
Precarious Young Adults’ Mental Health during the Pandemic: The Major Impact of Food Insecurity Independently of COVID-19 Diagnosis

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Measures
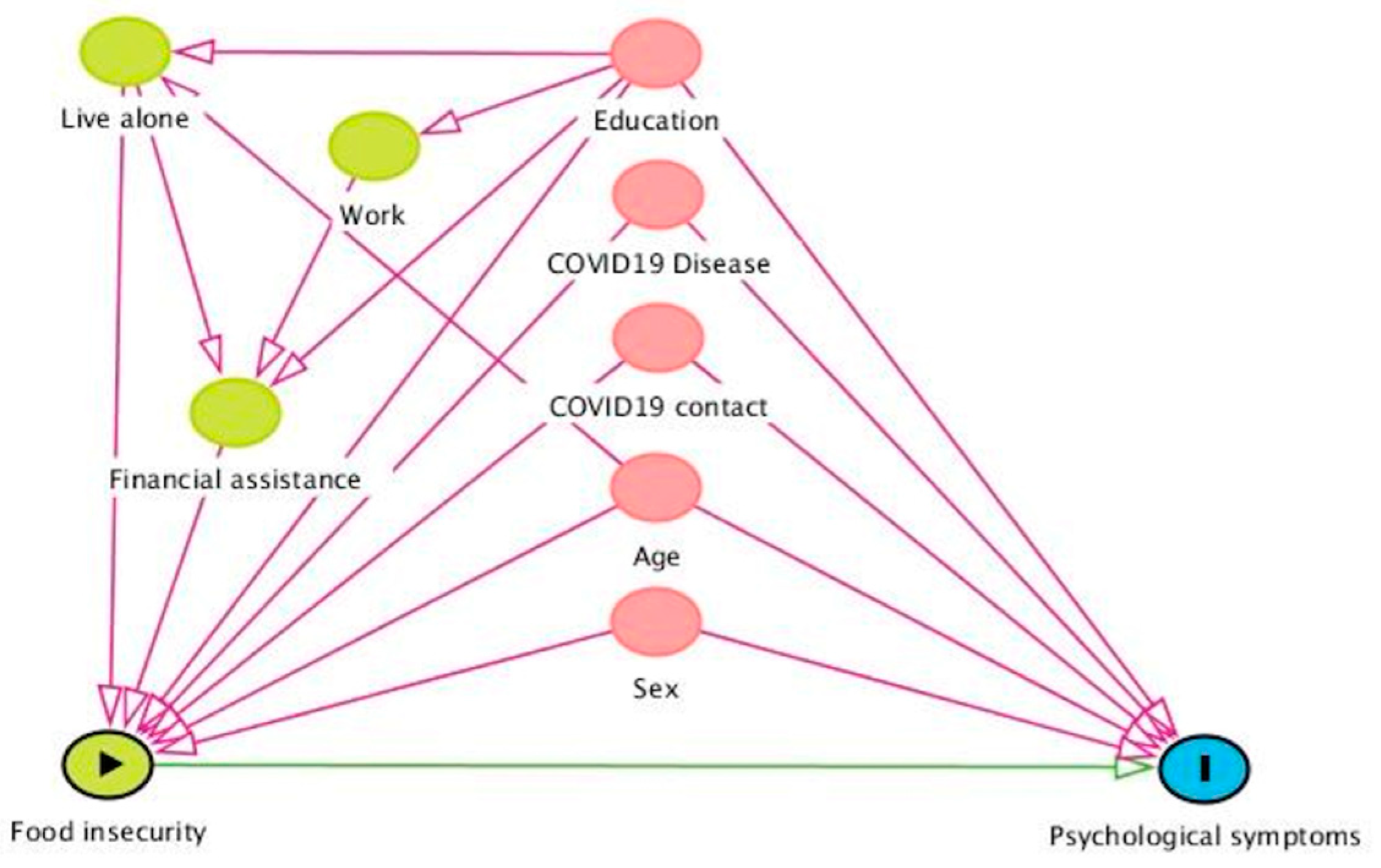
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Mental Health
3.3. Factors Associated with Depression, Anxiety, Distress and Suicidal Ideation
4. Discussion
4.1. Prevalence
4.2. Food Insecurity
4.3. Limits
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Min, K.-B.; Park, S.-G.; Hwang, S.H.; Min, J.-Y. Precarious employment and the risk of suicidal ideation and suicide attempts. Prev. Med. 2015, 71, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Elbogen, E.B.; Lanier, M.; Blakey, S.M.; Wagner, H.R.; Tsai, J. Suicidal ideation and thoughts of self-harm during the COVID-19 pandemic: The role of COVID-19-related stress, social isolation, and financial strain. Depress. Anxiety 2021, 38, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Wresinski, J. Grande Pauvreté et Précarité Économique et Sociale; Journal Officiel: Paris, France, 1987. [Google Scholar]
- Scarlett, H.; Davisse-Paturet, C.; Longchamps, C.; Aarbaoui, T.E.; Allaire, C.; Colleville, A.-C.; Convence-Arulthas, M.; Crouzet, L.; Ducarroz, S.; Melchior, M. Depression during the COVID-19 pandemic amongst residents of homeless shelters in France. J. Affect. Disord. Rep. 2021, 6, 100243. [Google Scholar] [CrossRef]
- Glowacz, F.; Schmits, E. Psychological distress during the COVID-19 lockdown: The young adults most at risk. Psychiatry Res. 2020, 293, 113486. [Google Scholar] [CrossRef] [PubMed]
- Ayuso-Mateos, J.L.; Morillo, D.; Haro, J.M.; Olaya, B.; Lara, E.; Miret, M. Changes in depression and suicidal ideation under severe lockdown restrictions during the first wave of the COVID-19 pandemic in Spain: A longitudinal study in the general population. Epidemiol. Psychiatr. Sci. 2021, 30, e49. [Google Scholar] [CrossRef] [PubMed]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors Associated with Mental Health Disorders among University Students in France Confined during the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar] [CrossRef]
- Essadek, A.; Rabeyron, T. Mental health of French students during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 392–393. [Google Scholar] [CrossRef]
- Brown, A.D.; Seligman, H.; Sliwa, S.; Barnidge, E.; Krupsky, K.L.; Demissie, Z.; Liese, A.D. Food Insecurity and Suicidal Behaviors among US High School Students. J. Sch. Health 2022, 92, 898–906. [Google Scholar] [CrossRef]
- Essadek, A.; Gressier, F.; Krebs, T.; Corruble, E.; Falissard, B.; Rabeyron, T. Assessment of mental health of university students faced with different lockdowns during the coronavirus pandemic, a repeated cross-sectional study. Eur. J. Psychotraumatol. 2022, 13, 2141510. [Google Scholar] [CrossRef]
- Hodgson, K.J.; Shelton, K.H.; van den Bree, M.B.M. Psychopathology among young homeless people: Longitudinal mental health outcomes for different subgroups. Br. J. Clin. Psychol. 2015, 54, 307–325. [Google Scholar] [CrossRef]
- Vancea, M.; Shore, J.; Utzet, M. Role of employment-related inequalities in young adults’ life satisfaction: A comparative study in five European welfare state regimes. Scand. J. Public Health 2019, 47, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Melchior, M.; Chastang, J.F.; Falissard, B.; Galèra, C.; Tremblay, R.; Côtè, S.; Boivin, M. EPA-0669—Food insecurity and children’s symptoms of hyperactivity and inattention. Eur. Psychiatry 2014, 29, 1. [Google Scholar] [CrossRef]
- Fang, D.; Thomsen, M.R.; Nayga, R.M. The association between food insecurity and mental health during the COVID-19 pandemic. BMC Public Health 2021, 21, 607. [Google Scholar] [CrossRef]
- Polsky, J.Y.; Gilmour, H. Food insecurity and mental health during the COVID-19 pandemic. Health Rep. 2020, 31, 3–11. [Google Scholar] [CrossRef]
- Rogers, A.M.; Lauren, B.N.; Woo Baidal, J.A.; Ozanne, E.M.; Hur, C. Persistent effects of the COVID-19 pandemic on diet, exercise, risk for food insecurity, and quality of life: A longitudinal study among U.S. adults. Appetite 2021, 167, 105639. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef]
- Guo, Q.; Zheng, Y.; Shi, J.; Wang, J.; Li, G.; Li, C.; Fromson, J.A.; Xu, Y.; Liu, X.; Xu, H.; et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: A mixed-method study. Brain. Behav. Immun. 2020, 88, 17–27. [Google Scholar] [CrossRef]
- Leung, T.Y.M.; Chan, A.Y.L.; Chan, E.W.; Chan, V.K.Y.; Chui, C.S.L.; Cowling, B.J.; Gao, L.; Ge, M.Q.; Hung, I.F.N.; Ip, M.S.M.; et al. Short- and potential long-term adverse health outcomes of COVID-19: A rapid review. Emerg. Microbes Infect. 2020, 9, 2190–2199. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2021, 19, 1875–1888. [Google Scholar] [CrossRef]
- Miller, L.; Déchelotte, P.; Ladner, J.; Tavolacci, M.-P. Effect of the COVID-19 Pandemic on Healthy Components of Diet and Factors Associated with Unfavorable Changes among University Students in France. Nutrients 2022, 14, 3862. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, M.; Lapierre, S.; Balbinotti, M.A.A.; Desjardins, S.; Vasiliadis, H.-M. Validation de contenu de la version francophone du questionnaire Impact of Event Scale-Revised selon les critères du DSM-5. Prat. Psychol. 2018, 24, 21–34. [Google Scholar] [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. CMAJ 2012, 184, E191–E196. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated with Mental Health Outcomes among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Wathelet, M.; Fovet, T.; Jousset, A.; Duhem, S.; Habran, E.; Horn, M.; Debien, C.; Notredame, C.-E.; Baubet, T.; Vaiva, G.; et al. Prevalence of and factors associated with post-traumatic stress disorder among French university students 1 month after the COVID-19 lockdown. Transl. Psychiatry 2021, 11, 327. [Google Scholar] [CrossRef]
- Rossom, R.C.; Coleman, K.J.; Ahmedani, B.K.; Beck, A.; Johnson, E.; Oliver, M.; Simon, G.E. Suicidal ideation reported on the PHQ9 and risk of suicidal behavior across age groups. J. Affect. Disord. 2017, 215, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis; Macmillan: New York, NY, USA, 1995. [Google Scholar]
- Shrier, I.; Platt, R.W. Reducing bias through directed acyclic graphs. BMC Med. Res. Methodol. 2008, 8, 70. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef] [PubMed]
- Winkler, P.; Mohrova, Z.; Mlada, K.; Kuklova, M.; Kagstrom, A.; Mohr, P.; Formanek, T. Prevalence of current mental disorders before and during the second wave of COVID-19 pandemic: An analysis of repeated nationwide cross-sectional surveys. J. Psychiatr. Res. 2021, 139, 167–171. [Google Scholar] [CrossRef]
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; Symonds, M.E.; Miraghajani, M. Food insecurity and mental health: A systematic review and meta-analysis. Public Health Nutr. 2020, 23, 1778–1790. [Google Scholar] [CrossRef]
- Bruening, M.; Dinour, L.M.; Chavez, J.B.R. Food insecurity and emotional health in the USA: A systematic narrative review of longitudinal research. Public Health Nutr. 2017, 20, 3200–3208. [Google Scholar] [CrossRef] [PubMed]
- Huddleston-Casas, C.; Charnigo, R.; Simmons, L.A. Food insecurity and maternal depression in rural, low-income families: A longitudinal investigation. Public Health Nutr. 2009, 12, 1133–1140. [Google Scholar] [CrossRef]
- Nagata, J.M.; Palar, K.; Gooding, H.C.; Garber, A.K.; Whittle, H.J.; Bibbins-Domingo, K.; Weiser, S.D. Food Insecurity Is Associated With Poorer Mental Health and Sleep Outcomes in Young Adults. J. Adolesc. Health 2019, 65, 805–811. [Google Scholar] [CrossRef]
- Christian, V.J.; Miller, K.R.; Martindale, R.G. Food Insecurity, Malnutrition, and the Microbiome. Curr. Nutr. Rep. 2020, 9, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Pryor, L.; Lioret, S.; van der Waerden, J.; Fombonne, É.; Falissard, B.; Melchior, M. Food insecurity and mental health problems among a community sample of young adults. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Loh, I.H.; Oddo, V.M.; Otten, J. Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers. Int. J. Environ. Res. Public. Health 2020, 18, 170. [Google Scholar] [CrossRef]
- Oswald, T.K.; Rumbold, A.R.; Kedzior, S.G.E.; Kohler, M.; Moore, V.M. Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature. Int. J. Environ. Res. Public. Health 2021, 18, 5630. [Google Scholar] [CrossRef]
- Whittle, H.J.; Palar, K.; Seligman, H.K.; Napoles, T.; Frongillo, E.A.; Weiser, S.D. How food insecurity contributes to poor HIV health outcomes: Qualitative evidence from the San Francisco Bay Area. Soc. Sci. Med. 2016, 170, 228–236. [Google Scholar] [CrossRef]
- Niles, M.T.; Bertmann, F.; Belarmino, E.H.; Wentworth, T.; Biehl, E.; Neff, R. The Early Food Insecurity Impacts of COVID-19. Nutrients 2020, 12, 2096. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.I.; Lachaud, J.; Hwang, S.W.; Mejia-Lancheros, C. Food insecurity and mental health outcomes among homeless adults: A scoping review. Public Health Nutr. 2021, 24, 1766–1777. [Google Scholar] [CrossRef]
- Owens, M.R.; Brito-Silva, F.; Kirkland, T.; Moore, C.E.; Davis, K.E.; Patterson, M.A.; Miketinas, D.C.; Tucker, W.J. Prevalence and Social Determinants of Food Insecurity among College Students during the COVID-19 Pandemic. Nutrients 2020, 12, 2515. [Google Scholar] [CrossRef] [PubMed]
- Palar, K.; Frongillo, E.A.; Escobar, J.; Sheira, L.A.; Wilson, T.E.; Adedimeji, A.; Merenstein, D.; Cohen, M.H.; Wentz, E.L.; Adimora, A.A.; et al. Food Insecurity, Internalized Stigma, and Depressive Symptoms among Women Living with HIV in the United States. AIDS Behav. 2018, 22, 3869–3878. [Google Scholar] [CrossRef] [PubMed]
- Keenan, G.S.; Christiansen, P.; Owen, L.J.; Hardman, C.A. The association between COVID-19 related food insecurity and weight promoting eating behaviours: The mediating role of distress and eating to cope. Appetite 2022, 169, 105835. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Arnaiz, M. The precarisation of daily life in Spain: Austerity, social policy and food insecurity. Appetite 2022, 171, 105906. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total n = 823 n (%) or Mean [SD] |
|---|---|
| Age | 21.23 [2.11] |
| Gender | |
| Female | 410 (49.82) |
| Level | |
| Higher than baccalaureate | 116 (14.10) |
| Baccalaureate | 281 (34.14) |
| Lower than baccalaureate | 426 (51.76) |
| Accommodation | |
| Family | 514 (62.5) |
| Tenant | 178 (21.6) |
| Emergency shelter | 65 (7.9) |
| Homeless | 66 (8) |
| Live Alone | |
| Yes | 257 (31.23) |
| Financial assistance | |
| Yes | 195 (23.69) |
| Jobless | |
| Yes | 645 (78.37) |
| Financial resources | |
| No resource | 413 (50.18) |
| <500 Euros | 220 (26.73) |
| >500 et <1000 Euros | 132 (16.04) |
| >à 1000 Euros | 58 (7.05) |
| COVID | |
| Confirmed | 56 (6.81) |
| COVID contact | |
| Yes | 195 (23.69) |
| Food Consumption | |
| 3 meals a day | 429 (52.13) |
| 1 meal per day | 353 (42.89) |
| <than 1 meal a day | 41 (4.98) |
| Psychiatric symptoms | |
| PHQ-9 | 9.35 [2.11] |
| GAD-7 | 6.37 [5.96] |
| IES-R | 22.35 [5.96] |
| Psychiatric symptoms with cut-offs | |
| PHQ-9 ≥ 10 | 378 (45.93) |
| GAD-7 ≥ 8 | 302 (36.69) |
| IES-R ≥ 26 | 321 (39.00) |
| Suicidal ideation | 209 (25.39) |
| Depression (PHQ-9) | Anxiety (GAD-7) | Distress (IES-R) | Suicidal Ideation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Affected No. (%) | Odds Ratio (95%IC) | p-Value | Affected No. (%) | Odds Ratio (95%IC) | p-Value | Affected No. (%) | Odds Ratio (95%IC) | p-Value | Affected No. (%) | Odds Ratio (95%IC) | p-Value | |
| SEX | ||||||||||||
| MALE | 173 (45.77) | REFERENCE | NA | 133 (44.04) | REFERENCE | NA | 161 (50.16) | REFERENCE | NA | 105 (50.24) | REFERENCE | NA |
| FEMALE | 205 (54.23) | 1.39 (1.05–1.83) | 0.02 | 169 (55.96) | 1.47 (1.11–1.96) | 0.007 | 160 (49.84) | 1 (0.76–1.33) | 1 | 104 (49.76) | 1 (0.73–1.37) | 1 |
| LEVEL STUDY | ||||||||||||
| HIGHER THAN BACCALAUREATE | 59 (15.61) | REFERENCE | NA | 50 (16.56) | REFERENCE | NA | 47 (14.64) | REFERENCE | NA | 26 (12.44) | REFERENCE | NA |
| BACCALAUREATE | 140 (37.04) | 0.95 (0.62–1.48) | 0.09 | 114 (37.75) | 0.90 (0.58–1.39) | 0.66 | 108 (33.65) | 0.91 (0.59–1.42) | 0.74 | 71 (33.97) | 1.17 (0.70–1.95) | 0.61 |
| LOWER THAN BACCALAUREATE | 179 (47.35) | 0.70 (0.46–1.06) | 0.09 | 138 (45.69) | 0.63 (0.41–0.96) | 0.04 | 166 (51.71) | 0.93 (0.62–1.42) | 0.83 | 112 (53.59) | 1.23 (0.76–2.01) | 0.47 |
| HOUSING | ||||||||||||
| FAMILY | 236 (62.43) | REFERENCE | NA | 182 (60.27) | REFERENCE | NA | 186 (57.94) | REFERENCE | NA | 108 (51.67) | REFERENCE | NA |
| TENANT | 78 (20.64) | 0.91 (0.65–1.29) | 0.66 | 65 (21.52) | 1.05 (0.73–1.49) | 0.79 | 73 (22.74) | 1.22 (0.86–1.73) | 0.28 | 51 (24.40) | 1.51 (1.02–2.22) | 0.04 |
| EMERGENCY SHELTER | 31 (8.20) | 1.07 (0.64–1.80) | 0.79 | 25 (8.28) | 1.14 (0.67–1.94) | 0.68 | 31 (9.66) | 1.60 (0.96–2.70) | 0.08 | 22 (10.53) | 1.92 (1.10–3.35) | 0.03 |
| HOMELESS | 33 (8.73) | 1.79 (0.70–1.97) | 0.60 | 30 (9.93) | 1.52 (0.90–2.54) | 0.13 | 31 (9.66) | 1.56 (0.93–2.61) | 0.10 | 28 (13.40) | 2.77 (1.62–4.71) | <0.001 |
| FINANCIAL RESOURCES | ||||||||||||
| >1000 €UROS | 22 (5.82) | REFERENCE | NA | 21 (6.95) | REFERENCE | NA | 12 (3.74) | REFERENCE | NA | 8 (3.83) | REFERENCE | NA |
| >500 ET < 1000 €UROS | 68 (17.99) | 1.73 (0.92–3.26) | 0.11 | 57 (18.87) | 1.34 (0.71–2.53) | 0.43 | 55 (17.13) | 2.73 (1.33–5.64) | 0.005 | 36 (17.22) | 2.34 (1.01–5.42) | 0.06 |
| <500 €UROS | 101 (26.72) | 1.39 (0.77–2.51) | 0.30 | 81 (26.83) | 1.03 (0.56–1.87) | 1 | 98 (30.53) | 3.08 (1.55–6.13) | <0.001 | 61 (39.19) | 2.39 (1.07–5.35) | 0.04 |
| NO RESOURCES | 187 (49.47) | 1.35 (0.77–2.38) | 0.32 | 143 (47.35) | 0.93 (0.53–1.65) | 0.88 | 156 (48.60) | 2.32 (1.29–4.53) | 0.01 | 104 (49.76) | 2.10 (0.96–4.58) | 0.07 |
| LIVE ALONE | ||||||||||||
| NO | 249 (65.87) | REFERENCE | NA | 195 (64.57) | REFERENCE | NA | 206 (64.17) | REFERENCE | NA | 121 (57.89) | REFERENCE | NA |
| YES | 129 (34.13) | 1.28 (0.95–1.72) | 0.11 | 107 (35.43) | 1.36 (1.00–1.84) | 0.05 | 115 (35.83) | 1.41 (1.05–1.91) | 0.025 | 88 (42.11) | 1.91 [1.38–2.65] | <0.001 |
| WORKING | ||||||||||||
| YES | 72 (19.05) | REFERENCE | NA | 63 (20.86) | REFERENCE | NA | 57 (17.76) | REFERENCE | NA | 43 (20.57) | REFERENCE | NA |
| NO | 306 80.95) | 1.32 (0.95–1.86) | 0.11 | 239 (79.14) | 1.07 (0.76–1.52) | 0.73 | 264 (82.24) | 1.47 (1.03–2.09) | 0.04 | 166 (79.43) | 1.08 [0.74–1.60] | 0.70 |
| COVID DIAGNOSIS | ||||||||||||
| NO | 344 (91.01) | REFERENCE | NA | 272 (90.07) | REFERENCE | NA | 292 (90.96) | REFERENCE | NA | 194 (92.82) | REFERENCE | NA |
| YES | 34 (8.99) | 1.90 (1.09–3.31) | 0.025 | 30 (9.93) | 2.09 (1.21–3.62) | 0.009 | 29 (9.04) | 1.74 (0.97–3.13) | 0.047 | 15 (7.18) | 1.08 (0.58–1.99) | 0.87 |
| COVID CONTACT | ||||||||||||
| NO | 266 (70.37) | REFERENCE | NA | 216 (71.52) | REFERENCE | NA | 228 (71.03) | REFERENCE | NA | 162 (77.51) | REFERENCE | NA |
| YES | 112 (29.63) | 1.83 (1.32–2.54) | <0.001 | 86 (28.48) | 1.50 (1.08–2.09) | 0.02 | 93 (28.97) | 1.83 (1.32–2.54) | <0.001 | 47 (22.49) | 0.91 (0.63–1.33) | 0.71 |
| FOOD INSECURITY | ||||||||||||
| 2 AND MORE MEALS | 163 (43.12) | REFERENCE | NA | 134 (44.36) | REFERENCE | NA | 140 (43.62) | REFERENCE | NA | 77 (36.84) | REFERENCE | NA |
| 1 MEAL | 193 (51.06) | 1.97 (1.48–2.62) | <0.001 | 148 (49.01) | 1.59 (1.18–2.13) | 0.002 | 160 (49.84) | 1.71 (1.27–2.29) | <0.001 | 111 (53.11) | 2.1 (1.50–2.93) | <0.001 |
| <1 MEAL | 22 (5.82) | 1.89 (0.99–3.59) | 0.07 | 22 (7.28) | 2.10 (1.10–4.00) | 0.04 | 21 (6.54) | 2.16 (1.14–4.13) | 0.02 | 21 (10.05) | 4.8 (2.48–9.29) | <0.001 |
| Depression (PHQ-9) | Anxiety (GAD-7) | Distress (IES-R) | Suicidal Ideation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Affected No. (%) | Odds-Ratio (95%IC) | p-Value | Affected No. (%) | Odds-Ratio (95%IC) | p-Value | Affected No. (%) | Odds-Ratio (95%IC) | p-Value | Affected No. (%) | Odds-Ratio (95%IC) | p-Value | |
| FOOD INSECURITY | ||||||||||||
| 2 AND MORE MEALS | 163 (43.12) | REFERENCE | NA | 134 (44.36) | REFERENCE | NA | 140 (43.62) | REFERENCE | NA | 77 (36.84) | REFERENCE | NA |
| 1 MEAL | 193 (51.06) | 2.11 (1.57–2.84) | <0.001 | 148 (49.01) | 1.70 (1.25–2.30) | 0.001 | 160 (49.84) | 1.71 (1.27–2.30) | 0.001 | 111 (53.11) | 2.10 (1.50–2.96) | <0.001 |
| <1 MEAL | 22 (5.82) | 2.30 (1.19–4.51) | 0.005 | 22 (7.28) | 2.51 (1.29–4.88) | 0.006 | 21 (6.54) | 2.36 (1.23–4.57) | 0.01 | 21 (10.05) | 4.81 (2.46–9.44) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Essadek, A.; Shadili, G.; Bergami Goulart Barbosa, P.; Assous, A.; Widart, F.; Payan, S.; Rabeyron, T.; Corruble, E.; Falissard, B.; Gressier, F. Precarious Young Adults’ Mental Health during the Pandemic: The Major Impact of Food Insecurity Independently of COVID-19 Diagnosis. Nutrients 2023, 15, 3260. https://doi.org/10.3390/nu15143260
Essadek A, Shadili G, Bergami Goulart Barbosa P, Assous A, Widart F, Payan S, Rabeyron T, Corruble E, Falissard B, Gressier F. Precarious Young Adults’ Mental Health during the Pandemic: The Major Impact of Food Insecurity Independently of COVID-19 Diagnosis. Nutrients. 2023; 15(14):3260. https://doi.org/10.3390/nu15143260
Chicago/Turabian StyleEssadek, Aziz, Gérard Shadili, Pablo Bergami Goulart Barbosa, Adèle Assous, Frédéric Widart, Ségolène Payan, Thomas Rabeyron, Emmanuelle Corruble, Bruno Falissard, and Florence Gressier. 2023. "Precarious Young Adults’ Mental Health during the Pandemic: The Major Impact of Food Insecurity Independently of COVID-19 Diagnosis" Nutrients 15, no. 14: 3260. https://doi.org/10.3390/nu15143260
APA StyleEssadek, A., Shadili, G., Bergami Goulart Barbosa, P., Assous, A., Widart, F., Payan, S., Rabeyron, T., Corruble, E., Falissard, B., & Gressier, F. (2023). Precarious Young Adults’ Mental Health during the Pandemic: The Major Impact of Food Insecurity Independently of COVID-19 Diagnosis. Nutrients, 15(14), 3260. https://doi.org/10.3390/nu15143260