four or more times | 3 (1.8) | 5 (2.9) | 2 (4.7) | ||
| I do not consume | 34 (20.4) | 30 (17.6) | 6 (14) | ||
| Water consumption/day | <1 L | 48 (28.7) | 47 (27.6) | 15 (34.9) | 0.952 |
| 1–1.5 L | 89 (53.3) | 93 (54.7) | 19 (44.2) | ||
| 1.5–2 L | 19 (11.4) | 19 (11.2) | 6 (14) | ||
| >2 L | 11 (6.6) | 11 (6.5) | 3 (7) | ||
| Supplement intake | Multivitamins | 30 (18.4) | 33 (17.5) | 11 (19) | 0.505 |
| Vitamin D | 39 (23.9) | 46 (24.3) | 14 (24.1) | ||
| Vitamin B12 | 16 (9.8) | 21 (11.1) | 4 (6.9) | ||
| Vitamin C | 11 (6.7) | 12 (6.3) | 7 (12.0) | ||
| Folic acid | 10 (6.1) | 12 (6.3) | 2 (3.6) | ||
| Iron | 34 (20.8) | 24 (12.7) | 8 (13.8) | ||
| Cod liver oil | 6 (3.7) | 13 (6.8) | 3 (5.1) | ||
| Protein supplements/bars | 16 (9.8) | 26 (13.8) | 8 (13.8) | ||
| Chlorophyll | 0 (0.0) | 1 (0.5) | 0 (0.0) | ||
| Zinc | 1 (0.6) | 1 (0.5) | 0 (0.0) | ||
| Variables | Items | EES n (%) | p-Value | ||
|---|---|---|---|---|---|
| Low | Moderate | High | |||
| BMI | Underweight | 29 (17.4) | 29 (17.1) | 5 (11.6) | 0.562 |
| Normal weight | 94 (56.3) | 90 (52.9) | 21 (48.8) | ||
| Overweight | 28 (16.8) | 38 (22.4) | 13 (30.2) | ||
| Obese | 16 (9.6) | 13 (7.6) | 4 (9.3) | ||
| Range | 2.8–48.4 | 1.3–46.1 | 2.8–48.6 | ||
| Mean ± SD | 24.6 ± 9.4 | 23.6 ± 9.3 | 23.6 ± 10.8 | ||
| FFM | Range | 27–60.8 | 9.7–58 | 34.1–58.8 | 0.521 |
| Mean ± SD | 41.9 ± 4.7 | 41.9 ± 5.6 | 42.9 ± 5.5 | ||
| WHR | Low | 159 (95.2) | 158 (92.9) | 38 (88.4) | 0.299 |
| Intermediate | 7 (4.2) | 7 (4.1) | 4 (9.3) | ||
| High | 1 (0.6) | 5 (2.9) | 1 (2.3) | ||
| Variables | Unadjusted | Adjusted | Adj. R2 | ||||
|---|---|---|---|---|---|---|---|
| B ± SE | Std. Beta | p-Value | B ± SE | Std. Beta | p-Value | ||
| Age | 0.006 ± 1.277 | 0.000 | 0.996 | −3.081 ± 1.833 | −0.124 | 0.094 | 0.007 |
| Education level | 2.999 ± 1.553 | 0.099 | 0.054 | 5.403 ± 2.126 | 0.178 | 0.011 * | 0.017 |
| Family income level | 0.178 ± 0.627 | 0.015 | 0.777 | 0.206 ± 0.642 | 0.017 | 0.749 | 0.000 |
| BMI | 0.004 ± 0.132 | 0.002 | 0.975 | 0.045 ± 0.133 | 0.018 | 0.735 | 0.000 |
| Daily activity | 0.507 ± 0.948 | 0.027 | 0.593 | 0.653 ± 0.965 | 0.035 | 0.499 | 0.001 |
| Number of meals | −0.393 ± 0.808 | −0.025 | 0.627 | −0.287 ± 0.82 | −0.018 | 0.726 | 0.000 |
| Fat intake | 2.978 ± 1.322 | 0.115 | 0.025 * | 3.243 ± 1.496 | 0.125 | 0.031 * | 0.012 |
| Sugar intake | 0.863 ± 1.496 | 0.030 | 0.564 | −0.678 ± 1.659 | −0.023 | 0.683 | 0.000 |
| Carb intake | −2.943 ± 7.130 | −0.021 | 0.680 | −1.492 ± 7.176 | −0.011 | 0.835 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alharbi, R.M.; Alharbi, H.F. The Indicator of Emotional Eating and Its Effects on Dietary Patterns among Female Students at Qassim University. Nutrients 2023, 15, 3553. https://doi.org/10.3390/nu15163553
Alharbi RM, Alharbi HF. The Indicator of Emotional Eating and Its Effects on Dietary Patterns among Female Students at Qassim University. Nutrients. 2023; 15(16):3553. https://doi.org/10.3390/nu15163553
Chicago/Turabian StyleAlharbi, Razan M., and Hend F. Alharbi. 2023. "The Indicator of Emotional Eating and Its Effects on Dietary Patterns among Female Students at Qassim University" Nutrients 15, no. 16: 3553. https://doi.org/10.3390/nu15163553
APA StyleAlharbi, R. M., & Alharbi, H. F. (2023). The Indicator of Emotional Eating and Its Effects on Dietary Patterns among Female Students at Qassim University. Nutrients, 15(16), 3553. https://doi.org/10.3390/nu15163553