

Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review
 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Question
2.2. Search Strategy
2.3. Study Selection
2.4. Risk of Bias Assessment
3. Results
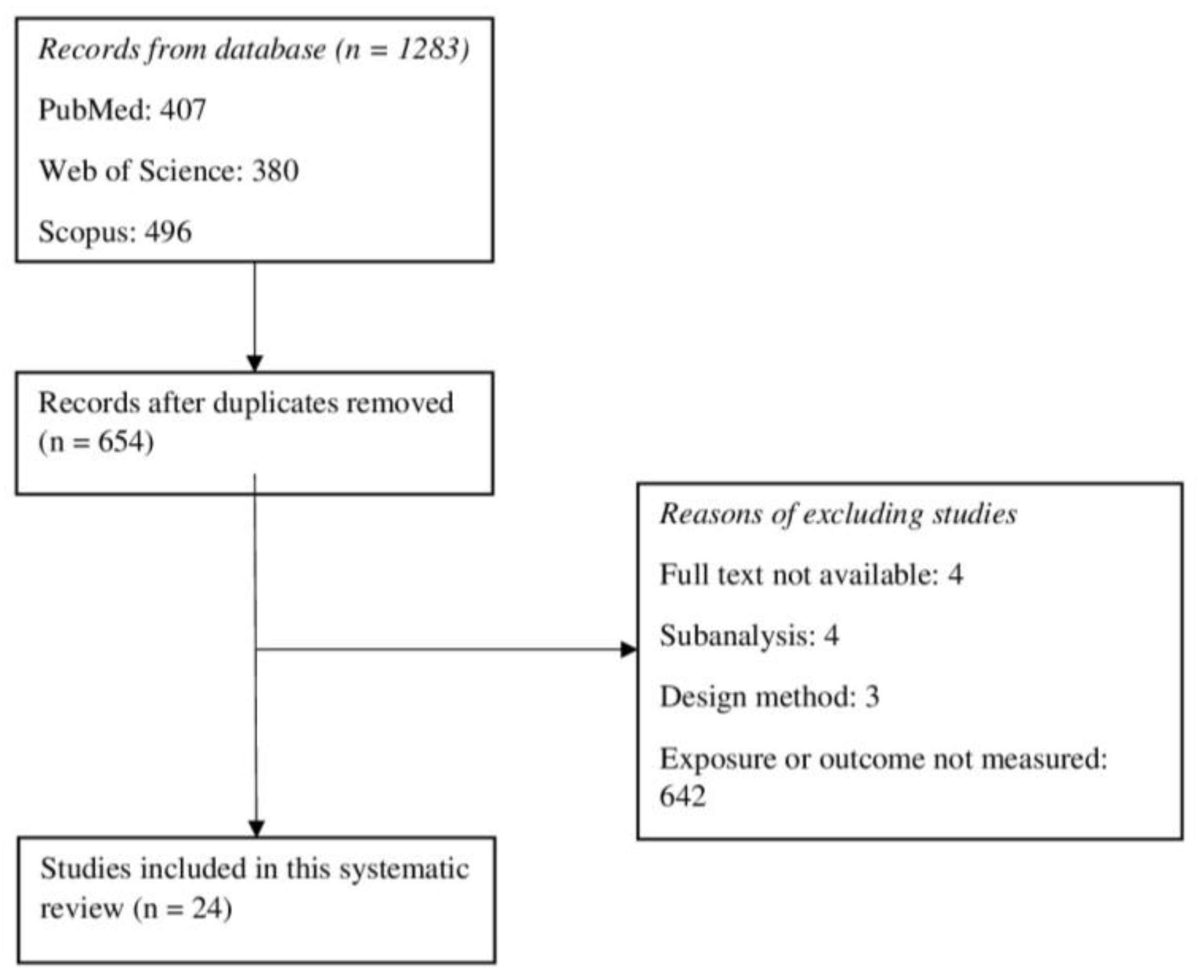
3.1. Study Selection
3.2. Study Characteristics
3.3. Impact of Mediterranean Diet on Cardiovascular Outcomes and Death in the General Population (Primary Prevention)
3.3.1. All-Cause Mortality
3.3.2. Cardiovascular Mortality
3.3.3. Major Cardiovascular Events
3.4. Impact of Mediterranean Diet on Cardiovascular Outcomes and Death in Patients with a Prior Cardiovascular Disease (Secondary Prevention)
3.4.1. All-Cause Mortality
3.4.2. Cardiovascular Mortality
3.4.3. Composite Cardiovascular Outcomes
3.5. Methodological Quality and Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Million Hearts: Strategies to Reduce the Prevalence of Leading Cardiovascular Disease Risk Factors. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1251. [Google Scholar]
- Francula-Zaninovic, S.; Nola, I.A. Management of Measurable Variable Cardiovascular Disease’ Risk Factors. Curr. Cardiol. Rev. 2018, 14, 153–163. [Google Scholar] [CrossRef]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar]
- World Health Organization. Cardiovascular Diseases; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Instituto Nacional de Estadística. Defunciones Según la Causa de Muerte Año 2020; Instituto Nacional de Estadística: Madrid, Spain, 2021.
- Castellano, J.M.; Narula, J.; Castillo, J.; Fuster, V. Promoción de la salud cardiovascular global: Estrategias, retos y oportunidades. Rev. Esp. Cardiol. 2014, 67, 724–730. [Google Scholar]
- Franco, M.; Cooper, R.; Bilal, U.; Fuster, V. Control of Coronary Heart Disease Risk Factors and Evidence-Based Therapies: Joint Efforts for Coronary Heart Disease Prevention in Spain. Rev. Esp. Cardiol. 2011, 64, 962–964. [Google Scholar]
- de Backer, G. Epidemiology and prevention of cardiovascular disease: Quo vadis? Eur. J. Prev. Cardiol. 2017, 24, 768–772. [Google Scholar]
- Perk, J.; de Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) * Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar]
- Arós, F.; Estruch, R. Mediterranean Diet and Cardiovascular Prevention. Rev. Esp. Cardiol. 2013, 66, 771–774. [Google Scholar]
- Kastorini, C.-M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The Effect of Mediterranean Diet on Metabolic Syndrome and its Components. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Felices, R.Y.; Escudero, G.A.; Soto, M.C.; García, F.M.; Mjm, A.; Aliaga Li Planells, E.M.; Lisbona, F. Lipidic metabolism and healthy habits in a group of university students from Granada. Ars. Pharm. 2010, 51, 407–419. [Google Scholar]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean Diet, its Components, and Cardiovascular Disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Becerra-Tomás, N.; García-Gavilán, J.F.; Bulló, M.; Barrubés, L. Mediterranean Diet and Cardiovascular Disease Prevention: What Do We Know? Prog. Cardiovasc. Dis. 2018, 61, 62–67. [Google Scholar] [PubMed]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0, the Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Effectiveness of the Mediterranean Diet: Can It Help Delay or Prevent Alzheimer’s Disease? J. Alzheimer’s Dis. 2010, 20, 795–801. [Google Scholar]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [PubMed]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Yubero-Serrano, E.M.; et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): A randomised controlled trial. Lancet 2022, 399, 1876–1885. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Declaración PRISMA 2020, una guía actualizada para la publicación de revisiones sistemáticas. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar]
- Wells, G.; Shea, B.; O’Conell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hosp. Res. Inst. 2014, 7, 79550924. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [PubMed]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Agudo, A.; Travier, N.; Huerta, J.M.; Cirera, L.; Tormo, M.J.; Navarro, C.; Chirlaque, M.D.; Moreno-Iribas, C.; Ardanaz, E.; et al. Adherence to the Mediterranean diet reduces mortality in the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Spain). Br. J. Nutr. 2011, 106, 1581–1591. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef]
- Gardener, H.; Wright, C.B.; Gu, Y.; Demmer, R.T.; Boden-Albala, B.; Elkind, M.S.; Sacco, R.L.; Scarmeas, N. Mediterranean-style diet and risk of ischemic stroke, myocardial infarction, and vascular death: The Northern Manhattan study. Am. J. Clin. Nutr. 2011, 94, 1458–1464. [Google Scholar]
- Hoevenaar-Blom, M.P.; Nooyens, A.C.; Kromhout, D.; Spijkerman, A.M.; Beulens, J.W.; Van Der Schouw, Y.T.; Bueno-de-Mesquita, B.; Verschuren, W.M. Mediterranean Style Diet and 12-Year Incidence of Cardiovascular Diseases: The EPIC-NL Cohort Study. PLoS ONE 2012, 7, e45458. [Google Scholar]
- Knoops, K.T.B.; De Groot, L.C.P.G.M.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; Van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar]
- Lagiou, P.; Trichopoulos, D.; Sandin, S.; Lagiou, A.; Mucci, L.; Wolk, A.; Elisabete, E.; Adami, H.O. Mediterranean dietary pattern and mortality among young women: A cohort study in Sweden. Br. J. Nutr. 2006, 96, 384–392. [Google Scholar]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovas. Dis. 2011, 21, 237–244. [Google Scholar]
- Martínez-González, M.A.; Guillén-Grima, F.; De Irala, J.; Ruíz-Canela, M.; Bes-Rastrollo, M.; Beunza, J.J.; López del Burgo, C.; Toledo, E.; Carlos, S.; Sánchez-Villegas, A.; et al. The Mediterranean diet is associated with a reduction in premature mortality among middle-aged adults. J. Nutr. 2012, 142, 1672–1678. [Google Scholar] [PubMed]
- Mitrou, P.N.; Kipnis, V.; Thiébaut, A.C.; Reedy, J.; Subar, A.F.; Wirfält, E.; Flood, A.; Mouw, T.; Hollenbeck, A.R.; Leitzmann, M.F.; et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population. Arch. Intern. Med. 2007, 167, 2461–2468. [Google Scholar] [CrossRef]
- Tektonidis, T.G.; Åkesson, A.; Gigante, B.; Wolk, A.; Larsson, S.C. A Mediterranean diet and risk of myocardial infarction, heart failure and stroke: A population-based cohort study. Atherosclerosis 2015, 243, 93–98. [Google Scholar]
- Tong, T.Y.N.; Wareham, N.J.; Khaw, K.T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-Mediterranean population: The EPIC-Norfolk study. BMC Med. 2016, 14, 135. [Google Scholar]
- Tognon, G.; Lissner, L.; Sæbye, D.; Walker, K.Z.; Heitmann, B.L. The Mediterranean diet in relation to mortality and CVD: A Danish cohort study. Br. J. Nutr. 2014, 111, 151–159. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Barzi, F.; Woodward, M.; Marfisi, R.M.; Tavazzi, L.; Valagussa, F.; Marchioli, R. Mediterranean diet and all-causes mortality after myocardial infarction: Results from the GISSI-Prevenzione trial. Eur. J. Clin. Nutr. 2003, 57, 604–611. [Google Scholar] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; De Curtis, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Moli-sani Study Investigators. Interaction between Mediterranean diet and statins on mortality risk in patients with cardiovascular disease: Findings from the Moli-sani Study. Int. J. Cardiol. 2019, 276, 248–254. [Google Scholar]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar]
- Iestra, J.; Knoops, K.; Kromhout, D.; de Groot, L.; Grobbee, D.; Van Staveren, W. Lifestyle, Mediterranean diet and survival in European post-myocardial infarction patients. Eur. J. Prev. Cardiol. 2006, 13, 894–900. [Google Scholar]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Fung, T.T.; Li, S.; Willett, W.C.; Rimm, E.B.; Hu, F.B. The mediterranean-style dietary pattern and mortality among men and women with cardiovascular disease. Am. J. Clin. Nutr. 2014, 99, 172–180. [Google Scholar] [PubMed]
- Shikany, J.M.; Safford, M.M.; Bryan, J.; Newby, P.K.; Richman, J.S.; Durant, R.W.; Brown, T.M.; Judd, S.E. Dietary patterns and Mediterranean diet score and hazard of recurrent coronary heart disease events and all-cause mortality in the regards study. J. Am. Heart Assoc. 2018, 7, e008078. [Google Scholar]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457. [Google Scholar] [PubMed]
- Trichopoulou, A.; Bamia, C.; Norat, T.; Overvad, K.; Schmidt, E.B.; Tjønneland, A.; Halkjaer, J.; Clavel-Chapelon, F.; Vercambre, M.N.; Boutron-Ruault, M.C.; et al. Modified Mediterranean diet and survival after myocardial infarction: The EPIC-Elderly study. Eur. J. Epidemiol. 2007, 22, 871–881. [Google Scholar]
- Trichopoulou, A.; Bamia, C.; Trichopoulos, D. Mediterranean diet and survival among patients with coronary heart disease in Greece. Arch. Intern. Med. 2005, 165, 929–935. [Google Scholar] [PubMed]
- Kim, J.Y.; Yang, Y.J.; Yang, Y.K.; Oh, S.Y.; Hong, Y.C.; Lee, E.K.; Kwon, O. Diet quality scores and oxidative stress in Korean adults. Eur. J. Clin. Nutr. 2011, 65, 1271–1278. [Google Scholar] [PubMed]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [PubMed]
- Rumawas, M.E.; Dwyer, J.T.; McKeown, N.M.; Meigs, J.B.; Rogers, G.; Jacques, P.F. The development of the Mediterranean-style dietary pattern score and its application to the American diet in the Framingham Offspring Cohort. J. Nutr. 2009, 139, 1150–1156. [Google Scholar]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food Sci. Nutr. 2017, 68, 757–762. [Google Scholar]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease: A Cochrane Database Review. Glob. Heart 2020, 15, 56. [Google Scholar] [PubMed]


{kind=link}
| Author (Year) | Participants n, Age (Years) | Country | MD Assessment | Design and Follow-Up | Outcomes |
|---|---|---|---|---|---|
| Buckland G et al., (2009) [25] | 41,078 29–69 (range); 49.3 (mean) | Spain | rMED (0–18) | Prospective cohort 10.4 years (mean) | Fatal and non-fatal MI, angina requiring revascularization |
| Buckland G et al., (2011) [26] | 40,622 29–69 (range); 49.3 (mean) | Spain | rMED (0–18) | Prospective cohort 13.4 years (mean) | All-cause and cardiovascular mortality |
| Estruch R et al., (2013) [27] | 7447 participants with high CVD risk 50–80 (range); 67 (mean) | Spain | Quantitative score (0–14) Biomarkers | RCT (MD with EVOO/nuts vs. control) 4.8 years (median) | Composite of MI, stroke, and cardiovascular mortality |
| Fung TT et al., (2009) [28] | 74,886 women 38–63 (range) | USA | Alternate MDS | Prospective cohort 20 years | CAD mortality, CAD |
| Gardener H et al., (2011) [29] | 2568 >40; 68.6 (mean) | USA | MDS (0–9) | Prospective cohort 9 years | Composite of ischemic stroke, MI, or cardiovascular mortality |
| Hoevenaar-Blom MP et al., (2012) [30] | 34,708 20–70 (range) | Netherlands | MDS (0–9) | Prospective cohort 11.8 years (mean) | Cardiovascular mortality, CVD, MI, and stroke |
| Knoops KTB et al., (2004) [31] | 2339 70–90 (range) | Europe | mMDS (0–8) | Prospective cohort 10 years | All-cause, CVD and CAD mortality |
| Lagiou P et al., (2006) [32] | 42,237 women 30–49 (range) | Sweden | MDS (0–9) | Prospective cohort 12 years | All-cause mortality |
| Martínez-González MA et al., (2011) [33] | 13,609 38 (mean) | Spain | MDS (0–9) | Prospective cohort 4.9 years | Cardiovascular disease |
| Martínez-González MA et al., (2012) [34] | 15,535 38 (mean) | Spain | MDS (0–9) | Prospective cohort 6.8 years | All-cause mortality |
| Mitrou PN et al., (2007) [35] | 380,296 50–71 (range) | USA | aMDS (0–9) | Prospective cohort 10 years | All-cause and CVD mortality |
| Tektonidis TG et al., (2015) [36] | 32,921 women 48–83 (range) | Sweden | mMDS (0–8) | Prospective cohort 10 years | MI, heart failure and stroke |
| Tong TYN et al., (2016) [37] | 23,902 40–79 (range) | UK | tMDS (0–18) MDS (0–9) Others | Prospective cohort 17 years | Cardiovascular mortality, CVD |
| Tognon G et al., (2013) [38] | 1849 | Denmark | mMDS (0–8) | Prospective cohort | All-cause mortality, cardiovascular mortality, CVD, MI |
| Trichopoulou A et al., (2003) [39] | 41,078 29–69 (range); 49.3 (mean) | Greece | MDS (0–9) | Prospective cohort 44 months (median) | All-cause and cardiovascular mortality |
| Author (Year) | Participants n, Age (Years) | Country | MD Assessment | Design and Follow-Up | Outcomes |
|---|---|---|---|---|---|
| Barzi F et al., (2003) [40] | 11,323 patients with MI 19–90 (range); 59.4 (mean) | Italy | Overall nutrition score 0–10 | Prospective cohort 6.5 years | All-cause mortality |
| Bonaccio M et al., (2018) [41] | 1180 patients with prior CVD ≥35; 67.7 (mean) | Italy | MDS (0–9) | Prospective cohort 7.9 years | All-cause mortality, cardiovascular and CAD mortality |
| Delgado-Lista J et al., (2022) [21] | 1002 patients with previous CAD (ACS or high-risk CAD) | Spain | Quantitative score 0–14 | RCT (MD vs. low-fat diet) 7 years | Composite of MI, revascularization, stroke, peripheral artery disease, and CVD death |
| De Lorgeril M et al., (1999) [42] | 423 patients < 70 years with prior MI | France | NA | RCT (MD vs. control) 46 months | Composite outcome CVD death, MI, angina, stroke, heart failure, pulmonary, or peripheral embolism |
| Iestra J et al., (2006) [43] | 426 patients with prior MI ≥70 | Europe | MDS (0–9) | Prospective cohort 10 years | All-cause mortality |
| Lopez-Garcia E et al., (2014) [44] | 17,415 participants with prior MI, stroke, angina, bypass or angioplasty 40–75 (range); 69 (mean) | USA | Alternate MDS | Prospective cohort 7.7 years (median) | All-cause mortality, cardiovascular mortality |
| Shikany JM et al., (2018) [45] | 3562 participants with previous CAD, ≥45; 68.9 (mean) | USA | MDS (0–9) | Prospective cohort 7.1 years | All-cause mortality, CAD (MI and CAD death) |
| Trichopoulou A et al., (2005) [46] | 1302 participants with CAD 20–86 (range) | Greece | MDS (0–9) | Prospective cohort 3.78 years | All-cause mortality, cardiovascular mortality |
| Trichopoulou A et al., (2007) [47] | 2671 patients with previous MI >60 | Europe | MDS (0–9) | Prospective cohort 6.7 years | All-cause mortality |
| Prospective Cohort Studies | ||||
| Author (Year) | Score | Medium vs. Low | High vs. Low | Per Point Increase |
| Buckland G et al., (2011) [26] | rMED | 0.88 (0.79–0.99) | 0.79 (0.69–0.91) | 0.94 (0.9–0.97) every 2 points |
| Martínez-González MA et al., (2012) [34] | MDS | 0.66 (0.39–1.11) | 0.44 (0.24–0.79) | 0.76 (0.61–0.94) every 2 points |
| Knoops KTB et al., (2004) [31] | mMDS | NA | 0.77 (0.68–0.88) | NA |
| Tong TYN, et al., (2016) [37] | rMED MDS | NA NA | NA NA | 0.97 (0.94–0.99) per SD 0.96 (0.93–0.98) per SD |
| Tognon G, et al., (2013) [38] | mMDS | NA | NA | 0.95 (0.91–1.00) per point |
| Trichopoulou A et al., (2003) [39] | MDS | NA | NA | 0.75 (0.64–0.87) every 2 points |
| Randomized Clinical Trial | ||||
| Author (Year) | MD with EVOO | MD with Nuts | Combined MD | |
| Estruch R et al., (2013) [27] | 0.82 (0.64–1.07) | 0.97 (0.74–1.26) | 0.89 (0.71–1.12) | |
| Prospective Cohort Studies | ||||
| Author (Year) | Score | Medium vs. Low Risk | High vs. Low Risk | Per Point Increase |
| Buckland G et al., (2011) [34] | rMED | 0.84 (0.66–1.09) | 0.66 (0.49–0.89) | 0.88 (0.81–0.95) every 2 points |
| Gardener H et al., (2011) [29] | MDS | 4p: 0.70 (0.48–1.02) 5p: 0.69 (0.47–1.00) | 0.71 (0.49–1.04) | 0.91 (0.85–0.98) per point |
| Hoevenaar-Blom MP et al., (2012) [30] | MDS | 0.60 (0.44–0.80) | 0.44 (0.30–0.66) | 0.78 (0.69–0.88) per point |
| Knoops KTB et al., (2004) [31] | mMDS | NA | 0.71 (0.58–0.88) | NA |
| Tong TYN, et al., (2016) [37] | rMED MDS | NA | NA | 0.94 (0.90–0.99) per SD 0.94 (0.89–0.98) per SD |
| Tognon G, et al., (2013) [38] | mMDS | NA | NA | 0.96 (0.89–1.05) per unit |
| Randomized Clinical Trial | ||||
| Author (Year) | MD with EVOO | MD with Nuts | Combined MD | |
| Estruch R et al., (2013) [26] | 0.69 (0.41–1.16) | 1.01 (0.61–1.66) | 0.83 (0.54–1.29) | |
| Prospective Cohort Studies | ||||
| Author (Year) | Score | Medium vs. Low | High vs. Low | Per Point Increase |
| Buckland G et al., (2009) [25] Fatal and non-fatal MI, angina requiring revascularization | rMED | 0.86 (0.7–1.04) | 0.6 (0.47–0.77) | 0.94 (0.91–0.97) |
| Hoevenaar-Blom MP et al., (2012) [30] MI, stroke, CVD death | MDS | 0.72 (0.61–0.85) | 0.65 (0.53–0.80) | 0.85 (0.80–0.91) per point |
| Randomized Clinical Trial | ||||
| Author (Year) | MD with EVOO | MD with Nuts | Combined MD | |
| Estruch R et al., (2013) [27] MI, stroke, CVD death | 0.70 (0.54–0.92) | 0.72 (0.54–0.96) | 0.71 (0.56–0.90) | |
| Author (Year) | Score | Medium vs. Low | High vs. Low | Per Point Increase |
|---|---|---|---|---|
| Barzi F et al., (2003) [40] | Other | 0.69 (0.61–0.79) | 0.51 (0.44–0.59) | 0.85 (0.82–0.88) per point |
| Bonaccio M et al., (2018) [41] | MDS | 0.82 (0.60–1.12) | 0.69 (0.47–0.99) | 0.84 (0.70–1.00) every 2 points |
| Iestra J et al., (2006) [43] | MDS | NA | 0.75 (0.57–0.97) | NA |
| Lopez-Garcia E et al., (2014) [44] | aMDS | Q2: 0.98 (0.89, 1.08) Q3: 0.90 (0.81, 1.00) | Q4: 0.94 (0.81, 1.08) Q5: 0.81 (0.72–0.91) | 0.93 (0.89, 0.97) every 2 points |
| Shikany JM et al., (2018) [45] | MDS | 0.98 (0.85–1.13) | 0.80 (0.67–0.95) | NA |
| Trichopoulou A et al., (2005) [48] | MDS | NA | NA | 0.73 (0.58–0.93) every 2 points |
| Trichopoulou A et al., (2007) [47] | MDS | NA | NA | 0.82 (0.73–0.93) every 2 points |
| Prospective Cohort Studies | ||||
|---|---|---|---|---|
| Author (Year) | Score | Medium vs. Low | High vs. Low | Per Point Increase |
| Bonaccio M et al., (2018) [41] | MDS | 0.73 (0.48–1.12) | 0.61 (0.35–1.01) | 0.77 (0.61–0.97) every 2 points |
| Lopez-Garcia E et al., (2014) [44] | aMDS | Q2: 1.00 (0.79, 1.27) Q3: 0.99 (0.78, 1.25) | Q4: 1.02 (0.87, 1.21) Q5: 0.85 (0.67, 1.09) | 0.96 (0.89, 1.04) every 2 points |
| Trichopoulou A et al., (2005) [48] | MDS | NA | NA | 0.69 (0.52–0.93) every 2 points |
| Prospective Cohort Studies | |||
| Author (Year) | Score | Medium vs. Low | High vs. Low |
| Shikany JM et al., (2018) [45] MI, CAD mortality | MDS | 0.91 (0.76–1.10) | 0.78 (0.62–0.98) |
| RCT | |||
| Author (Year) | Mediterranean Diet vs. Control Diet | ||
| Delgado-Lista J et al., (2022) [21] MI, revascularization, stroke, peripheral artery disease, and cardiovascular death | HR (7 models) ranged from 0.719 (95% CI 0.541–0.957) to 0.753 (0.568–0.998) | ||
| De Lorgeril M et al., (1999) [42] | CO 1 (MI, CVD death): 0.23 (0.11–0.48) CO 2 (MI, CVD death, unstable angina, HF, stroke, embolism): 0.30 (0.18–0.51) | ||
| Primary Prevention | |||||
| Author (Year) | Medium vs. Low | High vs. Low | Per Point Increase | p | |
| Buckland G et al., (2011) [26] | Men (15,324) | 0.88 (0.75–1.02) | 0.76 (0.63–0.9) | - | p-interaction: 0.512 |
| Women (25,298) | 0.89 (0.75–1.06) | 0.85 (0.68–1.06) | - | ||
| Martínez-González MA et al., (2012) [34] | Men (6271) | - | - | 0.67 (0.51–0.88) every 2 points | p-trend 0.004 |
| Women (9264) | - | - | 0.83 (0.53–1.29) every 2 points | p-trend 0.41 | |
| Mitrou PN et al., (2007) [35] | Men (214 284) | 0.91 (0.88–0.94) | 0.79 (0.76–0.83) | - | - |
| Women (166 012) | 0.89 (0.85–0.93) | 0.80 (0.75–0.85) | - | - | |
| Trichopoulou A et al., (2003) [39] | Men (8895) | - | - | 0.78 (0.65–0.94) every 2 points | - |
| Women (13,148) | - | - | 0.69 (0.53–0.90) every 2 points | - | |
| Secondary Prevention | |||||
| Barzi F et al., (2003) [40] | Men (9625) | - | - | 0.86 (0.83–0.89) per point | p-interaction: 0.13 |
| Women (1698) | - | - | 0.81 (0.74–0.87) per point | ||
| Iestra J et al., (2006) [43] | Men (284) | - | 0.74 (0.55–1.00) | - | - |
| Women (142) | - | 0.86 (0.46–1.61) | - | - | |
| López-García E et al., (2014) [44] | Men (6137) | 0.85 (0.74, 0.98) * | 0.79 (0.68, 0.91) * | 0.92 (0.86, 0.97) every 2 points | p-trend: 0.003 |
| Women (11,278) | 0.95 (0.81, 1.11) * | 0.85 (0.71, 1.02) * | 0.95 (0.88, 1.01) every 2 points | p-trend: 0.11 | |
| Trichopoulou A et al., (2005) [48] | Men (726) | 0.69 (0.53–0.90) every 2 points | p-interaction: 0.33 | ||
| Women (576) | 0.89 (0.56–1.41) every 2 points | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laffond, A.; Rivera-Picón, C.; Rodríguez-Muñoz, P.M.; Juárez-Vela, R.; Ruiz de Viñaspre-Hernández, R.; Navas-Echazarreta, N.; Sánchez-González, J.L. Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review. Nutrients 2023, 15, 3356. https://doi.org/10.3390/nu15153356
Laffond A, Rivera-Picón C, Rodríguez-Muñoz PM, Juárez-Vela R, Ruiz de Viñaspre-Hernández R, Navas-Echazarreta N, Sánchez-González JL. Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review. Nutrients. 2023; 15(15):3356. https://doi.org/10.3390/nu15153356
Chicago/Turabian StyleLaffond, Ana, Cristina Rivera-Picón, Pedro Manuel Rodríguez-Muñoz, Raúl Juárez-Vela, Regina Ruiz de Viñaspre-Hernández, Noelia Navas-Echazarreta, and Juan Luis Sánchez-González. 2023. "Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review" Nutrients 15, no. 15: 3356. https://doi.org/10.3390/nu15153356
APA StyleLaffond, A., Rivera-Picón, C., Rodríguez-Muñoz, P. M., Juárez-Vela, R., Ruiz de Viñaspre-Hernández, R., Navas-Echazarreta, N., & Sánchez-González, J. L. (2023). Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review. Nutrients, 15(15), 3356. https://doi.org/10.3390/nu15153356