
The Association between Nutrition, Physical Activity, and Cardiometabolic Health at 6 Months following a Hypertensive Pregnancy: A BP2 Sub-Study

 and
and
Abstract
:1. Introduction
Aims
- Describe lifestyle behaviours (nutrition and physical activity) of women 6 months post-HDP.
- Compare lifestyle behaviours between four HDP subgroups (CH, GH, preeclampsia, and CH + PE).
- Identify associations between lifestyle behaviours and cardiometabolic outcomes including body mass index (BMI), waist circumference, and blood pressure (BP).
2. Materials and Methods
2.1. Ethics Approval
2.2. Participant Eligibility and Recruitment
2.3. Sub-Study Data Collection
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
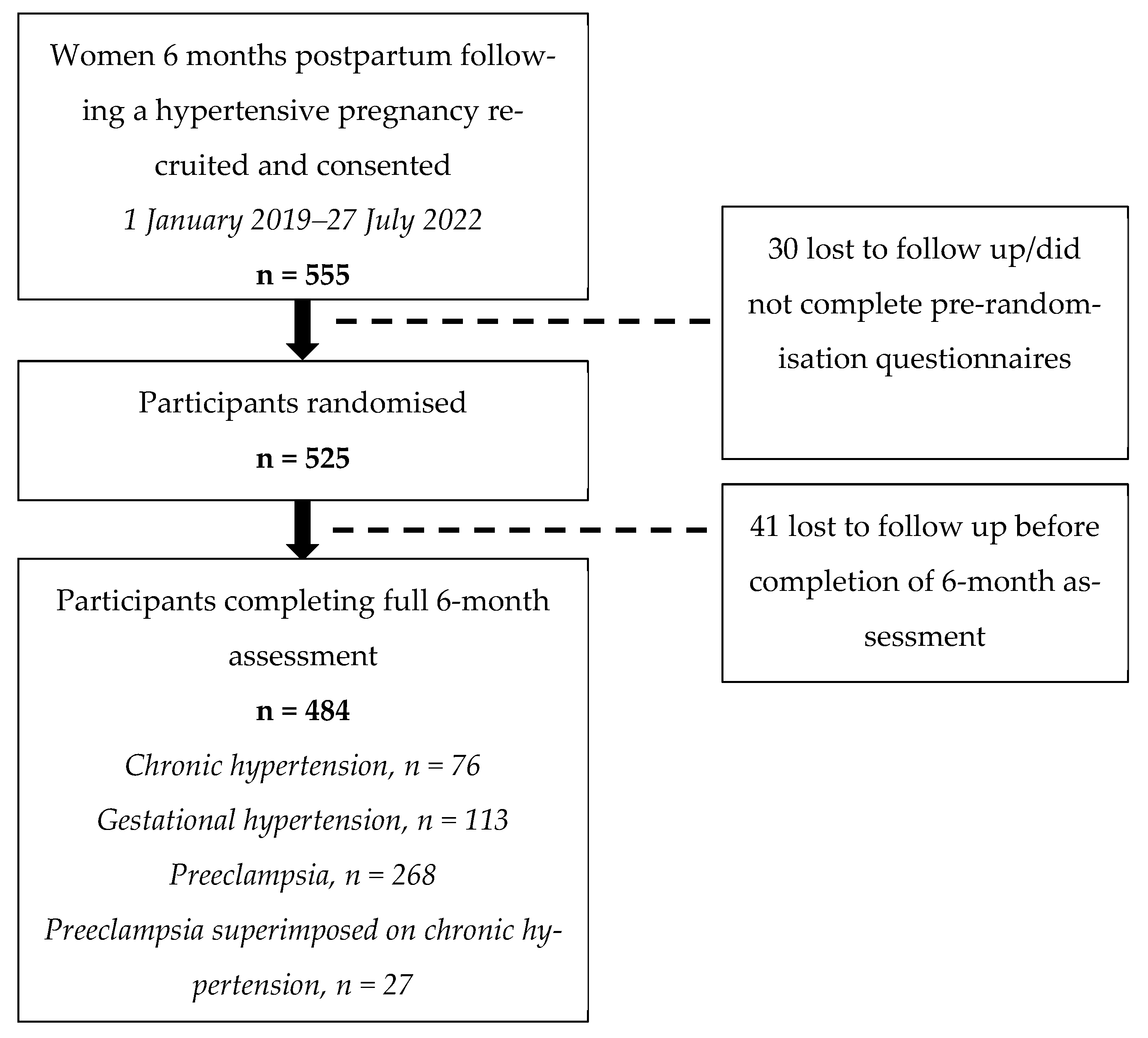
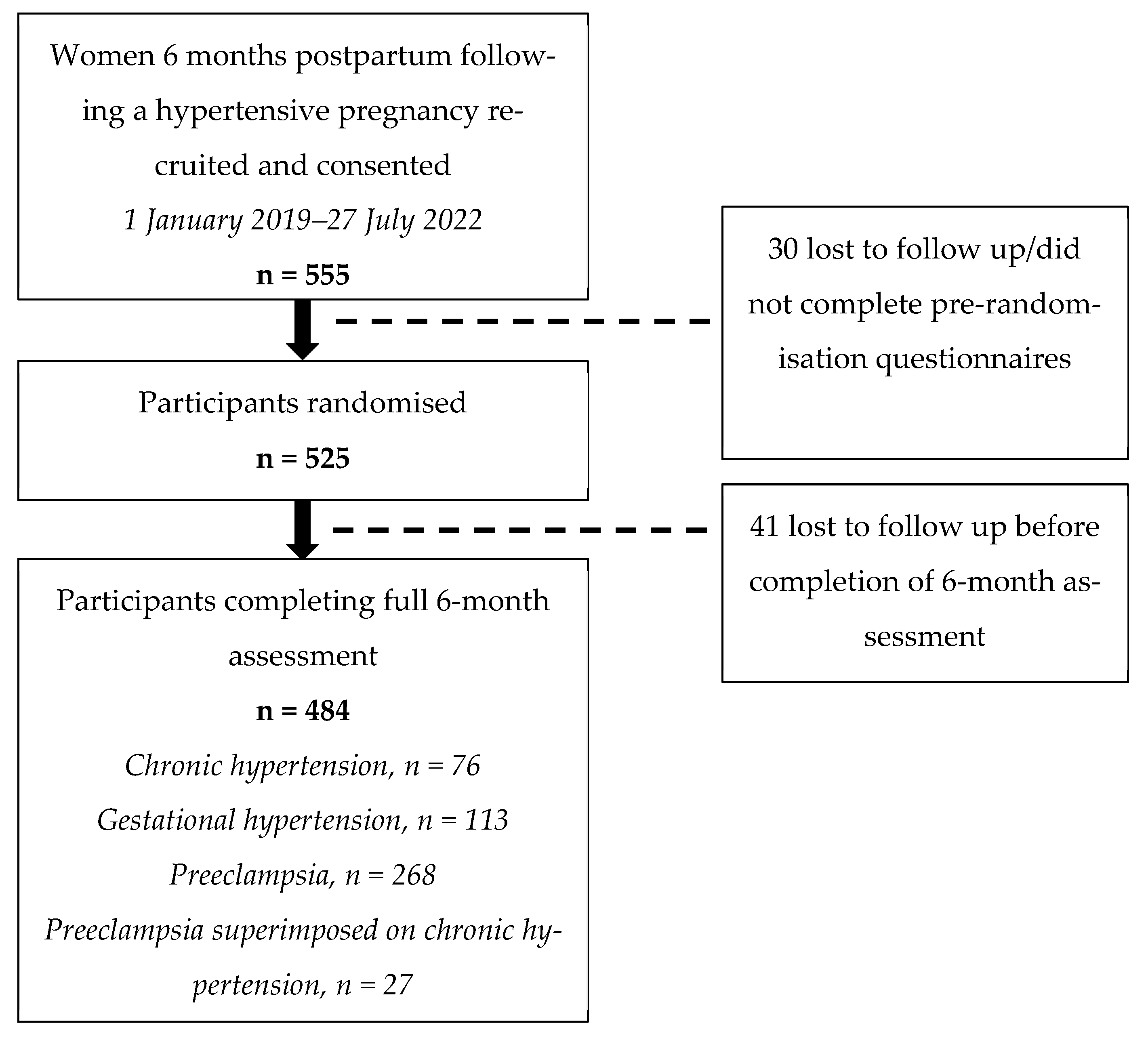
3.1. Study Population Characteristics
3.2. Primary Lifestyle Outcomes
3.2.1. Nutrition
3.2.2. Physical Activity
3.3. Weight Outcomes
3.4. Correlations between Lifestyle Behaviours and Cardiometabolic Outcomes
4. Discussion
4.1. Nutrition
4.2. Physical Activity
4.3. Weight Outcomes
4.4. Correlations between Lifestyle Behaviours and Weight Outcomes
4.4.1. Nutrition
4.4.2. Physical Activity
4.5. Limitations
4.6. Strengths and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef] [PubMed]
- Melchiorre, K.; Thilaganathan, B.; Giorgione, V.; Ridder, A.; Memmo, A.; Khalil, A. Hypertensive disorders of pregnancy and future cardiovascular health. Front. Cardiovasc. Med. 2020, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, B.; Hanson, C.; Sharma, S.; Magee, L.; von Dadelszen, P. Epidemiology of the hypertensive disorders of pregnancy. In The FIGO Textbook of Pregnancy Hypertension: An Evidence-Based Guide to Monitoring, Prevention and Management; Magee, L., Von Dadelszen, P., Stones, W., Matthews, M., Eds.; The Global Library of Women’s Medicine: London, UK, 2016; pp. 63–74. [Google Scholar]
- Siritharan, S.S.; Henry, A.; Gow, M.L.; Roberts, L.M.; Yao, A.; Ojurovic, M.; O’Sullivan, A.J. Maternal macro- and micronutrient intake six months after hypertensive versus normotensive pregnancy: Is poor diet quality contributing to future cardiometabolic disease risk? Pregnancy Hypertens. 2021, 23, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Seely, E.W.; Ecker, J. Chronic hypertension in pregnancy. N. Engl. J. Med. 2011, 365, 439–446. [Google Scholar] [CrossRef]
- Henry, A.; Arnott, C.; Makris, A.; Davis, G.; Hennessy, A.; Beech, A.; Pettit, F.; Se Homer, C.; Craig, M.E.; Roberts, L.; et al. Blood pressure postpartum (BP2) RCT protocol: Follow-up and lifestyle behaviour change strategies in the first 12 months after hypertensive pregnancy. Pregnancy Hypertens. 2020, 22, 1–6. [Google Scholar] [CrossRef]
- Poon, L.C.; Nguyen-Hoang, L.; Smith, G.N.; Bergman, L.; O’Brien, P.; Hod, M.; Okong, P.; Kapur, A.; Maxwell, C.V.; McIntyre, H.D.; et al. Hypertensive disorders of pregnancy and long-term cardiovascular health: FIGO Best Practice Advice. Int. J. Gynaecol. Obstet. 2023, 160 (Suppl. S1), 22–34. [Google Scholar] [CrossRef]
- Garovic, V.D.; White, W.M.; Vaughan, L.; Saiki, M.; Parashuram, S.; Garcia-Valencia, O.; Weissgerber, T.L.; Milic, N.; Weaver, A.; Mielke, M.M. Incidence and long-term outcomes of hypertensive disorders of pregnancy. J. Am. Coll. Cardiol. 2020, 75, 2323–2334. [Google Scholar] [CrossRef]
- Parikh, N.I.; Gonzalez, J.M.; Anderson, C.A.M.; Judd, S.E.; Rexrode, K.M.; Hlatky, M.A.; Gunderson, E.P.; Stuart, J.J.; Vaidya, D. Adverse pregnancy outcomes and cardiovascular disease risk: Unique opportunities for cardiovascular disease prevention in women: A scientific statement from the American Heart Association. Circulation 2021, 143, e902–e916. [Google Scholar] [CrossRef]
- Magee, L.A.; Brown, M.A.; Hall, D.R.; Gupte, S.; Hennessy, A.; Karumanchi, S.A.; Kenny, L.C.; McCarthy, F.; Myers, J.; Poon, L.C.; et al. The 2021 International Society for the Study of Hypertension in Pregnancy classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2022, 27, 148–169. [Google Scholar] [CrossRef]
- Theilen, L.H.; Meeks, H.; Fraser, A.; Esplin, M.S.; Smith, K.R.; Varner, M.W. Long-term mortality risk and life expectancy following recurrent hypertensive disease of pregnancy. Am. J. Obstet. Gynecol. 2018, 219, 107.e1–107.e7. [Google Scholar] [CrossRef] [Green Version]
- Behrens, I.; Basit, S.; Melbye, M.; Lykke, J.A.; Wohlfahrt, J.; Bundgaard, H.; Thilaganathan, B.; Boyd, H.A. Risk of post-pregnancy hypertension in women with a history of hypertensive disorders of pregnancy: Nationwide cohort study. BMJ 2017, 358, j3078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groenhof, T.K.J.; van Rijn, B.B.; Franx, A.; Roeters van Lennep, J.E.; Bots, M.L.; Lely, A.T. Preventing cardiovascular disease after hypertensive disorders of pregnancy: Searching for the how and when. Eur. J. Prev. Cardiol. 2017, 24, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Berks, D.; Hoedjes, M.; Raat, H.; Duvekot, J.J.; Steegers, E.A.; Habbema, J.D. Risk of cardiovascular disease after pre-eclampsia and the effect of lifestyle interventions: A literature-based study. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 924–931. [Google Scholar] [CrossRef]
- Cardiovascular Diseases. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 18 July 2023).
- Hauspurg, A.; Countouris, M.E.; Catov, J.M. Hypertensive disorders of pregnancy and future maternal health: How can the evidence guide postpartum management? Curr. Hypertens. Rep. 2019, 21, 96. [Google Scholar] [CrossRef] [PubMed]
- Berks, D.; Hoedjes, M.; Raat, H.; Franx, A.; Looman, C.W.N.; Van Oostwaard, M.F.; Papatsonis, D.N.M.; Duvekot, J.J.; Steegers, E.A.P. Feasibility and effectiveness of a lifestyle intervention after complicated pregnancies to improve risk factors for future cardiometabolic disease. Pregnancy Hypertens. 2019, 15, 98–107. [Google Scholar] [CrossRef]
- Roth, H.; LeMarquand, G.; Henry, A.; Homer, C. Assessing Knowledge Gaps of Women and Healthcare Providers Concerning Cardiovascular Risk After Hypertensive Disorders of Pregnancy-A Scoping Review. Front. Cardiovasc. Med. 2019, 6, 178. [Google Scholar] [CrossRef]
- Roth, H.; Homer, C.S.E.; Arnott, C.; Roberts, L.; Brown, M.; Henry, A. Assessing knowledge of healthcare providers concerning cardiovascular risk after hypertensive disorders of pregnancy: An Australian national survey. BMC Pregnancy Childbirth 2020, 20, 717. [Google Scholar] [CrossRef]
- Dipietro, L.; Evenson, K.R.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E. Benefits of physical activity during pregnancy and postpartum: An umbrella review. Med. Sci. Sports Exerc. 2019, 51, 1292–1302. [Google Scholar] [CrossRef]
- Spencer, L.; Rollo, M.; Hauck, Y.; MacDonald-Wicks, L.; Wood, L.; Hutchesson, M.; Giglia, R.; Smith, R.; Collins, C. The effect of weight management interventions that include a diet component on weight-related outcomes in pregnant and postpartum women: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 88–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rich-Edwards, J.W.; Stuart, J.J.; Skurnik, G.; Roche, A.T.; Tsigas, E.; Fitzmaurice, G.M.; Wilkins-Haug, L.E.; Levkoff, S.E.; Seely, E.W. Randomized trial to reduce cardiovascular risk in women with recent preeclampsia. J. Women’s Health 2019, 28, 1493–1504. [Google Scholar] [CrossRef]
- Muñóz Muñóz, A.; Gómez-Cantarino, S.; De Dios Aguado, M.L.M.; Velasco Abellán, M.; González López, B.; Molina Gallego, B.; González Pascual, J.L.; Arias Palencia, N.M. Nutritional habits and levels of physical activity during pregnancy, birth and the postpartum period of women in Toledo (Spain): Study protocol for a two-year prospective cohort study (the PrePaN study). BMJ Open 2019, 9, e029487. [Google Scholar] [CrossRef]
- Shay, C.M.; Stamler, J.; Dyer, A.R.; Brown, I.J.; Chan, Q.; Elliott, P.; Zhao, L.; Okuda, N.; Miura, K.; Daviglus, M.L.; et al. Nutrient and food intakes of middle-aged adults at low risk of cardiovascular disease: The international study of macro-/micronutrients and blood pressure (INTERMAP). Eur. J. Nutr. 2012, 51, 917–926. [Google Scholar] [CrossRef] [Green Version]
- Chiu, H.F.; Venkatakrishnan, K.; Golovinskaia, O.; Wang, C.K. Impact of Micronutrients on Hypertension: Evidence from Clinical Trials with a Special Focus on Meta-Analysis. Nutrients 2021, 13, 588. [Google Scholar] [CrossRef] [PubMed]
- Janmohamed, R.; Montgomery-Fajic, E.; Sia, W.; Germaine, D.; Wilkie, J.; Khurana, R.; Nerenberg, K.A. Cardiovascular risk reduction and weight management at a hospital-based postpartum preeclampsia clinic. J. Obstet. Gynaecol. Can. 2015, 37, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Hutchesson, M.; Campbell, L.; Leonard, A.; Vincze, L.; Shrewsbury, V.; Collins, C.; Taylor, R. Do modifiable risk factors for cardiovascular disease post-pregnancy influence the association between hypertensive disorders of pregnancy and cardiovascular health outcomes? A systematic review of observational studies. Pregnancy Hypertens. 2022, 27, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Lui, N.A.; Jeyaram, G.; Henry, A. Postpartum interventions to reduce long-term cardiovascular disease risk in women after hypertensive disorders of pregnancy: A systematic review. Front. Cardiovasc. Med. 2019, 6, 160. [Google Scholar] [CrossRef]
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines, Obesity Expert Panel. Executive summary: Guidelines (2013) for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a systematic review from the Obesity Expert Panel, 2013. Obesity (Silver Spring) 2014, 22 (Suppl. S2), S5–S39. [CrossRef] [Green Version]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut off Points. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- NSW Population Health Surveys. Available online: https://www.health.nsw.gov.au/surveys/Pages/default.aspx (accessed on 22 March 2022).
- Dubasi, S.K.; Ranjan, P.; Arora, C.; Vikram, N.K.; Dwivedi, S.N.; Singh, N.; Kaloiya, G.S.; Shalimar. Questionnaire to assess adherence to diet and exercise advices for weight management in lifestyle-related diseases. J. Fam. Med. Prim. Care 2019, 8, 689–694. [Google Scholar] [CrossRef]
- van der Pligt, P.; Olander, E.K.; Ball, K.; Crawford, D.; Hesketh, K.D.; Teychenne, M.; Campbell, K. Maternal dietary intake and physical activity habits during the postpartum period: Associations with clinician advice in a sample of Australian first time mothers. BMC Pregnancy Childbirth 2016, 16, 27. [Google Scholar] [CrossRef] [Green Version]
- Wiltheiss, G.A.; Lovelady, C.A.; West, D.G.; Brouwer, R.J.N.; Krause, K.M.; Østbye, T. Diet quality and weight change among overweight and obese postpartum women enrolled in a behavioral intervention program. J. Acad. Nutr. Diet 2013, 113, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Fowles, E.R.; Walker, L.O. Correlates of dietary quality and weight retention in postpartum women. J. Community Health Nurs. 2006, 23, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Bassett-Gunter, R.L.; Levy-Milne, R.; Naylor, P.J.; Symons Downs, D.; Benoit, C.; Warburton, D.E.; Blanchard, C.M.; Rhodes, R.E. Oh baby! Motivation for healthy eating during parenthood transitions: A longitudinal examination with a theory of planned behavior perspective. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timperio, A.; Salmon, J.; Crawford, D. Validity and reliability of a physical activity recall instrument among overweight and non-overweight men and women. J. Sci. Med. Sport 2003, 6, 477–491. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Giroux, I.; Sopper, M.M.; Mottola, M.F. Postpartum exercise regardless of intensity improves chronic disease risk factors. Med. Sci. Sports Exerc. 2011, 43, 951–958. [Google Scholar] [CrossRef]
- Makama, M.; Awoke, M.A.; Skouteris, H.; Moran, L.J.; Lim, S. Barriers and facilitators to a healthy lifestyle in postpartum women: A systematic review of qualitative and quantitative studies in postpartum women and healthcare providers. Obes. Rev. 2021, 22, e13167. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.A.; Lappen, H.; Bihuniak, J.D. Barriers and facilitators to healthy eating and physical activity postpartum: A qualitative systematic review. J. Acad. Nutr. Diet 2022, 122, 602–613.e602. [Google Scholar] [CrossRef]
- Almli, I.; Haugdahl, H.S.; Sandsæter, H.L.; Rich-Edwards, J.W.; Horn, J. Implementing a healthy postpartum lifestyle after gestational diabetes or preeclampsia: A qualitative study of the partner’s role. BMC Pregnancy Childbirth 2020, 20, 66. [Google Scholar] [CrossRef]
- Pregnancy Care Guidelines: Weight and Body Mass Index. Available online: https://www.health.gov.au/resources/pregnancy-care-guidelines/part-d-clinical-assessments/weight-and-body-mass-index (accessed on 18 June 2023).
- McLennan, S.L.; Henry, A.; Roberts, L.M.; Siritharan, S.S.; Ojurovic, M.; Yao, A.; Davis, G.K.; Mangos, G.; Pettit, F.; Brown, M.A.; et al. Maternal Adiposity and Energy Balance After Normotensive and Preeclamptic Pregnancies. J. Clin. Endocrinol. Metab. 2021, 106, e2941–e2952. [Google Scholar] [CrossRef]
- Bijlholt, M.; Ameye, L.; van Uytsel, H.; Devlieger, R.; Bogaerts, A. Evolution of postpartum weight and body composition after excessive gestational weight gain: The role of lifestyle behaviors-data from the INTER-ACT Control Group. Int. J. Environ. Res. Public Health 2021, 18, 6344. [Google Scholar] [CrossRef]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Li, Y.; Wang, H.; Wang, K.; Wang, W.; Dong, F.; Qian, Y.; Gong, H.; Xu, G.; Li, G.; Pan, L.; et al. Optimal body fat percentage cut-off values for identifying cardiovascular risk factors in Mongolian and Han adults: A population-based cross-sectional study in Inner Mongolia, China. BMJ Open 2017, 7, e014675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, M.; Mayhew, L.; Richardson, J.; Rickayzen, B. Waist-to-height ratio is more predictive of years of life lost than body mass index. PLoS ONE 2014, 9, e103483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedayatnia, M.; Asadi, Z.; Zare-Feyzabadi, R.; Yaghooti-Khorasani, M.; Ghazizadeh, H.; Ghaffarian-Zirak, R.; Nosrati-Tirkani, A.; Mohammadi-Bajgiran, M.; Rohban, M.; Sadabadi, F.; et al. Dyslipidemia and cardiovascular disease risk among the MASHAD study population. Lipids Health Dis. 2020, 19, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajnik, C.S.; Katre, P.A.; Joshi, S.M.; Kumaran, K.; Bhat, D.S.; Lubree, H.G.; Memane, N.; Kinare, A.S.; Pandit, A.N.; Bhave, S.A.; et al. Higher glucose, insulin and insulin resistance (HOMA-IR) in childhood predict adverse cardiovascular risk in early adulthood: The Pune Children’s Study. Diabetologia 2015, 58, 1626–1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tano, S.; Kotani, T.; Ushida, T.; Yoshihara, M.; Imai, K.; Nakano-Kobayashi, T.; Moriyama, Y.; Iitani, Y.; Kinoshita, F.; Yoshida, S.; et al. Annual body mass index gain and risk of hypertensive disorders of pregnancy in a subsequent pregnancy. Sci. Rep. 2021, 11, 22519. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Arablou, T.; Jayedi, A.; Salehi-Abargouei, A. Adherence to the dietary approaches to stop hypertension (DASH) diet in relation to all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective cohort studies. Nutr. J. 2020, 19, 37. [Google Scholar] [CrossRef] [Green Version]
- Ardalan, M.R.; Rafieian-Kopaei, M. Antioxidant supplementation in hypertension. J. Renal. Inj. Prev. 2014, 3, 39–40. [Google Scholar] [CrossRef]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.K.; Appel, L.J.; Brands, M.; Howard, B.V.; Lefevre, M.; Lustig, R.H.; Sacks, F.; Steffen, L.M.; Wylie-Rosett, J. Dietary sugars intake and cardiovascular health: A scientific statement from the American Heart Association. Circulation 2009, 120, 1011–1020. [Google Scholar] [CrossRef] [Green Version]
- Gupta, L.; Khandelwal, D.; Dutta, D.; Kalra, S.; Lal, P.R.; Gupta, Y. The twin white herrings: Salt and sugar. Indian J. Endocrinol. Metab. 2018, 22, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Pinckard, K.; Baskin, K.K.; Stanford, K.I. Effects of exercise to improve cardiovascular health. Front. Cardiovasc. Med. 2019, 6, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, S.J.; Jung, M.H.; Ihm, S.H.; Yang, Y.J.; Youn, H.J. Effect of physical activity on the cardiometabolic profiles of non-obese and obese subjects: Results from the Korea National Health and Nutritional Examination Survey. PLoS ONE 2019, 14, e0208189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone Gibbs, B.; Hivert, M.F.; Jerome, G.J.; Kraus, W.E.; Rosenkranz, S.K.; Schorr, E.N.; Spartano, N.L.; Lobelo, F. Physical activity as a critical component of first-line treatment for elevated blood pressure or cholesterol: Who, what, and how?: A scientific statement from the American Heart Association. Hypertension 2021, 78, e26–e37. [Google Scholar] [CrossRef] [PubMed]
- Gow, M.L.; Rossiter, C.; Roberts, L.; Henderson, M.J.; Yang, L.; Roche, J.; Hayes, E.; Canty, A.; Denney-Wilson, E.; Henry, A. COVID-19, lifestyle behaviors and mental health: A mixed methods study of women 6 months following a hypertensive pregnancy. Front. Public Health 2022, 10, 1000371. [Google Scholar] [CrossRef]
- Roth, H.; Henry, A.; Roberts, L.; Hanley, L.; Homer, C.S.E. Exploring education preferences of Australian women regarding long-term health after hypertensive disorders of pregnancy: A qualitative perspective. BMC Women’s Health 2021, 21, 384. [Google Scholar] [CrossRef]

{kind=link}
| Demographic (Missing) | Total (n = 484) | CH (n = 76) | GH (n = 113) | Preeclampsia (n = 268) | CH + PE (n = 27) | p-Value |
|---|---|---|---|---|---|---|
| Number (%) | ||||||
| Ethnicity (0) | ||||||
| Caucasian | 285 (59) | 41 (54) | 79 (70) | 150 (56) | 15 (56) | 0.06 |
| Asian | 79 (16) | 18 (24) | 15 (13) | 39 (15) | 7 (26) | 0.1 |
| Aboriginal or Torres Strait Islander | 3 (1) | 0 (0) | 1 (1) | 2 (1) | 0 (0) | 0.84 |
| Polynesian | 8 (2) | 3 (4) | 0 (0) | 5 (2) | 0 (0) | 0.18 |
| European | 33 (7) | 2 (3) | 9 (8) | 21 (8) | 1 (4) | 0.37 |
| Middle Eastern | 9 (2) | 0 (0) | 1 (1) | 7 (3) | 1 (4) | 0.34 |
| African | 11 (2) | 4 (5) | 1 (1) | 6 (2) | 0 (0) | 0.2 |
| Other ⊚ | 53 (11) | 8 (11) | 6 (5) | 36 (13) | 3 (11) | 0.15 |
| Highest education (4) | 0.02 * | |||||
| University degree | 326 (68) | 42 (56) | 82 (74) | 180 (67) | 22 (82) | |
| Trade/certificate/diploma | 108 (23) | 18 (24) | 25 (23) | 61 (23) | 4 (15) | |
| Secondary school | 46 (10) | 15 (20) | 4 (4) | 26 (10) | 1 (4) | |
| Index pregnancy first baby (0) | 326 (67) | 35 (46) | 75 (66) | 205 (77) | 11 (41) | <0.001 * |
| Index pregnancy planned (3) | 384 (80) | 60 (79) | 92 (82) | 212 (80) | 20 (74) | 0.81 |
| Index pregnancy twin pregnancy (0) | 16 (3) | 0 (0) | 2 (2) | 14 (5) | 0 (0) | 0.06 |
| Gestation at HDP diagnosis (1) | <0.001 * | |||||
| Pre-existing | 39 (8) | 39 (51) | 0 (0) | 0 (0) | 0 (0) | |
| During pregnancy | 409 (85) | 37 (49) | 99 (88) | 246 (92) | 25 (93) | |
| Completed weeks—median (IQR) | 36.0 (6.0) | 15.0 (5.0) | 37.0 (4.0) | 36.0 (5.0) | 35.0 (7.0) | |
| Intrapartum | 5 (1) | 0 (0) | 2 (2) | 3 (1) | 0 (0) | |
| Postpartum | 31 (6) | 0 (0) | 12 (11) | 19 (7) | 2 (7) | |
| Median (IQR)⋄ | ||||||
| Index pregnancy BMI at first antenatal appointment (kg/m2) (5) | 25.0 (7.3) | 29.0 (8.6) | 25.1 (6.0) | 23.9 (6.9) | 25.6 (6.5) | <0.001 * |
| Overweight; BMI 25.0–29.9, n (%) | 130 (27) | 24 (32) | 34 (30) | 65 (24) | 7 (26) | |
| Obese; BMI ≥ 30, n (%) | 112 (23) | 31 (42) | 24 (21) | 50 (19) | 7 (26) | |
| Gestation at birth (completed weeks) (0) | 38.0 (3.0) | 38.0 (1.8) | 39.0 (1.0) | 37.0 (4.8) | 36.0 (4.0) | <0.001 * |
| Maternal hospital days stay at birth (0) | 6.0 (3.0) | 5.0 (3.0) | 5.0 (3.0) | 7.0 (4.0) | 8.0 (4.0) | <0.001 * |
| Mean ± standard deviation | ||||||
| Maternal age at 6 M assessment(years) (0) | 34.5 ± 5.2 | 36.1 ± 5.1 | 35.1 ± 4.8 | 33.5 ± 5.3 | 36.4 ± 4.0 | <0.001 * |
| Number (%) | ||||||
| Currently in a relationship (4) | 442 (91) | 70 (93) | 105 (94) | 242 (91) | 25 (93) | 0.79 |
| Breastfeeding at 6 months (3) | 0.40 | |||||
| Yes, n (%) | 297 (62) | 47 (62) | 72 (64) | 163 (61) | 15 (56) | |
| No (never breastfed), n (%) | 43 (9) | 8 (11) | 5 (5) | 25 (9) | 5 (19) | |
| No (I’ve stopped now), n (%) | 141 (29) | 21 (28) | 35 (31) | 78 (29) | 7 (26) | |
| When stopped (months after birth), median (IQR) | 3.0 (2.4) | 3.0 (3.6) | 3.5 (2.7) | 3.0 (2.5) | 2.0 (2.0) | |
| Pregnant at time of follow-up (3) | 4 (1) | 1 (1) | 0 (0) | 3 (1) | 0 (0) | 0.65 |
| Mean gestation ± SD | 8.7 ± 4.7 | 5.0 ± 0.0 | 10.5 ± 5.0 | |||
| Currently taking antihypertensives (0) | 106 (22) | 49 (65) | 8 (7) | 26 (10) | 23 (85) | <0.001 * |
| Current daily smoker, n (%) | 8 (2) ⋄ | 3 (4) | 2 (2) ❖ | 3 (1) | 0 (0) | 0.08 0.61 |
| 1–10 cigarettes per day, n (%) | 6 (1) | 3 (4) | 1 (1) | 2 (1) | N/A | |
| 11–20 cigarettes per day, n (%) | 1 (0) | 0 (0) | 0 (0) | 1 (0) | ||
| 21 or more cigarettes per day, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Don’t know, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Occasional smoker, n (%) | 4 (1) | 0 (0) | 1 (1) | 2 (1) | 1 (4) | |
| Past smoker, n (%) | 107 (22) | 21 (28) | 30 (27) | 53 (20) | 3 (11) | |
| Non-smoker, n (%) ⊕ | 365 (75) | 52 (68) | 80 (71) | 210 (78) | 23 (85) | |
| Don’t know, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| (0) | ||||||
| Current daily e-cigarette user, n (%) | 2 (0) | 2 (3) | 0 (0) | 0 (0) | 0 (0) | 0.19 |
| Occasional e-cigarette user, n (%) | 4 (1) | 1 (1) | 0 (0) | 3 (1) | 0 (0) | |
| Past e-cigarette user, n (%) | 6 (1) | 0 (0) | 3 (3) | 2 (1) | 1 (4) | |
| Non-e-cigarette user, n (%) ⊕ | 460 (95) | 71 (93) | 110 (97) | 255 (96) | 24 (89) | |
| Don’t know, n (%) | 10 (2) | 1 (1) | 0 (0) | 7 (3) | 2 (7) | |
| Refused, n (%) | 1 (0) | 1 (1) | 0 (0) | 0 (0) | 0 (0) | |
| (1) | ||||||
| Median (IQR)⋄ | ||||||
| Number of children at time of 6 M follow-up (5) | 1.0 (1.0) | 2.0 (2.0) | 1.0 (1.0) | 1.0 (2.0) | 2.0 (1.0) | <0.001 * |
| Lifestyle Behaviour (Missing) | Total (n = 484) | CH (n = 76) | GH (n = 113) | Preeclampsia (n = 268) | CH + PE (n = 27) | p-Value |
|---|---|---|---|---|---|---|
| Nutrition | ||||||
| Vegetable serves/day, median [IQR] (0) | 2.0 [2.0] | 2.0 [2.0] | 2.0 [1.8] | 2.0 [2.0] | 2.0 [1.5] | 0.61 |
| Meeting recommended 5 vegetable serves/day, n (%) (0) | 44 (9) | 5 (7) | 11 (10) | 25 (9) | 3 (11) | 0.85 |
| Fruit serves/day, median [IQR] (0) | 1.0 [1.0] | 1.0 [1.5] | 2.0 [1.0] | 1.0 [1.0] | 1.0 [1.0] | 0.13 |
| Meeting recommended 2 fruit serves/day, n (%) (0) | 220 (46) | 23 (30) | 57 (50) | 130 (49) | 10 (37) | 0.018 * |
| Meeting both recommended 5 vegetable serves and 2 fruit serves/day, n (%) (0) | 31 (6) | 2 (3) | 9 (8) | 18 (7) | 2 (7) | 0.51 |
| Processed meat serves/week, median [IQR] (0) | 1.0 [2.0] | 1.0 [2.4] | 1.0 [1.9] | 1.0 [1.8] | 1.0 [2.0] | 0.49 |
| Fried potato serves/week, median [IQR] (0) | 1.0 [0.8] | 1.0 [1.7] | 1.0 [0.8] | 1.0 [0.8] | 0.7 [1.8] | 0.43 |
| Salty snack serves/week, median [IQR] (0) | 0.5 [1.0] | 0.5 [1.0] | 0.5 [1.0] | 0.5 [1.0] | 1.0 [1.0] | 0.63 |
| Takeaway occurrences/week, median [IQR] (0) | 0.5 [0.8] | 1.0 [0.5] | 0.7 [0.8] | 0.5 [0.8] | 0.5 [2.0] | 0.25 |
| Types of milk, n (%) (0) | 0.06 | |||||
| Full fat | 243 (50) | 48 (63) | 50 (44) | 129 (48) | 16 (59) | |
| Low/reduced fat | 73 (15) | 10 (13) | 16 (14) | 41 (15) | 6 (22) | |
| Skim | 48 (10) | 5 (7) | 12 (11) | 30 (11) | 1 (4) | |
| Evaporated or sweetened | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Almond/rice/oat milk | 69 (14) | 6 (8) | 19 (17) | 42 (16) | 2 (7) | |
| Don’t drink milk | 21 (4) | 6 (8) | 4 (4) | 9 (3) | 2 (7) | |
| Other | 29 (6) | 1 (1) | 12 (11) | 16 (6) | 0 (0) | |
| Don’t know | 1 (0) | 0 (0) | 0 (0) | 1 (0) | 0 (0) | |
| Cups of soft drinks/day, median [IQR] (0) | 0.0 [0.4] | 0.2 [1.0] | 0.0 [0.4] | 0.0 [0.3] | 0.1 [0.6] | 0.005 * |
| Cups of fruit juice/day, median [IQR] (0) | 0.0 [0.3] | 0.0 [0.3] | 0.0 [0.3] | 0.0 [0.3] | 0.0 [0.3] | 0.52 |
| Cups of water/day, median [IQR] (0) | 7.0 [4.0] | 7.0 [6.0] | 7.0 [4.0] | 7.0 [3.0] | 8.0 [4.0] | 0.63 |
| Physical activity | ||||||
| Minutes spent doing vigorous household chores in the past week, median [IQR] (1) | 0.0 [60.0] | 5.0 [120.0] | 0.0 [60.0] | 0.0 [60.0] | 0.0 [60.0] | 0.004 * |
| Minutes spent doing vigorous yard work in the past week, median [IQR] (1) | 0.0 [0.0] | 0.0 [0.0] | 0.0 [0.0] | 0.0 [0.0] | 0.0 [0.0] | 0.27 |
| Minutes spent continuously walking in the past week, median [IQR] (0) | 180.0 [230.0] | 120.0 [208.0] | 190.0 [210.0] | 180.0 [240.0] | 140.0 [210.0] | 0.19 |
| Minutes spent doing vigorous physical activity in the past week, median [IQR] (0) | 0.0 [60.0] | 0.0 [37.5] | 0.0 [97.5] | 0.0 [60.0] | 0.0 [10.0] | 0.047 * |
| Including activity previously mentioned, minutes spent doing strength/toning activities in the past week, median [IQR] (3) | 0.0 [45.0] | 0.0 [45.0] | 0.0 [60.0] | 0.0 [40.0] | 0.0 [0.0] | 0.10 |
| Combined minutes spent doing moderate–vigorous physical activity in the past week, median [IQR] (0) | 210.0 [270.0] | 150.0 [297.5] | 240.0 [300.0] | 235.0 [281.3] | 180.0 [300.0] | 0.11 |
| Meeting recommended 150 min/week, n (%) (0) | 313 (65) | 40 (53) | 81 (72) | 178 (66) | 14 (52) | 0.023 * |
| Number of moderate–vigorous physical activity sessions in the past week, median [IQR] (0) | 6.0 [6.0] | 4.5 [6.8] | 7.0 [6.0] | 6.5 [6.0] | 6.0 [4.0] | 0.71 |
| Meeting recommended 5 sessions/week, n (%) (0) | 311 (64) | 38 (50) | 80 (71) | 176 (66) | 17 (63) | 0.028 * |
| Meeting both recommended 150 min in 5 sessions/week, n (%) (0) | 278 (57) | 35 (46) | 71 (63) | 160 (60) | 12 (44) | 0.050 ⦿ |
| Meeting recommendations for 150 min of moderate–vigorous physical activity in 5 sessions/week, as well as 5 vegetable and 2 fruit serves daily, n (%) (0) | 22 (5) | 1 (1) | 6 (5) | 13 (5) | 2 (7) | 0.469 |
| Alcohol | ||||||
| Alcohol intake occurrences/week, median [IQR] (0) | 0.0 [1.0] | 0.0 [0.3] | 0.0 [1.4] | 0.0 [1.0] | 0.0 [1.0] | 0.187 |
| Standard drinks/week, median [IQR] (0) | 0.0 [1.5] | 0.0 [0.7] | 0.0 [2.0] | 0.0 [2.0] | 0.0 [1.5] | 0.592 |
| Consumption of more than 4 standard drinks in one session in past 4 weeks, n (%) (207) | 55 (20) | 5 (14) | 12 (17) | 36 (23) | 2 (20) | 0.598 |
| Outcomes (Missing) | Total (n = 484) | CH (n = 76) | GH (n = 113) | Preeclampsia (n = 268) | CH + PE (n = 27) | p-Value |
|---|---|---|---|---|---|---|
| Median [IQR] | ||||||
| BMI (kg/m2) (2) | 26.6 [8.4] | 30.2 [8.5] | 26.8 [7.7] | 25.5 [7.5] | 27.3 [8.1] | <0.001 * |
| Overweight; BMI 25.0–29.9, n (%) | 155 (32) | 24 (32) | 44 (39) | 77 (29) | 10 (37) | <0.001 * |
| Obese; BMI ≥ 30, n (%) | 146 (30) | 39 (51) | 32 (28) | 66 (25) | 9 (33) | <0.001 * |
| Waist-circumference (cm) (24) | 90.0 [21.9] | 101.5 [22.6] | 90.5 [20.5] | 87.0 [20.9] | 94.0 [18.5] | <0.001 * |
| Average systolic BP (mmHg) (6) | 122.0 [15.0] | 130.0 [16.0] | 122.0 [12.0] | 119.0 [14.5] | 130.0 [21.0] | <0.001 * |
| Average systolic BP > 120, n (%) | 280 (58) | 65 (86) | 68 (60) | 126 (47) | 21 (78) | <0.001 * |
| Average diastolic BP (mmHg) (6) | 81.0 [14.0] | 88.0 [11.0] | 81.0 [11.0] | 79.0 [14.0] | 88.0 [13.0] | <0.001 * |
| Average diastolic BP > 80, n (%) | 266 (55) | 63 (83) | 62 (55) | 120 (45) | 21 (78) | <0.001 * |
| Mean ± standard deviation | ||||||
| Body fat mass (%) (202) | 37.0 ± 8.4 | 41.6 ± 9.2 | 37.7 ± 7.3 | 35.5 ± 8.4 | 35.6 ± 6.2 | <0.001 * |
| Number (%) | ||||||
| Returned to index pregnancy’s first antenatal appointment BMI or lower (7) | 140 (29) | 24 (33) | 21 (19) | 87 (33) | 8 (30) | 0.052 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirsch, C.; Roberts, L.; Salisbury, J.; Denney-Wilson, E.; Henry, A.; Gow, M. The Association between Nutrition, Physical Activity, and Cardiometabolic Health at 6 Months following a Hypertensive Pregnancy: A BP2 Sub-Study. Nutrients 2023, 15, 3294. https://doi.org/10.3390/nu15153294
Hirsch C, Roberts L, Salisbury J, Denney-Wilson E, Henry A, Gow M. The Association between Nutrition, Physical Activity, and Cardiometabolic Health at 6 Months following a Hypertensive Pregnancy: A BP2 Sub-Study. Nutrients. 2023; 15(15):3294. https://doi.org/10.3390/nu15153294
Chicago/Turabian StyleHirsch, Camilla, Lynne Roberts, Justine Salisbury, Elizabeth Denney-Wilson, Amanda Henry, and Megan Gow. 2023. "The Association between Nutrition, Physical Activity, and Cardiometabolic Health at 6 Months following a Hypertensive Pregnancy: A BP2 Sub-Study" Nutrients 15, no. 15: 3294. https://doi.org/10.3390/nu15153294
APA StyleHirsch, C., Roberts, L., Salisbury, J., Denney-Wilson, E., Henry, A., & Gow, M. (2023). The Association between Nutrition, Physical Activity, and Cardiometabolic Health at 6 Months following a Hypertensive Pregnancy: A BP2 Sub-Study. Nutrients, 15(15), 3294. https://doi.org/10.3390/nu15153294