Methylsulfonylmethane Improves Knee Quality of Life in Participants with Mild Knee Pain: A Randomized, Double-Blind, Placebo-Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Aim
2.2. Participants
2.3. Study Design
2.4. Outcomes
2.5. Sample Size and Statistical Analysis
3. Results
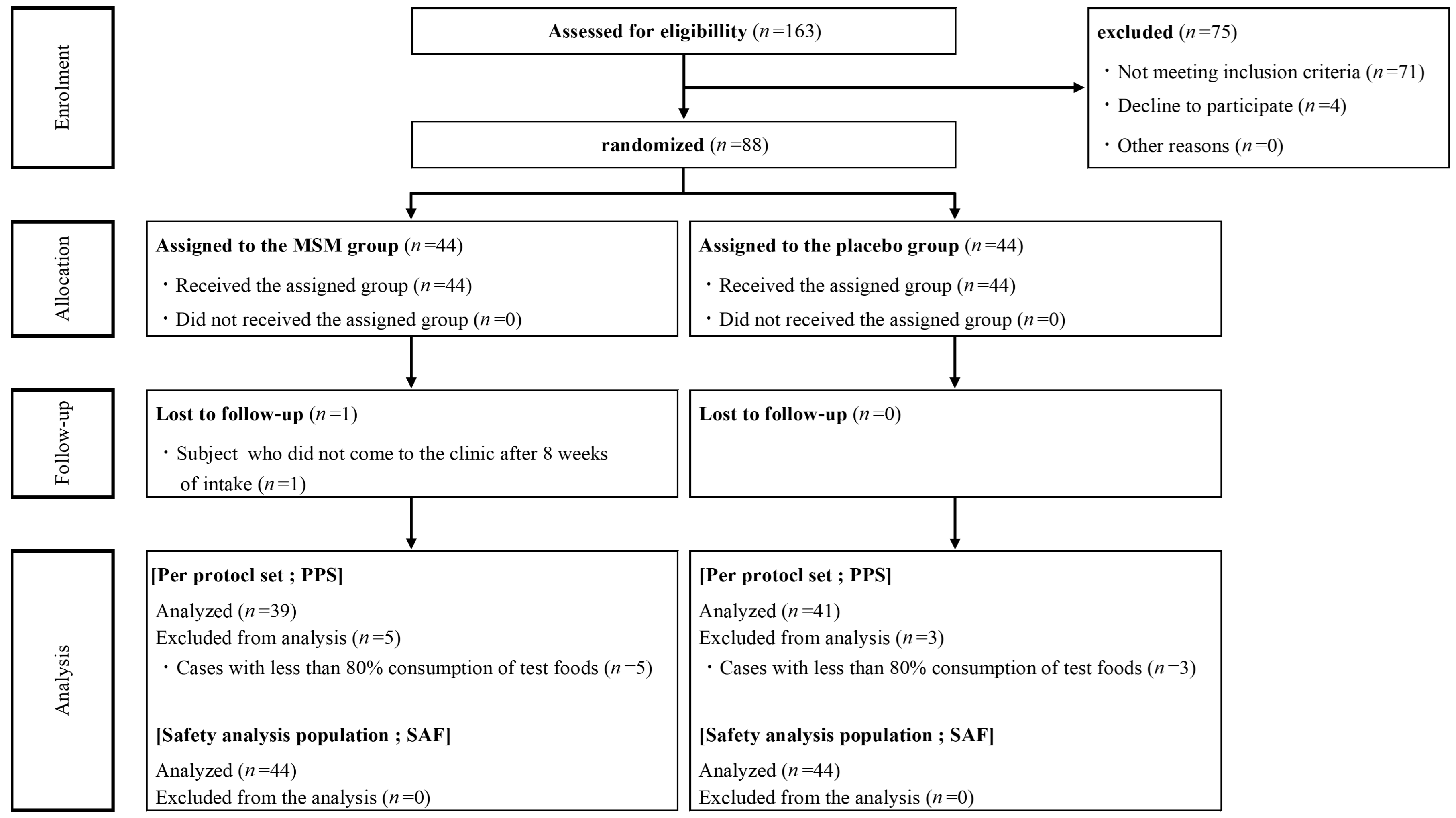
3.1. Participant Flow
3.2. JKOM Scores, JOA Scores, and Inflammation Markers
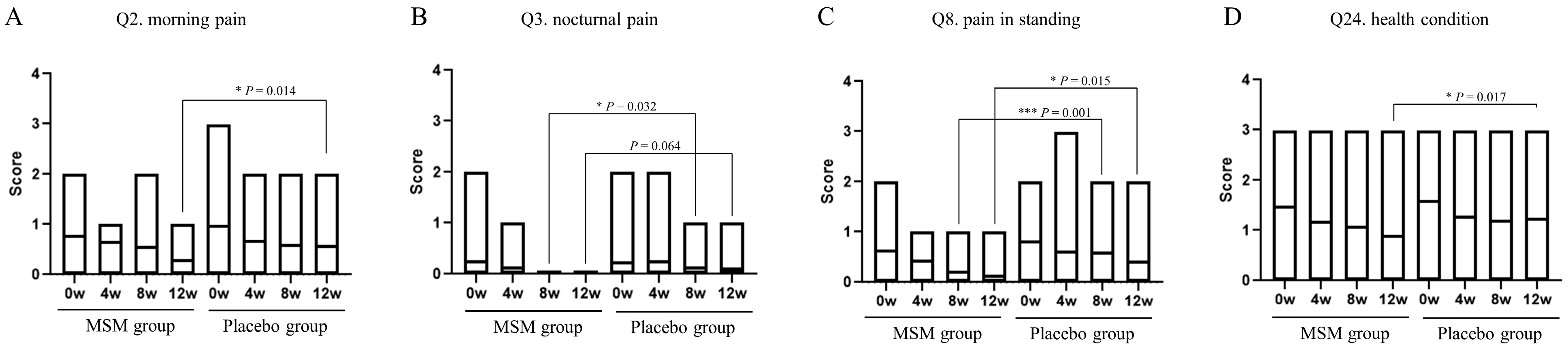
3.3. Questionaries
3.4. Safety Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Magnuson, B.A.; Appleton, J.; Ames, G.B. Pharmacokinetics and distribution of [35S]methylsulfonylmethane following oral administration to rats. J. Agric. Food Chem. 2007, 55, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Otsuki, S.; Qian, W.; Ishihara, A.; Kabe, T. Elucidation of dimethylsulfone metabolism in rat using a 35S radioisotope tracer method. Nutr. Res. 2002, 22, 313–322. [Google Scholar] [CrossRef]
- Colletti, A.; Cicero, A.F.G. Nutraceutical approach to chronic osteoarthritis: From molecular research to clinical evidence. Int. J. Mol. Sci. 2021, 22, 12920. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.T.; Sharma, A.R.; Chakraborty, C.; Saibaba, B.; Ahn, M.E.; Lee, S.S. Review of prospects of biological fluid biomarkers in osteoarthritis. Int. J. Mol. Sci. 2017, 18, 601. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Joung, Y.H.; Lim, E.J.; Darvin, P.; Chung, S.C.; Jang, J.W.; Park, K.D.; Lee, H.K.; Kim, H.S.; Park, T.; Yang, Y.M. MSM enhances GH signaling via the Jak2/STAT5b pathway in osteoblast-like cells and osteoblast differentiation through the activation of STAT5b in MSCs. PLoS ONE 2012, 7, e47477. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Bertacco, J.; Marchetto, G.; Cheri, S.; Deiana, M.; Minoia, A.; Tiso, N.; Mottes, M.; Valenti, M.T. Methylsulfonylmethane enhances MSC chondrogenic commitment and promotes pre-osteoblast formation. Stem Cell. Res. Ther. 2021, 12, 326. [Google Scholar] [CrossRef]
- Kim, D.N.; Joung, Y.H.; Darvin, P.; Kang, D.Y.; Sp, N.; Byun, H.J.; Cho, K.H.; Park, K.D.; Lee, H.K.; Yang, Y.M. Methylsulfonylmethane enhances BMP 2 induced osteoblast differentiation in mesenchymal stem cells. Mol. Med. Rep. 2016, 14, 460–466. [Google Scholar] [CrossRef]
- Aljohani, H.; Senbanjo, L.T.; Chellaiah, M.A. Methylsulfonylmethane increases osteogenesis and regulates mineralization of the matrix by transglutaminase 2 in SHED cells. PLoS ONE 2019, 14, e0225598. [Google Scholar] [CrossRef]
- Joung, Y.H.; Darvin, P.; Kang, D.Y.; Sp, N.; Byun, H.J.; Lee, C.H.; Lee, H.K.; Yang, Y.M. Methylsulfonylmethane inhibits RANKL-induced osteoclastogenesis in BMMs by suppressing NF-κB and STAT3 activity. PLoS ONE 2016, 11, e0159891. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, D.H.; Lim, H.; Baek, D.Y.; Shin, H.K.; Kim, J.K. Anti-inflammatory effects of methylsulfonylmethane on lipopolysaccharide-induced inflammatory responses in murine macrophages. Biol. Pharm. Bull. 2009, 32, 651–656. [Google Scholar] [CrossRef]
- Oeckinghaus, A.; Ghosh, S. NF-κB family of transcription factors and their regulation. Cold Spring Harb. Perspect. Biol. 2009, 1, a000034. [Google Scholar] [CrossRef]
- Ahn, H.; Kim, J.; Lee, M.J.; Kim, Y.J.; Cho, Y.W.; Lee, G.S. Methylsulfonylmethane inhibits NLRP3 inflammasome activation. Cytokine 2015, 71, 223–231. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ueno, S.; Kumamoto, S.; Yoshikai, Y. Suppressive effect of methylsulfonylmethane (MSM) on type II collagen-induced arthritis in DBA/1j mice. Jpn. Pharmacol. Ther. 2004, 32, 421–427. [Google Scholar]
- Ezaki, J.; Hashimoto, M.; Hosokawa, Y.; Ishimi, Y. Assessment of safety and efficacy of methylsulfonylmethane on bone and knee joints in osteoarthritis animal model. J. Bone Miner. Metab. 2013, 31, 16–25. [Google Scholar] [CrossRef]
- Debbi, E.M.; Agar, G.; Fichman, G.; Bar Ziv, Y.; Kardosh, R.; Halperin, N.; Elbaz, A.; Beer, Y.; Debi, R. Efficacy of methylsulfonylmethane supplementation on osteoarthritis of the knee: A randomized controlled study. BMC Complement. Altern. Med. 2011, 11, 50. [Google Scholar] [CrossRef]
- Usha, P.R.; Naidu, M.U. Randomized, double-blind, parallel, placebo-controlled study of oral glucosamine, methylsulfonylmethane, and their combination in osteoarthritis. Clin. Drug Investig. 2004, 24, 353–363. [Google Scholar] [CrossRef]
- Kim, L.S.; Axelrod, L.J.; Howard, P.; Buratovich, N.; Waters, R.F. Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain of the knee: A pilot clinical trial. Osteoarthr. Cartil. 2006, 14, 286–294. [Google Scholar] [CrossRef]
- Pagonis, T.A.; Givissis, P.A.; Kritis, A.C.; Christodoulou, A.C. Effect of methylsulfonylmethane on osteoarthritic large joints and mobility. Int. J. Orthop. 2014, 1, 19–24. [Google Scholar]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- Akai, M.; Doi, T.; Fujino, K.; Iwaya, T.; Kurosawa, H.; Nasu, T. An outcome measure for Japanese people with knee osteoarthritis. J. Rheumatol. 2005, 32, 1524–1532. [Google Scholar] [PubMed]
- Braham, R.; Dawson, B.; Goodman, C. The effect of glucosamine supplementation on people experiencing regular knee pain. Br. J. Sports Med. 2003, 37, 45–49, discussion 49. [Google Scholar] [CrossRef] [PubMed]
- Suchy, F.J.; Brannon, P.M.; Carpenter, T.O.; Fernandez, J.R.; Gilsanz, V.; Gould, J.B.; Hall, K.; Hui, S.L.; Lupton, J.; Mennella, J.; et al. NIH consensus development conference statement: Lactose intolerance and health. NIH Consens. State Sci. Statements 2010, 27, 1–27. [Google Scholar]
- Butawan, M.; Benjamin, R.L.; Bloomer, R.J. Methylsulfonylmethane: Applications and safety of a novel dietary supplement. Nutrients 2017, 9, 290. [Google Scholar] [CrossRef]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Okuda, M.; Omokawa, S.; Okahashi, K.; Akahane, M.; Tanaka, Y. Validity and reliability of the Japanese Orthopaedic Association score for osteoarthritic knees. J. Orthop. Sci. 2012, 17, 750–756. [Google Scholar] [CrossRef]
- Suzuki, N.; Baba, A.; Kakinuma, T.; Sano, Y.; Tanaka, M.; Ouchi, S.; Watanabe, T.; Yamamoto, K. A novel dietary questionnaire: The Calorie and Nutrition Diary (CAND). New Food Indust. 2019, 61, 721–732. [Google Scholar]
- Oberg, A.L.; Mahoney, D.W. Linear mixed effects models. Methods Mol. Biol. 2007, 404, 213–234. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162, Erratum in Arthritis Care Res. 2021, 73, 764. [Google Scholar] [CrossRef]
- Liu, Q.; Niu, J.; Li, H.; Ke, Y.; Li, R.; Zhang, Y.; Lin, J. Knee symptomatic osteoarthritis, walking disability, NSAIDs use, and all-cause mortality: Population-based Wuchuan osteoarthritis study. Sci. Rep. 2017, 7, 3309. [Google Scholar] [CrossRef]
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008, 58, 26–35. [Google Scholar] [CrossRef]
- Guccione, A.A.; Felson, D.T.; Anderson, J.J.; Anthony, J.M.; Zhang, Y.; Wilson, P.W.; Kelly-Hayes, M.; Wolf, P.A.; Kreger, B.E.; Kannel, W.B. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am. J. Public Health 1994, 84, 351–358. [Google Scholar] [CrossRef]
- Fayet, M.; Hagen, M. Pain characteristics and biomarkers in treatment approaches for osteoarthritis pain. Pain Manag. 2021, 11, 59–73. [Google Scholar] [CrossRef]
- Birmingham, J.D.; Vilim, V.; Kraus, V.B. Collagen biomarkers for arthritis applications. Biomark. Insights 2007, 1, 61–76. [Google Scholar] [CrossRef]
- Papaneophytou, C.; Alabajos-Cea, A.; Viosca-Herrero, E.; Calvis, C.; Costa, M.; Christodoulides, A.E.; Kroushovski, A.; Lapithis, A.; Lapithi, V.M.; Papayiannis, I.; et al. Associations between serum biomarkers of cartilage metabolism and serum hyaluronic acid, with risk factors, pain categories, and disease severity in knee osteoarthritis: A pilot study. BMC Musculoskelet. Disord. 2022, 23, 195. [Google Scholar] [CrossRef]
- He, G.; Chen, X.; Zhang, G.; Lin, H.; Li, R.; Wu, X. Detection of urine C2C and trace element level in patients with knee osteoarthritis. Cell Biochem. Biophys. 2014, 70, 475–479. [Google Scholar] [CrossRef]
- Nigoro, K.; Ito, H.; Kawata, T.; Ishie, S.; Morita, Y.; Nishitani, K.; Aoyama, T.; Tabara, Y.; Matsuda, F.; Narumiya, S.; et al. Differential Contribution of the Medial and the Lateral Side of the Joint to Symptoms in Knee Osteoarthritis: A Radiographic and Laboratory Analysis in the Nagahama Study. Cartilage 2021, 13 (Suppl. S1), 1648S–1657S. [Google Scholar] [CrossRef]
- Iijima, H.; Aoyama, T.; Nishitani, K.; Ito, H.; Fukutani, N.; Isho, T.; Kaneda, E.; Kuroki, H.; Matsuda, S. Coexisting lateral tibiofemoral osteoarthritis is associated with worse knee pain in patients with mild medial osteoarthritis. Osteoarthr. Cartil. 2017, 25, 1274–1281. [Google Scholar] [CrossRef]
- Stannus, O.P.; Jones, G.; Blizzard, L.; Cicuttini, F.M.; Ding, C. Associations between serum levels of inflammatory markers and change in knee pain over 5 years in older adults: A prospective cohort study. Ann. Rheum. Dis. 2013, 72, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J. Meta-analysis of serum C-reactive protein and cartilage oligomeric matrix protein levels as biomarkers for clinical knee osteoarthritis. BMC Musculoskelet. Disord. 2018, 19, 22. [Google Scholar] [CrossRef] [PubMed]
- Otterness, I.G.; Weiner, E.; Swindell, A.C.; Zimmerer, R.O.; Ionescu, M.; Poole, A.R. An analysis of 14 molecular markers for monitoring osteoarthritis. Relationship of the markers to clinical end-points. Osteoarthr. Cartil. 2001, 9, 224–231. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pearle, A.D.; Scanzello, C.R.; George, S.; Mandl, L.A.; DiCarlo, E.F.; Peterson, M.; Sculco, T.P.; Crow, M.K. Elevated high-sensitivity C-reactive protein levels are associated with local inflammatory findings in patients with osteoarthritis. Osteoarthr. Cartil. 2007, 15, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Kim, D.H.; Lee, E.K.; Chung, K.W.; Chung, S.; Lee, B.; Seo, A.Y.; Chung, J.H.; Jung, Y.S.; Im, E.; et al. Redefining Chronic Inflammation in Aging and Age-Related Diseases: Proposal of the Senoinflammation Concept. Aging Dis. 2019, 10, 367–382. [Google Scholar] [CrossRef]
- Beavers, K.M.; Beavers, D.P.; Newman, J.J.; Anderson, A.M.; Loeser, R.F., Jr.; Nicklas, B.J.; Lyles, M.F.; Miller, G.D.; Mihalko, S.L.; Messier, S.P. Effects of total and regional fat loss on plasma CRP and IL-6 in overweight and obese, older adults with knee osteoarthritis. Osteoarthr. Cartil. 2015, 23, 249–256. [Google Scholar] [CrossRef]
- Minguzzi, M.; Cetrullo, S.; D’Adamo, S.; Silvestri, Y.; Flamigni, F.; Borzì, R.M. Emerging Players at the Intersection of Chondrocyte Loss of Maturational Arrest, Oxidative Stress, Senescence and Low-Grade Inflammation in Osteoarthritis. Oxid. Med. Cell Longev. 2018, 2018, 3075293. [Google Scholar] [CrossRef]
- Olivotto, E.; Otero, M.; Marcu, K.B.; Goldring, M.B. Pathophysiology of osteoarthritis: Canonical NF-κB/IKKβ-dependent and kinase-independent effects of IKKα in cartilage degradation and chondrocyte differentiation. RMD Open 2015, 1 (Suppl. S1), e000061. [Google Scholar] [CrossRef]
- Lepetsos, P.; Papavassiliou, A.G. ROS/oxidative stress signaling in osteoarthritis. Biochim. Biophys. Acta. 2016, 1862, 576–591. [Google Scholar] [CrossRef]
- Tudorachi, N.B.; Totu, E.E.; Fifere, A.; Ardeleanu, V.; Mocanu, V.; Mircea, C.; Isildak, I.; Smilkov, K.; Cărăuşu, E.M. The Implication of Reactive Oxygen Species and Antioxidants in Knee Osteoarthritis. Antioxidants 2021, 10, 985. [Google Scholar] [CrossRef]
- Miller, L.; Thompson, K.; Pavlenco, C.; Mettu, V.S.; Haverkamp, H.; Skaufel, S.; Basit, A.; Prasad, B.; Larsen, J. The Effect of Daily Methylsulfonylmethane (MSM) Consumption on High-Density Lipoprotein Cholesterol in Healthy Overweight and Obese Adults: A Randomized Controlled Trial. Nutrients 2021, 13, 3620. [Google Scholar] [CrossRef]
- Kim, H.O.; Kim, H.S.; Youn, J.C.; Shin, E.C.; Park, S. Serum cytokine profiles in healthy young and elderly population assessed using multiplexed bead-based immunoassays. J. Transl. Med. 2011, 9, 113. [Google Scholar] [CrossRef]
- Perruccio, A.V.; Badley, E.M.; Power, J.D.; Canizares, M.; Kapoor, M.; Rockel, J.; Chandran, V.; Gandhi, R.; Mahomed, N.M.; Davey, J.R.; et al. Sex differences in the relationship between individual systemic markers of inflammation and pain in knee osteoarthritis. Osteoarthr. Cartil. Open 2019, 1, 100004. [Google Scholar] [CrossRef]
- Tschon, M.; Contartese, D.; Pagani, S.; Borsari, V.; Fini, M. Gender and Sex Are Key Determinants in Osteoarthritis Not Only Confounding Variables. A Systematic Review of Clinical Data. J. Clin. Med. 2021, 10, 3178. [Google Scholar] [CrossRef]
- Phyomaung, P.P.; Dubowitz, J.; Cicuttini, F.M.; Fernando, S.; Wluka, A.E.; Raaijmaakers, P.; Wang, Y.; Urquhart, D.M. Are depression, anxiety and poor mental health risk factors for knee pain? A systematic review. BMC Musculoskelet. Disord. 2014, 15, 10. [Google Scholar] [CrossRef]
- De Rooij, M.; van der Leeden, M.; Heymans, M.W.; Holla, J.F.; Häkkinen, A.; Lems, W.F.; Roorda, L.D.; Veenhof, C.; Sanchez-Ramirez, D.C.; de Vet, H.C.; et al. Prognosis of Pain and Physical Functioning in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2016, 68, 481–492. [Google Scholar] [CrossRef]
- Iijima, H.; Aoyama, T.; Fukutani, N.; Isho, T.; Yamamoto, Y.; Hiraoka, M.; Miyanobu, K.; Jinnouchi, M.; Kaneda, E.; Kuroki, H.; et al. Psychological health is associated with knee pain and physical function in patients with knee osteoarthritis: An exploratory cross-sectional study. BMC Psychol. 2018, 6, 19. [Google Scholar] [CrossRef]
- Mabey, T.; Honsawek, S.; Tanavalee, A.; Yuktanandana, P.; Wilairatana, V.; Poovorawan, Y. Plasma and synovial fluid inflammatory cytokine profiles in primary knee osteoarthritis. Biomarkers 2016, 21, 639–644. [Google Scholar] [CrossRef]
- Giordano, R.; Petersen, K.K.; Andersen, H.H.; Simonsen, O.; Arendt-Nielsen, L. Serum inflammatory markers in patients with knee osteoarthritis: A proteomic approach. Clin. J. Pain. 2020, 36, 229–237. [Google Scholar] [CrossRef]
- Siebuhr, A.S.; Petersen, K.K.; Arendt-Nielsen, L.; Egsgaard, L.L.; Eskehave, T.; Christiansen, C.; Simonsen, O.; Hoeck, H.; Karsdal, M.; Bay-Jensen, A. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthr. Cartil. 2014, 22, 44–50. [Google Scholar] [CrossRef]
- Kokebie, R.; Aggarwal, R.; Lidder, S.; Hakimiyan, A.A.; Rueger, D.C.; Block, J.A.; Chubinskaya, S. The role of synovial fluid markers of catabolism and anabolism in osteoarthritis, rheumatoid arthritis and asymptomatic organ donors. Arthritis Res. Ther. 2011, 13, R50. [Google Scholar] [CrossRef] [PubMed]
- Orita, S.; Koshi, T.; Mitsuka, T.; Miyagi, M.; Inoue, G.; Arai, G.; Ishikawa, T.; Hanaoka, E.; Yamashita, K.; Yamashita, M.; et al. Associations between proinflammatory cytokines in the synovial fluid and radiographic grading and pain-related scores in 47 consecutive patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2011, 12, 144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | PSS | SAF | |||||
|---|---|---|---|---|---|---|---|
| (Unit) | MSM Group | Placebo Group | p Value 1 | MSM Group | Placebo Group | p Value 1 | |
| (n = 39) | (n = 41) | (n = 44) | (n = 44) | ||||
| Sex | female/male | 28/11 | 30/11 | 1.000 | 31/13 | 32/12 | 1.000 |
| K-L grade | grade 1/grade 0 | 14/25 | 17/24 | 0.652 | 18/26 | 17/27 | 1.000 |
| Age | Mean ± SD | 48.9 ± 13.7 | 48.9 ± 13.8 | 0.988 | 49.3 ± 13.7 | 49.2 ± 13.7 | 0.975 |
| (years) | Med | 52.0 | 48.0 | 52.0 | 47.5 | ||
| Min–Max | 26–85 | 23–80 | 26–85 | 23–80 | |||
| Mean ± SD | 161.5 ± 7.5 | 163.1 ± 7.7 | 0.335 | 161.9 ± 7.8 | 163.2 ± 7.5 | 0.424 | |
| Height | Med | 161.00 | 161.00 | 161.00 | 161.00 | ||
| (cm) | Min–Max | 144.0–174.0 | 148.5–180.0 | 144.0–188.0 | 148.5–180.0 | ||
| Weight | Mean ± SD | 62.0 ± 15.8 | 60.7 ± 13.8 | 0.686 | 61.8 ± 15.7 | 60.3 ± 13.6 | 0.631 |
| (kg) | Med | 59.50 | 61.10 | 59.30 | 59.75 | ||
| Min–Max | 44.3–117.5 | 36.1–93.7 | 43.2–117.5 | 36.1–93.7 | |||
| BMI | Mean ± SD | 23.6 ± 5.2 | 22.6 ± 4.3 | 0.354 | 23.4 ± 5.0 | 22.5 ± 4.2 | 0.353 |
| (kg/cm2) | Med | 22.40 | 21.40 | 22.60 | 21.40 | ||
| Min–Max | 18.4–42.6 | 16.4–36.6 | 17.5–42.6 | 16.4–36.6 | |||
| PBF | Mean ± SD | 29.1 ± 10.0 | 27.9 ± 9.6 | 0.605 | 28.3 ± 9.7 | 27.6 ± 9.7 | 0.732 |
| (%) | Med | 26.90 | 26.30 | 26.80 | 25.85 | ||
| Min–Max | 13.4–58.8 | 12.7–55.5 | 13.4–58.8 | 12.7–55.5 | |||
| Systolic BP | Mean ±S D | 119.9 ± 11.2 | 118.8 ± 16.4 | 0.716 | 121.3 ± 12.5 | 119.0 ± 16.7 | 0.480 |
| (mmHg) | Med | 117.0 | 112.0 | 117.5 | 112.5 | ||
| Min–Max | 103–149 | 90–159 | 103–157 | 90–159 | |||
| Diastolic BP | Mean ± SD | 77.8 ± 7.8 | 76.7 ± 11.5 | 0.628 | 78.1 ± 8.9 | 76.8 ± 11.5 | 0.541 |
| (mmHg) | Med | 76.0 | 73.0 | 76.0 | 73.5 | ||
| Min–Max | 66–93 | 60–106 | 64–107 | 60–106 | |||
| Pulse | Mean ± SD | 72.6 ± 11.3 | 76.5 ± 12.9 | 0.155 | 72.5 ± 10.8 | 75.8 ± 12.8 | 0.195 |
| (bpm) | Med | 74.0 | 77.0 | 74.0 | 74.5 | ||
| Min–Max | 45–103 | 55–112 | 45–103 | 55–112 | |||
| 0 Week | 4 Week | 8 Week | 12 Week | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | ||
| Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | ||||||
| JKOM | Ⅰ:VAS | 37.9 ± 21.9 | 41.3 ± 20.7 | −3.4 (−12.9 to 6.1) | 0.478 | 34.1 ± 22.2 | 32.9 ± 21.0 | 1.2 (−8.4 to 10.8) | 0.801 | 25.3 ± 18.6 | 29.0 ± 22.3 | −3.7 (−12.9 to 5.4) | 0.416 | 24.4 ± 21.7 | 25.2 ± 22.1 | −0.7 (−10.5 to 9.0) | 0.881 |
| Ⅱ: Pain and stiffiness in knees | 6.8 ± 2.5 | 7.1 ± 3.3 | −0.4 (−1.7 to 0.9) | 0.566 | 5.2 ± 2.8 | 5.7 ± 3.9 | −0.5 (−2.0 to 1.0) | 0.548 | 4.1 ± 2.7 | 4.8 ± 3.4 | −0.7 (−2.1 to 0.7) | 0.306 | 2.7 ± 2.2 | 3.9 ± 3.4 | −1.2 (−2.4 to 0.1) | 0.073 | |
| Ⅲ: Condition in daily life | 4.4 ± 3.4 | 4.7 ± 3.4 | −0.3 (−1.8 to 1.2) | 0.674 | 2.9 ± 4.4 | 3.4 ± 4.6 | −0.5 (−2.5 to 1.5) | 0.645 | 2.5 ± 2.3 | 2.8 ± 4.1 | −0.3 (−1.8 to 1.1) | 0.643 | 1.5 ± 1.8 | 2.1 ± 3.1 | −0.6 (−1.7 to 0.5) | 0.300 | |
| Ⅳ: General activities | 4.6 ± 2.1 | 5.4 ± 2.4 | -0.8 (−1.8 to 0.2) | 0.118 | 3.7 ± 1.6 | 4.0 ± 1.6 | −0.3 (−1.0 to 0.5) | 0.478 | 3.2 ± 1.5 | 3.6 ± 1.7 | −0.4 (−1.1 to 0.3) | 0.263 | 2.7 ± 1.5 | 3.1 ± 1.5 | −0.5 (−1.1 to 0.2) | 0.153 | |
| Ⅴ: Health conditions | 2.5 ± 0.9 | 2.6 ± 0.9 | −0.1 (−0.5 to 0.2) | 0.461 | 1.8 ± 1.0 | 2.0 ± 1.2 | -0.2 (−0.7 to 0.3) | 0.415 | 1.6 ± 1.0 | 1.7 ± 1.1 | −0.2 (−0.6 to 0.3) | 0.476 | 1.2 ± 1.0 | 1.8 ± 1.2 | −0.6 (−1.0 to−0.1) | 0.027 * | |
| Total JKOM score | 18.2 ± 6.7 | 19.9 ± 7.5 | −1.6 (−4.8 to 1.5) | 0.305 | 13.6 ± 7.7 | 15.0 ± 10.1 | −1.4 (−5.4 to 2.6) | 0.492 | 11.3 ± 5.4 | 13.0 ± 8.4 | −1.6 (−4.8 to 1.5) | 0.307 | 8.1 ± 4.2 | 10.9 ± 7.6 | −2.8 (−5.5 to−0.1) | 0.046 * | |
| JOA | Total score | 95.9 ± 5.9 | 95.9 ± 5.0 | 0.0 (−2.4 to 2.5) | 0.972 | 95.4 ± 5.2 | 96.5 ± 5.1 | −1.1 (−3.4 to 1.2) | 0.352 | 96.5 ± 4.1 | 96.5 ± 4.4 | −0.1 (−1.9 to 1.8) | 0.958 | 96.4 ± 5.3 | 96.6 ± 5.3 | −0.2 (−2.6 to 2.1) | 0.843 |
| 0 Week | 4 Week | 8 Week | 12 Week | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | ||
| (Unit) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | |||||
| IL-1β | (pg/mL) | 0.0 ± 0.1 | 0.0 ± 0.0 | 0.0 (0.0 to 0.1) | 0.478 | 0.0 ± 0.1 | 0.0 ± 0.0 | 0.0 (0.0 to 0.0) | 0.324 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 (0.0 to 0.0) | 0.761 | 0.0 ± 0.1 | 0.0 ± 0.0 | 0.0 (0.0 to 0.1) | 0.349 |
| IL-6 | (pg/mL) | 1.0 ± 0.8 | 1.0 ± 0.6 | 0.0 (−0.3 to 0.3) | 0.937 | 1.4 ± 1.0 | 1.4 ± 1.0 | 0.1 (−0.4 to 0.5) | 0.807 | 1.2 ± 0.6 | 1.4 ± 0.7 | -0.2 (−0.5 to 0.1) | 0.227 | 1.2 ± 0.6 | 1.3 ± 0.8 | −0.1 (−0.4 to 0.3) | 0.737 |
| Hs-CRP | (mg/dL) | 0.2 ± 0.3 | 0.1 ± 0.2 | 0.0 (−0.1 to 0.1) | 0.428 | 0.2 ± 0.3 | 0.2 ± 0.5 | 0.0 (−0.2 to 0.2) | 0.856 | 0.1 ± 0.2 | 0.1 ± 0.2 | 0.0 (−0.1 to 0.1) | 0.854 | 0.2 ± 0.4 | 0.1 ± 0.2 | 0.1 (−0.1 to 0.2) | 0.306 |
| PⅡCP | (ng/mL) | 111.6 ± 58.6 | 94.9 ± 45.5 | 16.7 (−6.8 to 40.2) | 0.160 | 121.9 ± 45.2 | 112.1 ± 33.7 | 9.7 (−8.1 to 27.6) | 0.280 | 135.2 ± 76.9 | 106.2 ± 70.6 | 29.0 (−3.9 to 61.9) | 0.083 | 61.4 ± 18.6 | 60.0 ± 22.8 | 1.5 (−7.8 to 10.7) | 0.754 |
| CⅡC | (ng/mL) | 154.8 ± 30.0 | 146.3 ± 21.7 | 8.5 (−3.2 to 20.3) | 0.152 | 164.6 ± 24.6 | 167.3 ± 31.6 | −2.7 (−15.3 to 9.8) | 0.667 | 129.0 ± 17.1 | 124.8 ± 16.2 | 4.1 (−3.3 to 11.6) | 0.270 | 144.9 ± 22.8 | 141.3± 25.3 | 3.6 (−7.1 to 14.3) | 0.508 |
| 0 to 4 Week | 0 to 8 Week | 0 to 12 Week | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | MSM Group | Placebo Group | Difference | p Value 1 | ||
| (Unit) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | Mean ± SD | Mean ± SD | (95% CI) | ||||
| PⅡCP | (amount of change) | 10.3 ± 58.0 | 17.2 ± 57.0 | 6.7 (−15.5 to 28.9) | 0.554 | 23.6 ± 99.4 | 11.3 ± 84.8 | 30.0 (7.8 to 52.2) | 0.008 ** | −50.1 ± 52.7 | -34.9 ± 46.8 | −0.7 (−22.8 to 21.5) | 0.953 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toguchi, A.; Noguchi, N.; Kanno, T.; Yamada, A. Methylsulfonylmethane Improves Knee Quality of Life in Participants with Mild Knee Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2023, 15, 2995. https://doi.org/10.3390/nu15132995
Toguchi A, Noguchi N, Kanno T, Yamada A. Methylsulfonylmethane Improves Knee Quality of Life in Participants with Mild Knee Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2023; 15(13):2995. https://doi.org/10.3390/nu15132995
Chicago/Turabian StyleToguchi, Akifumi, Naoto Noguchi, Toshihiro Kanno, and Akira Yamada. 2023. "Methylsulfonylmethane Improves Knee Quality of Life in Participants with Mild Knee Pain: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 15, no. 13: 2995. https://doi.org/10.3390/nu15132995
APA StyleToguchi, A., Noguchi, N., Kanno, T., & Yamada, A. (2023). Methylsulfonylmethane Improves Knee Quality of Life in Participants with Mild Knee Pain: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients, 15(13), 2995. https://doi.org/10.3390/nu15132995