Intakes of Added Sugars, with a Focus on Beverages and the Associations with Micronutrient Adequacy in US Children, Adolescents, and Teens (NHANES 2003–2018)

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Added Sugars Intake
2.3. Added Sugars Intake and Micronutrient Adequacy
2.4. Statistical Analyses
3. Results
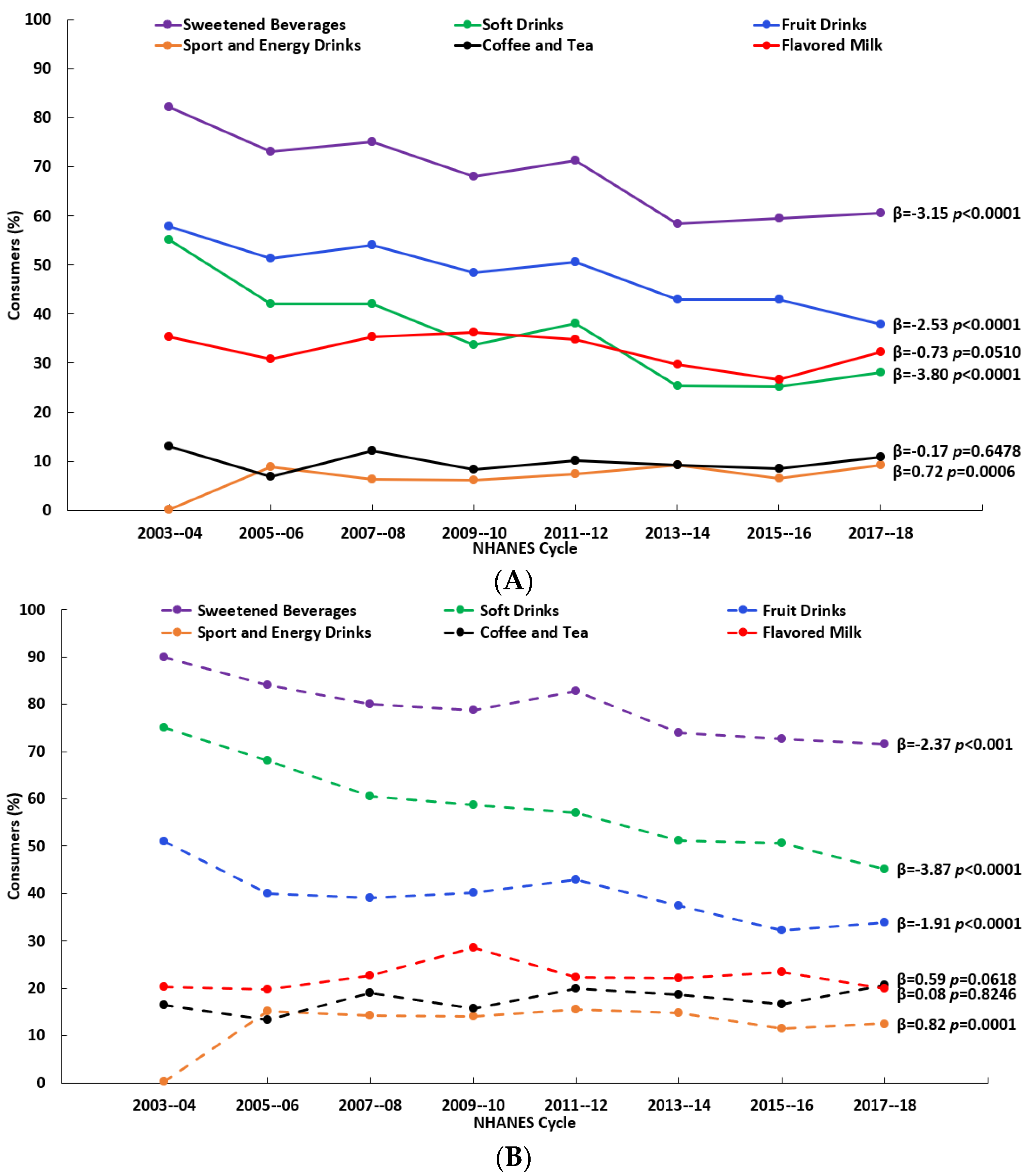
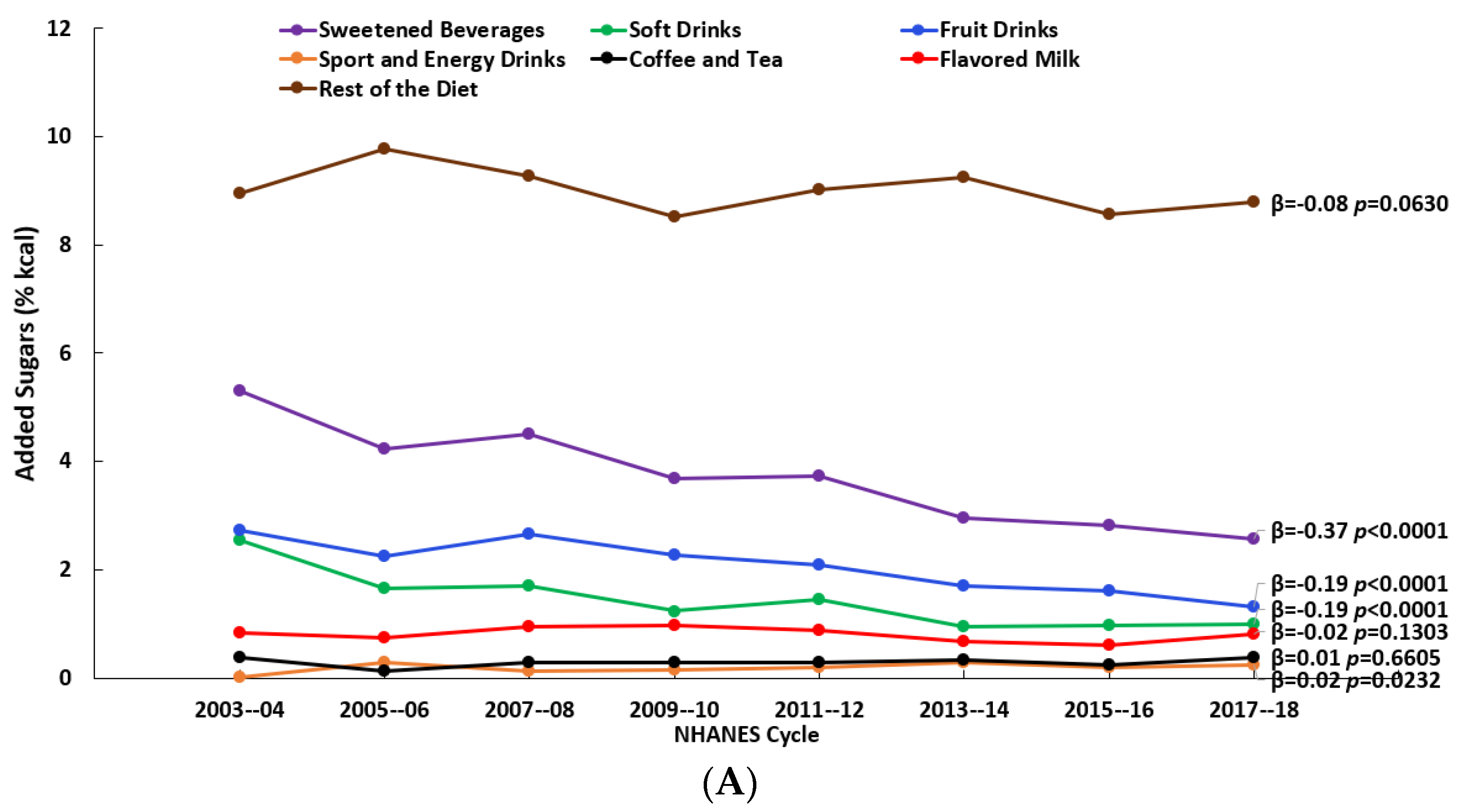
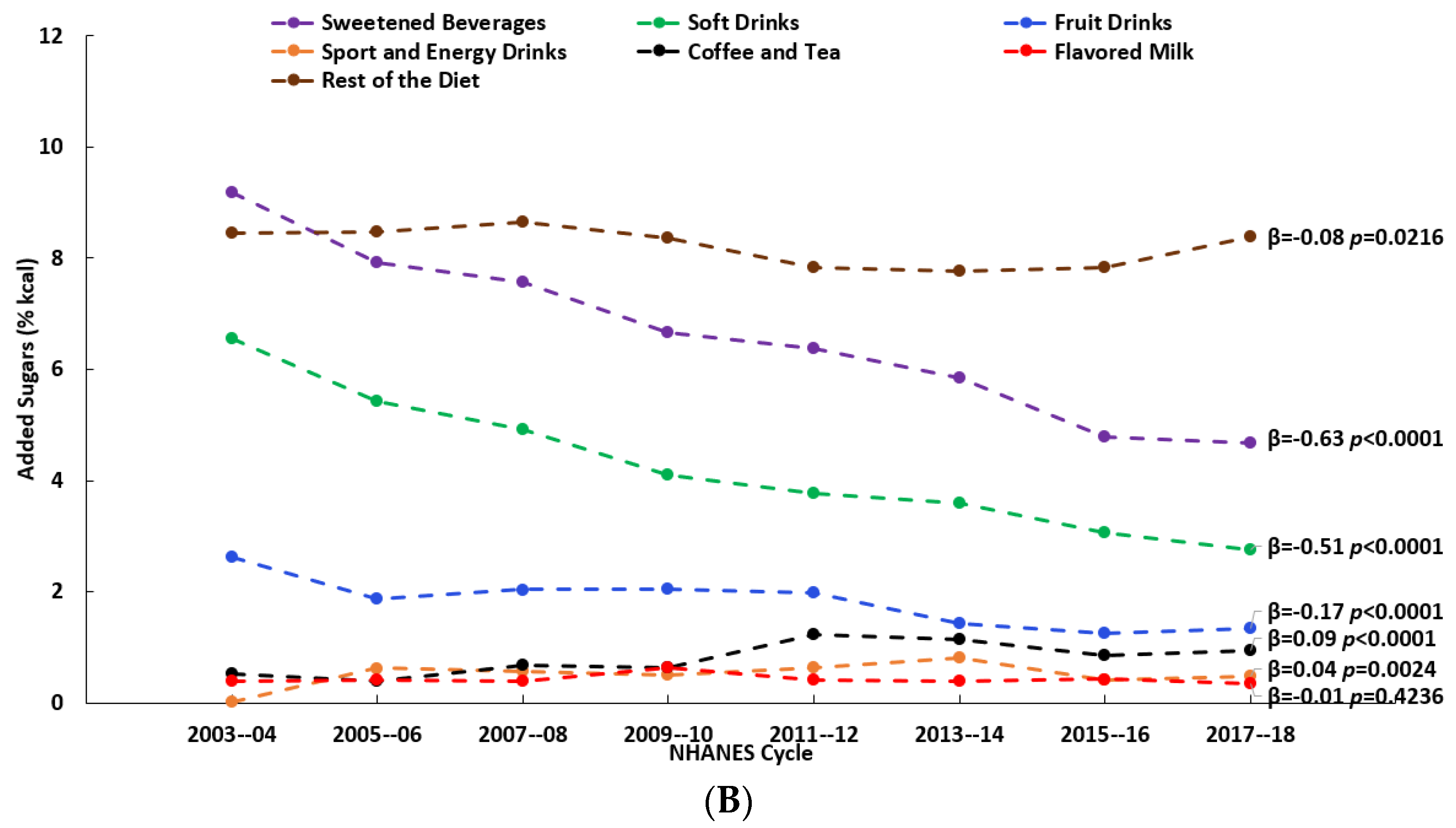
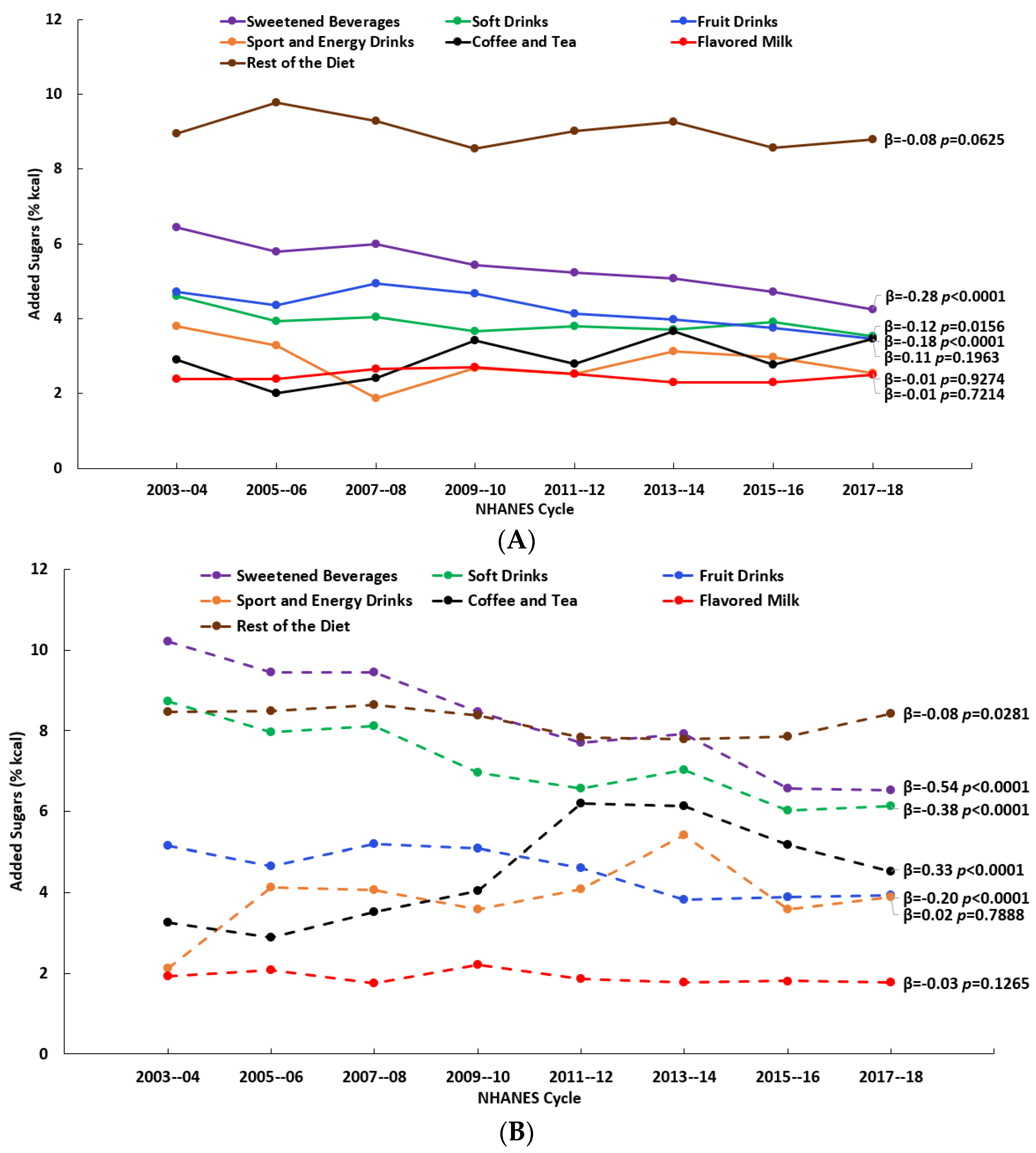
3.1. Consumption Patterns of Beverage Sources of Added Sugars and Added Sugars Intake
3.2. Associations between Added Sugars Intake and Micronutrient Adequacy by Beverage Source

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sweetened Beverages | |||||||
|---|---|---|---|---|---|---|---|
| Q1 2 n = 8,714,811 % <EAR (SE) | Q2 n = 11,013,572 % <EAR (SE) | Q3 n = 11,011,003 % <EAR (SE) | Q4 n = 11,028,124 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 62.09 (2.32) | 62.63 (1.86) | 68.26 (1.91) | 64.16 (2.03) | 1.07 (1.39), 0.52 | 2.96 (3.95), 0.53 | 0.66 (2.81), 0.85 |
| Magnesium | 55.50 (2.13) | 52.72 (1.65) | 61.35 (1.48) | 66.17 (1.30) | 4.42 (1.61), 0.11 | 4.87 (9.27), 0.65 | 6.68 (1.10), 0.10 |
| Phosphorus | 26.99 (2.12) | 25.86 (1.63) | 28.53 (1.69) | 19.01 (1.79) | −2.37 (1.89), 0.34 | −2.67 (6.85), 0.73 | −3.56 (3.52), 0.50 |
| Vitamin A | 32.06 (2.35) | 31.46 (1.89) | 43.79 (1.84) | 49.95 (2.36) | 6.94 (1.73), 0.06 | 10.07 (12.80), 0.51 | 9.18 (1.78), 0.12 |
| Vitamin C | 40.05 (2.41) | 27.56 (2.25) | 30.03 (2.31) | 28.01 (2.58) | −2.88 (2.15), 0.31 | −11.51 (1.80), 0.02 § | 0.18 (1.30), 0.91 |
| Vitamin D | 92.21 (1.08) | 93.89 (0.86) | 96.12 (0.67) | 96.39 (0.58) | 1.44 (0.31), 0.04 | 3.31 (1.85), 0.22 | 1.23 (0.57), 0.27 |
| Choline 1 | 6.01 (1.17) | 3.72 (0.70) | 3.13 (0.67) | 3.15 (0.64) | −0.86 (0.38), 0.15 | −2.67 (0.44), 0.03 | −0.29 (0.18), 0.35 |
| Potassium 1 | 32.41 (2.15) | 28.25 (2.04) | 25.52 (1.76) | 29.54 (1.77) | −0.85 (1.42), 0.61 | −4.62 (2.84), 0.25 | 0.72 (1.95), 0.78 |
| Soft Drinks | |||||||
| Q1 2 n = 17,449,876 % <EAR (SE) | Q2 n = 8,034,425 % <EAR (SE) | Q3 n = 8,161,395 % <EAR (SE) | Q4 n = 8,121,813 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 61.68 (1.51) | 66.03 (2.33) | 68.35 (2.43) | 62.56 (2.31) | 0.88 (1.50), 0.62 | 3.95 (2.66), 0.28 | −1.73 (2.32), 0.59 |
| Magnesium | 52.91 (1.22) | 56.57 (2.01) | 63.47 (1.47) | 70.28 (1.56) | 5.73 (0.51), 0.01 † | 10.50 (6.29), 0.24 | 6.85 (0.03), 0.00 † |
| Phosphorus | 25.92 (1.36) | 28.86 (1.70) | 25.31 (2.23) | 18.36 (2.12) | −2.17 (1.46), 0.28 | −1.73 (4.90), 0.76 | −5.25 (0.97), 0.12 |
| Vitamin A | 32.15 (1.63) | 36.61 (2.23) | 47.01 (2.31) | 51.74 (2.65) | 6.80 (0.72), 0.01 § | 12.92 (7.11), 0.21 | 7.57 (1.62), 0.13 |
| Vitamin C | 24.55 (1.63) | 28.31 (2.36) | 34.30 (2.89) | 44.14 (3.31) | 6.23 (0.88), 0.02 § | 11.01 (7.33), 0.27 | 7.91 (1.10), 0.09 |
| Vitamin D | 93.18 (0.61) | 95.85 (0.89) | 96.10 (0.79) | 95.66 (0.83) | 0.92 (0.47), 0.19 | 2.69 (0.20), 0.01 † | −0.09 (0.20), 0.73 |
| Choline 1 | 4.92 (0.70) | 3.74 (0.88) | 2.52 (0.79) | 3.35 (0.95) | −0.69 (0.31), 0.15 | −1.71 (0.56), 0.09 | −0.23 (0.60), 0.77 |
| Potassium 1 | 33.80 (1.54) | 24.35 (2.20) | 24.48 (1.80) | 26.42 (2.25) | −2.76 (1.76), 0.26 | −8.72 (1.06), 0.01 § | 1.03 (0.51), 0.29 |
| Fruit Drinks | |||||||
| Q1 2 n = 25,242,572 % <EAR (SE) | Q2 n = 5,506,152 % <EAR (SE) | Q3 n = 5,508,295 % <EAR (SE) | Q4 n = 5,510,490 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 63.35 (1.44) | 67.43 (2.48) | 66.09 (2.35) | 62.85 (2.54) | 0.18 (0.96), 0.87 | 1.87 (1.89), 0.43 | −2.34 (0.55), 0.15 |
| Magnesium | 61.84 (1.10) | 52.35 (2.15) | 56.40 (2.08) | 53.88 (1.77) | −2.69 (1.38), 0.19 | −7.57 (1.55), 0.04 § | 0.60 (1.88), 0.80 |
| Phosphorus | 25.24 (1.21) | 28.11 (2.41) | 25.81 (2.67) | 19.79 (2.18) | −1.34 (1.14), 0.36 | −1.10 (3.45), 0.78 | −4.25 (1.07), 0.16 |
| Vitamin A | 40.39 (1.45) | 36.02 (2.61) | 36.59 (2.25) | 42.68 (2.82) | 0.16 (1.34), 0.92 | −1.61 (2.99), 0.65 | 3.47 (1.58), 0.27 |
| Vitamin C | 46.02 (1.72) | 20.59 (2.94) | 6.96 (2.63) | 2.76 (1.77) | −15.58 (2.73), 0.03 § | −36.80 (7.14), 0.04 § | −8.68 (2.70), 0.19 |
| Vitamin D | 93.83 (0.59) | 96.22 (0.83) | 95.97 (0.83) | 96.00 (0.83) | 0.81 (0.34), 0.14 | 2.23 (0.10), 0.00 † | −0.10 (0.08), 0.44 |
| Choline 1 | 4.39 (0.63) | 3.17 (0.97) | 3.16 (0.64) | 4.31 (0.97) | −0.18 (0.31), 0.61 | −0.81 (0.52), 0.26 | 0.58 (0.33), 0.33 |
| Potassium 1 | 27.44 (1.32) | 25.66 (2.28) | 30.27 (2.63) | 37.41 (2.36) | 2.89 (1.17), 0.13 | 4.28 (4.70), 0.46 | 5.94 (0.72), 0.08 |
| Sport and Energy Drinks | |||||||
| Q1 2 n = 36,649,246 % <EAR (SE) | Q2 n = 1,670,286 % <EAR (SE) | Q3 n = 1,716,552 % <EAR (SE) | Q4 n = 1,978,772 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 64.95 (1.16) | 68.08 (4.46) | 60.40 (6.06) | 46.78 (5.51) | −4.30 (2.04), 0.17 | −5.92 (6.56), 0.46 | −10.57 (1.69), 0.10 |
| Magnesium | 58.63 (0.89) | 63.98 (3.67) | 62.81 (3.64) | 58.90 (5.06) | 1.05 (1.14), 0.46 | 3.40 (1.61), 0.17 | −2.50 (0.78), 0.19 |
| Phosphorus | 25.25 (1.04) | 32.42 (4.72) | 20.91 (5.05) | 18.47 (3.55) | −1.55 (1.91), 0.50 | −0.86 (4.63), 0.87 | −7.10 (2.58), 0.22 |
| Vitamin A | 39.49 (1.24) | 42.73 (4.10) | 44.41 (5.60) | 36.24 (7.14) | 0.25 (1.33), 0.87 | 1.78 (2.57), 0.56 | −3.10 (2.81), 0.47 |
| Vitamin C | 32.14 (1.37) | 14.00 (6.58) | 29.00 (4.85) | 22.26 (9.02) | −3.87 (3.18), 0.35 | −10.73 (4.67), 0.15 | 4.44 (6.19), 0.60 |
| Vitamin D | 94.74 (0.44) | 96.17 (1.65) | 95.42 (1.98) | 92.82 (2.63) | −0.21 (0.48), 0.71 | 0.16 (1.06), 0.89 | −1.65 (0.52), 0.20 |
| Choline 1 | 3.97 (0.46) | 3.31 (1.51) | 3.58 (1.65) | 6.39 (3.07) | 0.42 (0.40), 0.41 | 0.39 (1.03), 0.75 | 1.50 (0.72), 0.29 |
| Potassium 1 | 28.47 (1.15) | 23.70 (3.82) | 25.34 (4.51) | 39.00 (5.22) | 1.45 (2.14), 0.57 | 0.48 (5.04), 0.93 | 7.48 (3.42), 0.27 |
| Coffee and Tea | |||||||
| Q1 2 n = 34,438,767 % <EAR (SE) | Q2 n = 2,439,053 % <EAR (SE) | Q3 n = 2,454,977 % <EAR (SE) | Q4 n = 2,434,713 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 62.91 (1.25) | 77.82 (2.70) | 68.57 (4.17) | 63.34 (4.69) | 1.96 (3.00), 0.58 | 7.48 (4.60), 0.25 | −7.32 (1.19), 0.10 |
| Magnesium | 58.11 (0.93) | 61.89 (2.90) | 62.38 (2.62) | 64.19 (3.42) | 2.18 (0.36), 0.03 | 4.62 (0.74), 0.02 | 1.13 (0.39), 0.21 |
| Phosphorus | 24.55 (1.12) | 31.86 (2.94) | 26.06 (3.32) | 22.22 (4.67) | 0.24 (1.65), 0.90 | 2.49 (3.03), 0.50 | −4.85 (0.58), 0.08 |
| Vitamin A | 38.13 (1.26) | 44.44 (4.24) | 44.11 (4.49) | 50.64 (4.41) | 3.94 (0.67), 0.03 | 7.99 (2.23), 0.07 | 2.97 (2.03), 0.38 |
| Vitamin C | 28.91 (1.45) | 37.22 (4.51) | 38.41 (5.87) | 49.55 (5.77) | 6.31 (0.87), 0.02 § | 12.30 (4.13), 0.10 | 5.97 (2.95), 0.29 |
| Vitamin D | 94.26 (0.50) | 97.91 (0.79) | 97.62 (0.91) | 96.09 (1.85) | 1.15 (0.66), 0.23 | 3.03 (0.59), 0.04 | −0.88 (0.37), 0.25 |
| Choline 1 | 3.88 (0.46) | 3.48 (1.38) | 4.69 (2.02) | 5.42 (1.92) | 0.42 (0.18), 0.14 | 0.61 (0.62), 0.42 | 0.97 (0.14), 0.09 |
| Potassium 1 | 28.20 (1.18) | 26.19 (3.23) | 31.09 (3.59) | 38.20 (4.62) | 2.39 (1.17), 0.18 | 3.18 (3.72), 0.48 | 5.96 (0.65), 0.07 |
| Flavored Milk | |||||||
| Q1 2 n = 32,403,033 % <EAR (SE) | Q2 n = 2,768,510 % <EAR (SE) | Q3 n = 3,413,986 % <EAR (SE) | Q4 n = 3,181,981 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 69.34 (1.30) | 59.57 (4.78) | 48.09 (3.81) | 19.93 (4.45) | −14.40 (2.28), 0.02 § | −27.00 (13.11), 0.18 | −19.97 (5.14), 0.16 |
| Magnesium | 63.59 (0.99) | 46.12 (3.47) | 42.70 (2.78) | 37.14 (2.78) | −9.67 (1.63), 0.03 § | −21.68 (2.89), 0.02 § | −4.51 (0.66), 0.09 |
| Phosphorus | 29.62 (1.08) | 15.89 (2.68) | 9.52 (2.57) | 1.11 (0.75) | −9.84 (0.78), 0.01 † | −20.94 (4.73), 0.05 § | −7.41 (0.62), 0.05 |
| Vitamin A | 45.13 (1.32) | 21.93 (4.70) | 20.71 (3.40) | 13.23 (2.45) | −11.63 (2.33), 0.04 § | −26.49 (3.06), 0.01 § | −4.41 (1.93), 0.26 |
| Vitamin C | 32.18 (1.56) | 23.72 (2.94) | 27.23 (3.38) | 30.50 (3.30) | −1.47 (1.52), 0.44 | −4.93 (2.15), 0.15 | 3.39 (0.07), 0.01 |
| Vitamin D | 95.68 (0.43) | 99.14 (0.68) | 94.38 (2.03) | 90.49 (3.86) | −1.18 (0.98), 0.35 | −1.16 (2.75), 0.72 | −4.32 (0.27), 0.04 |
| Choline 1 | 3.58 (0.42) | 2.01 (0.97) | 5.37 (1.90) | 6.24 (2.22) | 0.78 (0.48), 0.24 | 1.02 (1.43), 0.55 | 2.11 (0.77), 0.22 |
| Potassium 1 | 25.69 (1.17) | 30.32 (3.64) | 37.22 (3.25) | 57.34 (3.98) | 8.84 (1.90), 0.04 § | 16.02 (9.04), 0.22 | 13.63 (4.08), 0.19 |
3.3. Associations between Added Sugars from the Rest of the Diet and Micronutrient Adequacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Adequate intake |
| DGA | Dietary Guidelines for Americans |
| EAR | Estimated average requirement |
| FPED | Food Patterns Equivalent Database |
| HEI | Healthy Eating Index |
| NCI | National Cancer Institute |
| SSB | Sugar-sweetened beverages |
| UI | Usual intake |
| WWEIA | What We Eat in America |
References
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025. 2020. Available online: https://www.dietaryguidelines.gov/ (accessed on 20 June 2023).
- Ricciuto, L.; Fulgoni, I.I.I.V.L.; Gaine, P.C.; Scott, M.O.; DiFrancesco, L. Sources of added sugars intake among the U.S. population: Analysis by selected sociodemographic factors using the National Health and Nutrition Examination Survey 2011–18. Front. Nutr. 2021, 8, 687643. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Fulgoni, I.I.I.V.L.; Cowan, A.E.; Gaine, P.C. Sources of added sugars in young children, adolescents, and adults with low and high intakes of added sugars. Nutrients 2018, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Ricciuto, L.; Fulgoni, V.L.; Gaine, C.; Scott, M.O.; DiFrancesco, L. Trends in added Sugars Intake and Sources Among US Children, Adolescents and Teens using NHANES 2001–2018. J. Nutr. 2021, 152, 568–578. [Google Scholar] [CrossRef]
- Vercammen, K.A.; Dowling, E.A.; Sharkey, A.L.; Curtis, C.J.; Wang, J.; Kenney, E.L.; Micha, R.; Mozaffarian, D.; Moran, A.J. Estimated reductions in added sugar intake among US children and youth in response to sugar reduction targets. J. Acad. Nutr. Diet. 2022, 122, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture, Agricultural Research Service, Food Surveys Research Group. Beverage Choices among Children: What We Eat in America, NHANES 2017–2018. Dietary Data Brief No. 32. October 2020. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/DBrief/32_Beverage_children_1718.pdf (accessed on 20 June 2023).
- Fiorito, L.M.; Marini, M.; Mitchell, D.C.; Smiciklas-Wright, H.; Birch, L.L. Girls’ early sweetened carbonated beverage intake predicts different patterns of beverage and nutrient intake across childhood and adolescence. J. Am. Diet. Assoc. 2010, 110, 543–550. [Google Scholar] [CrossRef]
- Barraj, L.M.; Bi, X.; Murphy, M.M.; Scrafford, C.G.; Tran, N.L. Comparison of nutrient intakes and diet quality among water-based beverage consumers. Nutrients 2019, 11, 314. [Google Scholar] [CrossRef] [Green Version]
- Doherty, A.M.; Lacko, A.M.; Popkin, B.M. Sugar-sweetened beverage (SSB) consumption is associated with lower quality of the non-SB diet in US adolescents and young adults. Am. J. Clin. Nutr. 2021, 113, 657–664. [Google Scholar] [CrossRef]
- Leung, C.W.; DiMatteo, S.G.; Gosliner, W.A.; Ritchie, L.D. Sugar-sweetened beverage and water intake in relation to diet quality in U.S. children. Am. J. Prev. Med. 2018, 54, 394–402. [Google Scholar] [CrossRef]
- Wang, J.W.; Shang, L.; Light, K.; O’Loughlin, J.; Paradis, G.; Gray-Donald, K. Associations between added sugar (solid vs. liquid) intakes, diet quality, and adiposity indicators in Canadian children. Appl. Physiol. Nutr. Metab. 2015, 40, 835–841. [Google Scholar] [CrossRef] [Green Version]
- Libuda, L.; Alexy, U.; Buyken, A.E.; Sichert-Hellert, W.; Stehle, P.; Kersting, M. Consumption of sugar-sweetened beverages and its association with nutrient intakes and diet quality in German children and adolescents. Br. J. Nutr. 2009, 101, 1549–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayet-Moore, F.; Cassettari, T.; McConnell, A.; Kim, J.; Petocz, P. Australian children and adolescents who were drinkers of plain and flavored milk has the highest intakes of milk, total dairy, and calcium. Nutr. Res. 2019, 66, 68–81. [Google Scholar] [CrossRef]
- Huth, P.J.; Fulgoni, I.I.I.V.L.; Keast, D.R.; Park, K.; Auestad, N. Major food sources of calories, added sugars, and saturated fat and their contribution to essential nutrient intakes in the U.S. diet: Data from the national health and nutrition examination survey (2003–2006). Nutr. J. 2013, 12, 116. [Google Scholar] [CrossRef] [Green Version]
- Fulgoni, V.L.; Gaine, P.C.; Scott, M.O.; Ricciuto, L.; DiFrancesco, L. Association of added sugars intake with micronutrient adequacy in US children and adolescents: NHANES 2009–2014. Curr. Dev. Nutr. 2019, 3, nzz126. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 20 June 2023).
- Centers for Disease Control and Prevention; National Center for Health Statistics. Survey Methods and Analytic Guidelines. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/AnalyticGuidelines.aspx (accessed on 20 June 2023).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- USDA. Agricultural Research Service. Food Patterns Equivalents Database (FPED). Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fped-overview/ (accessed on 20 June 2023).
- U.S. Department of Agriculture, Agricultural Research Service, Food Surveys Research Group. What We Eat in America: Documentation and Datasets. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweia-documentation-and-data-sets/ (accessed on 20 June 2023).
- USDA. Agricultural Research Service. What We Eat in America (WWEIA): Usual Intakes. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/usual/Usual_Intake_gender_WWEIA_2015_2018.pdf (accessed on 20 June 2023).
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat. Med. 2010, 29, 2857–2868. [Google Scholar] [CrossRef] [Green Version]
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Wallace, A.; Kirkpatrick, S.I.; Darlington, G.; Haines, J. Accuracy of parental reporting of preschoolers’ dietary intake using an online self-administered 24-h recall. Nutrients 2018, 10, 987. [Google Scholar] [CrossRef] [Green Version]




| Added Sugars Source | Description |
|---|---|
| Sweetened Beverages | Soft drinks; fruit drinks; sport and energy drinks; nutritional beverages; smoothies; grain drinks |
| Soft Drinks | |
| Fruit Drinks 1 | |
| Sport and Energy Drinks | |
| Coffee and Tea | Coffee; tea |
| Flavored Milk | Flavored milk: whole, reduced fat, low-fat, non-fat |
| Rest of the Diet * | Milk and dairy (flavored milk excluded); protein foods; mixed dishes; grains; snacks and sweets; fruit; vegetables; beverages (sweetened beverages and coffee and tea excluded); alcoholic beverages; water, fats and oils; condiments and sauces; sugars; baby foods and formulas; other |
| Consumers (%) Mean ± SE | ||
|---|---|---|
| Added Sugars Source | 2–8 y (n = 8599) | 9–18 y (n = 12,406) |
| Sweetened Beverages | 68.55 ± 0.99 | 79.13 ± 0.66 |
| Soft Drinks | 36.20 ± 1.09 | 58.22 ± 0.83 |
| Fruit Drinks | 48.29 ± 0.93 | 39.56 ± 0.79 |
| Sport and Energy Drinks | 6.69 ± 0.54 | 12.25 ± 0.57 |
| Coffee and Tea | 9.86 ± 0.74 | 17.55 ± 0.76 |
| Flavored Milk | 32.64 ± 0.89 | 22.42 ± 0.85 |
| Added Sugars Source | Added Sugars (% kcal) Mean ± SE | |||
|---|---|---|---|---|
| 2–8 y (n = 8599) | 9–18 y (n = 12,406) | |||
| All Individuals | Consumers Only | All Individuals | Consumers Only | |
| Sweetened Beverages | 3.72 ± 0.09 | 5.43 ± 0.10 | 6.61 ± 0.13 | 8.36 ± 0.14 |
| Soft Drinks | 1.44 ± 0.06 | 3.97 ± 0.11 | 4.26 ± 0.11 | 7.32 ± 0.14 |
| Fruit Drinks | 2.08 ± 0.06 | 4.31 ± 0.09 | 1.82 ± 0.05 | 4.59 ± 0.10 |
| Sport and Energy Drinks | 0.18 ± 0.02 | 2.75 ± 0.19 | 0.51 ± 0.04 | 4.13 ± 0.23 |
| Coffee and Tea | 0.29 ± 0.03 | 2.94 ± 0.18 | 0.80 ± 0.05 | 4.55 ± 0.25 |
| Flavored Milk | 0.81 ± 0.04 | 2.48 ± 0.07 | 0.43 ± 0.02 | 1.91 ± 0.05 |
| Rest of the Diet * | 9.01 ± 0.10 | 9.02 ± 0.10 | 8.23 ± 0.08 | 8.23 ± 0.08 |
| Total Added Sugars | 13.8 ± 0.12 | 16.1 ± 0.13 | ||
| Added Sugars Source | Quantile | 2–8 y (n = 8599) Range (% kcal) | 9–18 y (n = 12,406) Range (% kcal) |
|---|---|---|---|
| Sweetened Beverages | 1 * | 0 | 0 |
| 2 | >0 to ≤2.75 | >0 to ≤4.67 | |
| 3 | >2.75 to ≤6.16 | >4.67 to ≤9.49 | |
| 4 | >6.16 | >9.49 | |
| Soft Drinks | 1 * | 0 | 0 |
| 2 | >0 to ≤2.16 | >0 to ≤4.02 | |
| 3 | >2.16 to ≤4.26 | >4.02 to ≤7.89 | |
| 4 | >4.26 | >7.89 | |
| Fruit Drinks | 1 * | 0 | 0 |
| 2 | >0 to ≤2.18 | >0 to ≤2.32 | |
| 3 | >2.18 to ≤4.83 | >2.32 to ≤4.90 | |
| 4 | >4.83 | >4.90 | |
| Sport and Energy Drinks | 1 * | 0 | 0 |
| 2 | >0 to ≤1.30 | >0 to ≤2.26 | |
| 3 | >1.30 to ≤2.70 | >2.26 to ≤4.28 | |
| 4 | >2.70 | >4.28 | |
| Coffee and Tea | 1 * | 0 | 0 |
| 2 | >0 to ≤1.66 | >0 to ≤2.22 | |
| 3 | >1.66 to ≤2.81 | >2.22 to ≤4.57 | |
| 4 | >2.81 | >4.57 | |
| Flavored Milk | 1 * | 0 | 0 |
| 2 | >0 to ≤1.42 | >0 to ≤1.14 | |
| 3 | >1.42 to ≤2.49 | >1.14 to ≤2.03 | |
| 4 | >2.49 | >2.03 |
| Sweetened Beverages | |||||||
|---|---|---|---|---|---|---|---|
| Q1 2 n = 8,786,835 % <EAR (SE) | Q2 n = 6,338,167 % <EAR (SE) | Q3 n = 6,420,388 % <EAR (SE) | Q4 n = 6,392,984 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 15.72 (1.34) | 15.78 (1.19) | 25.41 (1.62) | 24.68 (1.70) | 3.59 (1.35), 0.12 | 6.48 (5.75), 0.38 | 4.33 (3.03), 0.39 |
| Magnesium | 0.64 (0.25) | 0.58 (0.15) | 0.80 (0.25) | 0.74 (0.20) | 0.05 (0.04), 0.33 | 0.07 (0.12), 0.64 | 0.08 (0.08), 0.52 |
| Phosphorus | 0.13 (0.07) | 0.08 (0.04) | 0.09 (0.04) | 0.02 (0.02) | −0.03 (0.01), 0.08 | −0.07 (0.04), 0.22 | −0.03 (0.02), 0.42 |
| Vitamin A | 2.72 (0.63) | 1.71 (0.50) | 3.71 (0.67) | 3.97 (0.75) | 0.55 (0.37), 0.28 | 0.47 (1.33), 0.76 | 1.11 (0.51), 0.27 |
| Vitamin C | 1.78 (0.52) | 0.99 (0.30) | 0.46 (0.21) | 0.79 (0.32) | −0.36 (0.18), 0.19 | −1.04 (0.29), 0.07 | −0.09 (0.25), 0.79 |
| Vitamin D | 85.50 (1.43) | 87.00 (1.28) | 90.42 (1.20) | 90.43 (1.15) | 1.82 (0.43), 0.05 | 3.87 (2.12), 0.21 | 1.67 (1.00), 0.34 |
| Choline 1 | 47.09 (1.94) | 45.26 (2.08) | 41.38 (2.03) | 42.02 (2.27) | −1.94 (0.59), 0.08 | −4.25 (2.20), 0.19 | −1.60 (1.33), 0.44 |
| Potassium 1 | 42.22 (1.96) | 41.65 (1.98) | 38.28 (1.78) | 39.55 (1.78) | −1.13 (0.58), 0.19 | −2.46 (1.83), 0.31 | −1.00 (1.36), 0.60 |
| Soft Drinks | |||||||
| Q1 2 n = 17,824,063 % <EAR (SE) | Q2 n = 3,322,242 % <EAR (SE) | Q3 n = 3,412,532 % <EAR (SE) | Q4 n = 3,379,537 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 17.48 (0.95) | 22.54 (2.10) | 24.05 (2.38) | 27.04 (2.32) | 3.27 (0.42), 0.02 | 6.95 (1.67), 0.05 | 2.23 (0.43), 0.12 |
| Magnesium | 0.61 (0.15) | 0.92 (0.35) | 0.55 (0.24) | 0.89 (0.28) | 0.07 (0.08), 0.46 | 0.18 (0.15), 0.35 | −0.02 (0.20), 0.93 |
| Phosphorus | 0.12 (0.04) | 0.11 (0.06) | 0.05 (0.04) | 0.02 (0.02) | −0.03 (0.01), 0.02 | −0.06 (0.03), 0.23 | −0.05 (0.01), 0.12 |
| Vitamin A | 2.46 (0.39) | 3.04 (0.91) | 3.31 (0.86) | 5.14 (1.22) | 0.76 (0.18), 0.05 | 1.32 (0.83), 0.25 | 1.03 (0.44), 0.26 |
| Vitamin C | 0.89 (0.23) | 0.39 (0.21) | 1.44 (0.55) | 1.70 (0.83) | 0.25 (0.17), 0.29 | 0.26 (0.52), 0.67 | 0.67 (0.22), 0.21 |
| Vitamin D | 87.54 (0.94) | 90.02 (1.47) | 88.80 (1.83) | 89.89 (1.45) | 0.79 (0.40), 0.19 | 2.04 (0.49), 0.05 | −0.09 (0.66), 0.91 |
| Choline 1 | 44.86 (1.40) | 42.67 (2.57) | 41.49 (3.11) | 45.46 (3.01) | −0.43 (0.81), 0.65 | −1.76 (1.41), 0.34 | 1.29 (1.47), 0.54 |
| Potassium 1 | 41.83 (1.28) | 38.80 (2.22) | 38.03 (3.07) | 38.65 (2.52) | −1.35 (0.49), 0.11 | −3.32 (0.30), 0.01 † | −0.09 (0.40), 0.85 |
| Fruit Drinks | |||||||
| Q1 2 n = 14,447,308 % <EAR (SE) | Q2 n = 4,473,337 % <EAR (SE) | Q3 n = 4,519,454 % <EAR (SE) | Q4 n = 4,498,275 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 17.84 (1.06) | 17.50 (1.85) | 25.52 (1.94) | 23.33 (1.87) | 2.31 (1.06), 0.16 | 4.45 (3.41), 0.32 | 2.76 (2.96), 0.52 |
| Magnesium | 0.82 (0.17) | 0.48 (0.17) | 0.51 (0.22) | 0.38 (0.15) | −0.15 (0.04), 0.07 | −0.37 (0.06), 0.02 | −0.05 (0.04), 0.45 |
| Phosphorus | 0.09 (0.04) | 0.06 (0.04) | 0.06 (0.04) | 0.01 (0.01) | −0.02 (0.00), 0.04 | −0.05 (0.03), 0.19 | −0.03 (0.01), 0.30 |
| Vitamin A | 2.87 (0.41) | 2.31 (0.81) | 2.44 (0.81) | 3.17 (0.77) | 0.03 (0.18), 0.87 | −0.21 (0.40), 0.65 | 0.44 (0.17), 0.24 |
| Vitamin C | 1.79 (0.35) | 0.16 (0.13) | 0.03 (0.06) | 0.02 (0.06) | −0.64 (0.24), 0.11 | −1.72 (0.07), 0.00 † | −0.07 (0.04), 0.32 |
| Vitamin D | 85.74 (0.98) | 90.05 (1.26) | 91.83 (1.28) | 91.39 (1.31) | 2.12 (0.65), 0.08 | 5.39 (0.76), 0.02 § | 0.63 (0.64), 0.50 |
| Choline 1 | 47.01 (1.30) | 42.52 (2.64) | 40.30 (2.69) | 38.69 (2.99) | −2.90 (0.41), 0.02 | −6.58 (1.59), 0.05 | −1.91 (0.18), 0.06 |
| Potassium 1 | 42.11 (1.35) | 37.00 (2.41) | 37.41 (2.12) | 41.23 (2.11) | −0.71 (1.23), 0.62 | −3.44 (2.00), 0.23 | 2.16 (0.99), 0.27 |
| Sport and Energy Drinks | |||||||
| Q1 2 n = 26,070,488 % <EAR (SE) | Q2 n = 661,024 % <EAR (SE) | Q3 n = 642,393 % <EAR (SE) | Q4 n = 647,097 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 19.71 (0.81) | 24.88 (4.89) | 13.40 (3.96) | 24.32 (4.15) | 0.31 (1.80), 0.88 | 0.74 (3.94), 0.87 | −0.04 (6.81), 1.00 |
| Magnesium | 0.58 (0.11) | 1.72 (0.90) | 1.01 (0.70) | 2.94 (1.32) | 0.63 (0.21), 0.10 | 1.28 (0.59), 0.16 | 0.64 (0.80), 0.57 |
| Phosphorus | 0.06 (0.02) | 0.17 (0.20) | 0.03 (0.09) | 0.64 (0.42) | 0.13 (0.07), 0.21 | 0.22 (0.19), 0.37 | 0.24 (0.23), 0.48 |
| Vitamin A | 2.92 (0.36) | 4.71 (2.01) | 1.55 (1.36) | 2.48 (1.77) | −0.20 (0.41), 0.67 | −0.12 (0.95), 0.91 | −1.07 (1.24), 0.55 |
| Vitamin C | 1.11 (0.20) | 0.04 (0.11) | 2.52 (1.71) | 0.02 (0.23) | −0.08 (0.40), 0.86 | −0.16 (0.88), 0.87 | −0.06 (1.52), 0.97 |
| Vitamin D | 88.17 (0.76) | 90.21 (3.80) | 83.59 (3.76) | 90.57 (3.83) | −0.07 (1.09), 0.95 | −0.28 (2.40), 0.92 | 0.33 (4.13), 0.95 |
| Choline 1 | 44.55 (1.14) | 42.09 (6.95) | 44.84 (5.77) | 39.60 (6.86) | −1.15 (0.64), 0.22 | −2.28 (1.61), 0.29 | −1.33 (2.43), 0.68 |
| Potassium 1 | 40.19 (1.09) | 38.63 (5.72) | 46.08 (6.02) | 38.34 (4.94) | 0.42 (1.24), 0.77 | 1.09 (2.68), 0.72 | −0.31 (4.62), 0.96 |
| Coffee and Tea | |||||||
| Q1 2 n = 25,183,581 % <EAR (SE) | Q2 n = 878,443 % <EAR (SE) | Q3 n = 951,216 % <EAR (SE) | Q4 n = 925,133 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 19.48 (0.83) | 23.31 (4.90) | 23.92 (4.37) | 26.41 (5.56) | 2.41 (0.33), 0.02 | 4.88 (0.96), 0.04 | 1.49 (0.54), 0.22 |
| Magnesium | 0.64 (0.11) | 0.61 (0.52) | 0.83 (0.48) | 0.87 (0.80) | 0.07 (0.03), 0.11 | 0.11 (0.09), 0.35 | 0.14 (0.05), 0.22 |
| Phosphorus | 0.07 (0.02) | 0.11 (0.11) | 0.01 (0.09) | 0.17 (0.25) | 0.01 (0.02), 0.56 | 0.03 (0.05), 0.61 | 0.02 (0.07), 0.85 |
| Vitamin A | 2.68 (0.33) | 4.84 (2.78) | 3.95 (1.50) | 6.33 (3.39) | 1.12 (0.31), 0.07 | 2.28 (0.69), 0.08 | 0.64 (0.94), 0.62 |
| Vitamin C | 0.89 (0.18) | 3.57 (1.77) | 0.36 (0.60) | 2.46 (1.85) | 0.46 (0.59), 0.51 | 1.32 (1.02), 0.32 | −0.72 (1.53), 0.72 |
| Vitamin D | 87.77 (0.78) | 93.36 (2.10) | 91.67 (2.71) | 87.51 (3.01) | 1.03 (1.26), 0.50 | 3.43 (1.77), 0.19 | −2.85 (0.71), 0.16 |
| Choline 1 | 44.65 (1.16) | 41.82 (4.58) | 45.58 (4.91) | 39.65 (4.37) | −1.08 (0.83), 0.32 | −2.14 (1.75), 0.35 | −0.78 (2.83), 0.83 |
| Potassium 1 | 40.29 (1.01) | 38.68 (5.09) | 37.62 (3.98) | 45.99 (5.33) | 0.60 (1.19), 0.66 | 0.06 (2.60), 0.98 | 3.36 (2.71), 0.43 |
| Flavored Milk | |||||||
| Q1 2 n = 18,819,476 % <EAR (SE) | Q2 n = 3,028,928 % <EAR (SE) | Q3 n = 2,928,578 % <EAR (SE) | Q4 n = 3,161,392 % <EAR (SE) | Quantile Trend 3 Beta (SE), p | Q1 vs. Q2, 3, 4 4 Beta (SE), p | Q2–Q4 Trend 5 Beta (SE), p | |
| Calcium | 23.88 (0.94) | 19.22 (3.26) | 10.13 (2.16) | 0.61 (0.67) | −7.39 (0.70), 0.01 † | −13.39 (6.58), 0.18 | −9.30 (0.12), 0.01 † |
| Magnesium | 1.00 (0.17) | 0.39 (0.26) | 0.11 (0.09) | 0.00 (0.00) | −0.38 (0.07), 0.03 | −0.82 (0.14), 0.03 | −0.20 (0.05), 0.15 |
| Phosphorus | 0.14 (0.05) | 0.00 (0.01) | 0.00 (0.00) | 0.00 (0.00) | −0.06 (0.02), 0.11 | −0.14 (0.00), 0.00 † | 0.00 (0.00), 0.32 |
| Vitamin A | 4.27 (0.44) | 0.53 (0.55) | 0.31 (0.22) | 0.12 (0.15) | −1.65 (0.52), 0.09 | −3.94 (0.14), 0.00 † | −0.20 (0.01), 0.02 |
| Vitamin C | 0.89 (0.22) | 1.04 (0.59) | 0.87 (0.44) | 1.77 (0.64) | 0.21 (0.11), 0.20 | 0.33 (0.33), 0.42 | 0.35 (0.30), 0.45 |
| Vitamin D | 89.56 (0.69) | 98.38 (1.01) | 92.49 (2.31) | 79.09 (4.78) | −1.66 (2.95), 0.63 | 0.85 (6.92), 0.91 | −9.56 (2.07), 0.14 |
| Choline 1 | 43.11 (1.28) | 32.67 (2.88) | 44.00 (4.12) | 64.39 (3.60) | 4.50 (4.18), 0.39 | 2.90 (11.23), 0.82 | 15.71 (2.53), 0.10 |
| Potassium 1 | 37.29 (1.05) | 32.02 (2.54) | 44.17 (3.62) | 68.76 (3.52) | 7.97 (3.89), 0.18 | 10.22 (13.13), 0.52 | 18.22 (3.44), 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricciuto, L.; Fulgoni, V.L., III; Gaine, P.C.; Scott, M.O.; DiFrancesco, L. Intakes of Added Sugars, with a Focus on Beverages and the Associations with Micronutrient Adequacy in US Children, Adolescents, and Teens (NHANES 2003–2018). Nutrients 2023, 15, 3285. https://doi.org/10.3390/nu15153285
Ricciuto L, Fulgoni VL III, Gaine PC, Scott MO, DiFrancesco L. Intakes of Added Sugars, with a Focus on Beverages and the Associations with Micronutrient Adequacy in US Children, Adolescents, and Teens (NHANES 2003–2018). Nutrients. 2023; 15(15):3285. https://doi.org/10.3390/nu15153285
Chicago/Turabian StyleRicciuto, Laurie, Victor L. Fulgoni, III, P. Courtney Gaine, Maria O. Scott, and Loretta DiFrancesco. 2023. "Intakes of Added Sugars, with a Focus on Beverages and the Associations with Micronutrient Adequacy in US Children, Adolescents, and Teens (NHANES 2003–2018)" Nutrients 15, no. 15: 3285. https://doi.org/10.3390/nu15153285
APA StyleRicciuto, L., Fulgoni, V. L., III, Gaine, P. C., Scott, M. O., & DiFrancesco, L. (2023). Intakes of Added Sugars, with a Focus on Beverages and the Associations with Micronutrient Adequacy in US Children, Adolescents, and Teens (NHANES 2003–2018). Nutrients, 15(15), 3285. https://doi.org/10.3390/nu15153285