
A Pilot Study Examining the Association of Parental Stress and Household Food Insecurity with Dietary Quality in Pre-School-Aged Children

Abstract
1. Introduction
2. Methods
2.1. Study Overview
2.2. Participants
2.3. Measures
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muñoz, K.A.; Krebs-Smith, S.M.; Ballard-Barbash, R.; Cleveland, L.E. Food intakes of US children and adolescents compared with recommendations. Pediatrics 1997, 100 Pt 1, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Micha, R.; Li, Y.; Mozaffarian, D. Trends in Food Sources and Diet Quality Among US Children and Adults, 2003–2018. JAMA Netw. Open 2021, 4, e215262. [Google Scholar] [CrossRef] [PubMed]
- Banfield, E.C.; Liu, Y.; Davis, J.S.; Chang, S.; Frazier-Wood, A.C. Poor Adherence to US Dietary Guidelines for Children and Adolescents in the National Health and Nutrition Examination Survey Population. J. Acad. Nutr. Diet. 2016, 116, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Molani Gol, R.; Kheirouri, S.; Alizadeh, M. Association of Dietary Diversity with Growth Outcomes in Infants and Children Aged under 5 Years: A Systematic Review. J. Nutr. Educ. Behav. 2022, 54, 65–83. [Google Scholar] [CrossRef] [PubMed]
- Dave, J.M.; Evans, A.E.; Saunders, R.P.; Watkins, K.W.; Pfeiffer, K.A. Associations among food insecurity, acculturation, demographic factors, and fruit and vegetable intake at home in Hispanic children. J. Am. Diet Assoc. 2009, 109, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Fisk, C.M.; Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Robinson, S.M.; Southampton Women’s Survey Study Group. Influences on the quality of young children’s diets: The importance of maternal food choices. Br. J. Nutr. 2011, 105, 287–296. [Google Scholar] [CrossRef]
- Papas, M.A.; Hurley, K.M.; Quigg, A.M.; Oberlander, S.E.; Black, M.M. Low-income, African American adolescent mothers and their toddlers exhibit similar dietary variety patterns. J. Nutr. Educ. Behav. 2009, 41, 87–94. [Google Scholar] [CrossRef]
- Cullen, K.W.; Baranowski, T.; Owens, E.; Marsh, T.; Rittenberry, L.; de Moor, C. Availability, accessibility, and preferences for fruit, 100% fruit juice, and vegetables influence children’s dietary behavior. Health Educ. Behav. 2003, 30, 615–626. [Google Scholar] [CrossRef]
- Laster, L.E.; Lovelady, C.A.; West, D.G.; Wiltheiss, G.A.; Brouwer, R.J.; Stroo, M.; Østbye, T. Diet quality of overweight and obese mothers and their preschool children. J. Acad. Nutr. Diet. 2013, 113, 1476–1483. [Google Scholar] [CrossRef]
- Jang, M.; Brown, R.; Vang, P.Y. The Relationships between Parental Stress, Home Food Environment, and Child Diet Patterns in Families of Preschool Children. Am. J. Health Promot. 2021, 35, 131–139. [Google Scholar] [CrossRef]
- Coleman-Jensen, A.R.; Matthew, P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2020; ERR-298; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2021. [Google Scholar]
- Darling, K.E.; Fahrenkamp, A.J.; Wilson, S.M.; D’Auria, A.L.; Sato, A.F. Physical and mental health outcomes associated with prior food insecurity among young adults. J. Health Psychol. 2017, 22, 572–581. [Google Scholar] [CrossRef]
- Thomas, M.M.C.; Miller, D.P.; Morrissey, T.W. Food Insecurity and Child Health. Pediatrics 2019, 144, e20190397. [Google Scholar] [CrossRef]
- Alaimo, K.; Olson, C.M.; Frongillo, E.A., Jr.; Briefel, R.R. Food insufficiency, family income, and health in US preschool and school-aged children. Am. J. Public Health 2001, 91, 781. [Google Scholar]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in US adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef]
- Cain, K.S.; Meyer, S.C.; Cummer, E.; Patel, K.K.; Casacchia, N.J.; Montez, K.; Palakshappa, D.; Brown, C.L. Association of Food Insecurity with Mental Health Outcomes in Parents and Children: A Systematic Review. Acad. Pediatr. 2022, 22, 1105–1114. [Google Scholar] [CrossRef]
- Minkin, R.; Horowitz, J.M. Parenting in America Today; Pew Research Center: Washington, DC, USA, 2023. [Google Scholar]
- Baskind, M.J. Parent-Perceived Stress and Its Association with Children’s BMI and Obesity-Related Behaviors. Ph.D. Thesis, Harvard University, Cambridge, MA, USA, 2018. [Google Scholar]
- Parks, E.P.; Kumanyika, S.; Moore, R.H.; Stettler, N.; Wrotniak, B.H.; Kazak, A. Influence of stress in parents on child obesity and related behaviors. Pediatrics 2012, 130, e1096–e1104. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- Dean, G.; Vitolins, M.Z.; Skelton, J.A.; Ip, E.H.; Lucas, C.B.; Brown, C.L. The association of food insecurity with mental health in preschool-aged children and their parents. Pediatr. Res. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Anderson, C.B.; Hughes, S.O.; Fisher, J.O.; Nicklas, T.A. Cross-cultural equivalence of feeding beliefs and practices: The psychometric properties of the child feeding questionnaire among Blacks and Hispanics. Prev. Med. 2005, 41, 521–531. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Frank, D.A. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [PubMed]
- Nord, M. Household Food Security in the United States (2008); DIANE Publishing: Collingdale, PA, USA, 2010. [Google Scholar]
- Arterburn, D.; Ichikawa, L.; Ludman, E.J.; Operskalski, B.; Linde, J.A.; Anderson, E.; Simon, G.E. Validity of clinical body weight measures as substitutes for missing data in a randomized trial. Obes. Res. Clin. Pract. 2008, 2, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States. Adv. Data 2000, 314, 1–27. [Google Scholar]
- Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Wilson, M.M.; Tooze, J.A. Applications of the Healthy Eating Index for Surveillance, Epidemiology, and Intervention Research: Considerations and Caveats. J. Acad. Nutr. Diet. 2018, 118, 1603–1621. [Google Scholar] [CrossRef]
- Jansen, E.; Thapaliya, G.; Aghababian, A.; Sadler, J.; Smith, K.; Carnell, S. Parental stress, food parenting practices and child snack intake during the COVID-19 pandemic. Appetite 2021, 161, 105119. [Google Scholar] [CrossRef]
- O’Connor, S.G.; Huh, J.; Schembre, S.M.; Lopez, N.V.; Dunton, G.F. The Association of Maternal Perceived Stress with Changes in Their Children’s Healthy Eating Index (HEI-2010) Scores Over Time. Ann. Behav. Med. Publ. Soc. Behav. Med. 2019, 53, 877–885. [Google Scholar] [CrossRef]
- Asfour, L.; Natale, R.; Uhlhorn, S.; Arheart, K.L.; Haney, K.; Messiah, S.E. Ethnicity, household food security, and Nutrition and activity patterns in families with preschool children. J. Nutr. Educ. Behav. 2015, 47, 498–505.e491. [Google Scholar] [CrossRef]
- Rossen, L.M.; Kobernik, E.K. Food insecurity and dietary intake among US youth, 2007–2010. Pediatr. Obes. 2016, 11, 187–193. [Google Scholar] [CrossRef]
- Nicklas, T.; Johnson, R. Position of the American Dietetic Association: Dietary guidance for healthy children ages 2 to 11 years. J. Am. Diet. Assoc. 2004, 104, 660–677. [Google Scholar]


{kind=link}
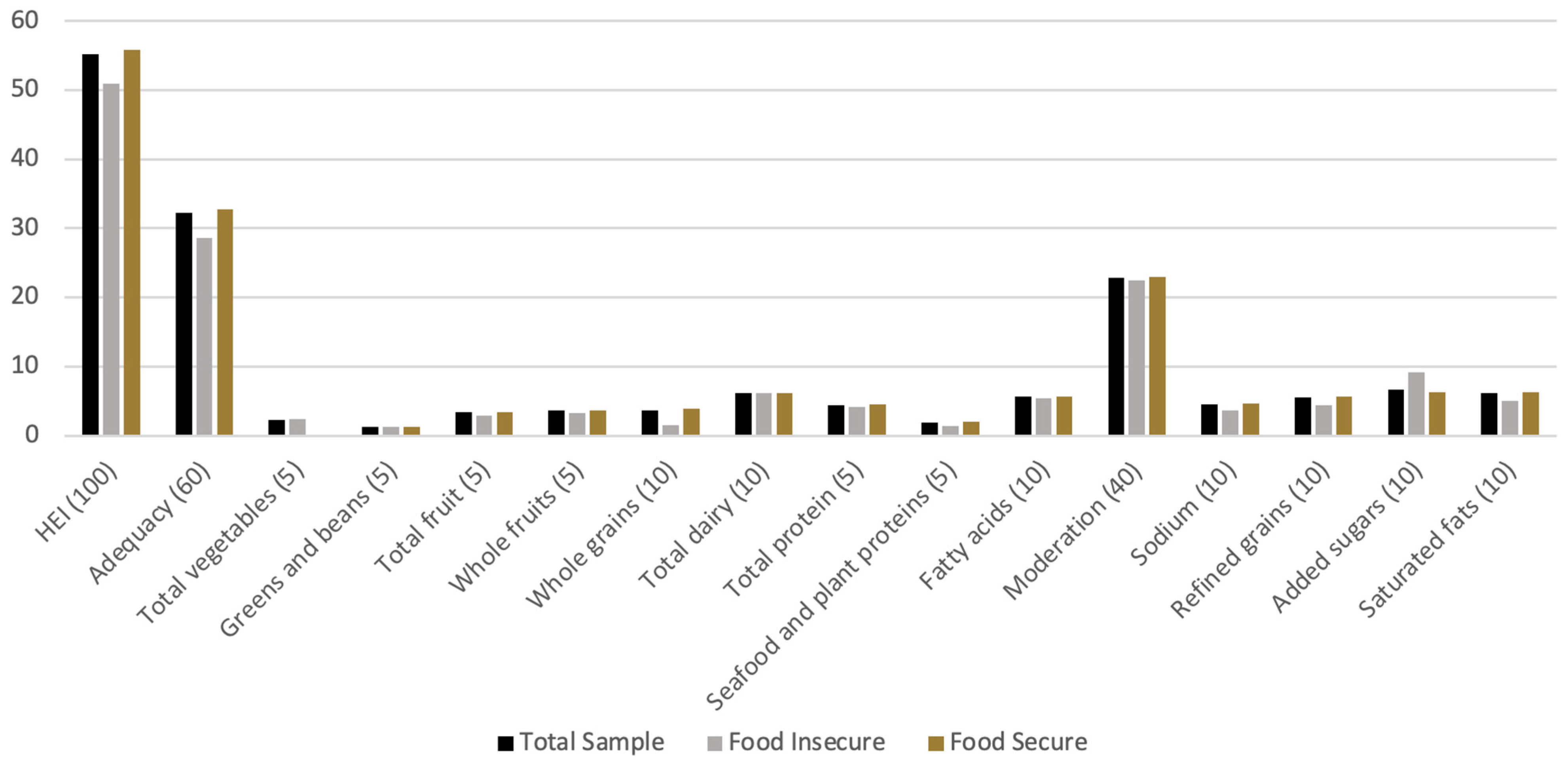
| Variable | Maximum Points | Total Sample Mean (SD) | Food Insecure Mean (SD) | Food Secure Mean (SD) | Effect Size | p-Value |
|---|---|---|---|---|---|---|
| HEI | 100 | 55.2 (10.9) | 51.0 (11.1) | 55.8 (11.0) | 0.44 | 0.5 |
| Adequacy | 60 | 32.2 (7.4) | 28.6 (6.2) | 32.8 (7.5) | 0.56 | 0.4 |
| Total vegetables | 5 | 2.2 (1.5) | 2.4 (1.0) | 2.2 (1.5) | 0.13 | 0.8 |
| Greens and beans | 5 | 1.2 (1.7) | 1.3 (1.5) | 1.2 (1.8) | 0.06 | 0.9 |
| Total fruit | 5 | 3.4 (1.6) | 2.9 (1.9) | 3.4 (1.6) | 0.31 | 0.6 |
| Whole fruits | 5 | 3.6 (1.5) | 3.3 (2.8) | 3.6 (1.3) | 0.23 | 0.7 |
| Whole grains | 10 | 3.6 (3.5) | 1.5 (1.3) | 3.9 (2.3) | 1.04 | 0.3 |
| Total dairy | 10 | 6.2 (2.9) | 6.2 (2.5) | 6.2 (2.9) | 0.00 | 0.9 |
| Total protein | 5 | 4.4 (0.8) | 4.2 (0.7) | 4.5 (0.8) | 0.38 | 0.6 |
| Seafood and plant proteins | 5 | 1.9 (2.0) | 1.4 (1.6) | 2.0 (2.1) | 0.29 | 0.6 |
| Fatty acids | 10 | 5.7 (3.5) | 5.4 (5.0) | 5.7 (3.4) | 0.09 | 0.9 |
| Moderation | 40 | 22.9 (4.6) | 22.4 (5.1) | 23.0 (4.6) | 0.13 | 0.8 |
| Sodium | 10 | 4.5 (2.6) | 3.7 (2.9) | 4.7 (2.6) | 0.38 | 0.6 |
| Refined grains | 10 | 5.5 (3.1) | 4.4 (5.1) | 5.7 (2.9) | 0.45 | 0.5 |
| Added sugars | 10 | 6.7 (2.4) | 9.2 (0.9) | 6.3 (2.3) | 1.26 | 0.04 |
| Saturated fats | 10 | 6.2 (2.7) | 5.0 (2.4) | 6.3 (2.7) | 0.48 | 0.4 |
| Separate Models with Dependent Variable of HEI Dietary Quality Component | Household Food Insecurity Beta (95%CI) | Parental Stress Beta (95%CI) | Income USD 20,000–USD 60,000 a Beta (95%CI) | Income USD 60,000 + a Beta (95%CI) | Child BMIz Beta (95%CI) | Male Sex Beta (95%CI) |
|---|---|---|---|---|---|---|
| HEI score (overall dietary quality) | −6.7 | −3.9 | −3.0 | 0.2 | −0.5 | 0.6 |
| Adequacy subscale | −5.7 | −3.6 | −1.1 | −0.003 | −0.6 | 1.0 |
| Total vegetables | 1.7 | −1.2 + | 2.3 * | 1.0 | 0.2 | −0.4 |
| Greens and beans | 0.4 | −1.5 * | 0.1 | −0.2 | 0.2 | −0.6 |
| Total fruit | −1.0 | 1.1 | −1.2 | −0.8 | 0.3 | 0.6 |
| Whole fruits | 0.001 | 0.6 | −0.2 | 0.6 | 0.1 | 0.1 |
| Whole grains | −1.1 | −1.0 | 0.6 | 4.0 + | −0.5 | −1.1 |
| Total dairy | 0.4 | 1.3 | −0.3 | −0.2 | 0.3 | −1.0 |
| Total protein | −1.3 * | −0.4 | −0.6 | −0.7 + | −0.3 * | 0.3 |
| Seafood and plant proteins | −0.4 | −1.3 | 1.0 | −0.4 | 0.2 | 0.3 |
| Fatty acids | −4.4 + | −1.3 | −2.8 | −3.2 | −1.1 + | 2.5 + |
| Moderation subscale | −1.0 | −0.3 | −1.9 | 0.02 | 0.1 | −0.4 |
| Sodium | 1.9 | 1.2 | 1.1 | 3.5 * | 0.8 + | 0.8 |
| Refined grains | −3.0 | −0.4 | −1.8 | −1.7 | −0.4 | −0.8 |
| Added sugars | 4.1 * | −1.5 | 2.1 | 1.1 | −0.05 | −1.8 + |
| Saturated fats | −4.1 + | 0.4 | −3.3 + | −2.8 + | −0.2 | 1.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCarthy, M.; Vitolins, M.Z.; Skelton, J.A.; Ip, E.H.; Brown, C.L. A Pilot Study Examining the Association of Parental Stress and Household Food Insecurity with Dietary Quality in Pre-School-Aged Children. Nutrients 2023, 15, 3154. https://doi.org/10.3390/nu15143154
McCarthy M, Vitolins MZ, Skelton JA, Ip EH, Brown CL. A Pilot Study Examining the Association of Parental Stress and Household Food Insecurity with Dietary Quality in Pre-School-Aged Children. Nutrients. 2023; 15(14):3154. https://doi.org/10.3390/nu15143154
Chicago/Turabian StyleMcCarthy, Madison, Mara Z. Vitolins, Joseph A. Skelton, Edward H. Ip, and Callie L. Brown. 2023. "A Pilot Study Examining the Association of Parental Stress and Household Food Insecurity with Dietary Quality in Pre-School-Aged Children" Nutrients 15, no. 14: 3154. https://doi.org/10.3390/nu15143154
APA StyleMcCarthy, M., Vitolins, M. Z., Skelton, J. A., Ip, E. H., & Brown, C. L. (2023). A Pilot Study Examining the Association of Parental Stress and Household Food Insecurity with Dietary Quality in Pre-School-Aged Children. Nutrients, 15(14), 3154. https://doi.org/10.3390/nu15143154