

Vitamin D Intake and Serum Levels in Pregnant and Postpartum Women

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Blood Samples and Cut-Off Points for Vitamin D and PTH Levels
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. General Characteristics
3.2. Dietary Intake
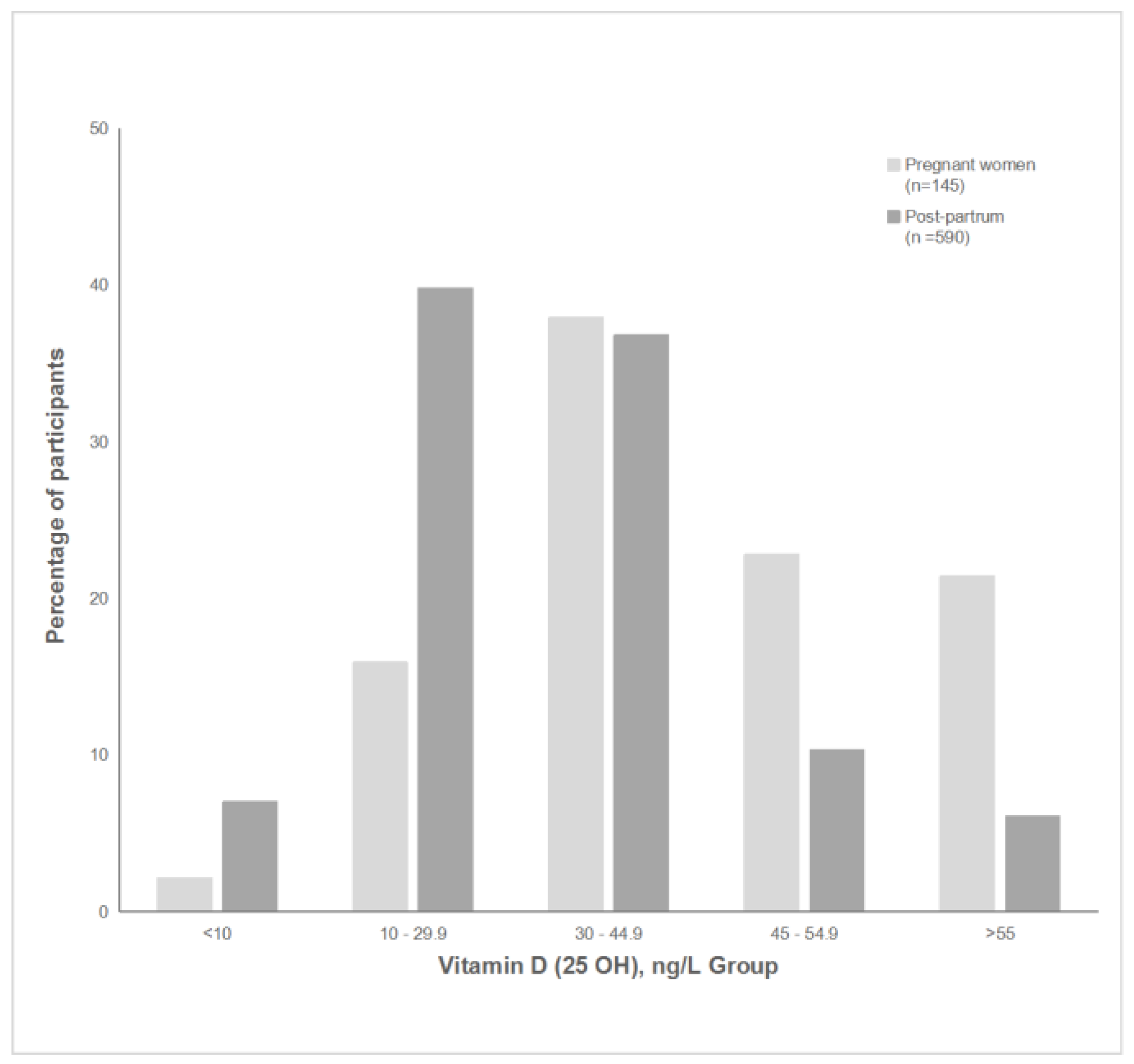
3.3. Serum Vitamin D and PTH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larqué, E.; Morales, E.; Leis, R.; Blanco-Carnero, J.E. Maternal and foetal health implications of vitamin D status during pregnancy. Ann. Nutr. Metab. 2018, 72, 179–192. [Google Scholar] [CrossRef]
- Wei, S.Q.; Qi, H.P.; Luo, Z.C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern.-Fetal Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef] [PubMed]
- Chrisostomo, K.R.; Junior, J.K.; Urbanetz, A.; Chrisostomo, E.R.; Nisihara, R.M. Current view of vitamin D in pregnant women: A review. Nascer Crescer-Birth Growth Med. J. 2019, 28, 77–83. [Google Scholar]
- Karras, S.N.; Fakhoury, H.; Muscogiuri, G.; Grant, W.B.; van den Ouweland, J.M.; Colao, A.M.; Kotsa, K. Maternal vitamin D levels during pregnancy and neonatal health: Evidence to date and clinical implications. Ther. Adv. Musculoskelet. Dis. 2016, 8, 124–135. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef]
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. Maternal vitamin D supplementation during pregnancy. Br. Med. Bull. 2018, 126, 57–77. [Google Scholar] [CrossRef]
- Ponsonby, A.L.; Lucas, R.M.; Lewis, S.; Halliday, J. Vitamin D status during pregnancy and aspects of offspring health. Nutrients 2010, 2, 389–407. [Google Scholar] [CrossRef]
- Looker, A.C.; Johnson, C.L.; Lacher, D.A.; Pfeiffer, C.M.; Schleicher, R.L.; Sempos, C.T. Vitamin D status: United States, 2001–2006. NCHS Data Brief. 2011, 59, 1–8. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Wagner, C.L.; Hollis, B.W. Early-life effects of vitamin D: A focus on pregnancy and lactation. Ann. Nutr. Metab. 2020, 76 (Suppl. 2), 16–28. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.L.; Hollis, B.W. The implications of vitamin D status during pregnancy on mother and her developing child. Front. Endocrinol. 2018, 9, 500. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic effects of vitamin D on human health and disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Ye, C.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B.; Retnakaran, R. The relationship between parathyroid hormone and 25-hydroxyvitamin D during and after pregnancy. J. Clin. Endocrinol. Metab. 2016, 101, 1729–1736. [Google Scholar] [CrossRef]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A.; et al. Guidelines for preventing and treating vitamin D deficiency: A 2023 update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef]
- Palacios, C.; De-Regil, L.M.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation during pregnancy: Updated meta-analysis on maternal outcomes. J. Steroid Biochem. Mol. Biol. 2016, 164, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; Van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Catov, J.M.; Roberts, J.M.; Simhan, H.N. Prepregnancy obesity predicts poor vitamin D status in mothers and their neonates. J. Nutr. 2007, 137, 2437–2442. [Google Scholar] [CrossRef] [PubMed]
- McAree, T.; Jacobs, B.; Manickavasagar, T.; Sivalokanathan, S.; Brennan, L.; Bassett, P.; Rainbow, S.; Blair, M. Vitamin D deficiency in pregnancy–still a public health issue. Matern. Child Nutr. 2013, 9, 23–30. [Google Scholar] [CrossRef]
- Karlsson, T.; Andersson, L.; Hussain, A.; Bosaeus, M.; Jansson, N.; Osmancevic, A.; Hulthén, L.; Holmäng, A.; Larsson, I. Lower vitamin D status in obese compared with normal-weight women despite higher vitamin D intake in early pregnancy. Clin. Nutr. 2015, 34, 892–898. [Google Scholar] [CrossRef]
- Wiciński, M.; Adamkiewicz, D.; Adamkiewicz, M.; Śniegocki, M.; Podhorecka, M.; Szychta, P.; Malinowski, B. Impact of vitamin D on physical efficiency and exercise performance—A review. Nutrients 2019, 11, 2826. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Maternal mineral and bone metabolism during pregnancy, lactation, and post-weaning recovery. Physiol. Rev. 2016, 96, 449–547. [Google Scholar] [CrossRef] [PubMed]
- Hysaj, O.; Marqués-Gallego, P.; Richard, A.; Elgizouli, M.; Nieters, A.; Quack Lötscher, K.C.; Rohrmann, S. Parathyroid hormone in pregnancy: Vitamin D and other determinants. Nutrients 2021, 13, 360. [Google Scholar] [CrossRef] [PubMed]
- Institute of Food Safety; Animal Health and Environment BIOR; Siksna, I.; Valciņa, O.; Ozoliņš, G.; Goldmanis, M. Latvian National Dietary Survey on the general population. EFSA Support. Publ. 2017, 14, 1307E. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Bärebring, L.; Bullarbo, M.; Glantz, A.; Hulthén, L.; Ellis, J.; Jagner, Å.; Schoenmakers, I.; Winkvist, A.; Augustin, H. Trajectory of vitamin D status during pregnancy in relation to neonatal birth size and fetal survival: A prospective cohort study. BMC Pregnancy Childbirth 2018, 18, 51. [Google Scholar] [CrossRef]
- Saraf, R.; Morton, S.M.; Camargo, C.A., Jr.; Grant, C.C. Global summary of maternal and newborn vitamin D status—A systematic review. Matern. Child Nutr. 2016, 12, 647–668. [Google Scholar] [CrossRef]
- Sinaci, S.; Ocal, D.F.; Yetiskin, D.F.Y.; Hendem, D.U.; Buyuk, G.N.; Ayhan, S.G.; Tanacan, A.; Ozgu-Erdinc, A.S.; Tekin, O.M.; Sahin, D. Impact of vitamin D on the course of COVID-19 during pregnancy: A case control study. J. Steroid Biochem. Mol. Biol. 2021, 213, 105964. [Google Scholar] [CrossRef]
- Ferrer-Sánchez, N.; Díaz-Goicoechea, M.; Mayoral-Cesar, V.; García-Solbas, S.; Nievas-Soriano, B.J.; Parrón-Carreño, T.; Fernández-Alonso, A.M. Serum 25 (OH) Vitamin D Levels in Pregnant Women with Coronavirus Disease 2019 (COVID-19): A Case-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 3965. [Google Scholar] [CrossRef]
- NHS. Vitamins, Supplements and Nutrition in Pregnancy. Available online: https://www.nhs.uk/pregnancy/keeping-well/vitamins-supplements-and-nutrition/ (accessed on 20 June 2023).
- Pérez-López, F.R.; Pilz, S.; Chedraui, P. Vitamin D supplementation during pregnancy: An overview. Curr. Opin. Obstet. Gynecol. 2020, 32, 316–321. [Google Scholar] [CrossRef]
- Aghajafari, F.; Field, C.J.; Kaplan, B.J.; Rabi, D.M.; Maggiore, J.A.; O’Beirne, M.; Hanley, D.A.; Eliasziw, M.; Dewey, D.; Weinberg, A.; et al. APrON Study Team. The current recommended vitamin D intake guideline for diet and supplements during pregnancy is not adequate to achieve vitamin D sufficiency for most pregnant women. PLoS ONE 2016, 11, e0157262. [Google Scholar] [CrossRef]
- Meija, L.; Rezeberga, D. Guidelines: Proper Maternal Nutrition during Pregnancy Planning and Pregnancy: A Healthy Start in Life Recommendations for Health Care Specialists-WHO-OMS; WHOOMS WHO: Geneva, Switzerland, 2017; pp. 1–31. [Google Scholar]
- World Health Organization. WHO Antenatal Care Recommendations for a Positive Pregnancy Experience: Nutritional Interventions Update: Vitamin D Supplements during Pregnancy; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hollis, B.W.; Johnson, D.; Hulsey, T.C.; Ebeling, M.; Wagner, C.L. Vitamin D supplementation during pregnancy: Double-blind, randomized clinical trial of safety and effectiveness. J. Bone Miner. Res. 2011, 26, 2341–2357. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Veugelers, P.J.; Pham, T.M.; Ekwaru, J.P. Optimal vitamin D supplementation doses that minimize the risk for both low and high serum 25-hydroxyvitamin D concentrations in the general population. Nutrients 2015, 7, 10189–10208. [Google Scholar] [CrossRef] [PubMed]
- Dalmar, A.; Raff, H.; Chauhan, S.P.; Singh, M.; Siddiqui, D.S. Serum 25-hydroxyvitamin D, calcium, and calcium-regulating hormones in preeclamptics and controls during first day postpartum. Endocrine 2015, 48, 287–292. [Google Scholar] [CrossRef]
- Santorelli, G.; Whitelaw, D.; Farrar, D.; West, J.; Lawlor, D.A. Associations of maternal vitamin D, PTH and calcium with hypertensive disorders of pregnancy and associated adverse perinatal outcomes: Findings from the Born in Bradford cohort study. Sci. Rep. 2019, 9, 1205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Pregnant | Postpartum | p | ||
|---|---|---|---|---|---|
| (n = 145) | (n = 590) | ||||
| n * | n * | ||||
| Age, years, Mnd (Q1 to Q3) | 142 | 31 (28 to 36) | 575 | 31 (28 to 35) | 0.370 |
| BMI before pregnancy **, kg/m2, Mnd (Q1 to Q3) | 138 | 21.6 (19.9 to 24.0) | 585 | 22.6 (20.7 to 25.6) | 0.001 |
| BMI group, n (%) | |||||
| <18.5 | 11 (8.0) | 28 (4.8) | 0.015 | ||
| 18.5–24.9 | 103 (74.6) | 388 (66.3) | |||
| 25.0–29.9 | 20 (14.5) | 114 (19.5) | |||
| ≥30 | 4 (2.9) | 55 (9.4) | |||
| Education level, n (%) | 143 | 585 | |||
| Primary or unfinished secondary | 3 (2.1) | 55 (9.4) | <0.001 | ||
| General secondary | 13 (9.1) | 129 (22.1) | |||
| Vocational secondary | 14 (9.8) | 57 (9.7) | |||
| Higher or unfinished higher | 113 (79.0) | 344 (58.8) | |||
| Marital status, n (%) | 144 | 590 | |||
| Married | 110 (76.4) | 376 (63.7) | 0.014 | ||
| Living in partnership | 33 (22.9) | 202 (34.2) | |||
| Single | 1 (0.7) | 12 (20.1) | |||
| Walking/cycling per day ***, n (%) | 144 | 586 | |||
| <15 min | 2 (1.4) | 29 (4.9) | 0.004 | ||
| 15–29 min | 28 (19.4) | 100 (17.1) | |||
| 30–60 min | 72 (50.0) | 215 (36.7) | |||
| ≥1 h | 42 (29.2) | 242 (41.3) | |||
| Number of births, n (%) | 95 | 588 | |||
| 1 | 48 (50.6) | 242 (41.2) | 0.230 | ||
| 2 | 31 (32.6) | 228 (38.8) | |||
| ≥3 | 16 (16.8) | 118 (20.0) | |||
| Time since previous delivery, years | 49 | 340 | |||
| <1 | 2 (4.0) | 4 (1.2) | 0.268 | ||
| 1–3 | 16 (32.7) | 102 (30.0) | |||
| >3 | 31 (63.3) | 234 (68.8) | |||
| Variable | Pregnant Women (n = 145) | Postpartum (n = 573) | p |
|---|---|---|---|
| Mnd (Q1 to Q3) | Mnd (Q1 to Q3) | ||
| Energy, kcal | 2338.5 (1788.9 to 2320.7) | 2320.7 (1770.9 to 3013.9) | 0.790 |
| Protein, g | 102.7 (78.6 to 142.6) | 103.7 (81.2 to 136.4) | 0.849 |
| Carbohydrates, g | 221.8 (168.6 to 280.5) | 220.6 (166.2 to 296.5) | 0.658 |
| Fat, g | 108.1 (77.6 to 137.2) | 107.7 (80.4 to 142.4) | 0.693 |
| Source | Pregnant Women (n = 145) | Postpartum (n = 573) | p | ||
|---|---|---|---|---|---|
| Used (n, %) | Mnd (Q1 to Q3) | Used (n, %) | Mnd (Q1 to Q3) | ||
| Food, mcg | 145 (100.0) | 2.5 (1.3 to 5.0) | 573 (100.0) | 2.0 (1.3 to 3.4) | 0.006 |
| Fish, mcg | 132 (91.0) | 1.33 (0.48 to 3.03) | 518 (90.4) | 0.85 (0.26 to 1.96) | <0.001 |
| Dairy products, mcg | 139 (98.6) | 0.21 (0.10 to 0.40) | 552 (96.3) | 0.29 (0.16 to 0.42) | 0.004 |
| Eggs, mcg | 143 (98.6) | 0.61 (0.29 to 1.05) | 566 (98.8 | 0.60 (0.30 to 0.94) | 0.148 |
| Mushrooms, mcg | 129 (89.0) | 0.04 (0.02 to 0.11) | 448 (78.2) | 0.02 (0.01 to 0.04) | <0.001 |
| Butter, mcg | 131 (90.3) | 0.02 (0.01 to 0.05) | 474 (82.7) | 0.04 (0.01 to 0.05) | 0.070 |
| All supplements, mcg | 136 (93.8) | 62.5 (18.5 to 112.5) | 480 (83.8) | 35.0 (12.5 to 72.5) | 0.107 |
| Vitamin D, mcg | 122 (84.1) | 62.5 (25.0 to 112.5) | 387 (67.5) | 62.5 (25.0 to 112.5) | 0.788 |
| Multivitamins, mcg | 76 (52.4) | 7.8 (5.0 to 10.0) | 282 (49.2) | 10.0 (5.0 to 10.0) | 0.011 |
| Food and supplements, mcg | 145 (100.0) | 63.5 (20.2 to 104.4) | 573 (100.0) | 28.2 (11.1 to 73.9) | 0.001 |
| Food g/Week | Pregnant Women (n = 145) | Postpartum (n = 573) | p | ||
|---|---|---|---|---|---|
| Used (n, %) | Mnd (Q1 to Q3) | Used (n, %) | Mnd (Q1 to Q3) | ||
| Fish | 132 (91.0) | 183.7 (93.2 to 344.6) | 518 (90.4) | 112.8 (50.6 to 237.2) | <0.001 |
| Dairy products | 139 (98.6) | 350.4 (235.8 to 539.9) | 552 (96.3) | 358.0 (235.4 to 529.6) | 0.682 |
| Eggs | 143 (98.6) | 211.7 (99.0 to 368.2) | 566 (98.8) | 209.4 (103.6 to 329.1) | 0.148 |
| Butter | 131 (90.3) | 2.5 (1.1 to 5.0) | 474 (82.7) | 3.9 (1.1 to 5.0) | 0.070 |
| Mushrooms | 129 (89.0) | 28.8 (11.5 to 74.8) | 448 (78.2) | 11.5 (5.8 to 28.8) | <0.001 |
| Status | PTH Concentration, pmol/L | BMI, kg/m2 | Education Level | Number of Births | Walking/ Cycling per Day | Sum of Vitamin D, mcg | Dietary Vitamin D, mcg | Supplement Vitamin D, mcg |
|---|---|---|---|---|---|---|---|---|
| Pregnant | −0.16 | −0.06 | −0.06 | −0.28 * | −0.08 | 0.38 * | −0.07 | 0.31 * |
| Postpartum | −0.21 * | −0.14 * | 0.20 | −0.17 * | −0.06 | 0.36 * | 0.02 | 0.15 * |
| ALL | −0.20 * | −0.17 * | 0.19 * | −0.19 * | −0.08 * | 0.38 * | 0.03 | 0.18 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meija, L.; Piskurjova, A.; Nikolajeva, K.; Aizbalte, O.; Rezgale, R.; Lejnieks, A.; Cauce, V. Vitamin D Intake and Serum Levels in Pregnant and Postpartum Women. Nutrients 2023, 15, 3493. https://doi.org/10.3390/nu15153493
Meija L, Piskurjova A, Nikolajeva K, Aizbalte O, Rezgale R, Lejnieks A, Cauce V. Vitamin D Intake and Serum Levels in Pregnant and Postpartum Women. Nutrients. 2023; 15(15):3493. https://doi.org/10.3390/nu15153493
Chicago/Turabian StyleMeija, Laila, Anna Piskurjova, Ksenija Nikolajeva, Olga Aizbalte, Roberta Rezgale, Aivars Lejnieks, and Vinita Cauce. 2023. "Vitamin D Intake and Serum Levels in Pregnant and Postpartum Women" Nutrients 15, no. 15: 3493. https://doi.org/10.3390/nu15153493
APA StyleMeija, L., Piskurjova, A., Nikolajeva, K., Aizbalte, O., Rezgale, R., Lejnieks, A., & Cauce, V. (2023). Vitamin D Intake and Serum Levels in Pregnant and Postpartum Women. Nutrients, 15(15), 3493. https://doi.org/10.3390/nu15153493