
Roux-en-Y Gastric Bypass Improves Adiponectin to Leptin Ratio and Inflammatory Profile in Severely Obese Women with and without Metabolic Syndrome: A Randomized Controlled Trial
 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
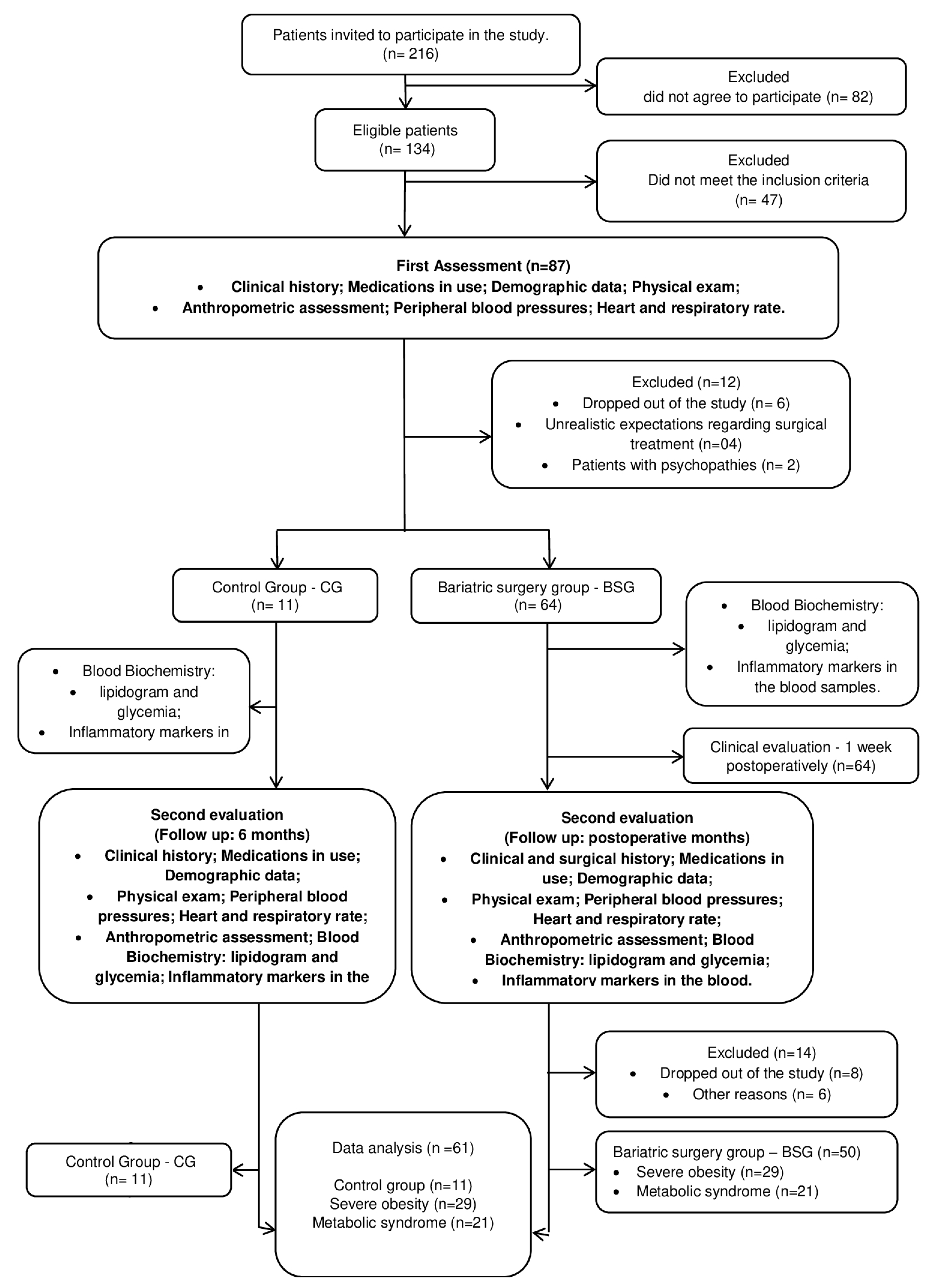
2.1. Trial Design
2.2. Study Setting
2.3. Participants and Eligibility Criteria
2.4. Recruitment and Randomization
2.5. Protocol for Clinical and Surgical Assessment
2.6. Blood Biochemical Analysis
2.7. Surgical Procedures
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaacks, L.M.; Vandevijvere, S.; Pan, A.; McGowan, C.J.; Wallace, C.; Imamura, F.; Mozaffarian, D.; Swinburn, B.; Ezzati, M. The Obesity Transition: Stages of the Global Epidemic. Lancet Diabetes Endocrinol. 2019, 7, 231–240. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. 5 July 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 7 June 2023).
- Piché, M.-E.; Poirier, P.; Lemieux, I.; Després, J.-P. Overview of Epidemiology and Contribution of Obesity and Body Fat Distribution to Cardiovascular Disease: An Update. Prog. Cardiovasc. Dis. 2018, 61, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Koliaki, C.; Liatis, S.; Kokkinos, A. Obesity and Cardiovascular Disease: Revisiting an Old Relationship. Metabolism 2019, 92, 98–107. [Google Scholar] [CrossRef]
- Mathew, B.; Francis, L.; Kayalar, A.; Cone, J. Obesity: Effects on Cardiovascular Disease and Its Diagnosis. J. Am. Board Fam. Med. 2008, 21, 562–568. [Google Scholar] [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.B.; Brewer, H.B., Jr.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C., Jr.; Stone, N.J. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef]
- Huang, P.L. A Comprehensive Definition for Metabolic Syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.; Misra, A. Prevalence and Trends of Metabolic Syndrome among Adults in the Asia-Pacific Region: A Systematic Review. BMC Public Health 2017, 17, 101. [Google Scholar] [CrossRef] [PubMed]
- do Vale Moreira, N.C.; Hussain, A.; Bhowmik, B.; Mdala, I.; Siddiquee, T.; Fernandes, V.O.; Júnior, R.M.M.; Meyer, H.E. Prevalence of Metabolic Syndrome by Different Definitions, and Its Association with Type 2 Diabetes, Pre-Diabetes, and Cardiovascular Disease Risk in Brazil. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1217–1224. [Google Scholar] [CrossRef]
- Friend, A.; Craig, L.; Turner, S. The Prevalence of Metabolic Syndrome in Children: A Systematic Review of the Literature. Metab. Syndr. Relat. Disord. 2013, 11, 71–80. [Google Scholar] [CrossRef]
- Tan, M.C.; Ng, O.C.; Wong, T.W.; Joseph, A.; Chan, Y.M.; Hejar, A.R. Prevalence of Metabolic Syndrome in Type 2 Diabetic Patients: A Comparative Study Using WHO, NCEP ATP III, IDF and Harmonized Definitions. Health 2013, 2013, 38005. [Google Scholar] [CrossRef]
- Reddy, P.; Lent-Schochet, D.; Ramakrishnan, N.; McLaughlin, M.; Jialal, I. Metabolic Syndrome Is an Inflammatory Disorder: A Conspiracy between Adipose Tissue and Phagocytes. Clin. Chim. Acta 2019, 496, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms Linking Obesity with Cardiovascular Disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef]
- Rodriguez-Ayala, E.; Gallegos-Cabrales, E.C.; Gonzalez-Lopez, L.; Laviada-Molina, H.A.; Salinas-Osornio, R.A.; Nava-Gonzalez, E.J.; Leal-Berumen, I.; Escudero-Lourdes, C.; Escalante-Araiza, F.; Buenfil-Rello, F.A. Towards Precision Medicine: Defining and Characterizing Adipose Tissue Dysfunction to Identify Early Immunometabolic Risk in Symptom-Free Adults from the GEMM Family Study. Adipocyte 2020, 9, 153–169. [Google Scholar] [CrossRef]
- Frühbeck, G.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Salvador, J.; Colina, I.; Gómez-Ambrosi, J. Adiponectin-Leptin Ratio Is a Functional Biomarker of Adipose Tissue Inflammation. Nutrients 2019, 11, 454. [Google Scholar] [CrossRef]
- Tchang, B.G.; Saunders, K.H.; Igel, L.I. Best Practices in the Management of Overweight and Obesity. Med. Clin. 2021, 105, 149–174. [Google Scholar] [CrossRef]
- Gómez, F.I.; Ortega, M.G.; Alonso, A.A.; Soler, I.O.; Tafalla, M.S.A.; Paredes, M.P.; Almela, M.L.L. Obesity, Endothelial Function and Inflammation: The Effects of Weight Loss after Bariatric Surgery. Nutr. Hosp. 2016, 33, 1340–1346. [Google Scholar]
- Chiappetta, S.; Schaack, H.M.; Wölnerhannsen, B.; Stier, C.; Squillante, S.; Weiner, R.A. The Impact of Obesity and Metabolic Surgery on Chronic Inflammation. Obes. Surg. 2018, 28, 3028–3040. [Google Scholar] [CrossRef] [PubMed]
- Villarreal-Calderon, J.R.; Cuellar-Tamez, R.; Castillo, E.C.; Luna-Ceron, E.; García-Rivas, G.; Elizondo-Montemayor, L. Metabolic Shift Precedes the Resolution of Inflammation in a Cohort of Patients Undergoing Bariatric and Metabolic Surgery. Sci. Rep. 2021, 11, 12127. [Google Scholar] [CrossRef]
- The Look AHEAD Research Group. Look AHEAD Research Group Look AHEAD (Action for Health in Diabetes): Design and Methods for a Clinical Trial of Weight Loss for the Prevention of Cardiovascular Disease in Type 2 Diabetes. Control. Clin. Trials 2003, 24, 610–628. [Google Scholar] [CrossRef] [PubMed]
- Look AHEAD Research Group. Eight-year Weight Losses with an Intensive Lifestyle Intervention: The Look AHEAD Study. Obesity 2014, 22, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Chao, A.M.; Bahnson, J.L.; Bantle, J.P.; Clark, J.M.; Gaussoin, S.A.; Jakicic, J.M.; Johnson, K.C.; Miller, G.D.; Unick, J.L. End-of-trial Health Outcomes in Look AHEAD Participants Who Elected to Have Bariatric Surgery. Obesity 2019, 27, 581–590. [Google Scholar] [CrossRef]
- Cordero, P.; Li, J.; Oben, J. Bariatric Surgery as a Treatment for Metabolic Syndrome. J. R. Coll. Physicians Edinb. 2017, 47, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Calvo, B.; Gracia, J.; Bielsa, M.; Martínez, M. Metabolic Effects and Outcomes of Sleeve Gastrectomy and Gastric Bypass: A Cohort Study. Surg. Endosc. 2020, 34, 5550–5557. [Google Scholar] [CrossRef]
- Yadav, R.; Hama, S.; Liu, Y.; Siahmansur, T.; Schofield, J.; Syed, A.A.; France, M.; Pemberton, P.; Adam, S.; Ho, J.H. Effect of Roux-En-Y Bariatric Surgery on Lipoproteins, Insulin Resistance, and Systemic and Vascular Inflammation in Obesity and Diabetes. Front. Immunol. 2017, 8, 1512. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.R. Inflammatory Markers and Bariatric Surgery: A Meta-Analysis. Inflamm. Res. 2012, 61, 789–807. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Dickersin, K.; Moher, D. SPIRIT 2013: New Guidance for Content of Clinical Trial Protocols. Lancet 2013, 381, 91–92. [Google Scholar] [CrossRef]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and Cardiovascular Disease: Pathophysiology, Evaluation, and Effect of Weight Loss: An Update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006, 113, 898–918. [Google Scholar]
- Lavie, C.J.; Arena, R.; Alpert, M.A.; Milani, R.V.; Ventura, H.O. Management of Cardiovascular Diseases in Patients with Obesity. Nat. Rev. Cardiol. 2018, 15, 45–56. [Google Scholar] [CrossRef]
- Poirier, P.; Alpert, M.A.; Fleisher, L.A.; Thompson, P.D.; Sugerman, H.J.; Burke, L.E.; Marceau, P.; Franklin, B.A. Cardiovascular Evaluation and Management of Severely Obese Patients Undergoing Surgery: A Science Advisory from the American Heart Association. Circulation 2009, 120, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Rafey, M.; Fang, C.; Ioana, I.; Griffin, H.; Hynes, M.; O’Brien, T.; McAnena, O.; O’Shea, P.; Collins, C.; Davenport, C. The Leptin to Adiponectin Ratio (LAR) Is Reduced by Sleeve Gastrectomy in Adults with Severe Obesity: A Prospective Cohort Study. Sci. Rep. 2020, 10, 16270. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde 2019: Atenção Primária à Saúde e Informações Antropométricas; IBGE: Rio de Janeiro, Brazil, 2020; p. 66. [Google Scholar]
- Stahl, J.M.; Malhotra, S. Obesity Surgery Indications and Contraindications; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Salari, N.; Jafari, S.; Darvishi, N.; Valipour, E.; Mohammadi, M.; Mansouri, K.; Shohaimi, S. The Best Drug Supplement for Obesity Treatment: A Systematic Review and Network Meta-Analysis. Diabetol. Metab. Syndr. 2021, 13, 110. [Google Scholar] [CrossRef]
- Mallipedhi, A.; Prior, S.L.; Barry, J.D.; Caplin, S.; Baxter, J.N.; Stephens, J.W. Changes in Inflammatory Markers after Sleeve Gastrectomy in Patients with Impaired Glucose Homeostasis and Type 2 Diabetes. Surg. Obes. Relat. Dis. 2014, 10, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- López-Jaramillo, P.; Gómez-Arbeláez, D.; López-López, J.; López-López, C.; Martínez-Ortega, J.; Gómez-Rodríguez, A.; Triana-Cubillos, S. The Role of Leptin/Adiponectin Ratio in Metabolic Syndrome and Diabetes. Horm. Mol. Biol. Clin. Investig. 2014, 18, 37–45. [Google Scholar] [CrossRef]
- Frühbeck, G.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Portincasa, P.; Gómez-Ambrosi, J. Normalization of Adiponectin Concentrations by Leptin Replacement in Ob/Ob Mice Is Accompanied by Reductions in Systemic Oxidative Stress and Inflammation. Sci. Rep. 2017, 7, 2752. [Google Scholar] [CrossRef] [PubMed]
- Frühbeck, G.; Méndez-Giménez, L.; Fernández-Formoso, J.-A.; Fernández, S.; Rodriguez, A. Regulation of Adipocyte Lipolysis. Nutr. Res. Rev. 2014, 27, 63–93. [Google Scholar] [CrossRef]
- Frühbeck, G.; Catalán, V.; Rodríguez, A.; Gómez-Ambrosi, J. Adiponectin-Leptin Ratio: A Promising Index to Estimate Adipose Tissue Dysfunction. Relation with Obesity-Associated Cardiometabolic Risk. Adipocyte 2018, 7, 57–62. [Google Scholar] [CrossRef]
- Milone, M.; Lupoli, R.; Maietta, P.; Di Minno, A.; Bianco, P.; Ambrosino, P.; Coretti, G.; Milone, F.; Di Minno, M.N.D.; Musella, M. Lipid Profile Changes in Patients Undergoing Bariatric Surgery: A Comparative Study between Sleeve Gastrectomy and Mini-Gastric Bypass. Int. J. Surg. 2015, 14, 28–32. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Catalán, V.; Rodríguez, A.; Andrada, P.; Ramírez, B.; Ibáñez, P.; Vila, N.; Romero, S.; Margall, M.A.; Gil, M.J. Increased Cardiometabolic Risk Factors and Inflammation in Adipose Tissue in Obese Subjects Classified as Metabolically Healthy. Diabetes Care 2014, 37, 2813–2821. [Google Scholar] [CrossRef]
- Frühbeck, G.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Salvador, J.; Portincasa, P.; Colina, I.; Gómez-Ambrosi, J. Involvement of the Leptin-Adiponectin Axis in Inflammation and Oxidative Stress in the Metabolic Syndrome. Sci. Rep. 2017, 7, 6619. [Google Scholar] [CrossRef] [PubMed]
- Unamuno, X.; Izaguirre, M.; Gómez-Ambrosi, J.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Valentí, V.; Moncada, R.; Silva, C.; Salvador, J.; et al. Increase of the Adiponectin/Leptin Ratio in Patients with Obesity and Type 2 Diabetes after Roux-en-Y Gastric Bypass. Nutrients 2019, 11, 2069. [Google Scholar] [CrossRef] [PubMed]
- Ion, R.M.; Sibianu, M.; Hutanu, A.; Beresescu, F.G.; Sala, D.T.; Flavius, M.; Rosca, A.; Constantin, C.; Scurtu, A.; Moriczi, R.; et al. A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status. J. Clin. Med. 2023, 12, 3818. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; McMahon, M.M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S. Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient—2013 Update: Cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surg. Obes. Relat. Dis. 2013, 9, 159–191. [Google Scholar]
- Fernández-Soto, M.L.; Martín-Leyva, A.; González-Jiménez, A.; García-Rubio, J.; Cózar-Ibáñez, A.; Zamora-Camacho, F.J.; Leyva-Martínez, M.S.; Jiménez-Ríos, J.A.; Escobar-Jiménez, F. Remission of Type 2 Diabetes Mellitus after Bariatric Surgery—Comparison between Procedures. Endokrynol. Pol. 2017, 68, 18–25. [Google Scholar] [CrossRef]
- Zagorski, S.M.; Papa, N.N.; Chung, M.H. The Effect of Weight Loss after Gastric Bypass on C-Reactive Protein Levels. Surg. Obes. Relat. Dis. 2005, 1, 81–85. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Control Group (n = 11) | p | Bariatric Surgery (BS) Group (n = 50) | p | ||
|---|---|---|---|---|---|---|
| Evaluation 1 | Evaluation 2 | Pre-Surgery | Post-Surgery | |||
| Weight | 108 ± 17.12 | 112.64 ± 17.75 | 0.0083 | 123 ± 20.35 | 85.5 ± 15.29 | <0.0001 |
| BMI | 45.73 ± 5.45 | 46.35 ± 5.06 | 0.0102 | 47 ± 6.25 | 33 ± 5.45 | <0.0001 |
| Triglycerides | 120 ± 42.22 | 124.82 ± 34.31 | 0.9226 | 148 ± 57.05 | 90 ± 19.91 | <0.0001 |
| Total Cholesterol | 196 ± 23.34 | 194.00 ± 21.07 | 0.9341 | 196 ± 33.25 | 110 ± 21.74 | <0.0001 |
| LDL cholesterol | 123 ± 35.9 | 121.18 ± 20.77 | 0.3864 | 131 ± 30.24 | 97 ± 20.13 | <0.0001 |
| HDL cholesterol | 42 ± 6.94 | 44.18 ± 5.75 | 0.4381 | 45.5 ± 13.15 | 53 ± 10.65 | 0.0054 |
| Glycemia | 91 ± 8.06 | 104.27 ± 6.62 | 0.0165 | 103 ± 13.05 | 86 ± 8.27 | <0.0001 |
| Parameters | Severe Obesity Bariatric Surgery Group (n = 29) | p | Bariatric Surgery Group Metabolic Syndrome (n = 21) | p | p | |||
|---|---|---|---|---|---|---|---|---|
| Pre-BS | Post-BS | Pre-BS | Post-BS | Pre-BS | Post-BS | |||
| Weight | 119.81 ± 11.8 | 83.72 ± 11.6 | <0.0001 | 127.07 ± 21.4 | 88.77 ± 15.8 | <0.0001 | 0.6192 | 0.5468 |
| BMI | 44.66 ± 5 | 31 ± 4.7 | <0.0001 | 48 ± 6.2 | 34 ± 5.4 | <0.0001 | 0.3285 | 0.4534 |
| Parameters | Severe Obesity Bariatric Surgery Group (n = 29) | p | Bariatric Surgery Group Metabolic Syndrome (n = 21) | p | p | |||
|---|---|---|---|---|---|---|---|---|
| Pre-BS | Post-BS | Pre-BS | Post-BS | Pre-BS | Post-BS | |||
| Glucose | 107.75 ± 14.4 | 83 ± 9.12 | <0.0001 | 102.92 ± 12.3 | 86.53 ± 7.9 | 0.0007 | 0.6378 | 0.3656 |
| TGC | 184.36 ± 67.3 | 95.27 ± 29.2 | <0.0001 | 145.51 ± 49.3 | 89.84 ± 16.4 | 0.0006 | 0.0384 | 0.4132 |
| Total Cholesterol | 208.72 ± 45.1 | 132.27 ± 24.3 | <0.0001 | 195.23 ± 28.6 | 118.58 ± 19.3 | 0.0002 | 0.5294 | 0.2939 |
| HDL | 41.45 ± 13.0 | 54.97 ± 5.7 | 0.0075 | 48.09 ± 12.6 | 52.32 ± 11.2 | 0.0284 | 0.3418 | 0.6037 |
| LDL | 129.27 ± 29.9 | 95.63 ± 13.1 | <0.0001 | 134.28 ± 30.2 | 97.66 ± 21.2 | 0.0012 | 0.6303 | 0.7152 |
| Parameters | Severe Obesity Bariatric Surgery Group (n = 29) | p | Bariatric Surgery Group Metabolic Syndrome (n = 21) | p | p | |||
|---|---|---|---|---|---|---|---|---|
| Pre-BS | Post-BS | Pre-BS | Post-BS | Pre-BS | Post-BS | |||
| Adip | 0.33 ± 0.3 | 1.23 ± 0.4 | <0.0001 | 0.42 ± 0.3 | 1.28 ± 0.5 | 0.0018 | 0.345 | 0.797 |
| Lep | 1.83 ± 0.5 | 0.32 ± 0.3 | <0.0001 | 2.01 ± 0.5 | 0.52 ± 0.4 | 0.0015 | 0.388 | 0.124 |
| Adip/Lep | 0.16 [0.04–0.041] | 2.70 [1.52–5.4] | 0.0053 | 0.1 [0.03–0.35] | 10.2 [2.31–23.57] | 0.0084 | 0.548 | 0.192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, S.M.B.P.; Bachi, A.L.L.; Jirjos, E.I.; Malheiros, C.A.; Vencio, S.; Alves, V.L.S.; Sousa, A.R.T.; Felipe, L.A.; Perez, E.A.; Lino, M.E.M.; et al. Roux-en-Y Gastric Bypass Improves Adiponectin to Leptin Ratio and Inflammatory Profile in Severely Obese Women with and without Metabolic Syndrome: A Randomized Controlled Trial. Nutrients 2023, 15, 3312. https://doi.org/10.3390/nu15153312
Moreira SMBP, Bachi ALL, Jirjos EI, Malheiros CA, Vencio S, Alves VLS, Sousa ART, Felipe LA, Perez EA, Lino MEM, et al. Roux-en-Y Gastric Bypass Improves Adiponectin to Leptin Ratio and Inflammatory Profile in Severely Obese Women with and without Metabolic Syndrome: A Randomized Controlled Trial. Nutrients. 2023; 15(15):3312. https://doi.org/10.3390/nu15153312
Chicago/Turabian StyleMoreira, Sandra M. B. P., André L. L. Bachi, Elias I. Jirjos, Carlos A. Malheiros, Sergio Vencio, Vera L. S. Alves, Alan R. T. Sousa, Lucenda A. Felipe, Eduardo A. Perez, Maria E. M. Lino, and et al. 2023. "Roux-en-Y Gastric Bypass Improves Adiponectin to Leptin Ratio and Inflammatory Profile in Severely Obese Women with and without Metabolic Syndrome: A Randomized Controlled Trial" Nutrients 15, no. 15: 3312. https://doi.org/10.3390/nu15153312
APA StyleMoreira, S. M. B. P., Bachi, A. L. L., Jirjos, E. I., Malheiros, C. A., Vencio, S., Alves, V. L. S., Sousa, A. R. T., Felipe, L. A., Perez, E. A., Lino, M. E. M., Souza, S. K. A., Santos, J. M. B., Oliveira, M. C., Fonseca, A. L., Silva, C. H. M., Vieira, R. P., Insalaco, G., Freitas Júnior, W. R., & Oliveira, L. V. F. (2023). Roux-en-Y Gastric Bypass Improves Adiponectin to Leptin Ratio and Inflammatory Profile in Severely Obese Women with and without Metabolic Syndrome: A Randomized Controlled Trial. Nutrients, 15(15), 3312. https://doi.org/10.3390/nu15153312