

Benefits of the Light Consumption of Red Wine in Pain, Tender Points, and Anxiety in Women with Fibromyalgia: A Pilot Study
 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection and Outcome Measures
2.4. Interventions
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Statistical Classification of Diseases and Related Health Problems 10th Revision, Version for 2007. Chapter XIII. Disease of the Musculoskeletal System and Connective Tissue (M00-M99). Soft Tissue Disorder (M60-M79). Fibromyalgia (M79.7). Available online: http://apps.who.int/classifications/apps/icd/icd10online/ (accessed on 3 February 2021).
- Velasco, M. Dolor musculo-esquelético: Fibromialgia y dolor miofascial. Rev. Med. Clin. Condes 2019, 30, 414–427. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Arthritis Rheum. 1990, 33, 150–172. [Google Scholar] [CrossRef]
- Goldenberg, D.L.; Burckhardt, C.; Crofford, L. Management of Fibromyalgia Syndrome. JAMA 2004, 292, 2388–2395. [Google Scholar] [CrossRef] [PubMed]
- Cabo, A.; Cerdá, G.; Trillo, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Assumpção, A.; Cavalcante, A.B.; Capela, C.E.; Sauer, J.F.; Chalot, S.D.; Pereira, C.A.B.; Marques, A.P. Prevalence of fibromyalgia in lowsocioeconomic status population. BMC Musculoskelet. Disord. 2009, 10, 64. [Google Scholar] [CrossRef]
- Rivera, J.; Alegre, C.; Ballina, F.; Carbonell, J.; Carmona, L.; Castel, B.; Collado, A.; Esteve, J.; Martínez, F.; Tornero, J.; et al. Documento de consenso de la Sociedad Española de Reumatología sobre la fibromialgia. Reumatol. Clin. 2006, 2, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Staud, R.; Spaeth, M. Psychophysical and Neurochemical Abnormalities of Pain Processing in Fibromyalgia. CNS Spectr. 2008, 13, 12–17. [Google Scholar] [CrossRef]
- Arnold, L.M.; Bradley, L.A.; Clauw, D.J.; Glass, J.; Goldenberg, D. Multidisciplinary care and stepwise treatment for fibromyalgia. J. Clin. Psychiatry 2009, 69, e35. [Google Scholar] [CrossRef] [PubMed]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Webber, S.C.; Musselman, K.E.; Overend, T.J.; Góes, S.M.; Bello-Haas, V.D.; Boden, C. Mixed exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2019, 5, CD013340. [Google Scholar] [CrossRef]
- Ley 24/2003, de 10 de Julio, de la Viña y el Vino. BOE Núm. 165. 2003. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2003-13864 (accessed on 1 February 2021).
- Fundación Dieta Mediterránea. Iº Congreso Internacional Sobre la Dieta Mediterránea. 1993. Available online: https://www.observatorio-acuicultura.es/comunicacion/agenda/ix-congreso-internacional-de-barcelona-sobre-la-dieta-mediterranea (accessed on 1 February 2011).
- Oser, M.L.; McKellar, J.; Moos, B.S.; Moos, R.H. Changes in Ambivalence Mediate the Relation between Entering Treatment and Change in Alcohol Use and Problems. Addict. Behav. 2010, 35, 367–369. [Google Scholar] [CrossRef]
- Bertholet, N.; Horton, N.J.; Saitz, R. Improvements in Readiness to Change and Drinking in Primary Care Patients with Unhealthy Alcohol Use: A Prospective Study. BMC Public Health 2009, 9, 101. [Google Scholar] [CrossRef]
- Wilkowska, A.; Czyżowska, A.; Ambroziak, W.; Adamiec, J. Structural, physicochemical and biological properties of spray-dried wine powders. Food Chem. 2017, 228, 77–84. [Google Scholar] [CrossRef]
- Lagha, A.; Andrian, E.; Grenier, D. Resveratrol attenuates the pathogenic and inflammatory properties of Porphyromonas gingivalis. Mol. Oral Microbiol. 2019, 34, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, J. Tratado de Enología; Ed. Mundi-Prensa: Madrid, Spain, 2003. [Google Scholar]
- Booyse, F.M.; Parks, D.A. Moderate wine and alcohol consumption: Beneficial effects on cardiovascular disease. Thromb. Haemost. 2001, 86, 517–528. [Google Scholar]
- Senault, C.; Betoulle, D.; Luc, G.; Hauw, P.; Rigaud, D.; Fumeron, F. Beneficial effects of a moderate consumption of red wine on cellular cholesterol efflux in young men. Nutr. Metab. Cardiovasc. Dis. 2000, 10, 63–69. [Google Scholar]
- Binkiewicz-Glińska, A.; Bakuła, S.; Tomczak, H.; Landowski, J.; Ruckemann-Dziurdzińska, K.; Zaborowska-Sapeta, K.; Kowalski, I.; Kiebzak, W. Fibromyalgia Syndrome—A multidisciplinary approach. Psychiatr. Pol. 2015, 49, 801–810. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Lippi, G.; Franchini, M.; Favaloro, E.J.; Targher, G. Moderate red wine consumption and cardiovascular disease risk: Beyond the “French paradox”. Semin. Thromb. Hemost. 2010, 36, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Brien, S.E.; Ronksley, P.E.; Turner, B.J.; Mukamal, K.J.; Ghali, W.A. Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: Systematic review and meta-analysis of interventional studies. BMJ 2011, 342, d636. [Google Scholar] [CrossRef]
- Gong, P.-Y.; Tian, Y.-S.; Guo, Y.-J.; Gu, L.-F.; Li, J.-Y.; Qi, J.; Yu, B.-Y. Comparisons of antithrombosis, hematopoietic effects and chemical profiles of dried and rice wine-processed Rehmanniae Radix extracts. J. Ethnopharmacol. 2019, 231, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Csiszar, A.; Labinskyy, N.; Pinto, J.T.; Ballabh, P.; Zhang, H.; Losonczy, G.; Pearson, K.; de Cabo, R.; Pacher, P.; Zhang, C.; et al. Resveratrol Induces Mitochondrial Biogenesis in Endothelial Cells. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.M.; Hsieh, T.C. Resveratrol: A cardioprotective substance. Ann. N. Y. Acad. Sci. 2011, 1215, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Pedrera, J.D.; Lavado, J.M.; Roncero, R.; Calderón, J.; Rodriguez, T.; Canal, M. Effect of Beer Drinking on Ultrasound Bone Mass in Women. Nutritio 2009, 25, 1057–1063. [Google Scholar] [CrossRef]
- Silva, T.R.; Martins, C.; Ferreira, L.L.; Spritzer, P.M. Mediterranean diet is associated with bone mineral density and muscle mass in postmenopausal women. Climacteric 2019, 22, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Sacanella, E.; Vázquez-Agell, M.; Mena, M.P.; Antúnez, E.; Fernández-Solá, J.; Nicolás, J.M.; Lamuela-Raventós, R.M.; Ros, E.; Estruch, R. Down-regulation of adhesion molecules and other inflammatory biomarkers alter moderate wine consumption in healthy women: A randomized trial. Am. J. Clin. Nutr. 2007, 86, 1463–1469. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, J.J.; Lin, J.W.; Shuo, W.; Hua, G. Anti-inflammatory and analgesic effects of ethanol and aqueous extracts of Pterocephalus hookeri (C.B. Clarke) Höeck. J. Ethnopharmacol. 2009, 123, 510–514. [Google Scholar] [CrossRef]
- Sales, C.; Oliviero, F.; Spinella, P. The Mediterranean diet model in inflammatory rheumatic diseases. Rheumatism 2009, 61, 10–14. [Google Scholar] [CrossRef][Green Version]
- Pattichis, K.; Louca, L.L.; Jarman, J.; Sandler, M.; Glover, V. 5-Hydroxytryptamine release from platelets by different red wines: Implications for migraine. Eur. J. Pharmacol. 1995, 292, 173–177. [Google Scholar] [CrossRef]
- Gomez, H.A.G.; Marques, M.O.M.; Borges, C.V.; Minatel, I.O.; Monteiro, G.C.; Ritschel, P.S.; Zanus, M.C.; Diamante, M.S.; Kluge, R.A.; Lima, G.P.P. Biogenic Amines and the Antioxidant Capacity of Juice and Wine from Brazilian Hybrid Grapevines. Plant Foods Hum. Nutr. 2020, 75, 258–264. [Google Scholar] [CrossRef]
- Welsch, P.; Üçeyler, N.; Klose, P.; Walitt, B.; Häuser, W. Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia. Cochrane Database Syst. Rev. 2018, 2, CD010292. [Google Scholar] [CrossRef]
- Paredes, S.; Cantillo, S.; Candido, K.D.; Knezevic, N.N. An Association of Serotonin with Pain Disorders and Its Modulation by Estrogens. Int. J. Mol. Sci. 2019, 20, 5729. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Rubio-Arias, J.Á.; Ramos-Campo, D.J.; Reche-García, C.; Leyva-Vela, B.; Nadal-Nicolás, Y. Psychological and Sleep Effects of Tryptophan and Magnesium-Enriched Mediterranean Diet in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 22–27. [Google Scholar] [CrossRef]
- Rezende, R.M.; Pelúzio, M.D.C.G.; Silva, F.d.J.; Della Lucia, E.M.; Favarato, L.S.C.; Martino, H.S.D.; Natali, A.J. Does aerobic exercise associated with tryptophan supplementation attenuates hyperalgesia and inflammation in female rats with experimental fibromyalgia? PLoS ONE 2019, 14, e0211824. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Li, W.; Li, Y.; Xu, W.; Yuan, Y.; Zheng, V.; Zhang, H.-T.; O’Donnell, J.M.; Xu, Y.; Yin, X. The antidepressant- and anxiolytic-like effects of resveratrol: Involvement of phosphodiesterase-4D inhibition. Neuropharmacology 2019, 153, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Human, D. Declaration of Helsinki. Lancet 2001, 357, 236. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Ramos, J.A.; Cordero, A. Validación de la versión castellana de la escala de Hamilton para la depresión. Actas Luso-Esp. Neurol. Psiquiatr. 1986, 14, 324–334. [Google Scholar]
- Carrobles, J.A.; Costa, M.; Del Ser, T.; Bartolomé, P. La Práctica de la Terapia de Conducta; Promolibro: Valencia, Spain, 1986. [Google Scholar]
- Rivera, J.; González, T. The Fibromyalgia Impact Questionnaire: A Validated Spanish Version to Assess the Health Status in Women with Fibromyalgia. Clin. Exp. Rheumatol. 2004, 22, 554–560. [Google Scholar]
- Ribera del Guadiana. Available online: http://www.riberadelguadiana.eu/ (accessed on 5 June 2021).
- World Medical Association. Available online: http://www.who.int/en/ (accessed on 2 February 2021).
- USDA National Nutrient Database for Standard Reference. Department of Agriculture, Agricultural Research Service. 2006. Available online: http://www.ars.usda.gov/ba/bhnrc/ndl (accessed on 15 January 2020).
- Pita, S. Metodología de la Investigación. Available online: http://www.fisterra.com/mbe/investiga/index.asp (accessed on 15 January 2021).
- Panconesi, A. Alcohol and migraine: Trigger factor, consumption, mechanisms. A review. J. Headache Pain 2008, 9, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Beidler, J.; Young, M. Resveratrol and Depression in Animal Models: A Systematic Review of the Biological Mechanisms. Molecule 2018, 23, 2197. [Google Scholar] [CrossRef]
- Song, Y.; Shan, B.; Zeng, S.; Zhang, J.; Jin, C.; Liao, Z.; Wang, T.; Zeng, Q.; He, H.; Wei, F.; et al. Raw and wine processed Schisandra chinensis attenuate anxiety like behavior via modulating gut microbiota and lipid metabolism pathway. J. Ethnopharmacol. 2021, 266, 113426. [Google Scholar] [CrossRef] [PubMed]
- Nickel, R.; Hardt, J.; Kappis, B.; Schwab, R.; Egle, U.T. Somatoform Disorders with Pain as the Predominant Symptom: Results to Distinguish a Common Group of Diseases. Schmerz 2009, 23, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Guallar, P.; Rodríguez, F.; Díez, L.D.; Banegas, J.R.; Lafuente, P.L.; Herruzo, R.H. Consumption of Alcoholic Beverages and Subjective Health in Spain. J. Epidemiol. Community Health 2001, 55, 648–652. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Smith, K.A.; Fairburn, C.G.; Cowen, P.J. Relapse of Depression after Rapid Depletion of Tryptophan. Lancet 1997, 349, 915–919. [Google Scholar] [CrossRef]
- Bennett, R. The Fibromyalgia Impact Questionnaire (FIQ): A Review of its Development, Current Version, Operating Characteristics and Uses. Clin. Exp. Rheumatol. 2005, 23, S154–S162. [Google Scholar]
- Guerrero, R.F.; García-Parrilla, M.C.; Puertas, B.; Cantos-Villar, E. Wine, resveratrol and health: A review. Nat. Prod. Commun. 2009, 4, 635–658. [Google Scholar] [CrossRef]
- Boban, M.; Stockley, C.; Teissedre, P.-L.; Restani, P.; Fradera, U.; Stein-Hammer, C.; Ruf, J.-C. Drinking pattern of wine and effects on human health: Why should we drink moderately and with meals. Food Funct. 2016, 7, 2937–2942. [Google Scholar] [CrossRef]
- Vecchio, R.; Decordi, G.; Grésillon, L.; Gugenberger, C.; Mahéo, M.; Jourjon, F. European consumer’s perception of moderate wine consumption on health. Wine Econ. Policy 2017, 6, 14–22. [Google Scholar] [CrossRef]
- Gronbaek, M.; Deis, A.; Sorensen, T.I.A.; Becker, U.; Borch-Johnsen, K.; Muller, C.; Schnohr, P.; Jensen, G. Influence of sex, age, body mass index, and smoking on alcohol intake and mortality. BMJ 1994, 308, 302–306. [Google Scholar] [CrossRef]
- Zaldívar, E.; García, A.T.P.; López, E.; Crespo, I.; del Pueyo, I. Vino ecológico, un beneficio probado en tu salud. Sem. Vitivinícola 2012, 3373, 454–464. [Google Scholar]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Guillén, M.; Lamuela-Raventós, R.M.; Llorach, R.; Andres-Lacueva, C.; et al. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, R.; Miranda, A.; Vergara, L. Modulation of endogenous antioxidant system by wine polyphenols in human disease. Clin. Chim. Acta 2011, 412, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Córdova, A.C.; Sumpio, B.J.; Sumpio, B.E. Perfecting the plate: Adding cardioprotective compounds to the diet. J. Am. Coll. Surg. 2012, 214, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Córdova, A.C.; Jackson, L.S.; Berke-Schlessel, D.W.; Sumpio, B.E. The cardiovascular protective effect of red wine. J. Am. Coll. Surg. 2005, 200, 428–439. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (N = 20) | Wine (N = 27) | Inter-Group Difference | Interaction | ||
|---|---|---|---|---|---|
| A: Pain (0–10) | VAS before | 6.50 ± 1.54 | 6.89 ± 1.22 | p = 0.557 b | p = 0.016 a |
| VAS after | 6.89 ± 1.49 | 5.89 ± 1.99 | p = 0.054 b | ||
| Intra-group difference | p = 0.390 c | p = 0.008 c | -- | ||
| B: Sensitive points (0–18) | # before | 14.83 ± 3.43 | 15.85 ± 3.23 | p = 0.427 b | p = 0.007 a |
| # after | 14.76 ± 3.51 | 12.22 ± 4.12 | p = 0.031 b | ||
| Intra-group difference | p = 0.977 c | p < 0.001 c | -- | ||
| C: Sadness (0–10) | VAS before | 5.56 ± 2.48 | 4.63 ± 2.42 | p = 0.971 b | p = 0.018 a |
| VAS after | 5.61 ± 2.73 | 3.78 ± 2.78 | p = 0.065 b | ||
| Intra-group difference | p = 0.106 c | p = 0.052 c | -- | ||
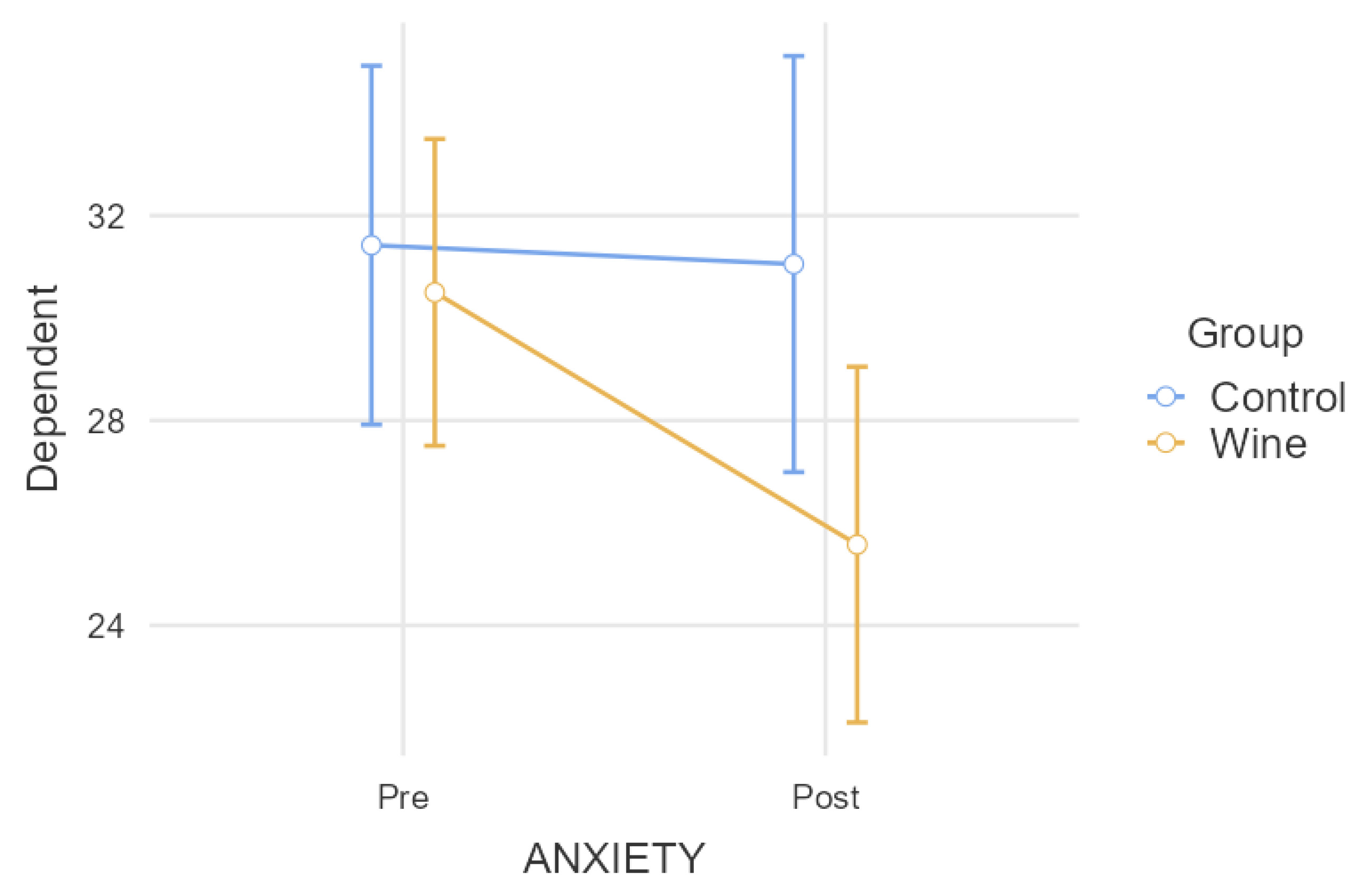
| D: Anxiety (0–56) | HAS before | 31.42 ± 8.05 | 30.59 ± 7.08 | p = 0.672 b | p = 0.078 a |
| HAS after | 31.05 ± 9.16 | 25.58 ± 8.49 | p = 0.038 b | ||
| Intra-group difference | p = 0.957 c | p = 0.006 c | -- | ||
| E: Depression (0–52) | HDRS before | 18.95 ± 4.42 | 18.63 ± 5.08 | p = 0.144 b | p = 0.737 a |
| HDRS after | 20.17 ± 4.38 | 16.62 ± 4.50 | p = 0.166 b | ||
| Intra-group difference | p = 0.775 c | p = 0.112 c | |||
| FM impact (0–100) | FIQ before | 60.84 ± 16.80 | 59.56 ± 14.10 | p = 0.851 b | p = 0.202 a |
| FIQ after | 60.76 ± 12.72 | 53.48 ± 11.62 | p = 0.058 b | ||
| Intra-group difference | p = 0.939 c | p = 0.053 c | |||
| Control (N = 20) | Wine (N = 27) | Inter-Group Difference | ||
|---|---|---|---|---|
| A: Analgesic | % before | 55.0 | 77.8 | p = 0.098 b |
| % follow-up | 60.0 | 70.4 | p = 0.458 b | |
| Intra-group difference | p = 0.317 a | p = 0.317 a | -- | |
| B: Anti-inflammatory | % before | 65.0 | 55.6 | p = 0.514 b |
| % follow-up | 65.0 | 51.9 | p = 0.367 b | |
| Intra-group difference | p = 1 a | p = 0.705 a | -- | |
| C: SSRI | % before | 85.0 | 40.7 | p = 0.002 b |
| % follow-up | 85.0 | 37.0 | p = 0.001 b | |
| Intra-group difference | p = 1 a | p = 0.317 a | -- | |
| D: Benzodiazepine | % before | 55.0 | 3.7 | p < 0.001 b |
| % follow-up | 50.0 | 0 | p < 0.001 b | |
| Intra-group difference | p = 0.317 a | -- | -- | |
| E: Tricylic antidepressant | % before | 10.0 | 40.7 | p = 0.020 b |
| % follow-up | 5.0 | 37.0 | p = 0.010 b | |
| Intra-group difference | p = 0.317 a | p = 0.564 a | -- | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López-Arza, M.V.; Triviño-Palomo, J.V.; Montanero-Fernández, J.; Garrido-Ardila, E.M.; González-Sánchez, B.; Jiménez-Palomares, M.; Rodríguez-Mansilla, J. Benefits of the Light Consumption of Red Wine in Pain, Tender Points, and Anxiety in Women with Fibromyalgia: A Pilot Study. Nutrients 2023, 15, 3469. https://doi.org/10.3390/nu15153469
González-López-Arza MV, Triviño-Palomo JV, Montanero-Fernández J, Garrido-Ardila EM, González-Sánchez B, Jiménez-Palomares M, Rodríguez-Mansilla J. Benefits of the Light Consumption of Red Wine in Pain, Tender Points, and Anxiety in Women with Fibromyalgia: A Pilot Study. Nutrients. 2023; 15(15):3469. https://doi.org/10.3390/nu15153469
Chicago/Turabian StyleGonzález-López-Arza, María Victoria, José Vicente Triviño-Palomo, Jesús Montanero-Fernández, Elisa María Garrido-Ardila, Blanca González-Sánchez, María Jiménez-Palomares, and Juan Rodríguez-Mansilla. 2023. "Benefits of the Light Consumption of Red Wine in Pain, Tender Points, and Anxiety in Women with Fibromyalgia: A Pilot Study" Nutrients 15, no. 15: 3469. https://doi.org/10.3390/nu15153469
APA StyleGonzález-López-Arza, M. V., Triviño-Palomo, J. V., Montanero-Fernández, J., Garrido-Ardila, E. M., González-Sánchez, B., Jiménez-Palomares, M., & Rodríguez-Mansilla, J. (2023). Benefits of the Light Consumption of Red Wine in Pain, Tender Points, and Anxiety in Women with Fibromyalgia: A Pilot Study. Nutrients, 15(15), 3469. https://doi.org/10.3390/nu15153469