
Full Breastfeeding and Allergic Diseases—Long-Term Protection or Rebound Effects?
 , ,
, ,  ,
,
Abstract
1. Introduction
- Is early eczema a determinant of the course of allergic diseases until early adulthood which should be considered in long-term analysis of breastfeeding effects?
- Does early eczema modify potential long-term associations of milk feeding with the development of atopic diseases?
2. Materials and Methods
2.1. Study Design of the GINIplus Study
2.2. Definition of Outcome and Exposure Variables
2.3. Statistics
3. Results
3.1. Study Population and Characteristics
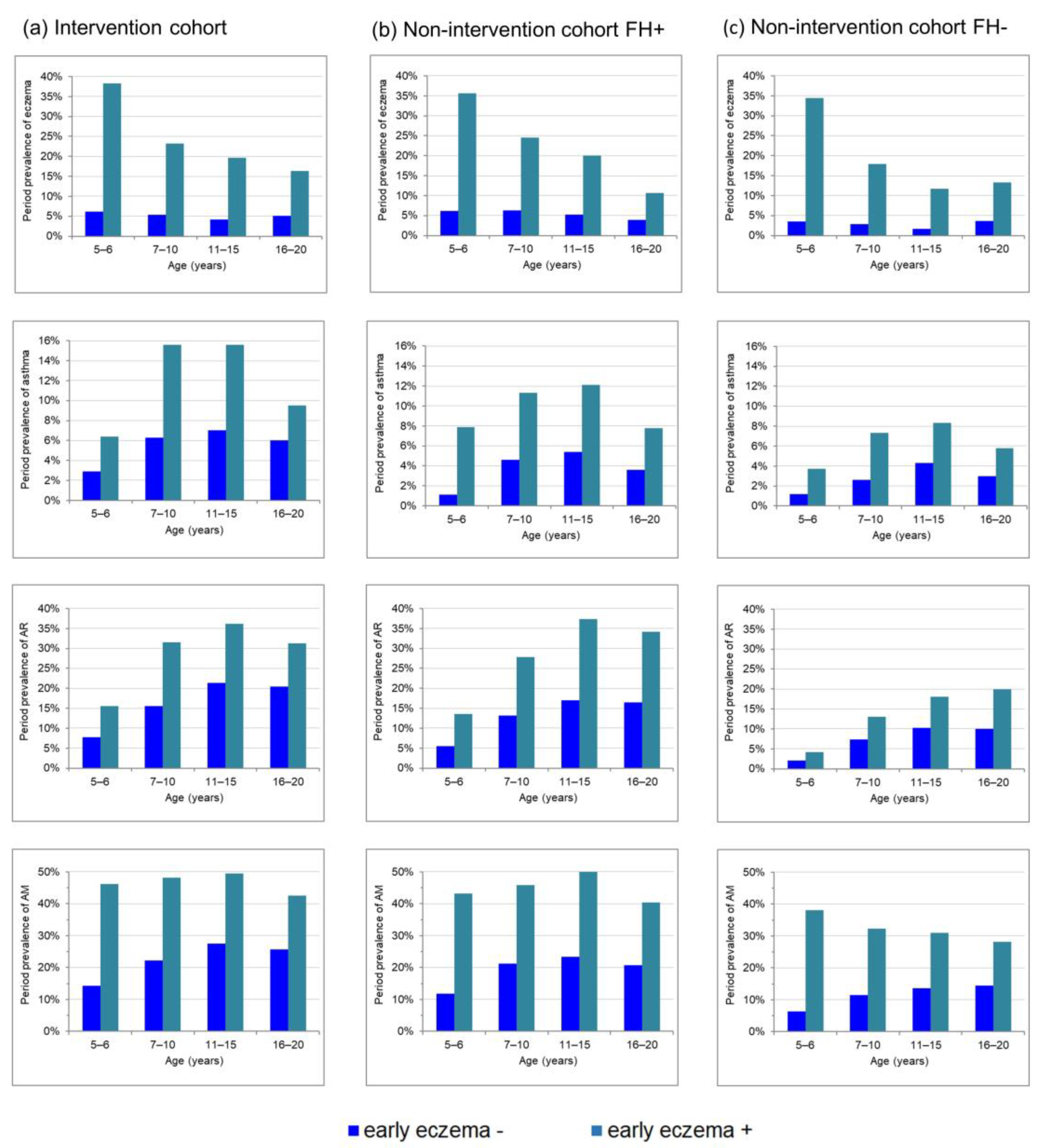
3.2. Development of Atopic Diseases up to Young Adulthood Depending on Early Eczema during the First Three Years of Life
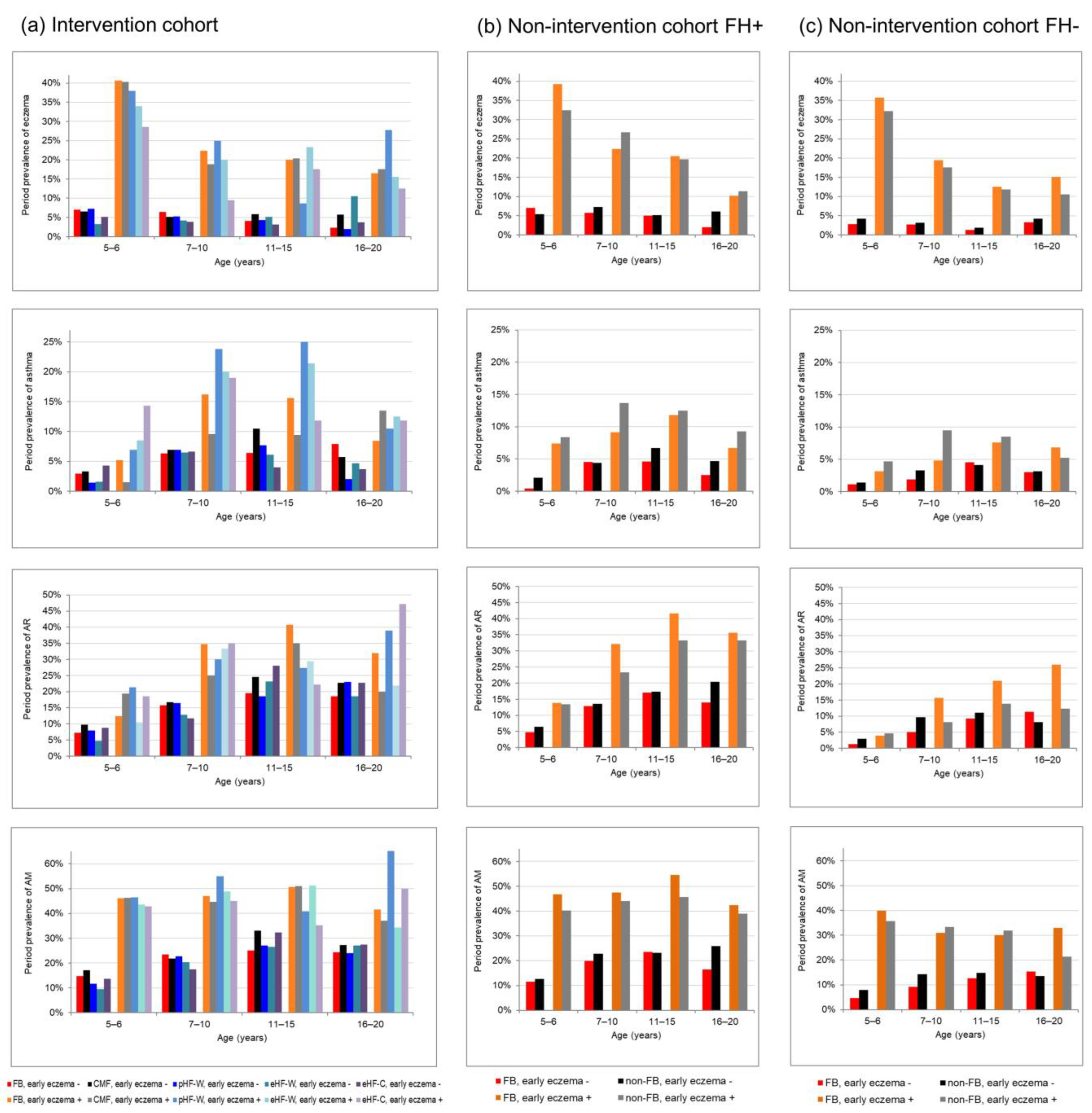
3.3. Short- and Long-Term Risk of Allergies in Fully-Breastfeed Children
3.4. Examination of a Potential Rebound Effect in Fully-Breastfed Children without Early Eczema

{kind=link}
{kind=link}
| Intervention Cohort (N = 1661) | Non-Intervention FH+ (N = 792) | Non-Intervention FH− (N = 1565) | ||
|---|---|---|---|---|
| Eczema | ||||
| Interaction feeding with early eczema * | p-value | 0.987 | 0.738 | 0.174 |
| Final Model | M1 | M2 | M1 | |
| FB vs. CMF/non FB | aOR (95%CI) | 1.1 (0.72–1.6) | 0.92 (0.62–1.3) | 0.94 (0.65–1.3) |
| eHF-C vs. CMF | aOR (95%CI) | 0.64 (0.34–1.2) | −1 | −1 |
| Interaction early eczema with time-periods | p-value | 0.002 | – | 0.006 |
| Early eczema effect at 5–6th years | aOR (95%CI) | 8.8 (6.3–12.3) | 14.4 (9.2–22.7) | |
| Early eczema effect at 7–10th years | aOR (95%CI) | 4.7 (3.2–7.0) | 7.7 (4.4–13.4) | |
| Early eczema effect at 11–15th years | aOR (95%CI) | 4.9 (3.1–7.7) | 8.6 (4.2–17.4) | |
| Early eczema effect at 16–20th years | aOR (95%CI) | 3.2 (2.0–5.1) | 3.9 (2.1–7.4) | |
| Early eczema effect | aOR (95%CI) | - | 5.0 (3.4–7.4) | - |
| Time-period 7–10th vs. 5–6th years | aOR (95%CI) | 0.76 (0.57–1.02) | ||
| 11–15th vs. 5–6th years | aOR (95%CI) | 0.58 (0.42–0.80) | ||
| 16–20th vs. 5–6th years | aOR (95%CI) | 0.34 (0.21–0.52) | ||
| Asthma | ||||
| Interaction feeding with early eczema * | p-value | 0.405 | 0.698 | 0.923 |
| Final model | M2 | M2 | M2 | |
| FB vs. CMF/non FB | aOR (95%CI) | 1.2 (0.72–2.1) | 0.78 (0.45–1.3) | 0.95 (0.59–1.5) |
| eHF-C vs. CMF | aOR (95%CI) | 1.1 (0.52–2.1) | −1 | −1 |
| Early eczema effect | aOR (95%CI | 2.2 (1.6–3.1) | 2.7 (1.6–4.9) | 2.4 (1.4–4.1) |
| Time-period 7–10th vs. 5–6th years | aOR (95%CI) | 2.5 (1.9–3.3) | 2.4 (1.6–3.6) | 2.0 (1.3–3.1) |
| 11–15th vs. 5–6th years | aOR (95%CI) | 2.7 (2.0–3.6) | 2.8 (1.7–4.5) | 3.1 (2.0–4.9) |
| 16–20th vs. 5–6th years | aOR (95%CI) | 1.9 (1.4–2.7) | 1.7 (1.0–3.0) | 2.2 (1.3–3.9) |
| AR | ||||
| Interaction feeding with early eczema * | p-value | 0.471 | 0.186 | 0.040 |
| Final model | M2 | M2 | M3 | |
| FB vs. CMF/non FB | aOR (95%CI) | 0.96 (0.68–1.3) | 0.98 (0.71–1.4) | - |
| eHF-C vs. CMF | aOR (95%CI) | 1.1 (0.69–1.7) | −1 | −1 |
| FB vs. non FB at early eczema - | aOR (95%CI) | 0.77 (0.53–1.1) | ||
| FB vs. non FB at early eczema + | aOR (95%CI) | 1.7 (0.84–3.4) | ||
| Early eczema effect | aOR (95%CI | 2.1 (1.7–2.7) | 2.7 (1.9–3.8) | |
| Early eczema effect at FB | aOR (95%CI) | 2.7 (1.7–4.5) | ||
| Early eczema effect at non FB | aOR (95%CI) | 1.2 (0.71–2.2) | ||
| Interaction feeding with time-periods | p-value | - | - | 0.004 |
| FB vs. non FB at 5 –6th years | aOR (95%CI) | 0.68 (0.33 –1.5) | ||
| FB vs. non FB at 7–10th years | aOR (95%CI) | 0.90 (0.55–1.5) | ||
| FB vs. non FB at 11–15th years | aOR (95%CI) | 1.3 (0.81–2.0) | ||
| FB vs. non FB at 16–20th years | aOR (95%CI) | 2.2 (1.3–3.6) | ||
| Time-period 7–10th vs. 5–6th years | aOR (95%CI) | 2.3 (1.9–2.8) | 2.5 (1.9–3.4) | |
| 11–15th vs. 5–6th years | aOR (95%CI) | 3.3 (2.7–4.0) | 3.6 (2.7–4.9) | |
| 16–20th vs. 5–6th years | aOR (95%CI) | 2.9 (2.4–3.6) | 3.4 (2.4–4.8) | |
| AM | ||||
| Interaction * feeding with early eczema | p-value | 0.558 | 0.169 | 0.177 |
| Final Model | M1 | M1 | M4 | |
| FB vs. CMF/non FB | aOR (95%CI) | 0.96 (0.72–1.3) | 1.0 (0.76–1.4) | − |
| eHF-C vs. CMF | aOR (95%CI) | 0.90 (0.61–1.3) | −1 | −1 |
| Interaction feeding with time-periods | p-value | − | − | 0.040 |
| FB vs. non FB at 5–6th years | aOR (95%CI) | 0.81 (0.55−1.2) | ||
| FB vs. non FB at 7–10th years | aOR (95%CI) | 0.70 (0.50–0.99) | ||
| FB vs. non FB at 11–15th years | aOR (95%CI) | 0.90 (0.64–1.3) | ||
| FB vs. non FB at 16–20th years | aOR (95%CI) | 1.3 (0.92–1.9) | ||
| Interaction early eczema with time-periods | p-value | 0.001 | 0.027 | 0.001 |
| Early eczema effect at 5–6th years | aOR (95%CI) | 5.2 (3.9–6.9) | 5.5 (3.6–8.4) | 9.1 (6.2–13.4) |
| Early eczema effect at 7–10th years | aOR (95%CI) | 3.2 (2.4–4.2) | 3.0 (2.0–4.5) | 3.6 (2.4–5.4) |
| Early eczema effect at 11–15th years | aOR (95%CI) | 2.5 (1.9–3.3) | 3.2 (2.2–4.8) | 2.8 (1.9–4.2) |
| Early eczema effect at 16–20th years | aOR (95%CI) | 2.1 (1.5–2.8) | 2.6 (1.6–4.2) | 2.2 (1.4–3.4) |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koletzko, B.; Bauer, C.-P.; Cierpka, M.; Cremer, M.; Flothkötter, M.; Graf, C.; Heindl, I.; Hellmers, C.; Kersting, M.; Krawinkel, M.; et al. Ernährung und Bewegung von Säuglingen und stillenden Frauen. Mon. Kinderheilkd 2016, 164, 771–798. [Google Scholar] [CrossRef]
- Kopp, M.V.; Muche-Borowski, C.; Abou-Dakn, M.; Ahrens, B.; Beyer, K.; Blümchen, K.; Bubel, P.; Chaker, A.; Cremer, M.; Ensenauer, R.; et al. S3 guideline Allergy Prevention. Allergol. Sel. 2022, 6, 61–97. [Google Scholar] [CrossRef] [PubMed]
- Van Meel, E.R.; de Jong, M.; Elbert, N.J.; den Dekker, H.T.; Reiss, I.K.; de Jongste, J.C.; Jaddoe, V.W.V.; Duijts, L. Duration and exclusiveness of breastfeeding and school-age lung function and asthma. Ann. Allergy Asthma Immunol. 2017, 119, 21–26.e2. [Google Scholar] [CrossRef] [PubMed]
- Groenwold, R.H.H.; Tilling, K.; Moons, K.G.M.; Hoes, A.W.; van der Ent, C.K.; Kramer, M.S.; Martin, R.M.; Sterne, J.A.C. Breast-feeding and health consequences in early childhood: Is there an impact of time-dependent confounding? Ann. Nutr. Metab. 2014, 65, 139–148. [Google Scholar] [CrossRef]
- Ajetunmobi, O.M.; Whyte, B.; Chalmers, J.; Tappin, D.M.; Wolfson, L.; Fleming, M.; MacDonald, A.; Wood, R.; Stockton, D.L. Breastfeeding is associated with reduced childhood hospitalization: Evidence from a Scottish Birth Cohort (1997–2009). J. Pediatr. 2015, 166, 620–625.e4. [Google Scholar] [CrossRef]
- Jelding-Dannemand, E.; Malby Schoos, A.-M.; Bisgaard, H. Breast-feeding does not protect against allergic sensitization in early childhood and allergy-associated disease at age 7 years. J. Allergy Clin. Immunol. 2015, 136, 1302–1308.e13. [Google Scholar] [CrossRef]
- Leung, J.Y.Y.; Kwok, M.K.; Leung, G.M.; Schooling, C.M. Breastfeeding and childhood hospitalizations for asthma and other wheezing disorders. Ann. Epidemiol. 2016, 26, 21–27.e3. [Google Scholar] [CrossRef]
- Filipiak-Pittroff, B.; Koletzko, S.; Krämer, U.; Standl, M.; Bauer, C.-P.; Berdel, D.; von Berg, A. Full breastfeeding and allergies from infancy until adolescence in the GINIplus cohort. Pediatr. Allergy Immunol. 2018, 29, 96–101. [Google Scholar] [CrossRef]
- Laubereau, B.; Brockow, I.; Zirngibl, A.; Koletzko, S.; Gruebl, A.; von Berg, A.; Filipiak-Pittroff, B.; Berdel, D.; Bauer, C.P.; Reinhardt, D.; et al. Effect of breast-feeding on the development of atopic dermatitis during the first 3 years of life--results from the GINI-birth cohort study. J. Pediatr. 2004, 144, 602–607. [Google Scholar] [CrossRef]
- Schoetzau, A.; Filipiak-Pittroff, B.; Franke, K.; Koletzko, S.; von Berg, A.; Gruebl, A.; Bauer, C.P.; Berdel, D.; Reinhardt, D.; Wichmann, H.-E. Effect of exclusive breast-feeding and early solid food avoidance on the incidence of atopic dermatitis in high-risk infants at 1 year of age. Pediatr. Allergy Immunol. 2002, 13, 234–242. [Google Scholar] [CrossRef]
- Lodge, C.J.; Tan, D.J.; Lau, M.X.Z.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.J.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef]
- Gappa, M.; Filipiak-Pittroff, B.; Libuda, L.; von Berg, A.; Koletzko, S.; Bauer, C.-P.; Heinrich, J.; Schikowski, T.; Berdel, D.; Standl, M. Long-term effects of hydrolyzed formulae on atopic diseases in the GINI study. Allergy 2021, 76, 1903–1907. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.v.; Krämer, U.; Link, E.; Bollrath, C.; Heinrich, J.; Brockow, I.; Koletzko, S.; Grübl, A.; Filipiak-Pittroff, B.; Wichmann, H.-E.; et al. Impact of early feeding on childhood eczema: Development after nutritional intervention compared with the natural course—The GINIplus study up to the age of 6 years. Clin. Exp. Allergy 2010, 40, 627–636. [Google Scholar] [CrossRef]
- Von Berg, A.; Filipiak-Pittroff, B.; Schulz, H.; Hoffmann, U.; Link, E.; Sußmann, M.; Schnappinger, M.; Brüske, I.; Standl, M.; Krämer, U.; et al. Allergic manifestation 15 years after early intervention with hydrolyzed formulas--the GINI Study. Allergy 2016, 71, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, J.; Brüske, I.; Cramer, C.; Hoffmann, U.; Schnappinger, M.; Schaaf, B.; von Berg, A.; Berdel, D.; Krämer, U.; Lehmann, I.; et al. GINIplus and LISAplus—Design and selected results of two German birth cohorts about natural course of atopic diseases and their determinants. Allergol. Sel. 2017, 1, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Von Berg, A.; Koletzko, S.; Grübl, A.; Filipiak-Pittroff, B.; Wichmann, H.-E.; Bauer, C.P.; Reinhardt, D.; Berdel, D. The effect of hydrolyzed cow’s milk formula for allergy prevention in the first year of life: The German Infant Nutritional Intervention Study, a randomized double-blind trial. J. Allergy Clin. Immunol. 2003, 111, 533–540. [Google Scholar] [CrossRef]
- Kleinbaum, D.G. Epidemiologic Research: Principles and Quantitative Methods; John Wiley & Sons: Hoboken, NJ, USA, 1982; ISBN 047128985X. [Google Scholar]
- Diggle, P. Analysis of Longitudinal Data, 2nd ed.; Oxford University Press: Oxford, UK, 2002; ISBN 0191664324. [Google Scholar]
- Kilanowski, A.; Thiering, E.; Wang, G.; Kumar, A.; Kress, S.; Flexeder, C.; Bauer, C.-P.; Berdel, D.; von Berg, A.; Bergström, A.; et al. Allergic disease trajectories up to adolescence: Characteristics, early-life, and genetic determinants. Allergy 2022, 78, 836–850. [Google Scholar] [CrossRef]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention 2022. Available online: https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf (accessed on 14 December 2022).
- Chen, C.-N.; Lin, Y.-C.; Ho, S.-R.; Fu, C.-M.; Chou, A.-K.; Yang, Y.-H. Association of Exclusive Breastfeeding with Asthma Risk among Preschool Children: An Analysis of National Health and Nutrition Examination Survey Data, 1999 to 2014. Nutrients 2022, 14, 4250. [Google Scholar] [CrossRef]
- Hou, W.; Guan, F.; Xia, L.; Xu, Y.; Huang, S.; Zeng, P. Investigating the influence of breastfeeding on asthma in children under 12 years old in the UK Biobank. Front. Immunol. 2022, 13, 967101. [Google Scholar] [CrossRef]
- Paramasivam, K.; Michie, C.; Opara, E.; Jewell, A.P. Human breast milk immunology: A review. Int. J. Fertil. Womens. Med. 2006, 51, 208–217. [Google Scholar]
- Flohr, C.; Henderson, A.J.; Kramer, M.S.; Patel, R.; Thompson, J.; Rifas-Shiman, S.L.; Yang, S.; Vilchuck, K.; Bogdanovich, N.; Hameza, M.; et al. Effect of an Intervention to Promote Breastfeeding on Asthma, Lung Function, and Atopic Eczema at Age 16 Years: Follow-up of the PROBIT Randomized Trial. JAMA Pediatr. 2018, 172, e174064. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Apfelbacher, C.; Chen, C.-M.; Romanos, M.; Sausenthaler, S.; Koletzko, S.; Bauer, C.-P.; Hoffmann, U.; Krämer, U.; Berdel, D.; et al. Infant-onset eczema in relation to mental health problems at age 10 years: Results from a prospective birth cohort study (German Infant Nutrition Intervention plus). J. Allergy Clin. Immunol. 2010, 125, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.J.; Carlin, J.B.; Bennett, C.M.; Abramson, M.J.; Hosking, C.S.; Hill, D.J.; Dharmage, S.C. Atopic disease and breast-feeding--cause or consequence? J. Allergy Clin. Immunol. 2006, 117, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Dulon, M.; Kersting, M.; Schach, S. Duration of breastfeeding and associated factors in Western and Eastern Germany. Acta Paediatr. 2001, 90, 931–935. [Google Scholar] [CrossRef] [PubMed]


| Intervention Cohort | Non-Intervention Cohort FH+ | Non-Intervention Cohort FH− | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Early Eczema − | Early Eczema + | Early Eczema − | Early Eczema + | Early Eczema − | Early Eczema + | |||||
| N = 1208 | N = 453 | Chi2 test | N = 597 | N = 207 | Chi2 test | N = 1353 | N = 240 | Chi2 test | ||
| n (%) | n (%) | p-value | n (%) | n (%) | p-value | n (%) | n (%) | p-value | ||
| Family history of allergy | no | 0 | 0 | 0 | 0 | 1353 (100) | 240 (100) | - | ||
| single | 846 (70.0) | 291 (64.2) | 0.024 | 503 (84.3) | 159 (76.8) | 0.016 | ||||
| double | 362 (30.0) | 162 (35.8) | 94 (15.7) | 48 (23.2) | ||||||
| Family risk for | eczema | 419 (34.7) | 249 (55.0) | <0.001 | 155 (26.0) | 96 (46.4) | <0.001 | - | - | |
| asthma | 329 (27.2) | 141 (31.1) | 0.117 | 108 (18.1) | 40 (19.3) | 0.693 | - | - | ||
| AR | 1033 (85.5) | 370 (81.7) | 0.055 | 453 (75.9) | 154 (74.4) | 0.669 | - | - | ||
| Sex | male | 615 (50.9) | 244 (53.9) | 0.284 | 294 (49.2) | 114 (55.1) | 0.149 | 687 (50.8) | 119 (49.6) | 0.733 |
| Study region | Munich | 635 (52.6) | 239 (52.8) | 0.944 | 364 (61.0) | 122 (58.9) | 0.606 | 469 (34.7) | 104 (43.3) | 0.010 |
| Siblings # | 0 | 719 (59.5) | 252 (55.6) | 0.246 | 262 (43.9) | 78 (37.7) | 0.256 | 675 (49.9) | 141 (58.8) | 0.037 |
| 1 | 373 (30.9) | 145 (32.0) | 241 (40.4) | 96 (46.4) | 520 (38.4) | 78 (32.5) | ||||
| >1 | 113 (9.4) | 53 (11.7)) | 94 (15.7) | 33 (15.9) | 158 (11.7) | 21 (8.8) | ||||
| Parental education # | low (<10 years) | 76 (6.3) | 28 (6.2) | 0.707 | 59 (9.9) | 19 (9.2) | 0.923 | 176 (13.0) | 34 (14.2) | 0.641 |
| middle (10–12 years) | 328 (27.2) | 132 (29.1) | 166 (27.8) | 60 (29.0) | 462 (34.1) | 74 (30.8) | ||||
| high (>12 years) | 804 (66.6) | 292 (64.5) | 372 (62.3) | 128 (61.8) | 714 (52.8) | 129 (53.8) | ||||
| Full breastfeeding for 4 months # | 533 (44.1) | 200 (44.2) | 0.992 | 302 (51.5) | 102 (49.5) | 0.618 | 633 (47.5) | 116 (50.0) | 0.479 | |
| Prevalence eczema | |||||||||
| 5 to 6th Year | 7 to 10th Year | 11 to 15th Year | 16 to 20th Year | ||||||
| Intervention | OR | 9.5 | (6.9–13.2) | 5.3 | (3.6–7.8) | 5.5 | (3.6–6.6) | 3.6 | (2.3–5.8) |
| aOR b | 8.7 | (6.2–12.2) | 5.0 | (3.4–7.6) | 5.0 | (3.2–7.9) | 3.4 | (2.1–5.5) | |
| Non-intervention FH+ | OR | 8.5 | (5.2–13.7) | 4.8 | (2.8–8.2) | 4.6 | (2.6–8.1) | 2.9 | (1.3–6.5) |
| aOR b | 8.1 | (4.9–13.4) | 4.4 | (2.5–7.6) | 4.1 | (2.2–7.4) | 2.4 | (1.0–5.6) | |
| Non-intervention FH− | OR | 14.6 | (9.4–22.6) | 7.4 | (4.3–12.8) | 8.3 | (4.1–16.9) | 4.0 | (2.2–7.5) |
| aOR c | 14.7 | (9.5–22.8) | 7.4 | (4.2–12.9) | 8.2 | (4.0–16.9) | 4.7 | (2.4–9.1) | |
| Prevalence asthma | |||||||||
| 5 to 6th year | 7 to 10th year | 11 to 15th year | 16 to 20th year | ||||||
| Intervention | OR | 2.3 | (1.3–4.0) | 2.7 | (1.8–4.1) | 2.5 | (1.6–3.7) | 1.6 | (1.0–2.7) |
| aOR b | 2.1 | (1.2–3.8) | 2.6 | (1.7–4.0) | 2.4 | (1.6–3.6) | 1.6 | (0.95–2.7) | |
| Non-intervention FH+ | OR | 7.4 | (2.8–19.8) | 2.6 | (1.4–5.1) | 2.4 | (1.3–4.5) | 2.2 | (0.93–5.4) |
| aOR b | 6.8 | (2.5–18.6) | 2.5 | (1.3–5.0) | 2.2 | (1.2–4.3) | 1.9 | (0.78–4.8) | |
| Non-intervention FH− | OR | 3.0 | (1.2–7.6) | 3.0 | (1.5–6.1) | 2.0 | (1.1–3.9) | 2.0 | (0.87–4.5) |
| aOR c | 2.9 | (1.1–7.3) | 3.2 | (1.5–6.5) | 2.1 | (1.1–4.1) | 2.1 | (0.89–4.7) | |
| Prevalence allergic rhinitis/hay fewer | |||||||||
| 5 to 6th year | 7 to 10th year | 11 to 15th year | 16 to 20th year | ||||||
| Intervention | OR | 2.2 | (1.5–3.2) | 2.5 | (1.9–3.4) | 2.1 | (1.6–2.8) | 1.8 | (1.3–2.4) |
| aOR b | 2.2 | (1.5–3.1) | 2.6 | (1.9–3.5) | 2.1 | (1.6–2.8) | 1.7 | (1.2–2.4) | |
| Non-intervention FH+ | OR | 2.7 | (1.5–4.8) | 2.5 | (1.6–4.0) | 2.9 | (1.9–4.4) | 2.6 | (1.6–4.3) |
| aOR b | 2.8 | (1.5–5.0) | 2.4 | (1.6–3.9) | 2.9 | (1.9–4.4) | 2.6 | (1.6–4.3) | |
| Non-intervention FH− | OR | 2.0 | (0.89–4.5) | 1.9 | (1.1–3.2) | 1.9 | (1.2–3.1) | 2.2 | (1.4–3.6) |
| aOR c | 2.0 | (0.87–4.5) | 1.9 | (1.1–3.2) | 2.0 | (1.2–3.1) | 2.1 | (1.3–3.4) | |
| Prevalence allergic diseases (Eczema, asthma or rhinitis/hay fewer) | |||||||||
| 5 to 6th year | 7 to 10th year | 11 to 15th year | 16 to 20th year | ||||||
| Intervention | OR | 5.1 | (3.9–6.7) | 3.3 | (2.5–4.3) | 2.6 | (2.0–3.4) | 2.1 | (1.6–2.9) |
| aOR b | 5.0 | (3.8–6.6) | 3.4 | (2.5–4.5) | 2.6 | (2.0–3.5) | 2.1 | (1.5–2.8) | |
| Non-intervention FH+ | OR | 5.7 | (3.8–8.5) | 3.1 | (2.1–4.6) | 3.3 | (2.2–4.9) | 2.6 | (1.6–4.1) |
| aOR b | 5.6 | (3.6–8.6) | 3.1 | (2.1–4.7) | 3.2 | (2.1–4.9) | 2.5 | (1.6–4.1) | |
| Non-intervention FH− | OR | 9.2 | (6.3–13.4) | 3.7 | (2.5–5.4) | 2.8 | (1.9–4.1) | 2.3 | (1.5–3.5) |
| aOR c | 9.1 | (6.2–13.4) | 3.7 | (2.5–5.5) | 2.8 | (1.9–4.2) | 2.3 | (1.5–3.5) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Libuda, L.; Filipiak-Pittroff, B.; Standl, M.; Schikowski, T.; von Berg, A.; Koletzko, S.; Bauer, C.-P.; Heinrich, J.; Berdel, D.; Gappa, M. Full Breastfeeding and Allergic Diseases—Long-Term Protection or Rebound Effects? Nutrients 2023, 15, 2780. https://doi.org/10.3390/nu15122780
Libuda L, Filipiak-Pittroff B, Standl M, Schikowski T, von Berg A, Koletzko S, Bauer C-P, Heinrich J, Berdel D, Gappa M. Full Breastfeeding and Allergic Diseases—Long-Term Protection or Rebound Effects? Nutrients. 2023; 15(12):2780. https://doi.org/10.3390/nu15122780
Chicago/Turabian StyleLibuda, Lars, Birgit Filipiak-Pittroff, Marie Standl, Tamara Schikowski, Andrea von Berg, Sibylle Koletzko, Carl-Peter Bauer, Joachim Heinrich, Dietrich Berdel, and Monika Gappa. 2023. "Full Breastfeeding and Allergic Diseases—Long-Term Protection or Rebound Effects?" Nutrients 15, no. 12: 2780. https://doi.org/10.3390/nu15122780
APA StyleLibuda, L., Filipiak-Pittroff, B., Standl, M., Schikowski, T., von Berg, A., Koletzko, S., Bauer, C.-P., Heinrich, J., Berdel, D., & Gappa, M. (2023). Full Breastfeeding and Allergic Diseases—Long-Term Protection or Rebound Effects? Nutrients, 15(12), 2780. https://doi.org/10.3390/nu15122780