
Efficacy of Fasting in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. State-of-the-Art of Intermittent and Periodic Fasting
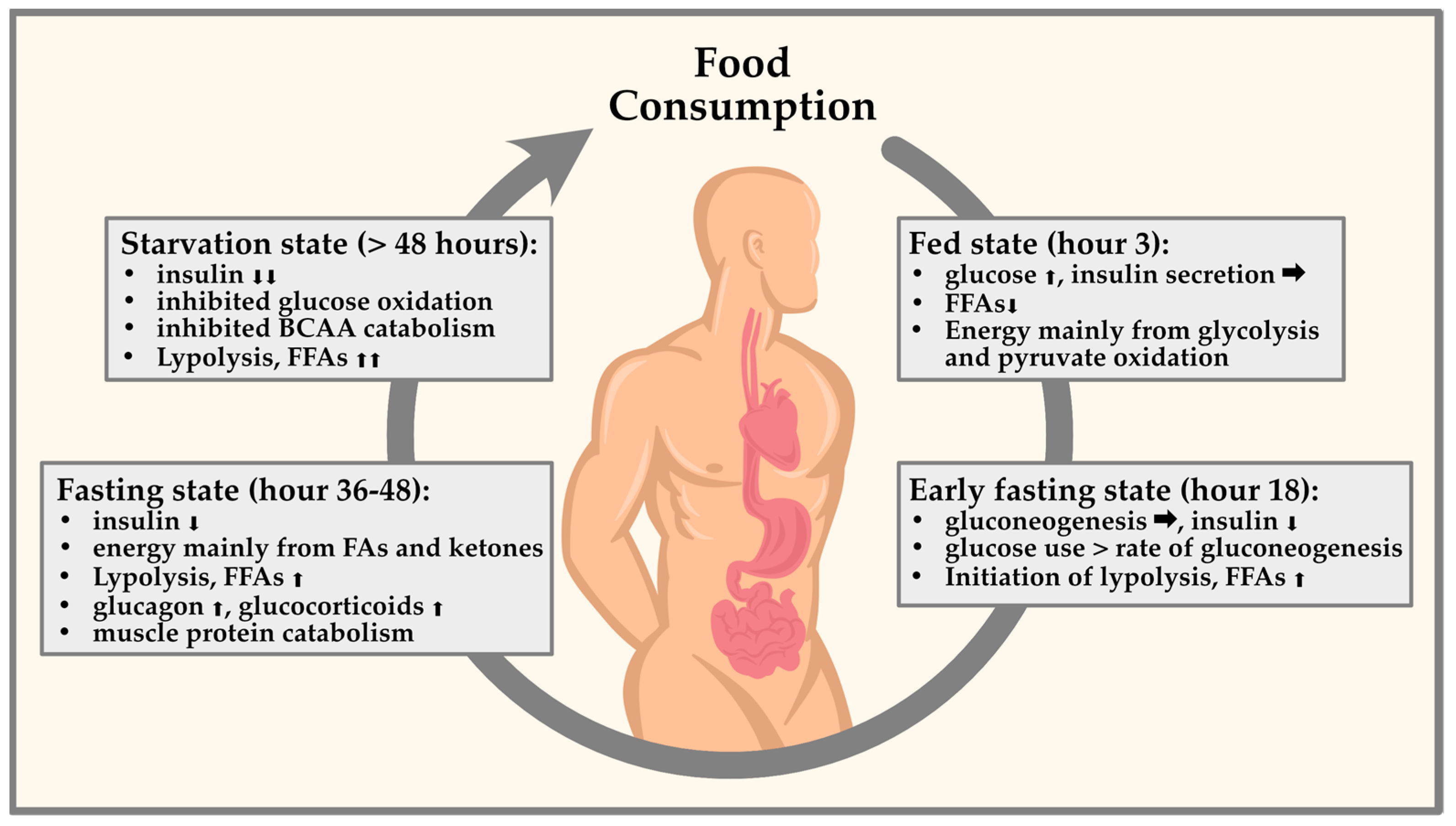
4. Physiological Pathways of Fasting
5. Impact of Fasting as an Adjuvant Therapy in T1DM and T2DM
5.1. Fasting and Its Effects on T1DM
5.2. Fasting and Its Effects on the Prevention of T2DM
5.3. Pharmacotherapy and Fasting in T2DM
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th Edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Patterson, C.C.; Harjutsalo, V.; Rosenbauer, J.; Neu, A.; Cinek, O.; Skrivarhaug, T.; Rami-Merhar, B.; Soltesz, G.; Svensson, J.; Parslow, R.C.; et al. Trends and Cyclical Variation in the Incidence of Childhood Type 1 Diabetes in 26 European Centres in the 25 Year Period 1989–2013: A Multicentre Prospective Registration Study. Diabetologia 2019, 62, 408–417. [Google Scholar] [PubMed]
- Furmli, S.; Elmasry, R.; Ramos, M.; Fung, J. Therapeutic Use of Intermittent Fasting for People with Type 2 Diabetes as an Alternative to Insulin. Case Rep. 2018, 2018, bcr-2017-221854. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef]
- Kilpatrick, E.S.; Rigby, A.S.; Atkin, S.L. Insulin Resistance, the Metabolic Syndrome, and Complication Risk in Type 1 Diabetes: “Double Diabetes” in the Diabetes Control and Complications Trial. Diabetes Care 2007, 30, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Deeb, A.; Al Qahtani, N.; Akle, M.; Singh, H.; Assadi, R.; Attia, S.; Al Suwaidi, H.; Hussain, T.; Naglekerke, N. Attitude, Complications, Ability of Fasting and Glycemic Control in Fasting Ramadan by Children and Adolescents with Type 1 Diabetes Mellitus. Diabetes Res. Clin. Pract. 2017, 126, 10–15. [Google Scholar] [CrossRef]
- Cienfuegos, S.; McStay, M.; Gabel, K.; Varady, K.A. Time Restricted Eating for the Prevention of Type 2 Diabetes. J. Physiol. 2022, 600, 1253–1264. [Google Scholar] [CrossRef] [PubMed]
- Reiter, J.; Wexler, I.D.; Shehadeh, N.; Tzur, A.; Zangen, D. Type 1 Diabetes and Prolonged Fasting. Diabet. Med. 2007, 24, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Berger, B.; Jenetzky, E.; Köblös, D.; Stange, R.; Baumann, A.; Simstich, J.; Michalsen, A.; Schmelzer, K.M.; Martin, D.D. Seven-Day Fasting as a Multimodal Complex Intervention for Adults with Type 1 Diabetes: Feasibility, Benefit and Safety in a Controlled Pilot Study. Nutrition 2021, 86, 111169. [Google Scholar] [CrossRef]
- Lustig, E.; Shubrook, J.H.; Pfotenhauer, K.M. Time-Restricted Feeding and Potential for Type 2 Diabetes Mellitus: A Narrative Review. J. Am. Osteopath. Assoc. 2020, 120, 560–567. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular Mechanisms and Clinical Applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Tapsell, L.; Batterham, M.; Huang, X.F.; Tan, S.Y.; Teuss, G.; Charlton, K.; Oshea, J.; Warensjö, E. Short Term Effects of Energy Restriction and Dietary Fat Sub-Type on Weight Loss and Disease Risk Factors. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 317–325. [Google Scholar] [CrossRef]
- Rothschild, J.; Hoddy, K.K.; Jambazian, P.; Varady, K.A. Time-Restricted Feeding and Risk of Metabolic Disease: A Review of Human and Animal Studies. Nutr. Rev. 2014, 72, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, A. Fasting for Weight Loss: An Effective Strategy or Latest Dieting Trend? Int. J. Obes. 2015, 39, 727–733. [Google Scholar] [CrossRef]
- Tinsley, G.M.; La Bounty, P.M. Effects of Intermittent Fasting on Body Composition and Clinical Health Markers in Humans. Nutr. Rev. 2015, 73, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, A.; Ismail-Beigi, F. Intermittent Fasting and ‘Metabolic Switch’: Effects on Metabolic Syndrome, Prediabetes and Type 2 Diabetes. Diabetes Obes. Metab. 2020, 22, 1496–1510. [Google Scholar] [CrossRef]
- Malinowski, B.; Zalewska, K.; Węsierska, A.; Sokołowska, M.M.; Socha, M.; Liczner, G.; Pawlak-Osińska, K.; Wiciński, M. Intermittent Fasting in Cardiovascular Disorders—An Overview. Nutrients 2019, 11, 673. [Google Scholar] [CrossRef]
- Bhutani, S.; Klempel, M.C.; Berger, R.A.; Varady, K.A. Improvements in Coronary Heart Disease Risk Indicators by Alternate-Day Fasting Involve Adipose Tissue Modulations. Obesity 2010, 18, 2152–2159. [Google Scholar] [CrossRef]
- Klempel, M.C.; Kroeger, C.M.; Varady, K.A. Alternate Day Fasting Increases LDL Particle Size Independently of Dietary Fat Content in Obese Humans. Eur. J. Clin. Nutr. 2013, 67, 783–785. [Google Scholar] [CrossRef]
- Trepanowski, J.F.; Bloomer, R.J. The Impact of Religious Fasting on Human Health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef]
- Abaïdia, A.E.; Daab, W.; Bouzid, M.A. Effects of Ramadan Fasting on Physical Performance: A Systematic Review with Meta-Analysis. Sports Med. 2020, 50, 1009–1026. [Google Scholar] [CrossRef]
- Emara, M.H.; Soliman, H.H.; Elnadry, M.; Mohamed Said, E.; Abd-Elsalam, S.; Elbatae, H.E.; Zaher, T.I.; Ezzeldin, S.; Bazeed, S.; Abdel-Razik, A.; et al. Ramadan Fasting and Liver Diseases: A Review with Practice Advices and Recommendations. Liver Int. 2021, 41, 436–448. [Google Scholar] [CrossRef] [PubMed]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-Hour Time Restricted Feeding on Body Weight and Metabolic Disease Risk Factors in Obese Adults: A Pilot Study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of Eight Weeks of Time-Restricted Feeding (16/8) on Basal Metabolism, Maximal Strength, Body Composition, Inflammation, and Cardiovascular Risk Factors in Resistance-Trained Males. J. Transl. Med. 2016, 14, 290. [Google Scholar]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-Restricted Feeding in Young Men Performing Resistance Training: A Randomized Controlled Trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Stekovic, S.; Hofer, S.J.; Tripolt, N.; Aon, M.A.; Royer, P.; Pein, L.; Stadler, J.T.; Pendl, T.; Prietl, B.; Url, J.; et al. Alternate Day Fasting Improves Physiological and Molecular Markers of Aging in Healthy, Non-Obese Humans. Cell Metab. 2019, 30, 462–476.e6. [Google Scholar] [CrossRef] [PubMed]
- Cook, F.; Langdon-Daly, J.; Serpell, L. Compliance of Participants Undergoing a “5-2” Intermittent Fasting Diet and Impact on Body Weight. Clin. Nutr. ESPEN 2022, 52, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Al-Hourani, H.; Atoum, M. Nutrient Intake and Physical Activity Patterns in Young Women during Ramadan. Orig. Artic. Singap. Med. J. 2007, 48, 906. [Google Scholar]
- Longo, V.D.; Di Tano, M.; Mattson, M.P.; Guidi, N. Intermittent and Periodic Fasting, Longevity and Disease. Nat. Aging 2021, 1, 47. [Google Scholar] [CrossRef]
- Brandhorst, S.; Longo, V.D. Fasting and Caloric Restriction in Cancer Prevention and Treatment. Recent Results Cancer Res. 2016, 207, 241–266. [Google Scholar] [CrossRef]
- Longo, V.D.; Panda, S. Fasting, Circadian Rhythms, and Time-Restricted Feeding in Healthy Lifespan. Cell Metab. 2016, 23, 1048–1059. [Google Scholar] [CrossRef] [PubMed]
- Nencioni, A.; Caffa, I.; Cortellino, S.; Longo, V.D. Fasting and Cancer: Molecular Mechanisms and Clinical Application. Nat. Rev. Cancer 2018, 18, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Haupt, S.; Eckstein, M.L.; Wolf, A.; Zimmer, R.T.; Wachsmuth, N.B.; Moser, O. Eat, Train, Sleep-Retreat? Hormonal Interactions of Intermittent Fasting, Exercise and Circadian Rhythm. Biomolecules 2021, 11, 516. [Google Scholar] [CrossRef]
- Réda, A.; Wassil, M.; Mériem, M.; Alexia, P.; Abdelmalik, H.; Sabine, B.; Nassir, M. Food Timing, Circadian Rhythm and Chrononutrition: A Systematic Review of Time-Restricted Eating’s Effects on Human Health. Nutrients 2020, 12, 3770. [Google Scholar] [CrossRef]
- Parr, E.B.; Heilbronn, L.K.; Hawley, J.A. A Time to Eat and a Time to Exercise. Exerc. Sport Sci. Rev. 2020, 48, 4. [Google Scholar] [CrossRef] [PubMed]
- Charlot, A.; Hutt, F.; Sabatier, E.; Zoll, J. Beneficial Effects of Early Time-Restricted Feeding on Metabolic Diseases: Importance of Aligning Food Habits with the Circadian Clock. Nutrients 2021, 13, 1405. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, H.; Beyl, R.A.; Manna, D.L.D.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef]
- Panda, S. Circadian Physiology of Metabolism. Science 2016, 354, 1008–1015. [Google Scholar] [CrossRef]
- Daas, M.C.; De Roos, N.M. Intermittent Fasting Contributes to Aligned Circadian Rhythms through Interactions with the Gut Microbiome. Benef. Microbes 2021, 12, 147–161. [Google Scholar] [CrossRef]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; De Cabo, R. A Time to Fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef]
- George, F.C. Fuel Metabolism in Starvation. Annu. Rev. Nutr. 2006, 26, 1–22. [Google Scholar] [CrossRef]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G.; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying Health Benefits of Fasting. Obesity 2018, 26, 254. [Google Scholar] [CrossRef] [PubMed]
- Afolabi, P.R.; Jahoor, F.; Jackson, A.A.; Stubbs, J.; Johnstone, A.M.; Faber, P.; Lobley, G.; Gibney, E.; Elia, M. The Effect of Total Starvation and Very Low Energy Diet in Lean Men on Kinetics of Whole Body Protein and Five Hepatic Secretory Proteins. Am. J. Physiol. Endocrinol. Metab. 2007, 293, 1580–1589. [Google Scholar] [CrossRef]
- Soeters, M.R.; Lammers, N.M.; Dubbelhuis, P.F.; Ackermans, M.T.; Jonkers-Schuitema, C.F.; Fliers, E.; Sauerwein, H.P.; Aerts, J.M.; Serlie, M.J. Intermittent Fasting Does Not Affect Whole-Body Glucose, Lipid, or Protein Metabolism. Am. J. Clin. Nutr. 2009, 90, 1244–1251. [Google Scholar] [CrossRef]
- Sakharova, A.A.; Horowitz, J.F.; Surya, S.; Goldenberg, N.; Harber, M.P.; Symons, K.; Barkan, A. Role of Growth Hormone in Regulating Lipolysis, Proteolysis, and Hepatic Glucose Production during Fasting. J. Clin. Endocrinol. Metab. 2008, 93, 2755. [Google Scholar] [CrossRef] [PubMed]
- Sarabhai, T.; Roden, M. Hungry for Your Alanine: When Liver Depends on Muscle Proteolysis. J. Clin. Investig. 2019, 129, 4563. [Google Scholar] [CrossRef] [PubMed]
- Hardie, D.G. AMPK: Positive and Negative Regulation, and Its Role in Whole-Body Energy Homeostasis. Curr. Opin. Cell Biol. 2015, 33, 1–7. [Google Scholar] [CrossRef]
- Mattson, M.P.; Moehl, K.; Ghena, N.; Schmaedick, M.; Cheng, A. Intermittent Metabolic Switching, Neuroplasticity and Brain Health. Nat. Rev. Neurosci. 2018, 19, 81–94. [Google Scholar] [CrossRef]
- Aksungar, F.B.; Topkaya, A.E.; Akyildiz, M. Interleukin-6, C-Reactive Protein and Biochemical Parameters during Prolonged Intermittent Fasting. Ann. Nutr. Metab. 2007, 51, 88–95. [Google Scholar] [CrossRef]
- Knapp, M.; Tu, X.; Wu, R. Vascular Endothelial Dysfunction, a Major Mediator in Diabetic Cardiomyopathy. Acta Pharmacol. Sin. 2019, 40, 1–8. [Google Scholar] [CrossRef]
- Mokhtari, P.; Metos, J.; Anandh Babu, P.V. Impact of Type 1 Diabetes on the Composition and Functional Potential of Gut Microbiome in Children and Adolescents: Possible Mechanisms, Current Knowledge, and Challenges. Gut. Microbes 2021, 13, 1926841. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Huang, E.; Gao, S. Type 1 Diabetes Mellitus and Cognitive Impairments: A Systematic Review. J. Alzheimer’s Dis. 2017, 57, 29–36. [Google Scholar] [CrossRef]
- Agashe, S.; Petak, S. Cardiac Autonomic Neuropathy in Diabetes Mellitus. Methodist Debakey Cardiovasc. J. 2018, 14, 251. [Google Scholar] [CrossRef] [PubMed]
- Silver, B.; Ramaiya, K.; Andrew, S.B.; Fredrick, O.; Bajaj, S.; Kalra, S.; Charlotte, B.M.; Claudine, K.; Makhoba, A. EADSG Guidelines: Insulin Therapy in Diabetes. Diabetes Ther. 2018, 9, 449–492. [Google Scholar] [CrossRef]
- Pathak, V.; Pathak, N.M.; O’Neill, C.L.; Guduric-Fuchs, J.; Medina, R.J. Therapies for Type 1 Diabetes: Current Scenario and Future Perspectives. Clin. Med. Insights Endocrinol. Diabetes 2019, 12, 1179551419844521. [Google Scholar] [CrossRef]
- Zimmermann, P.; Aberer, F.; Eckstein, M.L.; Haupt, S.; Erlmann, M.P.; Moser, O. Verapamil and Its Role in Diabetes. Diabetology 2022, 3, 393–406. [Google Scholar] [CrossRef]
- McGibbon, A.; Richardson, C.; Hernandez, C.; Dornan, J. Pharmacotherapy in Type 1 Diabetes. Can. J. Diabetes 2013, 37, S56–S60. [Google Scholar] [CrossRef]
- Deutsche Diabetes Gesellschaft. S3-Leitlinie Therapie Des Typ-1-Diabetes, 2nd ed.; 2018; Available online: www.awmf.org/leitlinien/detail/ll/057-013.html (accessed on 8 July 2023).
- Bjornstad, P.; Snell-Bergeon, J.K.; Nadeau, K.J.; Maahs, D.M. Insulin Sensitivity and Complications in Type 1 Diabetes: New Insights. World J. Diabetes 2015, 6, 8. [Google Scholar] [CrossRef]
- Purnell, J.Q.; John, E.H.; Cleary, P.A.; Nathan, D.M.; Lachin, J.M.; Zinman, B.; Brunzell, J.D. The Effect of Excess Weight Gain with Intensive Diabetes Mellitus Treatment on Cardiovascular Disease Risk Factors and Atherosclerosis in Type 1 Diabetes Mellitus: Results from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC) Study. Circulation 2013, 127, 180–187. [Google Scholar] [CrossRef]
- Hassanein, M.; Alamoudi, R.M.; Kallash, M.A.; Aljohani, N.J.; Alfadhli, E.M.; Tony, L.E.; Khogeer, G.S.; Alfadhly, A.F.; Khater, A.E.M.; Ahmedani, M.Y.; et al. Ramadan Fasting in People with Type 1 Diabetes during COVID-19 Pandemic: The DaR Global Survey. Diabetes Res. Clin. Pract. 2021, 172, 108626. [Google Scholar] [CrossRef]
- Al-Ozairi, E.; El Samad, A.; Al Kandari, J.; Aldibbiat, A.M. Intermittent Fasting Could Be Safely Achieved in People With Type 1 Diabetes Undergoing Structured Education and Advanced Glucose Monitoring. Front. Endocrinol. 2019, 10, 849. [Google Scholar]
- El-Hawary, A.; Salem, N.; Elsharkawy, A.; Metwali, A.; Wafa, A.; Chalaby, N.; El-Gilany, A.; Abo-Elmagd, M.; El-Ziny, M. Safety and Metabolic Impact of Ramadan Fasting in Children and Adolescents with Type 1 Diabetes. J. Pediatr. Endocrinol. Metab. 2016, 29, 533–541. [Google Scholar] [CrossRef]
- Salti, I.; Bénard, E.; Detournay, B.; Bianchi-Biscay, M.; Le Brigand, C.; Voinet, C.; Jabbar, A. A Population-Based Study of Diabetes and Its Characteristics during the Fasting Month of Ramadan in 13 Countries: Results of the Epidemiology of Diabetes and Ramadan 1422/2001 (EPIDIAR) Study. Diabetes Care 2004, 27, 2306–2311. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, K.; Al-Abdulrazzaq, D.; Fayed, A.; El Busairi, E.; Al Shawaf, F.; Abdul-Rasoul, M.; Shaltout, A.A. Fasting during the Holy Month of Ramadan among Older Children and Adolescents with Type 1 Diabetes in Kuwait. J. Pediatr. Endocrinol. Metab. 2019, 32, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Eckstein, M.L.; Mueller, A.; Tripolt, N.J.; Yildirim, H.; Abbas, F.; Pferschy, P.N.; Goswami, N.; Aberer, F.; Obermayer, A.; et al. Impact of a Single 36 Hours Prolonged Fasting Period in Adults With Type 1 Diabetes—A Cross-Over Controlled Trial. Front. Endocrinol. 2021, 12, 826. [Google Scholar]
- Afandi, B.; Kaplan, W.; Al Hassani, N.; Hadi, S.; Mohamed, A. Correlation between Pre-Ramadan Glycemic Control and Subsequent Glucose Fluctuation during Fasting in Adolescents with Type 1 Diabetes. J. Endocrinol. Investig. 2017, 40, 741–744. [Google Scholar] [CrossRef]
- Ibrahim, M.; Davies, M.J.; Ahmad, E.; Annabi, F.A.; Eckel, R.H.; Ba-Essa, E.M.; El Sayed, N.A.; Hess Fischl, A.; Houeiss, P.; Iraqi, H.; et al. Recommendations for Management of Diabetes during Ramadan: Update 2020, Applying the Principles of the ADA/EASD Consensus. BMJ Open Diabetes Res. Care 2020, 8, 1248. [Google Scholar] [CrossRef]
- Khan, R.M.M.; Chua, Z.J.Y.; Tan, J.C.; Yang, Y.; Liao, Z.; Zhao, Y. From Pre-Diabetes to Diabetes: Diagnosis, Treatments and Translational Research. Medicina 2019, 55, 546. [Google Scholar] [CrossRef]
- Association, A.D. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef]
- Abdul-Ghani, M.A.; Muller, F.L.; Liu, Y.; Chavez, A.O.; Balas, B.; Zuo, P.; Chang, Z.; Tripathy, D.; Jani, R.; Molina-Carrion, M.; et al. Deleterious Action of FA Metabolites on ATP Synthesis: Possible Link between Lipotoxicity, Mitochondrial Dysfunction, and Insulin Resistance. Am. J. Physiol. Endocrinol. Metab. 2008, 295, 678–685. [Google Scholar] [CrossRef]
- Carter, S.; Clifton, P.M.; Keogh, J.B. Effect of Intermittent Compared With Continuous Energy Restricted Diet on Glycemic Control in Patients With Type 2 Diabetes: A Randomized Noninferiority Trial. JAMA Netw. Open 2018, 1, e180756. [Google Scholar] [CrossRef] [PubMed]
- Lichtash, C.; Fung, J.; Ostoich, K.C.; Ramos, M. Therapeutic Use of Intermittent Fasting and Ketogenic Diet as an Alternative Treatment for Type 2 Diabetes in a Normal Weight Woman: A 14-Month Case Study. BMJ Case Rep. CP 2020, 13, e234223. [Google Scholar] [CrossRef]
- Hassanein, M.M.; Hanif, W.; Malek, R.; Jabbar, A. Changes in Fasting Patterns during Ramadan, and Associated Clinical Outcomes in Adults with Type 2 Diabetes: A Narrative Review of Epidemiological Studies over the Last 20 Years. Diabetes Res. Clin. Pract. 2021, 172, 108584. [Google Scholar] [CrossRef] [PubMed]
- Obermayer, A.; Tripolt, N.J.; Pferschy, P.N.; Kojzar, H.; Aziz, F.; Muller, A.; Schauer, M.; Oulhaj, A.; Aberer, F.; Sourij, C.; et al. Efficacy and Safety of Intermittent Fasting in People With Insulin-Treated Type 2 Diabetes (INTERFAST-2)—A Randomized Controlled Trial. Diabetes Care 2023, 46, 463. [Google Scholar] [CrossRef] [PubMed]
- Joaquim, L.; Faria, A.; Loureiro, H.; Matafome, P. Benefits, Mechanisms, and Risks of Intermittent Fasting in Metabolic Syndrome and Type 2 Diabetes. J. Physiol. Biochem. 2022, 78, 295–305. [Google Scholar] [CrossRef]
- Li, C.; Sadraie, B.; Steckhan, N.; Kessler, C.; Stange, R.; Jeitler, M.; Michalsen, A. Effects of A One-Week Fasting Therapy in Patients with Type-2 Diabetes Mellitus and Metabolic Syndrome—A Randomized Controlled Explorative Study. Exp. Clin. Endocrinol. Diabetes 2017, 125, 618–624. [Google Scholar]
- Corley, B.T.; Carroll, R.W.; Hall, R.M.; Weatherall, M.; Parry-Strong, A.; Krebs, J.D. Intermittent Fasting in Type 2 Diabetes Mellitus and the Risk of Hypoglycaemia: A Randomized Controlled Trial. Diabet. Med. 2018, 35, 588–594. [Google Scholar] [CrossRef]
- Van Den Burg, E.L.; Schoonakker, M.P.; Van Peet, P.G.; Van Den Akker-Van Marle, M.E.; Willems Van Dijk, K.; Willems Van Dijk, K.; Longo, V.D.; Longo, V.D.; Lamb, H.J.; Numans, M.E.; et al. Fasting in Diabetes Treatment (FIT) Trial: Study Protocol for a Randomised, Controlled, Assessor-Blinded Intervention Trial on the Effects of Intermittent Use of a Fasting-Mimicking Diet in Patients with Type 2 Diabetes. BMC Endocr. Disord. 2020, 20, 94. [Google Scholar] [CrossRef]
- Harris, K.B.; McCarty, D.J. Efficacy and Tolerability of Glucagon-like Peptide-1 Receptor Agonists in Patients with Type 2 Diabetes Mellitus. Ther. Adv. Endocrinol. Metab. 2015, 6, 3–18. [Google Scholar] [CrossRef]
- Cornell, S. A Review of GLP-1 Receptor Agonists in Type 2 Diabetes: A Focus on the Mechanism of Action of Once-Weekly Agents. J. Clin. Pharm. Ther. 2020, 45, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Uldal, S.; Clemmensen, K.K.B.; Persson, F.; Færch, K.; Quist, J.S. Is Time-Restricted Eating Safe in the Treatment of Type 2 Diabetes?—A Review of Intervention Studies. Nutrients 2022, 14, 2299. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Griffen, S.C.; Boulton, D.W.; Leil, T.A. Use of Systems Pharmacology Modeling to Elucidate the Operating Characteristics of SGLT1 and SGLT2 in Renal Glucose Reabsorption in Humans. Front. Pharmacol. 2014, 5, 274. [Google Scholar] [PubMed]
- Artasensi, A.; Pedretti, A.; Vistoli, G.; Fumagalli, L. Type 2 Diabetes Mellitus: A Review of Multi-Target Drugs. Molecules 2020, 25, 1987. [Google Scholar] [CrossRef]
- Scheen, A.J. Sodium–Glucose Cotransporter Type 2 Inhibitors for the Treatment of Type 2 Diabetes Mellitus. Nat. Rev. Endocrinol. 2020, 16, 556–577. [Google Scholar] [CrossRef]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.R.; Muscelli, E. Shift to Fatty Substrate Utilization in Response to Sodium–Glucose Cotransporter 2 Inhibition in Subjects Without Diabetes and Patients with Type 2 Diabetes. Diabetes 2016, 65, 1190–1195. [Google Scholar] [CrossRef]
- Lupsa, B.C.; Kibbey, R.G.; Inzucchi, S.E. Ketones: The Double-Edged Sword of SGLT2 Inhibitors? Diabetologia 2023, 66, 23–32. [Google Scholar]
- Ferrannini, E.; Mark, M.; Mayoux, E. CV Protection in the EMPA-REG OUTCOME Trial: A “Thrifty Substrate” Hypothesis. Diabetes Care 2016, 39, 1108–1114. [Google Scholar] [CrossRef]
- Selvaraj, S.; Kelly, D.P.; Margulies, K.B. Implications of Altered Ketone Metabolism and Therapeutic Ketosis in Heart Failure. Circulation 2020, 141, 1800–1812. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Muñoz-Hernández, L.; Márquez-López, Z.; Mehta, R.; Aguilar-Salinas, C.A. Intermittent Fasting as Part of the Management for T2DM: From Animal Models to Human Clinical Studies. Curr. Diab. Rep. 2020, 20, 13. [Google Scholar] [PubMed]
- Al-Arouj, M.; Assaad-Khalil, S.; Buse, J.; Fahdil, I.; Fahmy, M.; Hafez, S.; Hassanein, M.; Ibrahim, M.A.; Kendall, D.; Kishawi, S.; et al. Recommendations for Management of Diabetes During RamadanUpdate 2010. Diabetes Care 2010, 33, 1895–1902. [Google Scholar] [CrossRef]
- Wang, M.Y.; Chen, L.; Clark, G.O.; Lee, Y.; Stevens, R.D.; Ilkayeva, O.R.; Wenner, B.R.; Bain, J.R.; Charron, M.J.; Newgard, C.B.; et al. Leptin Therapy in Insulin-Deficient Type I Diabetes. Proc. Natl. Acad. Sci. USA 2010, 107, 4813–4819. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E.; Davis, S.N.; Shamoon, H. Hypoglycemia in Diabetes. Diabetes Care 2003, 26, 1902–1912. [Google Scholar] [CrossRef] [PubMed]
- Obermayer, A.; Tripolt, N.J.; Pferschy, P.N.; Kojzar, H.; Jacan, A.; Schauer, M.; Aziz, F.; Oulhaj, A.; Aberer, F.; Sourij, C.; et al. INTERmittent FASTing in People with Insulin-Treated Type 2 Diabetes Mellitus—The INTERFAST-2 Study Protocol. Diabetic Med. 2022, 39, e14813. [Google Scholar] [CrossRef] [PubMed]
- Elbarbary, N.S.; Ismail, E.A.R. Glycemic Control during Ramadan Fasting in Adolescents and Young Adults with Type 1 Diabetes on MiniMedTM 780G Advanced Hybrid Closed-loop System: A Randomized Controlled Trial. Diabetes Res. Clin. Pract. 2022, 191, 110045. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author and Year | Sample Size | Fasting Regime | Results |
|---|---|---|---|
| Al-Ozairi et al. (2019) [62] | n = 43 | RF | ↓ hypoglycemia |
| El-Hawary et al. (2016) [63] | n = 53 (children) | RF | ↓ fructosamine |
| ↑ TCH and LDL | |||
| ↓ HbA1c | |||
| Reiter et al. (2007) [8] | n = 43 | prolonged fasting (>25 h) | ↓ insulin dosage |
| ↑ HbA1c | |||
| Hassanein et al. (2020) [61] | n (<18 years) = 370 n = 279 (fasted) | RF | holistic reported hypoglycemia (60.7%) |
| n (>18 years) = 1113 n = 761 (fasted) | holistic reported hyperglycemia (44.8%) | ||
| Salti et al. (2004) [64] | n = 11,173 | RF | holistic reported hypoglycemia (0.14 episodes/Ramadan vs. 0.03 episodes/other months) |
| Mohamed et al. (2019) [65] | n = 50 | RF | Fasting on 20 ± 9.9 days in Ramadan (7.8% broke the fast due to mild hypoglycemia) |
| Berger et al. (2021) [9] | n = 20 (with T1DM) | 7-day fasting | ketoacidosis Ø |
| n = 10 (without disease) | blood glucose was stable (4.9 (±1.5) and 7.5 (±2.3) mmol/L) | ||
| ↑ quality of life | |||
| ↓ BMI | |||
| ↑ diastolic blood pressure 69.75 (±11.41) to 75.74 (±8.42) mmHg | |||
| Moser et al. (2021) [66] | n = 20 (with T1DM) | (a) overnight fasting—12 h fasting (b) prolonged fasting—36 h fasting | occurred hypoglycemia during the night period 12 h.: 0.07 ± 0.06 rate per hour vs. 36 h: 0.05 ± 0.03 rate per hour |
| fat oxidation 12 h: 90 ± 40 g/day vs. 36 h: 130 ± 35 g/day | |||
| carbohydrates oxidation 12 h: 305 ± 98 g/day vs. 36 h: 215 ± 63 g/day | |||
| Body weight 12 h: 76.7 ± 13.5 kg vs. 36 h: 75.4 ± 13.4 kg | |||
| BMI 12 h: 24.6 ± 2.8 kg/m2 vs. 36 h: 24.2 ± 2.8 kg/m2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herz, D.; Haupt, S.; Zimmer, R.T.; Wachsmuth, N.B.; Schierbauer, J.; Zimmermann, P.; Voit, T.; Thurm, U.; Khoramipour, K.; Rilstone, S.; et al. Efficacy of Fasting in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review. Nutrients 2023, 15, 3525. https://doi.org/10.3390/nu15163525
Herz D, Haupt S, Zimmer RT, Wachsmuth NB, Schierbauer J, Zimmermann P, Voit T, Thurm U, Khoramipour K, Rilstone S, et al. Efficacy of Fasting in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review. Nutrients. 2023; 15(16):3525. https://doi.org/10.3390/nu15163525
Chicago/Turabian StyleHerz, Daniel, Sandra Haupt, Rebecca Tanja Zimmer, Nadine Bianca Wachsmuth, Janis Schierbauer, Paul Zimmermann, Thomas Voit, Ulrike Thurm, Kayvan Khoramipour, Sian Rilstone, and et al. 2023. "Efficacy of Fasting in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review" Nutrients 15, no. 16: 3525. https://doi.org/10.3390/nu15163525
APA StyleHerz, D., Haupt, S., Zimmer, R. T., Wachsmuth, N. B., Schierbauer, J., Zimmermann, P., Voit, T., Thurm, U., Khoramipour, K., Rilstone, S., & Moser, O. (2023). Efficacy of Fasting in Type 1 and Type 2 Diabetes Mellitus: A Narrative Review. Nutrients, 15(16), 3525. https://doi.org/10.3390/nu15163525