
Association of Serum Vitamin B12 and Circulating Methylmalonic Acid Levels with All-Cause and Cardiovascular Disease Mortality among Individuals with Chronic Kidney Disease


Abstract
1. Introduction
2. Materials and Methods
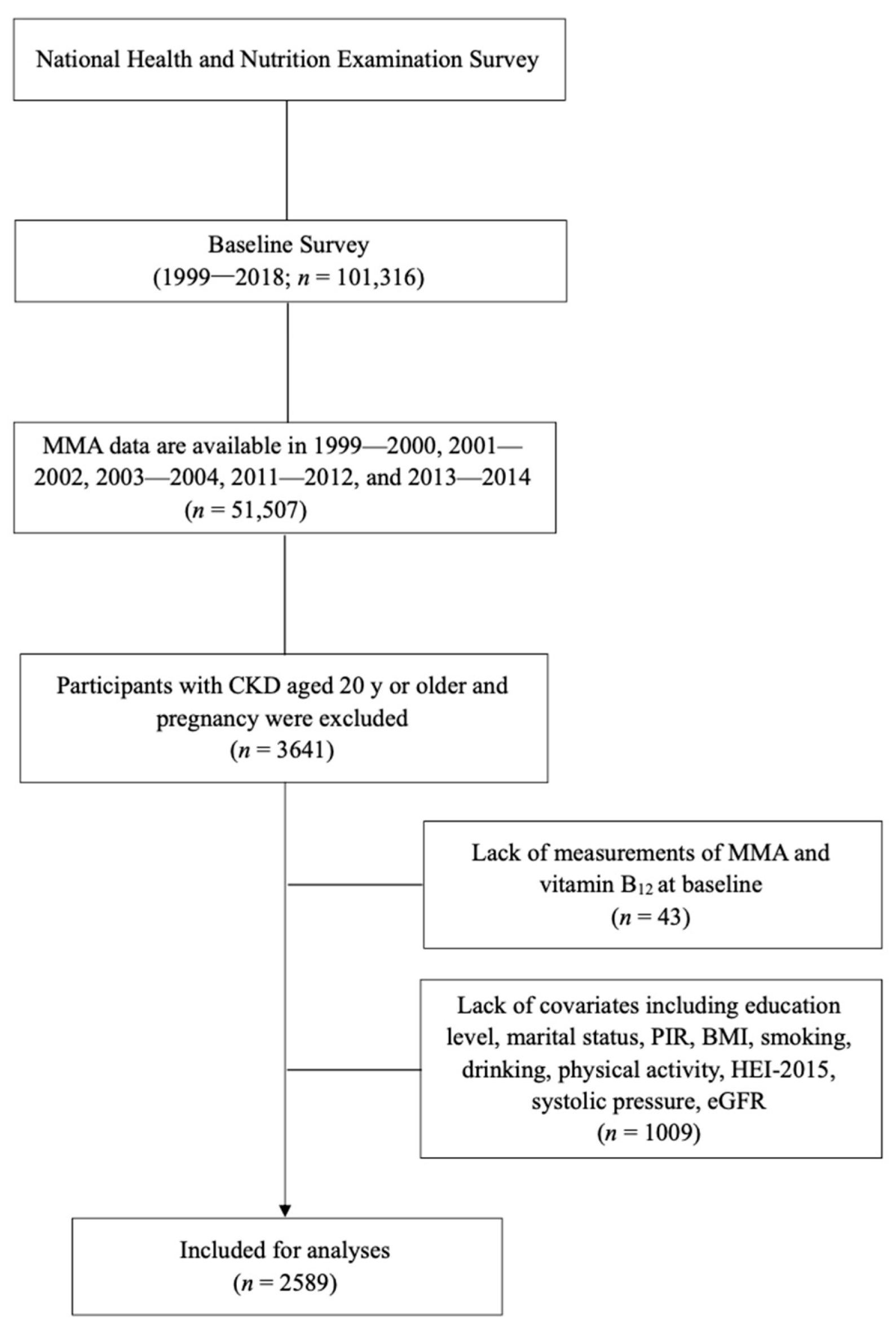
2.1. Study Population
2.2. Measurements of MMA and Vitamin B12
2.3. Ascertainment of Mortality
2.4. Measurement of Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
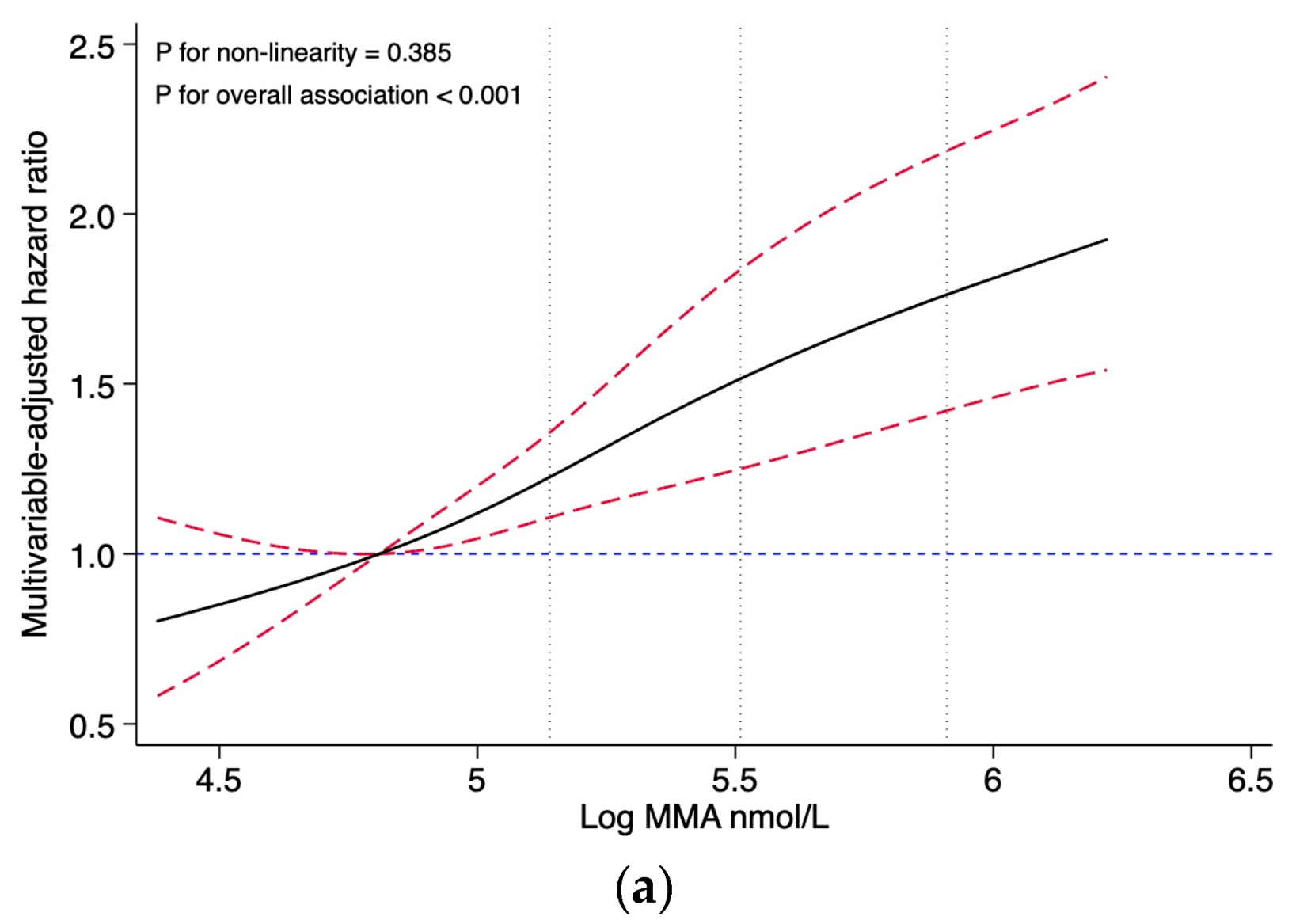
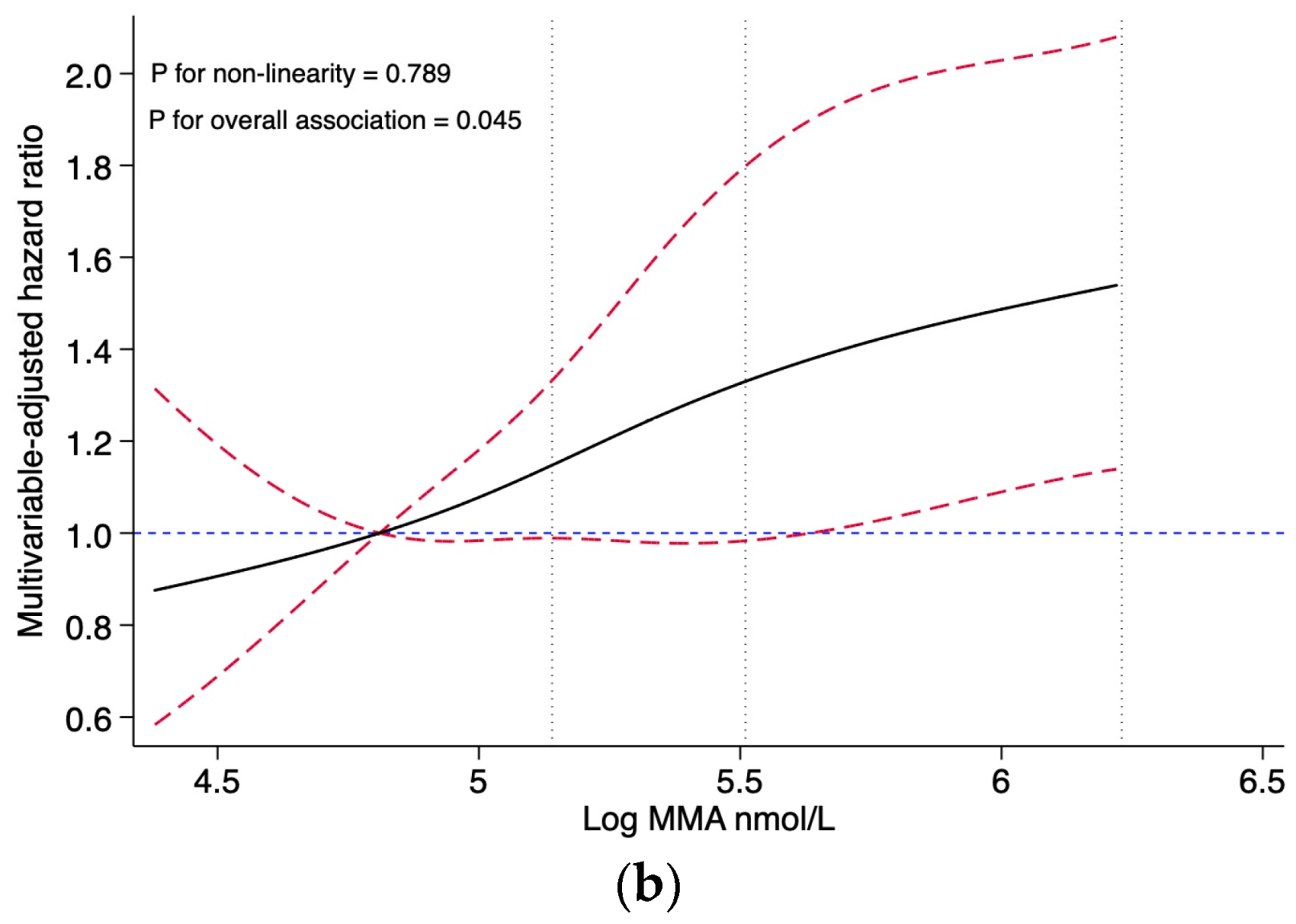
3.2. MMA and Mortality
3.3. Vitamin B12 and Mortality
3.4. Stratified and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.; Garcia-Garcia, G.; Lui, S.F.; Andreoli, S.; Fung, W.W.; Hradsky, A.; Kumaraswami, L.; Liakopoulos, V.; Rakhimova, Z.; Saadi, G.; et al. Kidney Health for Everyone Everywhere-From Prevention to Detection and Equitable Access to Care. J. Ren. Care 2020, 46, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Kazancioglu, R. Risk factors for chronic kidney disease: An update. Kidney Int. Suppl. 2013, 3, 368–371. [Google Scholar] [CrossRef]
- Green, R.; Allen, L.H.; Bjorke-Monsen, A.L.; Brito, A.; Gueant, J.L.; Miller, J.W.; Molloy, A.M.; Nexo, E.; Stabler, S.; Toh, B.H.; et al. Vitamin B(12) deficiency. Nat. Rev. Dis. Primers 2017, 3, 17040. [Google Scholar] [CrossRef]
- Allen, R.H.; Stabler, S.P.; Savage, D.G.; Lindenbaum, J. Metabolic abnormalities in cobalamin (vitamin B12) and folate deficiency. FASEB J. 1993, 7, 1344–1353. [Google Scholar] [CrossRef]
- Klee, G.G. Cobalamin and folate evaluation: Measurement of methylmalonic acid and homocysteine vs vitamin B(12) and folate. Clin. Chem. 2000, 46 Pt 2, 1277–1283. [Google Scholar] [CrossRef]
- Al-Lahham, S.H.; Peppelenbosch, M.P.; Roelofsen, H.; Vonk, R.J.; Venema, K. Biological effects of propionic acid in humans; metabolism, potential applications and underlying mechanisms. Biochim. Biophys. Acta 2010, 1801, 1175–1183. [Google Scholar] [CrossRef]
- Hosseini, E.; Grootaert, C.; Verstraete, W.; Van de Wiele, T. Propionate as a health-promoting microbial metabolite in the human gut. Nutr. Rev. 2011, 69, 245–258. [Google Scholar] [CrossRef]
- Riphagen, I.J.; Minovic, I.; Groothof, D.; Post, A.; Eggersdorfer, M.L.; Kootstra-Ros, J.E.; de Borst, M.H.; Navis, G.; Muskiet, F.A.J.; Kema, I.P.; et al. Methylmalonic acid, vitamin B12, renal function, and risk of all-cause mortality in the general population: Results from the prospective Lifelines-MINUTHE study. BMC Med. 2020, 18, 380. [Google Scholar] [CrossRef]
- van Loon, S.L.; Wilbik, A.M.; Kaymak, U.; van den Heuvel, E.R.; Scharnhorst, V.; Boer, A.K. Improved testing for vitamin B(12) deficiency: Correcting MMA for eGFR reduces the number of patients classified as vitamin B(12) deficient. Ann. Clin. Biochem. 2018, 55, 685–692. [Google Scholar] [CrossRef]
- Herrmann, W.; Schorr, H.; Geisel, J.; Riegel, W. Homocysteine, cystathionine, methylmalonic acid and B-vitamins in patients with renal disease. Clin. Chem. Lab. Med. 2001, 39, 739–746. [Google Scholar] [CrossRef]
- Stepien, K.M.; Heaton, R.; Rankin, S.; Murphy, A.; Bentley, J.; Sexton, D.; Hargreaves, I.P. Evidence of Oxidative Stress and Secondary Mitochondrial Dysfunction in Metabolic and Non-Metabolic Disorders. J. Clin. Med. 2017, 6, 71. [Google Scholar] [CrossRef]
- Chandler, R.J.; Zerfas, P.M.; Shanske, S.; Sloan, J.; Hoffmann, V.; DiMauro, S.; Venditti, C.P. Mitochondrial dysfunction in mut methylmalonic acidemia. FASEB J. 2009, 23, 1252–1261. [Google Scholar] [CrossRef]
- Galvan, D.L.; Green, N.H.; Danesh, F.R. The hallmarks of mitochondrial dysfunction in chronic kidney disease. Kidney Int. 2017, 92, 1051–1057. [Google Scholar] [CrossRef]
- Huang, Y.C.; Lee, M.S.; Wahlqvist, M.L. Prediction of all-cause mortality by B group vitamin status in the elderly. Clin. Nutr. 2012, 31, 191–198. [Google Scholar] [CrossRef]
- Mendonca, N.; Jagger, C.; Granic, A.; Martin-Ruiz, C.; Mathers, J.C.; Seal, C.J.; Hill, T.R. Elevated Total Homocysteine in All Participants and Plasma Vitamin B12 Concentrations in Women Are Associated with All-Cause and Cardiovascular Mortality in the Very Old: The Newcastle 85+Study. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 2018, 73, 1258–1264. [Google Scholar] [CrossRef]
- Callaghan, F.M.; Leishear, K.; Abhyankar, S.; Demner-Fushman, D.; McDonald, C.J. High vitamin B12 levels are not associated with increased mortality risk for ICU patients after adjusting for liver function: A cohort study. ESPEN J. 2014, 9, e76–e83. [Google Scholar] [CrossRef]
- Cappello, S.; Cereda, E.; Rondanelli, M.; Klersy, C.; Cameletti, B.; Albertini, R.; Magno, D.; Caraccia, M.; Turri, A.; Caccialanza, R. Elevated Plasma Vitamin B12 Concentrations Are Independent Predictors of In-Hospital Mortality in Adult Patients at Nutritional Risk. Nutrients 2017, 9, 1. [Google Scholar] [CrossRef]
- Soohoo, M.; Ahmadi, S.F.; Qader, H.; Streja, E.; Obi, Y.; Moradi, H.; Rhee, C.M.; Kim, T.H.; Kovesdy, C.P.; Kalantar-Zadeh, K. Association of serum vitamin B12 and folate with mortality in incident hemodialysis patients. Nephrol. Dial. Transplant. 2017, 32, 1024–1032. [Google Scholar] [CrossRef]
- Wolffenbuttel, B.H.R.; Heiner-Fokkema, M.R.; Green, R.; Gans, R.O.B. Relationship between serum B12 concentrations and mortality: Experience in NHANES. BMC Med. 2020, 18, 307. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tang, Y.; Liu, Y.; Cai, W.; Xu, J. Correlations between circulating methylmalonic acid levels and all-cause and cause-specific mortality among patients with diabetes. Front. Nutr. 2022, 9, 974938. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liu, Y.; Liu, J.; Tian, W.; Zhang, X.; Cai, H.; Fang, S.; Yu, B. Mitochondria-derived methylmalonic acid, a surrogate biomarker of mitochondrial dysfunction and oxidative stress, predicts all-cause and cardiovascular mortality in the general population. Redox Biol. 2020, 37, 101741. [Google Scholar] [CrossRef] [PubMed]
- Statistics NCfH. NHANES Questionnaires, Datasets, and Related Documentation. 2020. Available online: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx (accessed on 13 December 2022).
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- The Kidney Disease Improving Global Outcomes (KDIGO) Guideline. 2012. Available online: https://kdigo.org/guidelines/ckd-evaluation-and-management/ (accessed on 25 December 2022).
- Mineva, E.M.; Zhang, M.; Rabinowitz, D.J.; Phinney, K.W.; Pfeiffer, C.M. An LC-MS/MS method for serum methylmalonic acid suitable for monitoring vitamin B12 status in population surveys. Anal. Bioanal. Chem. 2015, 407, 2955–2964. [Google Scholar] [CrossRef]
- Yetley, E.A.; Pfeiffer, C.M.; Phinney, K.W.; Bailey, R.L.; Blackmore, S.; Bock, J.L.; Brody, L.C.; Carmel, R.; Curtin, L.R.; Durazo-Arvizu, R.A.; et al. Biomarkers of vitamin B-12 status in NHANES: A roundtable summary. Am. J. Clin. Nutr. 2011, 94, 313S–321S. [Google Scholar] [CrossRef]
- Odutayo, A.; Gill, P.; Shepherd, S.; Akingbade, A.; Hopewell, S.; Tennankore, K.; Hunn, B.H.; Emdin, C.A. Income Disparities in Absolute Cardiovascular Risk and Cardiovascular Risk Factors in the United States, 1999–2014. JAMA Cardiol. 2017, 2, 782–790. [Google Scholar] [CrossRef]
- Yang, X.; Xue, Q.; Wen, Y.; Huang, Y.; Wang, Y.; Mahai, G.; Yan, T.; Liu, Y.; Rong, T.; Wang, Y.; et al. Environmental polycyclic aromatic hydrocarbon exposure in relation to metabolic syndrome in US adults. Sci. Total Environ. 2022, 840, 156673. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef]
- NHANES Survey Methods and Analytic Guidelines. 2022. Available online: https://wwwn.cdc.gov/nchs/nhanes/analyticguidelines.aspx (accessed on 29 December 2022).
- Flores-Guerrero, J.L.; Minovic, I.; Groothof, D.; Gruppen, E.G.; Riphagen, I.J.; Kootstra-Ros, J.; Muller Kobold, A.; Hak, E.; Navis, G.; Gansevoort, R.T.; et al. Association of Plasma Concentration of Vitamin B12 with All-Cause Mortality in the General Population in the Netherlands. JAMA Netw. Open 2020, 3, e1919274. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Rochtchina, E.; Thiagalingam, A.; Mitchell, P. Serum homocysteine and folate but not vitamin B12 are predictors of CHD mortality in older adults. Eur. J. Prev. Cardiol. 2012, 19, 1420–1429. [Google Scholar] [CrossRef]
- Robinson, D.J.; O’Luanaigh, C.; Tehee, E.; O’Connell, H.; Hamilton, F.; Chin, A.V.; Coen, R.; Molloy, A.M.; Scott, J.; Lawlor, B.A.; et al. Vitamin B12 status, homocysteine and mortality amongst community-dwelling Irish elders. Ir. J. Med. Sci. 2011, 180, 451–455. [Google Scholar] [CrossRef]
- Liu, Y.; Geng, T.; Wan, Z.; Lu, Q.; Zhang, X.; Qiu, Z.; Li, L.; Zhu, K.; Liu, L.; Pan, A.; et al. Associations of Serum Folate and Vitamin B12 Levels with Cardiovascular Disease Mortality Among Patients with Type 2 Diabetes. JAMA Netw. Open 2022, 5, e2146124. [Google Scholar] [CrossRef]
- Dou, J.; Xu, W.; Ye, B.; Zhang, Y.; Mao, W. Serum vitamin B12 levels as indicators of disease severity and mortality of patients with acute-on-chronic liver failure. Clin. Chim. Acta 2012, 413, 1809–1812. [Google Scholar] [CrossRef]
- Capelli, I.; Cianciolo, G.; Gasperoni, L.; Zappulo, F.; Tondolo, F.; Cappuccilli, M.; La Manna, G. Folic Acid and Vitamin B12 Administration in CKD, Why Not? Nutrients 2019, 11, 383. [Google Scholar] [CrossRef]
- Dhar, I.; Lysne, V.; Ulvik, A.; Svingen, G.F.T.; Pedersen, E.R.; Bjornestad, E.O.; Olsen, T.; Borsholm, R.; Laupsa-Borge, J.; Ueland, P.M.; et al. Plasma methylmalonic acid predicts risk of acute myocardial infarction and mortality in patients with coronary heart disease: A prospective 2-cohort study. J. Intern. Med. 2023, 293, 508–519. [Google Scholar] [CrossRef]
- Mineva, E.M.; Sternberg, M.R.; Zhang, M.; Aoki, Y.; Storandt, R.; Bailey, R.L.; Pfeiffer, C.M. Age-specific reference ranges are needed to interpret serum methylmalonic acid concentrations in the US population. Am. J. Clin. Nutr. 2019, 110, 158–168. [Google Scholar] [CrossRef]
- Vogiatzoglou, A.; Oulhaj, A.; Smith, A.D.; Nurk, E.; Drevon, C.A.; Ueland, P.M.; Vollset, S.E.; Tell, G.S.; Refsum, H. Determinants of plasma methylmalonic acid in a large population: Implications for assessment of vitamin B12 status. Clin. Chem. 2009, 55, 2198–2206. [Google Scholar] [CrossRef]
- Piquereau, J.; Moulin, M.; Zurlo, G.; Mateo, P.; Gressette, M.; Paul, J.L.; Lemaire, C.; Ventura-Clapier, R.; Veksler, V.; Garnier, A. Cobalamin and folate protect mitochondrial and contractile functions in a murine model of cardiac pressure overload. J. Mol. Cell Cardiol. 2017, 102, 34–44. [Google Scholar] [CrossRef]
- van de Lagemaat, E.E.; de Groot, L.; van den Heuvel, E. Vitamin B(12) in Relation to Oxidative Stress: A Systematic Review. Nutrients 2019, 11, 482. [Google Scholar] [CrossRef]
- Clarke, R.; Refsum, H.; Birks, J.; Evans, J.G.; Johnston, C.; Sherliker, P.; Ueland, P.M.; Schneede, J.; McPartlin, J.; Nexo, E.; et al. Screening for vitamin B-12 and folate deficiency in older persons. Am. J. Clin. Nutr. 2003, 77, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Valente, E.; Scott, J.M.; Ueland, P.M.; Cunningham, C.; Casey, M.; Molloy, A.M. Diagnostic accuracy of holotranscobalamin, methylmalonic acid, serum cobalamin, and other indicators of tissue vitamin B₁₂ status in the elderly. Clin. Chem. 2011, 57, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A. Elevated serum methylmalonic acid. How much comes from cobalamin deficiency and how much comes from the kidneys? Scand. J. Clin. Lab. Investig. 2002, 62, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Fontecha-Barriuso, M.; Lopez-Diaz, A.M.; Guerrero-Mauvecin, J.; Miguel, V.; Ramos, A.M.; Sanchez-Niño, M.D.; Ruiz-Ortega, M.; Ortiz, A.; Sanz, A.B. Tubular Mitochondrial Dysfunction, Oxidative Stress, and Progression of Chronic Kidney Disease. Antioxidants 2022, 11, 1356. [Google Scholar] [CrossRef]
- Mc Guire, P.J.; Parikh, A.; Diaz, G.A. Profiling of oxidative stress in patients with inborn errors of metabolism. Mol. Genet. Metab. 2009, 98, 173–180. [Google Scholar] [CrossRef]
- Meijers, B.; Evenepoel, P.; Anders, H.J. Intestinal microbiome and fitness in kidney disease. Nat. Rev. Nephrol. 2019, 15, 531–545. [Google Scholar] [CrossRef]
- Melo, D.R.; Kowaltowski, A.J.; Wajner, M.; Castilho, R.F. Mitochondrial energy metabolism in neurodegeneration associated with methylmalonic acidemia. J. Bioenerg. Biomembr. 2011, 43, 39–46. [Google Scholar] [CrossRef]
- Weisfeld-Adams, J.D.; Morrissey, M.A.; Kirmse, B.M.; Salveson, B.R.; Wasserstein, M.P.; McGuire, P.J.; Sunny, S.; Cohen-Pfeffer, J.L.; Yu, C.; Caggana, M.; et al. Newborn screening and early biochemical follow-up in combined methylmalonic aciduria and homocystinuria, cblC type, and utility of methionine as a secondary screening analyte. Mol. Genet. Metab. 2010, 99, 116–123. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Participants, No. (%) | p-Value a | ||||
|---|---|---|---|---|---|---|
| MMA Levels, nmol/L | ||||||
| Total | Quartile 1 (<123) | Quartile 2 (123–169) | Quartile 3 (170–239) | Quartile 4 (≥240) | ||
| Participants, No. (%) | 2589 (100.0) | 642 (24.8) | 592 (22.8) | 665 (25.7) | 690 (26.7) | - |
| Age, years, mean (SE) | 59.04 (0.6) | 46.79 (0.8) | 57.75 (1.1) | 63.64 (0.9) | 67.55 (0.8) | <0.001 |
| Sex, n (%) | 0.095 | |||||
| Male | 1324 (46.8) | 294 (42.2) | 306 (47.1) | 360 (51.0) | 364 (46.6) | |
| Female | 1265 (53.2) | 348 (57.8) | 286 (52.9) | 305 (49.0) | 326 (53.4) | |
| Race, n (%) | <0.001 | |||||
| Hispanic | 580 (12.6) | 223 (23.6) | 124 (10.8) | 125 (9.4) | 108 (7.1) | |
| Non-Hispanic white | 1302 (69.7) | 190 (52.2) | 287 (70.1) | 389 (76.5) | 436 (79.6) | |
| Non-Hispanic black | 543 (11.5) | 189 (17.8) | 135 (12.4) | 121 (9.0) | 98 (7.1) | |
| Others | 164 (6.1) | 40 (6.4) | 46 (6.8) | 30 (5.1) | 48 (6.3) | |
| Education, n (%) | 0.179 | |||||
| Less than high school | 911 (25.2) | 226 (23.8) | 203 (24.8) | 239 (25.0) | 243 (27.0) | |
| High school | 594 (24.2) | 146 (22.4) | 133 (22.7) | 141 (23.9) | 174 (27.8) | |
| College or higher | 1084 (50.7) | 270 (53.9) | 256 (52.6) | 285 (51.1) | 273 (45.2) | |
| Marital status, n (%) | <0.001 | |||||
| Married | 1337 (53.9) | 330 (50.5) | 320 (55.6) | 354 (58.2) | 333 (51.1) | |
| Separated | 980 (34.4) | 204 (30.6) | 204 (31.7) | 260 (34.2) | 312 (40.6) | |
| Never married | 272 (11.9) | 108 (18.9) | 68 (12.8) | 51 (7.7) | 45 (8.4) | |
| PIR, n (%) | 0.089 | |||||
| ≤1 | 554 (17.0) | 154 (20.4) | 125 (16.2) | 139 (15.5) | 136 (16.1) | |
| 1 to 4 | 1512 (54.9) | 365 (53.5) | 351 (53.5) | 366 (52.6) | 430 (59.9) | |
| ≥4 | 523 (28.1) | 123 (26.1) | 116 (30.4) | 160 (31.9) | 124 (23.9) | |
| Smoking, n (%) | <0.001 | |||||
| Never | 2043 (76.9) | 463 (69.1) | 448 (73.6) | 548 (80.6) | 584 (83.8) | |
| Former | 68 (3.1) | 23 (5.2) | 14 (2.3) | 17 (2.9) | 14 (2.1) | |
| Current | 478 (20.0) | 156 (25.8) | 130 (24.0) | 100 (16.5) | 92 (14.0) | |
| Drinking, n (%) | 0.202 | |||||
| None | 900 (33.3) | 208 (30.5) | 195 (30.1) | 230 (33.2) | 267 (39.1) | |
| Moderate | 1492 (58.2) | 374 (59.8) | 342 (60.4) | 387 (58.2) | 389 (54.4) | |
| Heavy | 197 (8.6) | 60 (9.7) | 55 (9.6) | 48 (8.6) | 34 (6.5) | |
| Physical activity, n (%) | <0.001 | |||||
| Low | 1173 (49.1) | 339 (58.8) | 291 (53.6) | 292 (46.4) | 251 (37.8) | |
| Moderate | 549 (21.3) | 135 (20.2) | 118 (20.2) | 149 (23.0) | 147 (21.8) | |
| High | 867 (29.6) | 168 (21.0) | 183 (26.2) | 224 (30.6) | 292 (40.4) | |
| CKD stages | <0.001 | |||||
| Stage 1 | 938 (41.1) | 458 (74.7) | 253 (47.9) | 143 (27.5) | 84 (15.4) | |
| Stage 2 | 668 (24.2) | 135 (17.4) | 187 (27.1) | 205 (30.8) | 141 (21.2) | |
| Stage 3 | 908 (32.8) | 48 (7.8) | 150 (24.9) | 312 (41.1) | 398 (56.3) | |
| Stages 4 and 5 | 75 (2.0) | 1 (0.1) | 2 (0.1) | 5 (0.6) | 67 (7.2) | |
| BMI, kg/m2, mean (SE) | 29.43 (0.2) | 29.51 (0.4) | 29.32 (0.4) | 29.41 (0.3) | 29.49 (0.3) | 0.060 |
| HEI-2015, mean (SE) | 53.08 (0.4) | 50.88 (0.7) | 53.28 (0.6) | 53.82 (0.7) | 54.28 (0.6) | <0.001 |
| Systolic blood pressure, mm Hg, mean (SE) | 133.42 (0.5) | 127.90 (1.1) | 134.89 (1.1) | 134.81 (1.2) | 135.94 (1.2) | <0.001 |
| eGFR, mL/min/1.73 m2, mean (SE) | 81.42 (0.7) | 105.16 (1.3) | 86.74 (1.4) | 73.87 (1.2) | 60.77 (1.3) | <0.001 |
| Vitamin B12, pmol/L, mean (SE) | 481.77 (16.5) | 556.99 (50.8) | 493.10 (22.0) | 449.76 (11.6) | 430.01 (36.0) | <0.001 |
| Cause of death | MMA Levels (nmol/L), HR (95% CI) | p-Value for Trend a | ||||
|---|---|---|---|---|---|---|
| Log (MMA) | Quartile 1 (<123) | Quartile 2 (123–169) | Quartile 3 (170–239) | Quartile 4 (≥240) | ||
| All-cause mortality | ||||||
| No. of cases/person-years | 1192/24,301 | 169/7670 | 233/5888 | 337/5851 | 453/4892 | |
| Model 1 | 1.49 (1.29, 1.73) | 1.00 [Reference] | 1.16 (0.89, 1.51) | 1.22 (0.91, 1.62) | 1.96 (1.54, 2.50) | <0.001 |
| Model 2 | 1.50 (1.29, 1.75) | 1.00 [Reference] | 1.20 (0.91, 1.57) | 1.28 (0.94, 1.76) | 2.01 (1.54, 2.61) | <0.001 |
| Model 3 | 1.09 (0.90, 1.34) | 1.00 [Reference] | 1.20 (0.91, 1.57) | 1.28 (0.94, 1.76) | 2.01 (1.54, 2.62) | <0.001 |
| CVD mortality | ||||||
| No. of cases/person-years | 446/24,301 | 61/7670 | 95/5888 | 115/5851 | 175/4892 | |
| Model 1 | 1.39 (1.15, 1.68) | 1.00 [Reference] | 1.28 (0.86, 1.89) | 1.06 (0.74, 1.51) | 1.94 (1.38, 2.74) | <0.001 |
| Model 2 | 1.30 (1.08, 1.57) | 1.00 [Reference] | 1.29 (0.84, 1.97) | 1.04 (0.69, 1.58) | 1.76 (1.18, 2.63) | <0.001 |
| Model 3 | 1.30 (1.08, 1.57) | 1.00 [Reference] | 1.29 (0.85, 1.97) | 1.04 (0.69, 1.58) | 1.76 (1.18, 2.63) | <0.001 |
| Subgroup | MMA levels (nmol/L), HR (95% CI) | p-Value for Interaction a | ||||
|---|---|---|---|---|---|---|
| Log (MMA) | Quartile 1 (<123) | Quartile 2 (123–169) | Quartile 3 (170–239) | Quartile 4 (≥240) | ||
| Age, years | 0.255 | |||||
| <65 | 1.93 (1.50, 2.47) | 1.00 [Reference] | 1.39 (0.95, 2.06) | 1.84 (1.24, 2.73) | 2.83 (1.81, 4.43) | |
| ≥65 | 1.34 (1.20, 1.50) | 1.00 [Reference] | 1.02 (0.80, 1.30) | 1.19 (0.94, 1.50) | 1.75 (1.38, 2.21) | |
| Sex | 0.536 | |||||
| Male | 1.33 (1.17, 1.51) | 1.00 [Reference] | 1.08 (0.82, 1.42) | 1.21 (0.92, 1.58) | 1.73 (1.31, 2.29) | |
| Female | 1.69 (1.42, 2.01) | 1.00 [Reference] | 1.25 (0.91, 1.72) | 1.58 (1.15, 2.17) | 2.33 (1.69, 3.22) | |
| BMI, kg/m2 | 0.764 | |||||
| <30 | 1.26 (1.11, 1.42) | 1.00 [Reference] | 1.08 (0.84, 1.39) | 1.32 (1.02, 1.70) | 1.68 (1.30, 2.17) | |
| ≥30 | 2.05 (1.67, 2.51) | 1.00 [Reference] | 1.15 (0.81, 1.64) | 1.28 (0.90, 1.82) | 2.40 (1.68, 3.45) | |
| Smoking | 0.325 | |||||
| Never or former | 1.44 (1.29, 1.59) | 1.00 [Reference] | 1.17 (0.93, 1.48) | 1.39 (1.11, 1.75) | 1.99 (1.58, 2.51) | |
| Current | 1.67 (1.20, 2.34) | 1.00 [Reference] | 1.29 (0.80, 2.08) | 1.44 (0.87, 2.36) | 2.48 (1.41, 4.36) | |
| Drinking | 0.886 | |||||
| None | 1.45 (1.24, 1.69) | 1.00 [Reference] | 1.12 (0.78, 1.60) | 1.47 (1.03, 2.09) | 2.15 (1.51, 3.06) | |
| Moderate | 1.45 (1.26, 1.67) | 1.00 [Reference] | 1.14 (0.86, 1.50) | 1.28 (0.97, 1.69) | 1.85 (1.39, 2.47) | |
| Heavy | 1.84 (1.01, 3.33) | 1.00 [Reference] | 1.19 (0.55, 2.60) | 1.15 (0.51, 2.58) | 2.50 (1.03, 6.11) | |
| Physical activity | 0.128 | |||||
| Low | 1.46 (1.24, 1.72) | 1.00 [Reference] | 0.96 (0.70, 1.33) | 1.20 (0.88, 1.65) | 1.90 (1.37, 2.65) | |
| Moderate | 1.75 (1.36, 2.25) | 1.00 [Reference] | 1.51 (0.93, 2.44) | 1.98 (1.23, 3.19) | 2.96 (1.77, 4.96) | |
| High | 1.33 (1.14, 1.56) | 1.00 [Reference] | 1.16 (0.83, 1.63) | 1.20 (0.85, 1.69) | 1.80 (1.27, 2.54) | |
| eGFR, mL/min/1.73 m2 | 0.614 | |||||
| <60 | 1.31 (1.13, 1.52) | 1.00 [Reference] | 1.02 (0.65, 1.59) | 1.36 (0.90, 2.05) | 1.74 (1.15, 2.62) | |
| ≥60 | 1.44 (1.26, 1.66) | 1.00 [Reference] | 1.22 (0.96, 1.54) | 1.34 (1.04, 1.73) | 2.17 (1.66, 2.84) | |
| CKD stage | 0.147 | |||||
| 1 | 1.29 (1.02, 1.64) | 1.00 [Reference] | 1.07 (0.74, 1.54) | 1.49 (0.99, 2.24) | 1.92 (1.18, 3.14) | |
| 2 | 1.71 (1.41, 2.08) | 1.00 [Reference] | 1.37 (0.99, 1.89) | 1.35 (0.96, 1.91) | 2.44 (1.73, 3.46) | |
| Stage 3–5 | 1.31 (1.13, 1.52) | 1.00 [Reference] | 1.02 (0.65, 1.59) | 1.36 (0.90, 2.05) | 1.74 (1.15, 2.62) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.; Chang, W.; Xie, Z.; Yao, B.; Wang, X.; Yang, C. Association of Serum Vitamin B12 and Circulating Methylmalonic Acid Levels with All-Cause and Cardiovascular Disease Mortality among Individuals with Chronic Kidney Disease. Nutrients 2023, 15, 2980. https://doi.org/10.3390/nu15132980
Wu S, Chang W, Xie Z, Yao B, Wang X, Yang C. Association of Serum Vitamin B12 and Circulating Methylmalonic Acid Levels with All-Cause and Cardiovascular Disease Mortality among Individuals with Chronic Kidney Disease. Nutrients. 2023; 15(13):2980. https://doi.org/10.3390/nu15132980
Chicago/Turabian StyleWu, Shiyi, Wenling Chang, Zhihao Xie, Boshuang Yao, Xiaoyu Wang, and Chunxia Yang. 2023. "Association of Serum Vitamin B12 and Circulating Methylmalonic Acid Levels with All-Cause and Cardiovascular Disease Mortality among Individuals with Chronic Kidney Disease" Nutrients 15, no. 13: 2980. https://doi.org/10.3390/nu15132980
APA StyleWu, S., Chang, W., Xie, Z., Yao, B., Wang, X., & Yang, C. (2023). Association of Serum Vitamin B12 and Circulating Methylmalonic Acid Levels with All-Cause and Cardiovascular Disease Mortality among Individuals with Chronic Kidney Disease. Nutrients, 15(13), 2980. https://doi.org/10.3390/nu15132980