
Kiwifruit’s Allergy in Children: What Do We Know?
 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Methods
3. Epidemiology
4. Molecular Allergens
5. Pathophysiology
6. Clinical Manifestations
7. Cross-Reactions
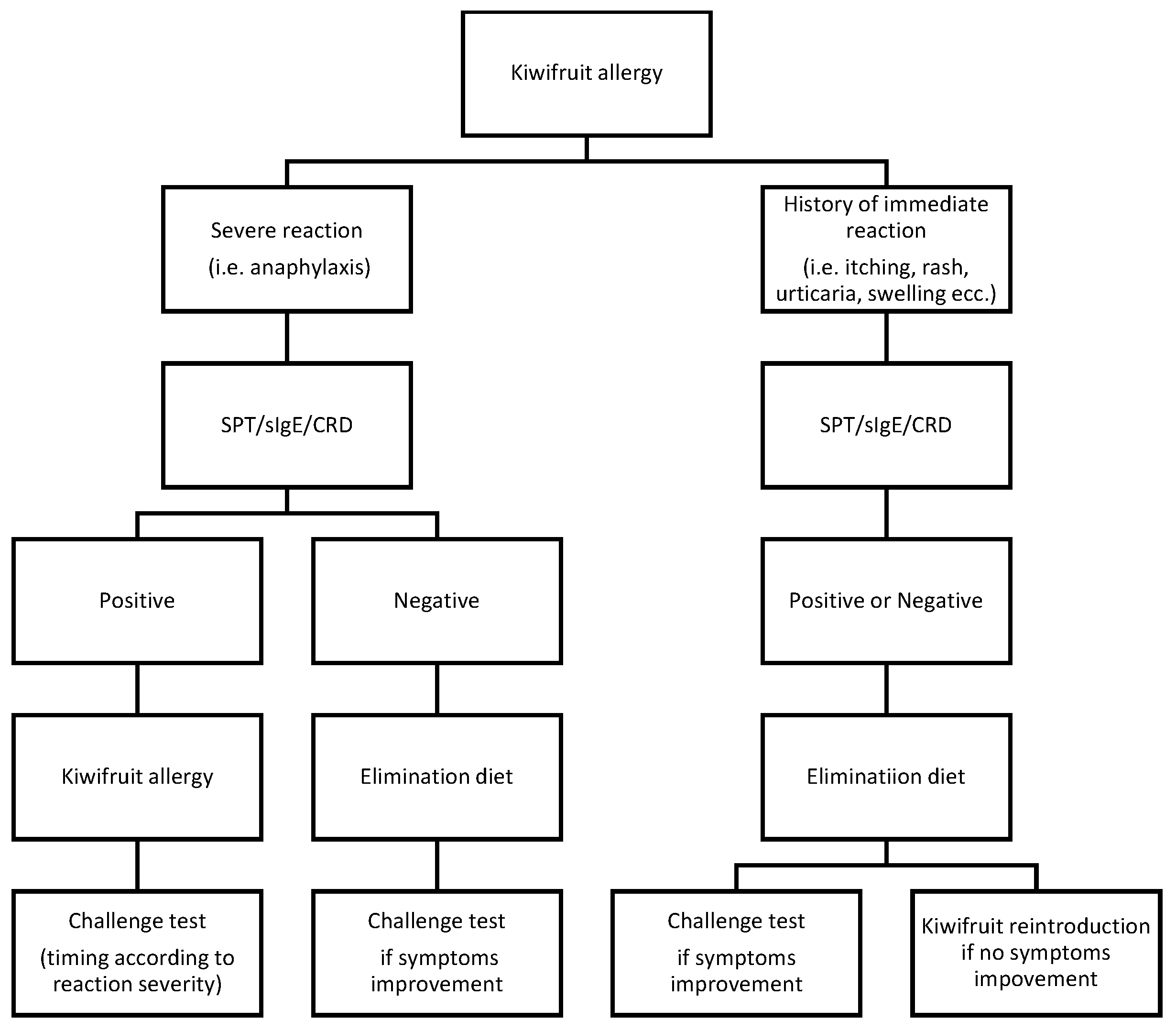
8. Diagnosis
9. Prevention and Therapy
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fine, A.J. Hypersensitivity reaction to kiwi fruit (Chinese gooseberry, Actinidia chinensis). J. Allergy Clin. Immunol. 1981, 68, 235–237. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture. Agricultural Research Service. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-details/168153/nutrients (accessed on 17 April 2023).
- Nishiyama, I. Fruits of the actinidia genus. Adv. Food Nutr. Res. 2007, 52, 293–324. [Google Scholar] [PubMed]
- Rancé, F.; Grandmottet, X.; Grandjean, H. Prevalence and main characteristics of schoolchildren diagnosed with food allergies in France. Clin. Exp. Allergy 2005, 35, 167–172. [Google Scholar] [CrossRef]
- Gall, H.; Kalveram, K.J.; Forck, G.; Sterry, W. Kiwi fruit allergy: A new birch pollen-associated food allergy. J. Allergy Clin. Immunol. 1994, 94, 70–76. [Google Scholar] [CrossRef]
- Pastorello, E.A.; Pravettoni, V.; Ispano, M.; Farioli, L.; Ansaloni, R.; Rotondo, F.; Incorvaia, C.; Åsman, I.; Bengtsson, A.; Ortolani, C. Identification of the allergenic components of kiwi fruit and evaluation of their cross-reactivity with timothy and birch pollens. J. Allergy Clin. Immunol. 1996, 98, 601–610. [Google Scholar] [CrossRef]
- Le, T.-M.; Bublin, M.; Breiteneder, H.; Fernández-Rivas, M.; Asero, R.; Ballmer-Weber, B.; Barreales, L.; Bures, P.; Belohlavkova, S.; de Blay, F.; et al. Kiwifruit allergy across Europe: Clinical manifestation and IgE recognition patterns to kiwifruit allergens. J. Allergy Clin. Immunol. 2013, 131, 164–171. [Google Scholar] [CrossRef]
- Lucas, J.S.; Grimshaw, K.E.; Collins, K.; Warner, J.O.; Hourihane, J.O. Kiwi fruit is a significant allergen and is associated with differing patterns of reactivity in children and adults. Clin. Exp. Allergy 2004, 34, 1115–1121. [Google Scholar] [CrossRef]
- Moreno Álvarez, A.; Sexto, L.V.; Bardina, L.; Grishina, G.; Sampson, H.A. Kiwifruit Allergy in Children: Characterization of Main Allergens and Patterns of Recognition. Children 2015, 2, 424–438. [Google Scholar] [CrossRef]
- Allergen Nomenclature WHO/IUIS Allergen Nomenclature Sub-Committee. Available online: www.allergen.org (accessed on 4 May 2023).
- Pastorello, E.A.; Conti, A.; Pravettoni, V.; Farioli, L.; Rivolta, F.; Ansaloni, R.; Ispano, M.; Incorvaia, C.; Giuffrida, M.G.; Ortolani, C. Identification of actinidin as the major allergen of kiwi fruit. J. Allergy Clin. Immunol. 1998, 101 Pt 1, 531–537. [Google Scholar] [CrossRef]
- Grozdanovic, M.M.; Čavić, M.; Nešić, A.; Andjelković, U.; Akbari, P.; Smit, J.J.; Gavrović-Jankulović, M. Kiwifruit cysteine protease actinidin compromises the intestinal barrier by disruptingtight junctions. Biochim. Biophys. Acta 2016, 1860, 516–526. [Google Scholar] [CrossRef]
- Saenz-De-Santamaria, M.; Postigo, I.; Gutierrez-Rodriguez, A.; Cardona, G.; Guisantes, J.A.; Asturias, J.; Martinez, J. The major allergen of Alternaria alternata (Alt a 1) is expressed in other members of the Pleosporaceae family. Mycoses 2006, 49, 91–95. [Google Scholar] [CrossRef]
- Barre, A.; Bienvenu, F.; Caze-Subra, S.; Degaud, M.; Viel, S.; Garnier, L.; Bienvenu, J.; Rouge, P. L’association Alt a 1 (Alternaria)–Act d 2 (kiwi): Origine et pertinence clinique possible. Rev. Française D’allergologie 2016, 56, 84–89. [Google Scholar] [CrossRef]
- Palacin, A.; Rodriguez, J.; Blanco, C.; Lopez-Torrejon, G.; Sánchez-Monge, R.; Varela, J.; Jiménez, M.A.; Cumplido, J.; Carrillo, T.; Crespo, J.F.; et al. Immunoglobulin E recognition patterns to purified kiwifruit (Actinidia deliciosa) allergens in patients sensitized to kiwi with different clinical symptoms. Clin. Exp. Allergy 2008, 38, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Bublin, M.; Pfister, M.; Radauer, C.; Oberhuber, C.; Bulley, S.; DeWitt, M.; Lidholm, J.; Reese, G.; Vieths, S.; Breiteneder, H.; et al. Component-resolved diagnosis of kiwifruit allergy with purified natural and recombinant kiwifruit allergens. J. Allergy Clin. Immunol. 2010, 125, 687–694.e1. [Google Scholar] [CrossRef] [PubMed]
- Tamburrini, M.; Cerasuolo, I.; Carratore, V.; Stanziola, A.A.; Zofra, S.; Romano, L.; Camardella, L.; Ciardiello, M.A. Kiwellin, a novel protein from kiwi fruit. Purification, biochemical characterization and identification as an allergen. Protein J. 2005, 24, 423–429. [Google Scholar] [CrossRef]
- Bublin, M.; Dennstedt, S.; Buchegger, M.; Ciardiello, M.A.; Bernardi, M.L.; Tuppo, L.; Harwanegg, C.; Hafner, C.; Ebner, C.; Ballmer-Weber, B.K.; et al. The performance of a component-based allergen microarray for the diagnosis of kiwifruit allergy. Clin. Exp. Allergy. 2011, 41, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Oberhuber, C.; Bulley, S.M.; Ballmer-Weber, B.K.; Bublin, M.; Gaier, S.; DeWitt, M.; Briza, P.; Hofstetter, G.; Lidholm, J.; Vieths, S.; et al. Characterization of Bet v 1-related allergens from kiwifruit relevant for patients with combined kiwifruit and birch pollen allergy. Mol. Nutr. Food Res. 2008, 52 (Suppl. S2), S230–S240. [Google Scholar] [CrossRef]
- D’Avino, R.; Bernardi, M.L.; Wallner, M.; Palazzo, P.; Camardella, L.; Tuppo, L.; Alessandri, C.; Breiteneder, H.; Ferreira, F.; Ciardiello, M.A.; et al. Kiwifruit Act d 11 is the first member of the ripening-related protein family identified as an allergen. Allergy 2011, 66, 870–877. [Google Scholar] [CrossRef]
- Sirvent, S.; Cantó, B.; Gómez, F.; Blanca, N.; Cuesta-Herranz, J.; Canto, G.; Blanca, M.; Rodríguez, R.; Villalba, M.; Palomares, O. Detailed characterization of Act d 12 and Act d 13 from kiwi seeds: Implication in IgE cross-reactivity with peanut and tree nuts. Allergy 2014, 69, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Asaumi, T.; Yanagida, N.; Sato, S.; Takahashi, K.; Ebisawa, M. Negative Act d 8 indicates systemic kiwifruit allergy among kiwifruit-sensitized children. Pediatr. Allergy Immunol. 2017, 28, 291–294. [Google Scholar] [CrossRef]
- Van Wijk, F.; Knippels, L. Initiating mechanisms of food allergy: Oral tolerance versus allergic sensitization. Biomed. Pharmacother. 2007, 61, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Morikawa, A. Anaphylaxis to kiwi fruit in a 12-year-old boy. J. Asthma. 1995, 32, 159–160. [Google Scholar] [CrossRef]
- Rance, F.; Dutau, G. Allergie alimentaire au kiwi chez l’enfant. Rev. Fr. D’allergol. D’immunol. Clin. 1992, 32, 203–206. [Google Scholar] [CrossRef]
- Visentini, D.; Zago, S.; Meroi, L. Diagnosi di allergia al kiwi in età pediatrica: Utilità della diagnostica molecolare. Riv. Ital. Med. Lab. 2018, 14, 227–233. [Google Scholar] [CrossRef]
- Moller, M. Characterization of allergens in kiwi fruit and detection of cross-reactivities with allergens of birch pollen and related fruit allergens. Food Agric. Immunol. 1997, 9, 107–121. [Google Scholar] [CrossRef]
- Voitenko, V.; Poulsen, L.K.; Nielsen, L.; Norgaard, A.; Bindslev-Jensen, C.; Skov, P.S. Allergenic properties of kiwi-fruit extract: Cross-reactivity between kiwi-fruit and birch-pollen allergens. Allergy 1997, 52, 136–143, Erratum in Allergy 1997, 52, 962. [Google Scholar] [CrossRef]
- Möller, M.; Kayma, M.; Vieluf, D.; Paschke, A.; Steinhart, H. Determination and characterization of cross-reacting allergens in latex, avocado, banana, and kiwi fruit. Allergy 1998, 53, 289–296. [Google Scholar] [CrossRef]
- Rudeschko, O.; Fahlbusch, B.; Steurich, F.; Schlenvoigt, G.; Jäger, L. Kiwi allergens and their cross-reactivity with birch, rye, timothy, and mugwort pollen. J. Investig. Allergol. Clin. Immunol. 1998, 8, 78–84. [Google Scholar]
- Gavrović-Jankulović, M.; Ćirković, T.; Vučković, O.; Atanasković-Marković, M.; Petersen, A.; Gojgić, G.; Burazer, L.; Jankov, R.M. Isolation and biochemical characterization of a thaumatin-like kiwi allergen. J. Allergy Clin. Immunol. 2002, 110, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.S.; Lewis, S.A.; Hourihane, J.O. Kiwi fruit allergy: A review. Pediatr. Allergy Immunol. 2003, 14, 420–428. [Google Scholar] [CrossRef]
- Alemán, A.; Sastre, J.; Quirce, S.; Heras, M.d.L.; Carnés, J.; Fernández-Caldas, E.; Pastor, C.; Blázquez, A.B.; Vivanco, F.; Cuesta-Herranz, J. Allergy to kiwi: A double-blind, placebo-controlled food challenge study in patients from a birch-free area. J. Allergy Clin. Immunol. 2004, 113, 543–550. [Google Scholar] [CrossRef]
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; Dutoit, G.; Eigenmann, P.; et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy 2014, 69, 1008–1025. [Google Scholar] [CrossRef]
- Jeon, Y.H.; Ahn, K.; Kim, J.; Shin, M.; Hong, S.-J.; Lee, S.-Y.; Pyun, B.Y.; Min, T.K.; Jung, M.; Lee, J.; et al. Clinical Characteristics of Atopic Dermatitis in Korean School-Aged Children and Adolescents According to Onset Age and Severity. J. Korean Med. Sci. 2022, 37, e30. [Google Scholar] [CrossRef]
- Lieberman, J.A.; Sicherer, S.H. Diagnosis of food allergy: Epicutaneous skin tests, in vitro tests, and oral food challenge. Curr. Allergy Asthma Rep. 2011, 11, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Siles, R.I.; Hsieh, F.H. Allergy blood testing: A practical guide for clinicians. Clevel. Clin. J. Med. 2011, 78, 585–592. [Google Scholar] [CrossRef]
- D’amelio, C.; Bernad, A.; García-Figueroa, B.; Garrido-Fernández, S.; Azofra, J.; Beristain, A.; Bueno-Díaz, C.; Garrido-Arandia, M.; Gastaminza, G.; Ferrer, M.; et al. Unraveling the Diagnosis of Kiwifruit Allergy: Usefulness of Current Diagnostic Tests. J. Investig. Allergol. Clin. Immunol. 2022, 32, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Ortolani, C.; Ispano, M.; Pastorello, E.; Bigi, A.; Ansaloni, R. The oral allergy syndrome. Ann. Allergy 1988, 61 Pt 2, 47–52. [Google Scholar]
- Feuille, E.; Nowak-Węgrzyn, A. Oral Immunotherapy for Food Allergies. Ann. Nutr. Metab. 2016, 68 (Suppl. S1), 19–31. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Vanga, S.K.; McCusker, C.; Raghavan, V. A Comprehensive Review on Kiwifruit Allergy: Pathogenesis, Diagnosis, Management, and Potential Modification of Allergens Through Processing. Compr. Rev. Food Sci. Food Saf. 2019, 18, 500–513. [Google Scholar] [CrossRef]
- Lieberman, J.A.; Chehade, M. Use of omalizumab in the treatment of food allergy and anaphylaxis. Curr. Allergy Asthma Rep. 2013, 13, 78–84. [Google Scholar] [CrossRef]
- Mousan, G.; Kamat, D. Cow’s Milk Protein Allergy. Clin. Pediatr. 2016, 55, 1054–1063. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Species | Shape | Density of Hairs | Fruit Flesh |
|---|---|---|---|
| A. deliciosa | Large, ovoid | Dense | Green |
| A. chinensis | Large, elliptical | Sparse or absent | Yellow, green, or red |
| A. arguta | Small, round | Absent | Green |
| A. eriantha | Long, cylindrical | Abundant, long, villose, white | Dark green |
| Allergen | Biochemical Name | Molecular Weight | Clinical Significance |
|---|---|---|---|
| Act d 1 | Cysteine protease (actinidin) | 30 kDa | Major allergen related to systemic reactions |
| Act d 2 | Thaumatin-like protein | 24 kDa | Major allergen |
| Act d 3 | 40 kDa | Minor allergen | |
| Act d 4 | Phytocystatin | 11 kDa | Minor allergen |
| Act d 5 | Kiwellin | 28 kDa | Minor allergen |
| Act d 6 | Pectin methylesterase inhibitor | 18 kDa | Minor allergen |
| Act d 7 | Pectin methylesterase | 50 kDa | Minor allergen |
| Act d 8 | Pathogenesis-related protein, PR-10, Bet v 1 family member | 17 kDa | Major allergen, negative predictive risk factor for systemic reactions |
| Act d 9 | Profilin | 14 kDa | Minor allergen |
| Act d 10 | nsLTP1 | 10 kDa | Minor allergen associated with mild symptoms, mainly in southern Europe |
| Act d 11 | Major latex protein/ripening-related protein (MLP/RRP), Bet v 1 family member | 17 kDa | Major allergen |
| Act d 12 | Cupin, 11S globulin, kiwifruit seed storage protein | 50,207.304 Da (mass spectrometry), six peptide sequences (C0HJF9, to be released upon publication) | Major allergen |
| Act d 13 | 2S albumin, kiwifruit seed storage protein | 11,359.6 Da (mass spectrometry), four peptide sequences (C0HJG, to be released upon publication) | Minor allergen |
| Author, Year [Reference] | Country | Study Design | Population and Sample Size | Comment |
|---|---|---|---|---|
| Fine et al., 1981 [1] | United States of America | Case report | A 53 y woman | First-reported allergic reaction to kiwifruit. |
| Rance et al., 1992 [25] | France | Case report | A 3 y boy and 8 y girl | New emerging allergies (kiwi) in children with systemic manifestations. |
| Shimizu et al., 1995 [24] | Japan | Case report | A 12 y boy | A case of anaphylaxis after handling and ingestion of kiwifruit. |
| Pastorello et al., 1996 [6] | Italy | Observational study | 30 pts (16–69 y) with OAS to kiwi | Identification and characterization of 11 kiwi allergens. |
| Möller et al., 1997 [27] | Germany | Observational study | 29 pts (23–57 y) | Cross-reactivity between allergens found both in kiwifruit and birch pollen. |
| Voitenko et al., 1997 [28] | Denmark | Observational study | 9 pts (20–54 y) | Production of a kiwi extract and characterization of cross-reactivity with birch pollen in vitro. |
| Möller et al., 1998 [29] | Germany | Observational study | 12 pts (20–58 y) | Cross-reactivity among allergens in latex, avocado, banana, and kiwi. |
| Fahlbusch et al., 1998 [30] | Germany | Observational study | 9 pts | Characterization of IgE-binding kiwifruit’s allergen epitopes. |
| Gavrovic-Jankulović et al., 2002 [31] | Yugoslavia | Observational study | 7 pts | Isolation and biochemical characterization of Act d 2. |
| Lucas et al., 2004 [8] | United Kingdom | Observational study | 273 pts (4 months–71 y) | Clinical differences in children and adults. |
| Palacin et al., 2008 [15] | Spain | 92 pts (6–55 y) | High IgE level against Act d 1 and Act d 3 is associated with severe symptomatology. | |
| Moreno Álvarez et al., 2015 [9] | Spain | Observational study | 24 pts (3–12 y) | Characterization of main allergens and patterns of recognition in children. |
| Visentini et al., 2018 [26] | Italy | Retrospective study | 25 pts (1–14 y) | Primary sensitization to kiwifruit is the most frequent in childhood. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bringheli, I.; Brindisi, G.; Morelli, R.; Marchetti, L.; Cela, L.; Gravina, A.; Pastore, F.; Semeraro, A.; Cinicola, B.; Capponi, M.; et al. Kiwifruit’s Allergy in Children: What Do We Know? Nutrients 2023, 15, 3030. https://doi.org/10.3390/nu15133030
Bringheli I, Brindisi G, Morelli R, Marchetti L, Cela L, Gravina A, Pastore F, Semeraro A, Cinicola B, Capponi M, et al. Kiwifruit’s Allergy in Children: What Do We Know? Nutrients. 2023; 15(13):3030. https://doi.org/10.3390/nu15133030
Chicago/Turabian StyleBringheli, Ivana, Giulia Brindisi, Rebecca Morelli, Lavinia Marchetti, Ludovica Cela, Alessandro Gravina, Francesca Pastore, Antonio Semeraro, Bianca Cinicola, Martina Capponi, and et al. 2023. "Kiwifruit’s Allergy in Children: What Do We Know?" Nutrients 15, no. 13: 3030. https://doi.org/10.3390/nu15133030
APA StyleBringheli, I., Brindisi, G., Morelli, R., Marchetti, L., Cela, L., Gravina, A., Pastore, F., Semeraro, A., Cinicola, B., Capponi, M., Gori, A., Pignataro, E., Piccioni, M. G., Zicari, A. M., & Anania, C. (2023). Kiwifruit’s Allergy in Children: What Do We Know? Nutrients, 15(13), 3030. https://doi.org/10.3390/nu15133030