
A Retrospective Chart Review and Infant Feeding Survey in the Irish Phenylketonuria (PKU) Population (2016–2020)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.1.1. Retrospective Chart Review
2.1.2. Parental Survey
2.2. Statistical Analysis
3. Results
3.1. Retrospective Chart Review
3.1.1. Demographic
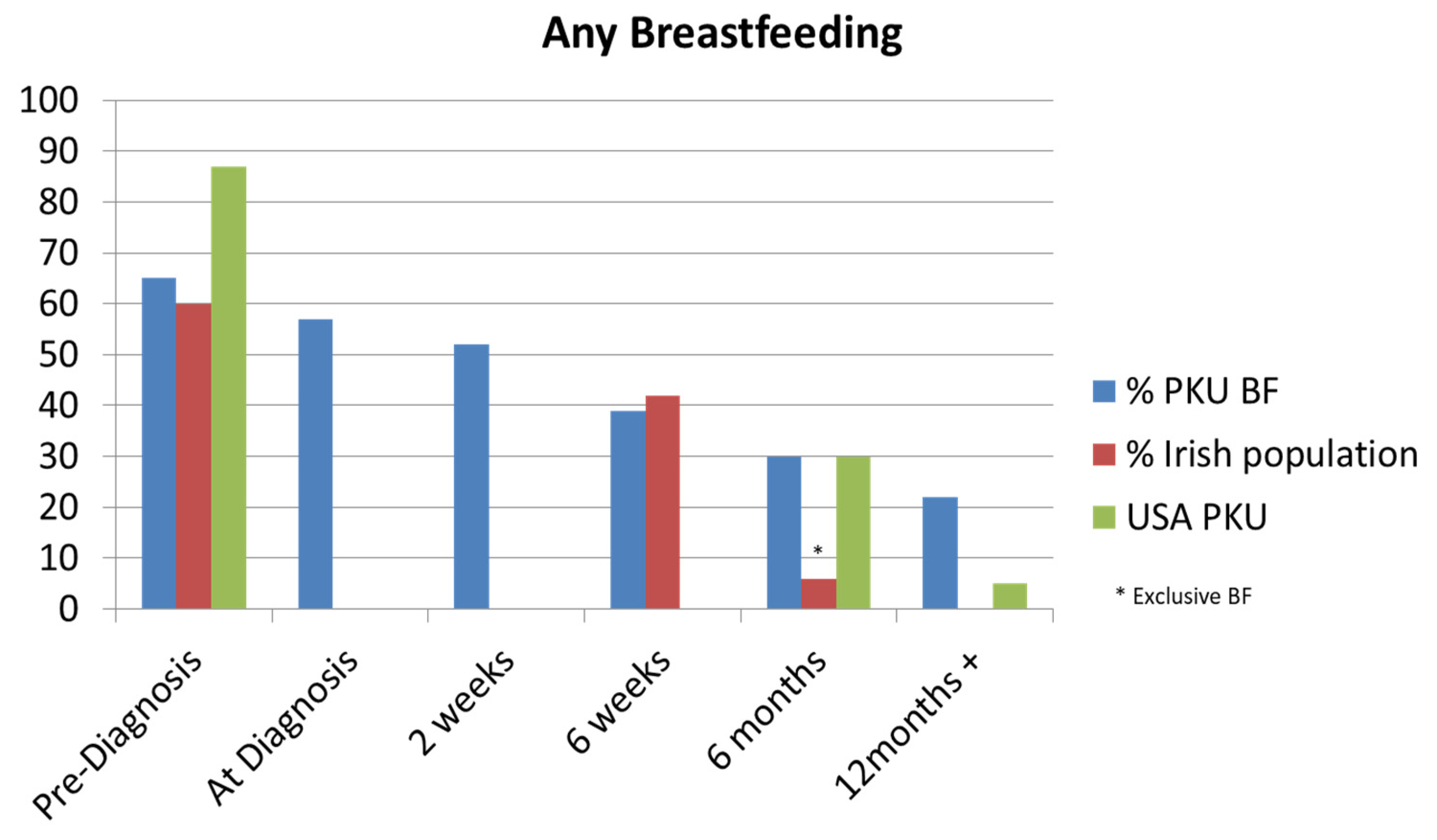
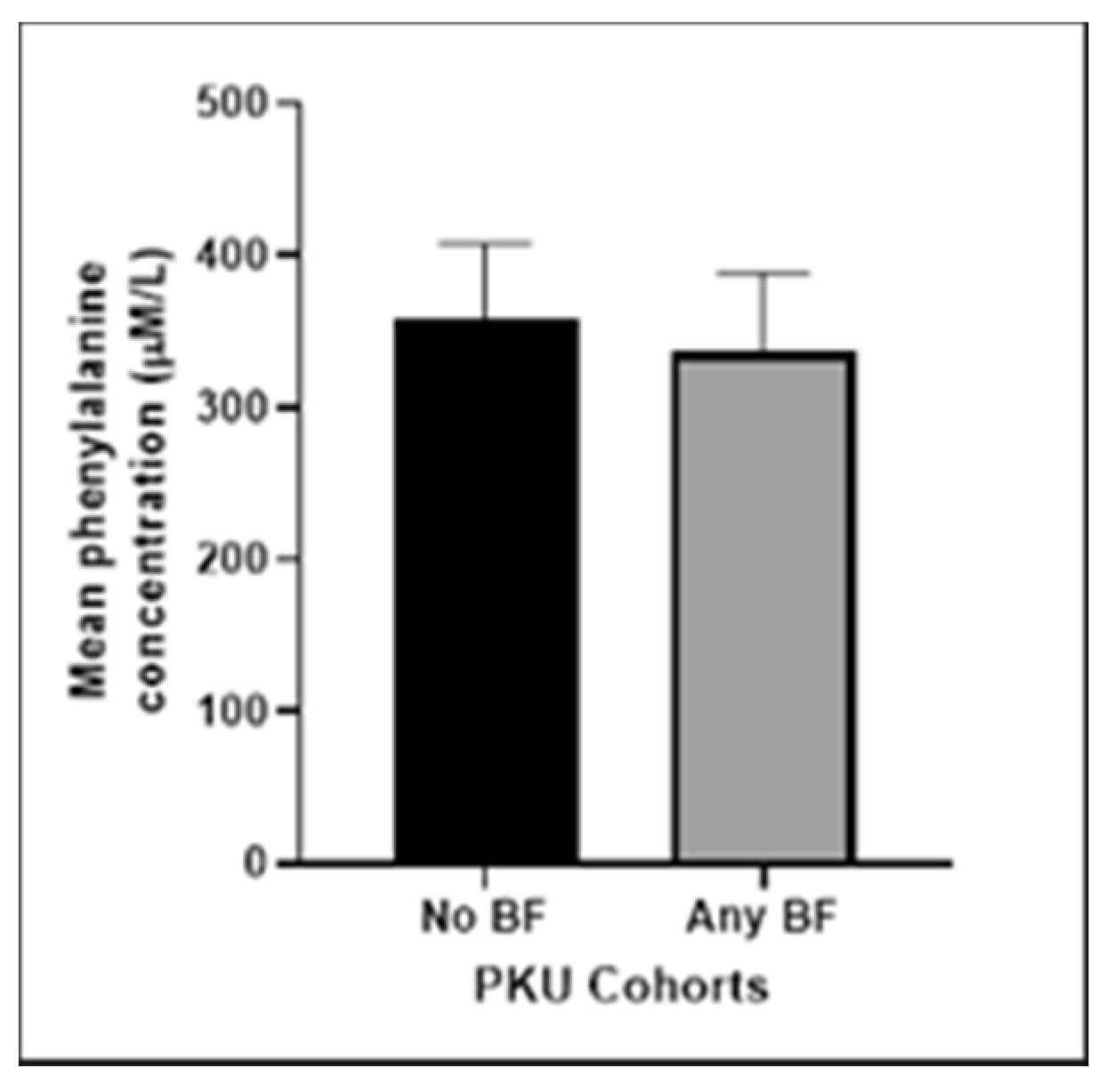
3.1.2. Feeding Method
3.1.3. Complementary Feeding
3.2. Parental Survey Results
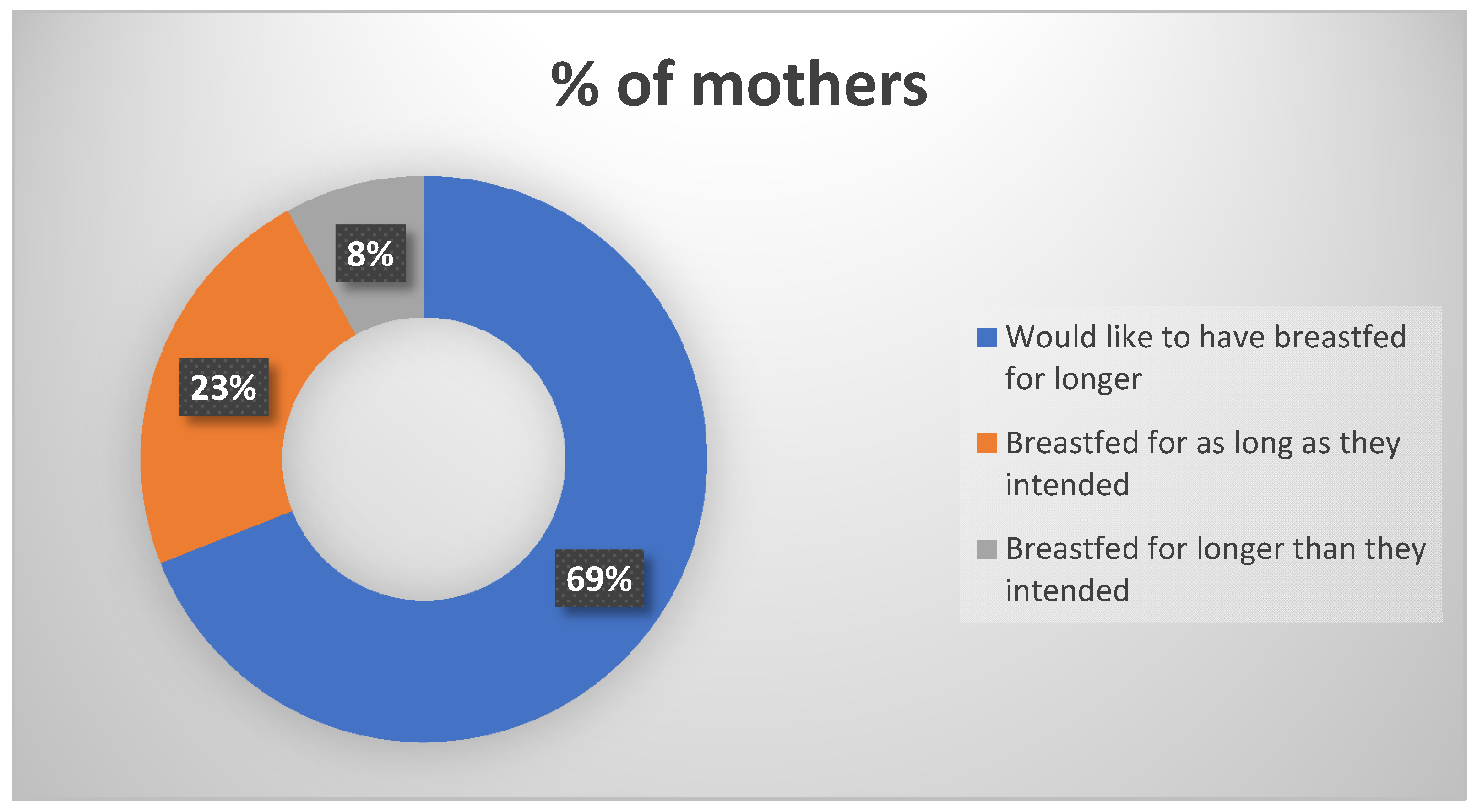
3.2.1. Breastfeeding Responses
3.2.2. Complementary Feeding Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elhawary, N.A.; AlJahdali, I.A.; Abumansour, I.S.; Elhawary, E.N.; Gaboon, N.; Dandini, M.; Madkhali, A.; Alosaimi, W.; Alzahrani, A.; Aljohani, F.; et al. Genetic etiology and clinical challenges of phenylketonuria. Hum. Genom. 2022, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- Ashe, K.; Kelso, W.; Farrand, S.; Panetta, J.; Fazio, T.; De Jong, G.; Walterfang, M. Psychiatric and Cognitive Aspects of Phenylketonuria: The Limitations of Diet and Promise of New Treatments. Front. Psychiatry 2019, 10, 561. [Google Scholar] [CrossRef] [PubMed]
- HSE. Available online: https://www.hse.ie/eng/health/child/newbornscreening/newbornbloodspotscreening/information-for-professionals/a-practical-guide-to-newborn-bloodspot-screening-in-ireland.pdf (accessed on 2 December 2022).
- Van Wegberg, A.M.J.; Macdonald, A.; Ahring, K.; BéLanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on Phenylketonuria: Diagnosis and treatment. Orphanet. J. Rare Dis. 2017, 12, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grummer-Strawn, L.M.; Rollins, N. Summarising the health effects of breastfeeding. Acta Paediatr. 2015, 104, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rijn, M.; Bekhof, J.; Dijkstra, T.; Smit, P.G.P.A.; Moddermam, P.; van Spronsen, F.J. A different approach to breast-feeding of the infant with phenylketonuria. Eur. J. Pediatr. 2003, 163, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Zuvadelli, J.; Paci, S.; Salvatici, E.; Giorgetti, F.; Cefalo, G.; Dionigi, A.R.; Rovelli, V.; Banderali, G. Breastfeeding in Phenylketonuria: Changing Modalities, Changing Perspectives. Nutrients 2022, 14, 4138. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Bélanger-Quintana, A.; Burlina, A.; Campistol, J.; Coşkun, T.; Feillet, F.; Giżewska, M.; et al. PKU dietary handbook to accompany PKU guidelines. Orphanet J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- Healthcare Pricing Office. Available online: https://www.hpo.ie/latest_hipe_nprs_reports/NPRS_2019/Perinatal_Statistics_Report_2019.pdf (accessed on 13 June 2023).
- HSE. Available online: https://www.hse.ie/eng/services/publications/performancereports/management-data-report-june-2020.pdf (accessed on 13 June 2023).
- Layte, R.; McCrory, C. Growing Up in Ireland: Maternal Health Behaviours and Child Growth in Infancy, Dublin: Stationery Office/Department of Children and Youth Affairs. 2015. Available online: https://www.esri.ie/publications/growing-up-in-ireland-maternal-health-behaviours-and-child-growth-in-infancy (accessed on 26 January 2019).
- Banta-Wright, S.A.; Shelton, K.C.; Lowe, N.D.; Knafl, K.A.; Houck, G.M. Breast-feeding Success Among Infants with Phenylketonuria. J. Pediatr. Nurs. 2011, 27, 319–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banta-Wright, S.A.; Press, N.; Knafl, K.A.; Steiner, R.D.; Houck, G.M. Breastfeeding Infants with Phenylketonuria in the United States and Canada. Breastfeed. Med. 2014, 9, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, A.; Adams, S.; Ahring, K.; Allen, H.; Almeida, M.; Garcia-Arenas, D.; Arslan, N.; Assoun, M.; Altınok, Y.A.; Barrio-Carreras, D.; et al. Early feeding practices in infants with phenylketonuria across Europe. Mol. Genet. Metab. Rep. 2018, 16, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Aksoy, B.; Kuyum, P.; Tuncer, N.; Arslan, N.; Ozturk, Y. The Effects of Breastfeeding in Infants with Phenylketonuria. J. Pediatr. Nurs. 2018, 38, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Unicef, UK, Baby-Friendly Initiative Standards. Available online: https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2014/02/Guide-to-the-Unicef-UK-Baby-Friendly-Initiative-Standards.pdf (accessed on 26 June 2023).
- Evans, S.; Daly, A.; Wildgoose, J.; Cochrane, B.; Chahal, S.; Ashmore, C.; Loveridge, N.; MacDonald, A. How Does Feeding Development and Progression onto Solid Foods in PKU Compare with Non-PKU Children During Weaning? Nutrients 2019, 11, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennox, A.; Sommerville, J.; Ong, K.; Henderson, H.; Allen, R. (Eds.) Diet and Nutrition Survey of Infants and Young Children; Department of Health and Social Care: London, UK, 2011.
- Clark, A.; Merrigan, C.; Crushell, E.; Hughes, J.; Knerr, I.; Monavari, A.A.; Treacy, E.; Coughlan, A. Ten-year retrospective review (2003–2013) of 56 inpatient admissions to stabilize elevated phenylalanine levels. JIMD Rep. 2019, 46, 70–74. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Benefits of Breastfeeding |
| “I felt at the time that I wanted to give my daughter the best possible start and thought the goodness of breast milk was better than formula”. “I had wanted to exclusively breastfeed anyway but when he was diagnosed I wanted prevent illnesses as much as possible so his Phe level wouldn’t increase”. “Terrifying to think my milk was harming baby but when assured formula would have shown same results decided to continue, secretly hoping deep down my milk would adapt to babies needs as it’s said to when they have a cold etc”. |
| Control/Accuracy/Precision |
| “Having to introduce a formula before breastfeeding, took away from breast only feeding. I did continue for approx.10 weeks, but found, PKU formula, breast and normal formula, very hard work to manage all”. |
| Overwhelming |
| “My baby was born 5 weeks premature, in SCBU for a week on CPAP, all prior to being diagnosed with PKU. I found it all overwhelming and decided to formula feed after a couple of weeks of feeding my baby expressed breast milk”. |
| Lack of Experience |
| “I was a first time mother, breast feeding can be stressful anyway but I found my baby was extremely stressed moving between the breast feeding and formula within the one feed. I was also dealing with my first baby and the worry of the diagnosis. A few years down the road and having breastfed my second child (without PKU) I think I would be more confident with breastfeeding should I have another child with PKU, having experience with breastfeeding and also PKU”. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rice, J.; McNulty, J.; O’Shea, M.; Gudex, T.; Knerr, I. A Retrospective Chart Review and Infant Feeding Survey in the Irish Phenylketonuria (PKU) Population (2016–2020). Nutrients 2023, 15, 3380. https://doi.org/10.3390/nu15153380
Rice J, McNulty J, O’Shea M, Gudex T, Knerr I. A Retrospective Chart Review and Infant Feeding Survey in the Irish Phenylketonuria (PKU) Population (2016–2020). Nutrients. 2023; 15(15):3380. https://doi.org/10.3390/nu15153380
Chicago/Turabian StyleRice, Jane, Jenny McNulty, Meabh O’Shea, Teresa Gudex, and Ina Knerr. 2023. "A Retrospective Chart Review and Infant Feeding Survey in the Irish Phenylketonuria (PKU) Population (2016–2020)" Nutrients 15, no. 15: 3380. https://doi.org/10.3390/nu15153380
APA StyleRice, J., McNulty, J., O’Shea, M., Gudex, T., & Knerr, I. (2023). A Retrospective Chart Review and Infant Feeding Survey in the Irish Phenylketonuria (PKU) Population (2016–2020). Nutrients, 15(15), 3380. https://doi.org/10.3390/nu15153380