
Nutritional Supplement Use in a UK High-Performance Swimming Club


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Data Groups for Analysis
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Supplement Type and Prevalence
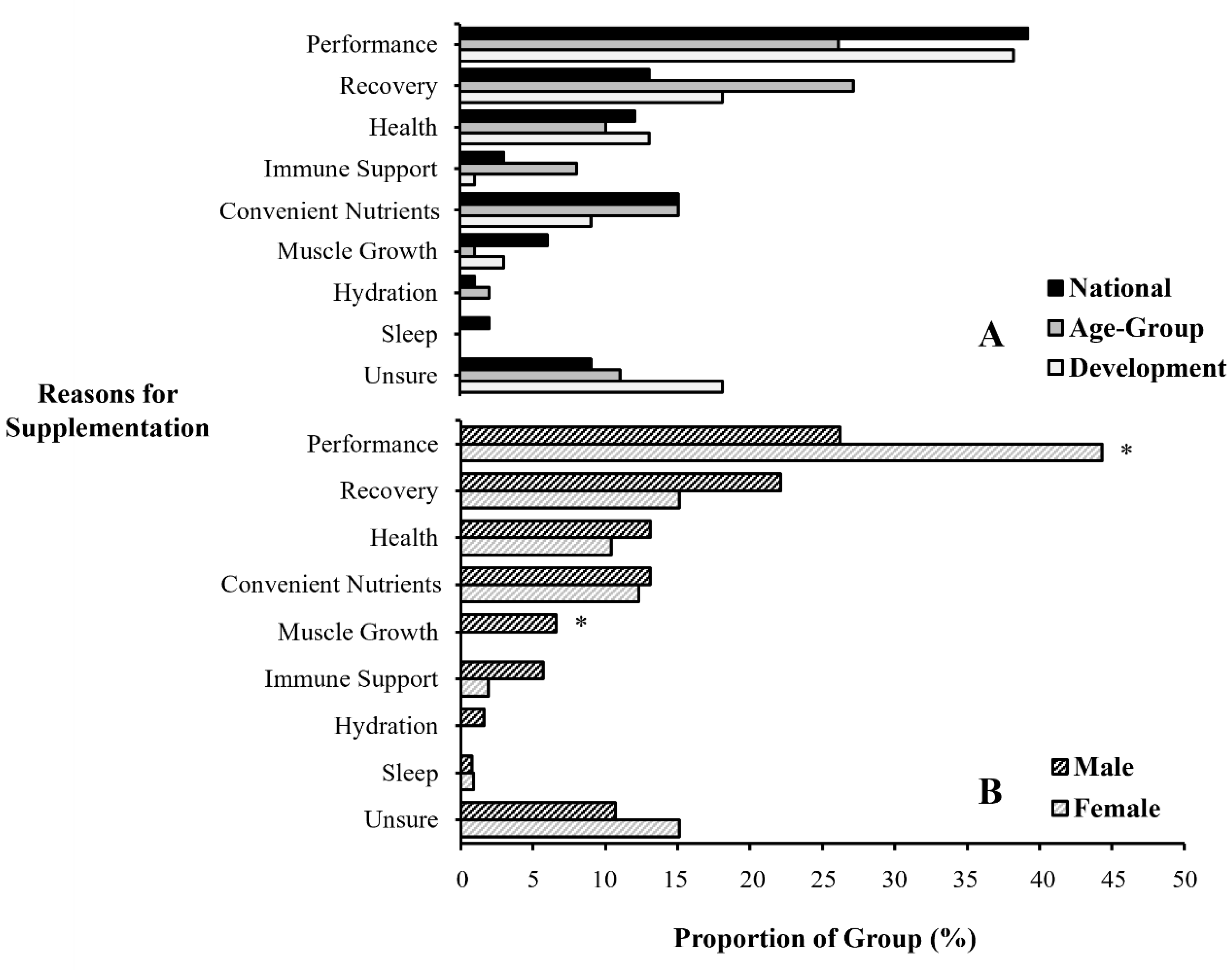
3.3. Reasons for Supplement Use
3.4. Information Sources
3.5. Supplement Frequency
3.6. Supplement Sources
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef] [PubMed]
- Garthe, I.; Maughan, R.J. Athletes and supplements: Prevalence and perspectives. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Winterstein, A.P.; Storrs, C.M. Herbal supplements: Considerations for the athletic trainer. J. Athl. Train. 2001, 36, 425–432. [Google Scholar]
- Shaw, G.; Slater, G.; Burke, L.M. Supplement use of elite Australian swimmers. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 249–258. [Google Scholar] [CrossRef]
- Mettler, S.; Lehner, G.; Morgan, G. Widespread supplement intake and use of poor quality information in elite adolescent Swiss athletes. Int. J. Sport Nutr. Exerc. Metab. 2022, 32, 41–48. [Google Scholar] [CrossRef]
- Ulery, J.A.; Melton, B.F.; Bland, H.; Riggs, A.J. Associations between health status, training level, motivations for exercise, and supplement use among recreational runners. J. Diet Suppl. 2022, 19, 640–655. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, B.; Kazlauskas, R. Medication use in athletes selected for doping control at the Sydney Olympics (2000). Clin. J. Sport Med. 2003, 13, 33–40. [Google Scholar] [CrossRef]
- Huang, S.H.; Johnson, K.; Pipe, A.L. The use of dietary supplements and medications by Canadian athletes at the Atlanta and Sydney Olympic Games. Clin. J. Sport Med. 2006, 16, 27–33. [Google Scholar] [CrossRef]
- Baylis, A.; Cameron-Smith, D.; Burke, L.M. Inadvertent doping through supplement use by athletes: Assessment and management of the risk in Australia. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 365–383. [Google Scholar] [CrossRef]
- Shaw, G.; Slater, G.; Burke, L.M. Changes in the supplementation practices of elite Australian swimmers over 11 years. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 565–571. [Google Scholar] [CrossRef]
- Jovanov, P.; Đorđić, V.; Obradović, B.; Barak, O.; Pezo, L.; Marić, A.; Sakač, M. Prevalence, knowledge and attitudes towards using sports supplements among young athletes. J. Int. Soc. Sports Nutr. 2019, 16, 27. [Google Scholar] [CrossRef]
- Moreno, B.; Veiga, S.; Sánchez-Oliver, A.J.; Domínguez, R.; Morencos, E. Analysis of sport supplement consumption by competitive swimmers according to sex and competitive level. Nutrients 2022, 14, 3218. [Google Scholar] [CrossRef] [PubMed]
- Dascombe, B.J.; Karunaratna, M.; Cartoon, J.; Fergie, B.; Goodman, C. Nutritional supplementation habits and perceptions of elite athletes within a state-based sporting institute. J. Sci. Med. Sport 2010, 13, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Berning, J.R.; Troup, J.P.; VanHandel, P.J.; Daniels, J.; Daniels, N. The nutritional habits of young adolescent swimmers. Int. J. Sport Nutr. 1991, 1, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.C.; Ward, K.D.; Mirza, B.; Slawson, D.L.; McClanahan, B.S.; Vukadinovich, C. Comparison of nutritional intake in US adolescent swimmers and non-athletes. Health 2012, 4, 873–880. [Google Scholar] [CrossRef]
- Martínez, S.; Pasquarelli, B.N.; Romaguera, D.; Arasa, C.; Tauler, P.; Aguiló, A. Anthropometric characteristics and nutritional profile of young amateur swimmers. J. Strength Cond. Res. 2011, 25, 1126–1133. [Google Scholar] [CrossRef]
- Parnell, J.A.; Wiens, K.P.; Erdman, K.A. Dietary intakes and supplement use in pre-adolescent and adolescent Canadian athletes. Nutrients 2016, 8, 526. [Google Scholar] [CrossRef]
- Petróczi, A.; Naughton, D.P.; Pearce, G.; Bailey, R.; Bloodworth, A.; McNamee, M. Nutritional supplement use by elite young UK athletes: Fallacies of advice regarding efficacy. J. Int. Soc. Sports Nutr. 2008, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Close, G.L.; Kasper, A.M.; Walsh, N.P.; Maughan, R.J. “Food first but not always food only”: Recommendations for using dietary supplements in sport. Int. J. Sport Nutr. Exerc. Metab. 2022, 32, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Derave, W.; Tipton, K.D. Dietary supplements for aquatic sports. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 437–449. [Google Scholar] [CrossRef]
- Desbrow, B.; McCormack, J.; Burke, L.M.; Cox, G.R.; Fallon, K.; Hislop, M.; Logan, R.; Marino, N.; Sawyer, S.M.; Shaw, G.; et al. Sports Dietitians Australia position statement: Sports nutrition for the adolescent athlete. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 570–584. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Jiménez-Alfageme, R.; Domínguez, R.; Sanchez-Oliver, A.J.; Tapia-Castillo, P.; Martínez-Sanz, J.M.; Sospedra, I. Analysis of the consumption of sports supplements in open water swimmers according to the competitive level. Nutrients 2022, 14, 5211. [Google Scholar] [CrossRef]
- Foo, W.L.; Faghy, M.A.; Sparks, A.; Newbury, J.W.; Gough, L.A. The effects of a nutrition education intervention on sports nutrition knowledge during a competitive season in highly trained adolescent swimmers. Nutrients 2021, 13, 2713. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Simič, V.; Mohorko, N. Nutritional strategies of Slovenian national junior swimming team. Ann. Kinesiol. 2018, 9, 15–34. [Google Scholar] [CrossRef][Green Version]
- Shaw, G.; Boyd, K.T.; Burke, L.M.; Koivisto, A. Nutrition for swimming. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 360–372. [Google Scholar] [CrossRef]
- Braun, H.; Koehler, K.; Geyer, H.; Kleiner, J.; Mester, J.; Schanzer, W. Dietary supplement use among elite young German athletes. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 97–109. [Google Scholar] [CrossRef]
- Wiens, K.; Erdman, K.A.; Stadnyk, M.; Parnell, J.A. Dietary supplement usage, motivation, and education in young, Canadian athletes. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 613–622. [Google Scholar] [CrossRef]
- Sanchez-Oliver, A.J. Suplementación Nutricional en la Actividad Físico-Deportiva: Análisis de la Calidad del Suplemento Proteico Consumido; Universidad de Granada: Granada, Spain, 2012. [Google Scholar]
- Lakens, D. Sample size justification. Collabra Psychol. 2022, 8, 33267. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measure | National (n = 11) | Age-Group (n = 13) | Development (n = 20) | Males (n = 21) | Females (n = 23) | Combined (n = 44) |
|---|---|---|---|---|---|---|
| Age (years) | 20 ± 2 | 15 ± 1 | 13 ± 1 | 16 ± 3 | 15 ± 3 | 15 ± 3 |
| Years competitive | 9 ± 2 *# | 5 ± 1 * | 3 ± 1 | 5 ± 3 | 5 ± 3 | 5 ± 3 |
| Weekly training sessions | 6.9 ± 1.2 * | 6.2 ± 0.8 * | 5.7 ± 0.5 | 6.0 ± 0.7 | 6.3 ± 1.1 | 6.2 ± 0.9 |
| Weekly training hours | 17.6 ± 3.2 * | 15.8 ± 2.4 * | 12.3 ± 1.2 | 14.4 ± 2.3 | 14.9 ± 3.8 | 14.6 ± 3.1 |
| WA points | 698 ± 59 *# | 622 ± 67 * | 483 ± 69 | 555 ± 123 | 598 ± 99 | 578 ± 112 |
| Category/Individual Supplements | Overall (n = 44) | National (n = 11) | Age-Group (n = 13) | Development (n = 20) | Males (n = 21) | Females (n = 23) |
|---|---|---|---|---|---|---|
| Total (supplements) | 5.2 ± 2.9 | 8.1 ± 3.4 ab | 4.8 ± 2.0 | 3.9 ± 1.7 | 5.9 ± 2.7 | 4.6 ± 2.9 |
| Sports (supplements) | 2.5 ± 1.0 *# | 2.7 ± 1.7 | 2.6 ± 0.7 | 2.6 ± 0.9 | 2.9 ± 0.8 † | 2.2 ± 1.0 |
| Dextrose/maltodextrin (%) | 0 | 0 | 0 | 5 | 0 | 4 |
| Electrolytes (%) | 18 | 18 | 38 | 5 | 29 | 9 |
| Liquid meals (%) | 9 | 18 | 0 | 10 | 0 | 17 ‡ |
| Protein bars (%) | 43 | 36 | 54 | 40 | 57 | 30 |
| Protein-enhanced food (%) | 45 | 45 | 46 | 45 | 62 ‡ | 30 |
| Protein powder (%) † | 45 | 82 | 54 | 20 | 52 | 39 |
| Sports bars (%) | 2 | 0 | 0 | 5 | 0 | 4 |
| Sports drinks (%) † | 68 | 27 | 62 | 95 | 67 | 70 |
| Sports gels (%) | 18 | 9 | 8 | 30 | 19 | 17 |
| Ergogenic (supplements) | 0.8 ± 1.4 | 2.4 ± 1.4 ab | 0.5 ± 0.5 b | 0.1 ± 0.2 | 0.8 ± 1.7 | 0.9 ± 1.2 |
| Beetroot juice (%) | 5 | 9 | 8 | 0 | 10 | 0 |
| Beta-alanine (%) † | 14 | 45 | 8 | 0 | 14 | 13 |
| Caffeine anhydrous (%) † | 30 | 82 | 23 | 5 | 14 | 43 ‡ |
| Caffeine drinks/gels (%) † | 9 | 36 | 0 | 0 | 10 | 9 |
| Citrulline malate (%) | 2 | 9 | 0 | 0 | 5 | 0 |
| Creatine monohydrate (%) † | 16 | 55 | 8 | 0 | 19 | 13 |
| Sodium bicarbonate (%) † | 9 | 36 | 0 | 0 | 10 | 9 |
| Health (supplements) | 1.8 ± 1.6 * | 3.0 ± 1.3 ab | 1.7 ± 1.8 | 1.3 ± 1.3 | 2.2 ± 1.4 | 1.5 ± 1.7 |
| Ginger (%) | 2 | 0 | 8 | 0 | 5 | 0 |
| Iron (%) | 20 | 27 | 15 | 20 | 24 | 17 |
| Magnesium (%) † | 5 | 18 | 0 | 0 | 10 | 0 |
| Melatonin (%) | 2 | 9 | 0 | 0 | 0 | 4 |
| Multi-vitamin (%) | 41 | 36 | 31 | 50 | 62 ‡ | 22 |
| Omega-3 fatty acids (%) † | 20 | 55 | 0 | 15 | 19 | 22 |
| Probiotics (%) | 20 | 9 | 38 | 15 | 24 | 17 |
| Vitamin C (%) | 18 | 27 | 31 | 5 | 24 | 13 |
| Vitamin D3 (%) † | 39 | 73 | 38 | 20 | 38 | 39 |
| Zinc (%) † | 11 | 45 | 0 | 0 | 10 | 13 |
| Information Source | Overall (n = 228) | National (n = 89) | Age-Group (n = 62) | Development (n = 77) | Males (n = 122) | Females (n = 106) |
|---|---|---|---|---|---|---|
| Performance nutritionist (%) * | 33 | 51 | 50 | 0 | 20 | 48 # |
| Swim coach (%) * | 6 | 12 | 3 | 1 | 7 | 5 |
| Parent/guardian (%) * | 42 | 16 | 40 | 74 | 50 # | 33 |
| NGB (%) | 3 | 4 | 2 | 1 | 4 | 1 |
| Medical doctor (%) | 3 | 1 | 3 | 4 | 4 | 1 |
| Other coach (%) | 4 | 7 | 0 | 3 | 6 # | 1 |
| Teammate (%) | 3 | 3 | 0 | 4 | 2 | 2 |
| Friends and siblings (%) | 2 | 2 | 0 | 4 | 1 | 0 |
| Media (%) * | 3 | 1 | 0 | 8 | 3 | 5 |
| Self-Research (%) | 2 | 2 | 2 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Newbury, J.W.; Sparks, S.A.; Cole, M.; Kelly, A.L.; Gough, L.A. Nutritional Supplement Use in a UK High-Performance Swimming Club. Nutrients 2023, 15, 3306. https://doi.org/10.3390/nu15153306
Newbury JW, Sparks SA, Cole M, Kelly AL, Gough LA. Nutritional Supplement Use in a UK High-Performance Swimming Club. Nutrients. 2023; 15(15):3306. https://doi.org/10.3390/nu15153306
Chicago/Turabian StyleNewbury, Josh W., S. Andy Sparks, Matthew Cole, Adam L. Kelly, and Lewis A. Gough. 2023. "Nutritional Supplement Use in a UK High-Performance Swimming Club" Nutrients 15, no. 15: 3306. https://doi.org/10.3390/nu15153306
APA StyleNewbury, J. W., Sparks, S. A., Cole, M., Kelly, A. L., & Gough, L. A. (2023). Nutritional Supplement Use in a UK High-Performance Swimming Club. Nutrients, 15(15), 3306. https://doi.org/10.3390/nu15153306