

Sociodemographic and Health Correlates of Multiple Health Behavior Adherence among Cancer Survivors: A Latent Class Analysis

 ,
,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Subpopulation Characteristics
2.3.2. Current Health Behaviors
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Differences in Health Behaviors by Latent Class Membership
3.3. Lower-Risk Lifestyle
3.4. Moderate-Risk Lifestyle
3.5. High-Risk Lifestyle
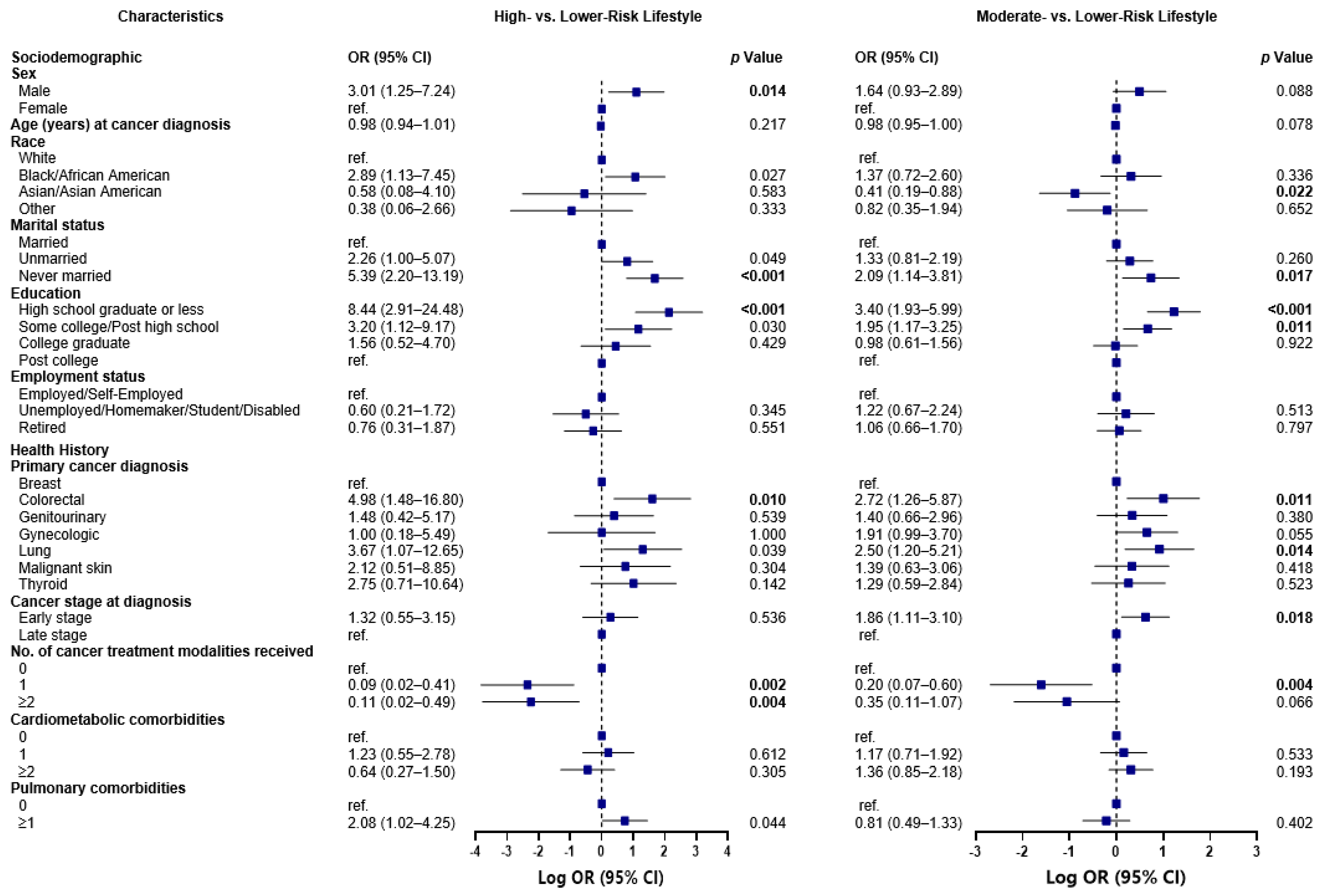
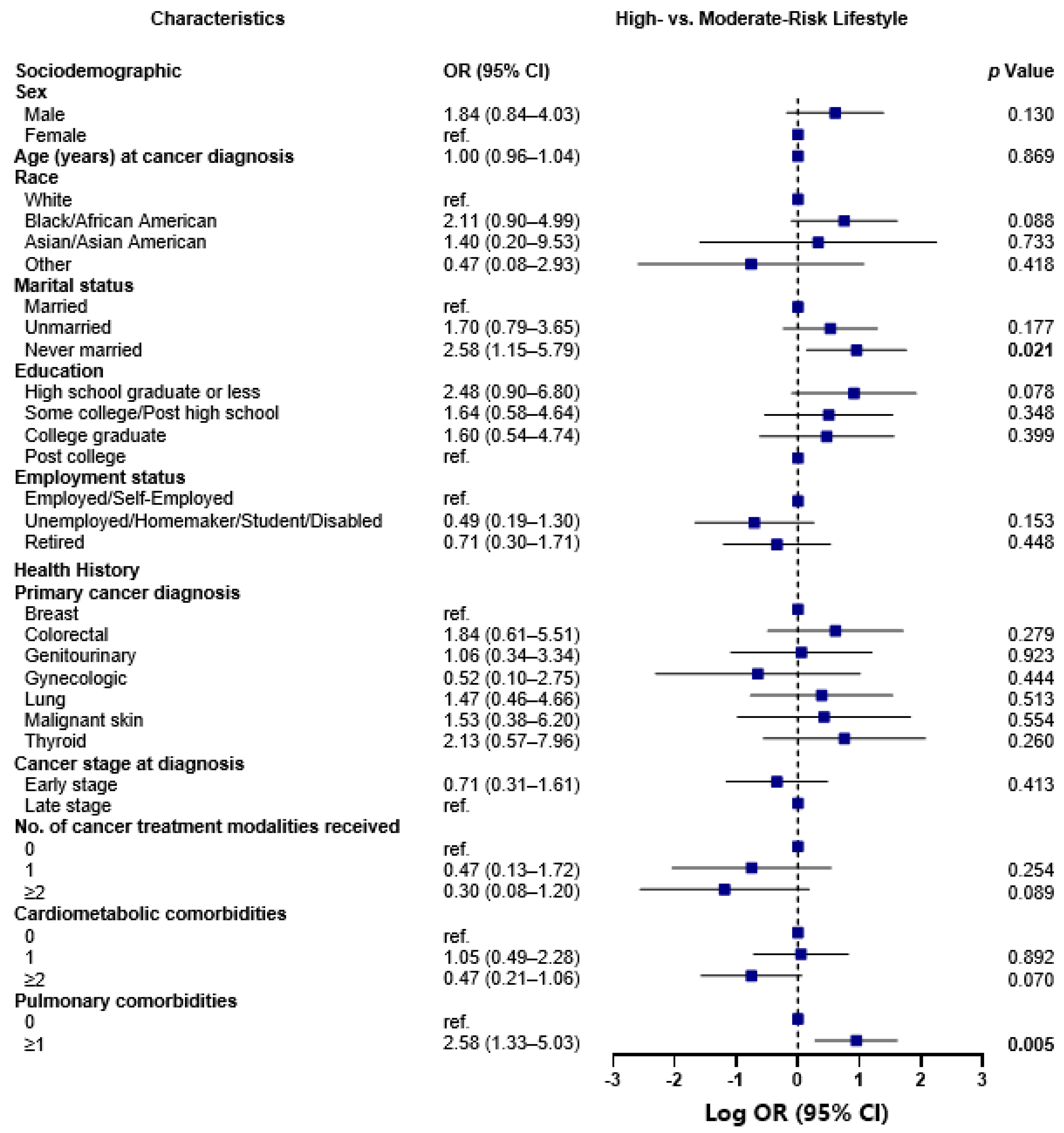
3.6. Sociodemographic and Health History Characteristics of Latent Classes
High-Risk versus Lower-Risk Lifestyle Class Comparison
3.7. Moderate-Risk versus Lower-Risk Lifestyle Class Comparison
3.8. High-Risk vs. Moderate-Risk Lifestyle Class Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Bluethmann, S.M.; Mariotto, A.B.; Rowland, J.H. Anticipating the “Silver Tsunami”: Prevalence Trajectories and Comorbidity Burden among Older Cancer Survivors in the United States. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1029–1036. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and psychological long-term and late effects of cancer. Cancer 2008, 112, 2577–2592. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Vallepu, S.; Barrios, C.; Hunter, K. Comparison of Comorbid Conditions Between Cancer Survivors and Age-Matched Patients Without Cancer. J. Clin. Med. Res. 2018, 10, 911–919. [Google Scholar] [CrossRef]
- Ogle, K.S.; Swanson, G.M.; Woods, N.; Azzouz, F. Cancer and comorbidity: Redefining chronic diseases. Cancer 2000, 88, 653–663. [Google Scholar] [CrossRef]
- Zullig, L.L.; Sung, A.D.; Khouri, M.G.; Jazowski, S.; Shah, N.P.; Sitlinger, A.; Blalock, D.V.; Whitney, C.; Kikuchi, R.; Bosworth, H.B.; et al. Cardiometabolic Comorbidities in Cancer Survivors. JACC CardioOncology 2022, 4, 149–165. [Google Scholar] [CrossRef]
- Brown, B.W.; Brauner, C.; Minnotte, M.C. Noncancer deaths in white adult cancer patients. J. Natl. Cancer Inst. 1993, 85, 979–987. [Google Scholar] [CrossRef]
- Stull, V.B.; Snyder, D.C.; Demark-Wahnefried, W. Lifestyle interventions in cancer survivors: Designing programs that meet the needs of this vulnerable and growing population. J. Nutr. 2007, 137, 243s–248s. [Google Scholar] [CrossRef]
- Bandera, E.V.; Alfano, C.M.; Qin, B.; Kang, D.W.; Friel, C.P.; Dieli-Conwright, C.M. Harnessing Nutrition and Physical Activity for Breast Cancer Prevention and Control to Reduce Racial/Ethnic Cancer Health Disparities; American Society of Clinical Oncology Educational Book: Alexandria, VA, USA, 2021; Volume 41, pp. 1–17. [Google Scholar] [CrossRef]
- Calle, E.E.; Rodriguez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 2003, 348, 1625–1638. [Google Scholar] [CrossRef]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef]
- Bandera, E.V.; Qin, B.; Lin, Y.; Zeinomar, N.; Xu, B.; Chanumolu, D.; Llanos, A.A.M.; Omene, C.O.; Pawlish, K.S.; Ambrosone, C.B.; et al. Association of Body Mass Index, Central Obesity, and Body Composition With Mortality among Black Breast Cancer Survivors. JAMA Oncol. 2021, 7, 1186–1195. [Google Scholar] [CrossRef] [PubMed]
- Amireault, S.; Fong, A.J.; Sabiston, C.M. Promoting Healthy Eating and Physical Activity Behaviors: A Systematic Review of Multiple Health Behavior Change Interventions Among Cancer Survivors. Am. J. Lifestyle Med. 2018, 12, 184–199. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Guidelines for Patients: Survivorship Care for Healthy Living; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2020. [Google Scholar]
- Tollosa, D.N.; Tavener, M.; Hure, A.; James, E.L. Compliance with Multiple Health Behaviour Recommendations: A Cross-Sectional Comparison between Female Cancer Survivors and Those with no Cancer History. Int. J. Environ. Res. Public Health 2019, 16, 1345. [Google Scholar] [CrossRef]
- Li, Q.; Lesseur, C.; Neugut, A.I.; Santella, R.M.; Parada, H., Jr.; Teitelbaum, S.; Chen, J. The associations of healthy lifestyle index with breast cancer incidence and mortality in a population-based study. Breast Cancer 2022, 29, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Steptoe, A.; Wardle, J. Is a cancer diagnosis a trigger for health behaviour change? Findings from a prospective, population-based study. Br. J. Cancer 2013, 108, 2407–2412. [Google Scholar] [CrossRef] [PubMed]
- Nayak, P.; Holmes, H.M.; Nguyen, H.T.; Elting, L.S. Self-reported physical activity among middle-aged cancer survivors in the United States: Behavioral Risk Factor Surveillance System Survey, 2009. Prev. Chronic Dis. 2014, 11, E156. [Google Scholar] [CrossRef]
- LeMasters, T.J.; Madhavan, S.S.; Sambamoorthi, U.; Kurian, S. Health behaviors among breast, prostate, and colorectal cancer survivors: A US population-based case-control study, with comparisons by cancer type and gender. J. Cancer Surviv. 2014, 8, 336–348. [Google Scholar] [CrossRef]
- Lee, E.; Zhu, J.; Velazquez, J.; Bernardo, R.; Garcia, J.; Rovito, M.; Hines, R.B. Evaluation of Diet Quality Among American Adult Cancer Survivors: Results From 2005-2016 National Health and Nutrition Examination Survey. J. Acad. Nutr. Diet. 2021, 121, 217–232. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the crest of the teachable moment: Promoting long-term health after the diagnosis of cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef]
- Kim, J.; Keegan, T.H. Characterizing risky alcohol use, cigarette smoking, e-cigarette use, and physical inactivity among cancer survivors in the USA-a cross-sectional study. J. Cancer Surviv. 2022. [Google Scholar] [CrossRef]
- Park, J.H.; Lee, J.; Oh, M.; Park, H.; Chae, J.; Kim, D.I.; Lee, M.K.; Yoon, Y.J.; Lee, C.W.; Park, S.; et al. The effect of oncologists’ exercise recommendations on the level of exercise and quality of life in survivors of breast and colorectal cancer: A randomized controlled trial. Cancer 2015, 121, 2740–2748. [Google Scholar] [CrossRef] [PubMed]
- White, A.; Pollack, L.A.; Smith, J.L.; Thompson, T.; Underwood, J.M.; Fairley, T. Racial and ethnic differences in health status and health behavior among breast cancer survivors--Behavioral Risk Factor Surveillance System, 2009. J. Cancer Surviv. 2013, 7, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.E.; Kreps, G.L.; Hesse, B.W.; Croyle, R.T.; Willis, G.; Arora, N.K.; Rimer, B.K.; Viswanath, K.V.; Weinstein, N.; Alden, S. The Health Information National Trends Survey (HINTS): Development; Design, and Dissemination. J. Health Commun. 2004, 9, 443–460. [Google Scholar] [CrossRef] [PubMed]
- Godin, G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. Validation of the Godin-Shephard Leisure-Time Physical Activity Questionnaire classification coding system using accelerometer assessment among breast cancer survivors. J. Cancer Surviv. 2015, 9, 532–540. [Google Scholar] [CrossRef]
- National Cancer Institute. Follow-Up Care Use among Survivors (FOCUS) Survey; National Cancer Institute: Bethesda, MD, USA, 2020. [Google Scholar]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef]
- Thomson, C.A.; Giuliano, A.; Rock, C.L.; Ritenbaugh, C.K.; Flatt, S.W.; Faerber, S.; Newman, V.; Caan, B.; Graver, E.; Hartz, V.; et al. Measuring dietary change in a diet intervention trial: Comparing food frequency questionnaire and dietary recalls. Am. J. Epidemiol. 2003, 157, 754–762. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. Medical Expenditure Panel Survey; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2018. [Google Scholar]
- Hyland, K.A.; Jacobs, J.M.; Lennes, I.T.; Pirl, W.F.; Park, E.R. Are cancer survivors following the national comprehensive cancer network health behavior guidelines? An assessment of patients attending a cancer survivorship clinic. J. Psychosoc. Oncol. 2018, 36, 64–81. [Google Scholar] [CrossRef]
- Blanchard, C.M.; Courneya, K.S.; Stein, K.; American Cancer Society’s, S.C.S., II. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Greenlee, H.; Ogden Gaffney, A.; Aycinena, A.C.; Koch, P.; Contento, I.; Karmally, W.; Richardson, J.M.; Shi, Z.; Lim, E.; Tsai, W.Y.; et al. Long-term Diet and Biomarker Changes after a Short-term Intervention among Hispanic Breast Cancer Survivors: The inverted exclamation markCocinar Para Su Salud! Randomized Controlled Trial. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1491–1502. [Google Scholar] [CrossRef]
- Greenlee, H.; Gaffney, A.O.; Aycinena, A.C.; Koch, P.; Contento, I.; Karmally, W.; Richardson, J.M.; Lim, E.; Tsai, W.Y.; Crew, K.; et al. Inverted exclamation markCocinar Para Su Salud!: Randomized Controlled Trial of a Culturally Based Dietary Intervention among Hispanic Breast Cancer Survivors. J. Acad. Nutr. Diet. 2015, 115, 709–723 e703. [Google Scholar] [CrossRef] [PubMed]
- Tollosa, D.N.; Tavener, M.; Hure, A.; James, E.L. Adherence to multiple health behaviours in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2019, 13, 327–343. [Google Scholar] [CrossRef] [PubMed]
- Gorman, B.K.; Read, J.G. Gender disparities in adult health: An examination of three measures of morbidity. J. Health Soc. Behav. 2006, 47, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Asare, M.; Fakhoury, C.; Thompson, N.; Culakova, E.; Kleckner, A.S.; Adunlin, G.; Reifenstein, K.; Benavidez, G.A.; Kamen, C.S. The Patient-Provider Relationship: Predictors of black/African American Cancer Patients’ Perceived Quality of Care and Health Outcomes. Health Commun. 2020, 35, 1289–1294. [Google Scholar] [CrossRef]
- Springfield, S.; Odoms-Young, A.; Tussing-Humphreys, L.; Freels, S.; Stolley, M. Adherence to American Cancer Society and American Institute of Cancer Research dietary guidelines in overweight African American breast cancer survivors. J. Cancer Surviv. 2019, 13, 257–268. [Google Scholar] [CrossRef]
- Lim, J.W.; Paek, M.S. The relationship between communication and health-related quality of life in survivorship care for Chinese-American and Korean-American breast cancer survivors. Support. Care Cancer 2013, 21, 1157–1166. [Google Scholar] [CrossRef]
- Winkels, R.M.; van Lee, L.; Beijer, S.; Bours, M.J.; van Duijnhoven, F.J.; Geelen, A.; Hoedjes, M.; Mols, F.; de Vries, J.; Weijenberg, M.P.; et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research lifestyle recommendations in colorectal cancer survivors: Results of the PROFILES registry. Cancer Med. 2016, 5, 2587–2595. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Overall N (%) | Missing N (%) |
|---|---|---|
| Sociodemographic | ||
| Sex | 0 (0.0) | |
| Male | 273 (41.3) | |
| Female | 388 (58.7) | |
| Age (years) at cancer diagnosis, mean ± SD | 60.8 ± 10.5 | 0 (0.0) |
| Race | 0 (0.0) | |
| White | 518 (78.4) | |
| Black/African American | 75 (11.3) | |
| Asian/Asian American | 39 (5.9) | |
| Other a | 29 (4.4) | |
| Hispanic ethnicity | 0 (0.0) | |
| Yes | 39 (5.9) | |
| No | 622 (94.1) | |
| US-born | 2 (0.3) | |
| Yes | 569 (86.1) | |
| No | 88 (13.3) | |
| Prefer not to answer | 2 (0.3) | |
| Marital status | 2 (0.3) | |
| Married | 452 (68.4) | |
| Unmarried | 119 (18.0) | |
| Never married | 82 (12.4) | |
| Don’t know/Prefer not to answer | 6 (0.9) | |
| Education b | 4 (0.6) | |
| High school graduate or less | 149 (22.5) | |
| Some college/Post high school | 152 (23.0) | |
| College graduate | 201 (30.4) | |
| Post college | 150 (22.7) | |
| Other-unspecified/Don’t know/Prefer not to answer | 5 (0.8) | |
| Employment status | 12 (1.8) | |
| Employed/Self-Employed | 284 (43.0) | |
| Unemployed/Homemaker/Student/Disabled | 84 (12.7) | |
| Retired | 277 (41.9) | |
| Other-unspecified/Don’t know/Prefer not to answer | 4 (0.6) | |
| Annual household income | 11 (1.7) | |
| <$50,000 | 161 (24.4) | |
| $50,000–$89,999 | 151 (22.8) | |
| ≥$90,000 | 211 (31.9) | |
| Don’t know | 127 (19.2) | |
| Health insurance status at cancer diagnosis | 0 (0.0) | |
| Uninsured | 8 (1.2) | |
| Private | 312 (47.2) | |
| Public | 277 (41.9) | |
| Insured, not otherwise specified | 40 (6.1) | |
| Don’t know | 24 (3.6) | |
| Health History | ||
| Primary cancer diagnosis | 0 (0.0) | |
| Breast | 169 (25.6) | |
| Colorectal | 66 (10.0) | |
| Genitourinary c | 183 (27.7) | |
| Gynecologic d | 67 (10.1) | |
| Lung | 66 (10.0) | |
| Malignant skin | 66 (10.0) | |
| Thyroid | 44 (6.7) | |
| Cancer stage at diagnosis e | 0 (0.0) | |
| Early stage | 515 (77.9) | |
| Late stage | 137 (20.7) | |
| Unstaged | 9 (1.4) | |
| Time (years) since cancer diagnosis, mean ± SD | 3.2 ± 0.7 | 0 (0.0) |
| Cancer treatment type | ||
| Surgery | 15 (2.3) | |
| Yes | 545 (82.5) | |
| No | 100 (15.1) | |
| Do not recall | 1 (0.2) | |
| Chemotherapy | 62 (9.4) | |
| Yes | 179 (27.1) | |
| No | 418 (63.2) | |
| Do not recall | 2 (0.3) | |
| Radiotherapy | 43 (6.5) | |
| Yes | 258 (39.0) | |
| No | 359 (54.3) | |
| Do not recall | 1 (0.2) | |
| No. of cancer treatment modalities received | 53 (8.0) | |
| 0 | 27 (4.1) | |
| 1 | 307 (46.4) | |
| ≥2 | 274 (41.5) | |
| Cardiometabolic comorbidities f | 14 (2.1) | |
| 0 | 188 (28.4) | |
| 1 | 174 (26.3) | |
| ≥2 | 285 (43.1) | |
| Pulmonary comorbidities g | 12 (1.8) | |
| 0 | 529 (80.0) | |
| ≥1 | 120 (18.2) | |
| Other comorbidities h | 16 (2.4) | |
| 0 | 446 (67.5) | |
| ≥1 | 199 (30.1) |
| BMI and Health Behaviors | Overall N (%) | Health Behavior Class † | ||
|---|---|---|---|---|
| High-Risk Lifestyle A (%) | Moderate-Risk Lifestyle B (%) | Lower-Risk Lifestyle C (%) | ||
| Latent Class Membership | 661 (100.0) | 55 (8.3) | 344 (52.0) | 262 (39.6) |
| BMI (kg/m2) a | ||||
| <25.0 | 194 (29.3) | 11 (20.0) | 90 (26.2) | 93 (35.5) A,B |
| 25.0–29.9 | 240 (36.3) | 20 (36.4) | 120 (34.9) | 100 (38.2) |
| ≥30.0 | 227 (34.3) | 24 (43.6) C | 134 (39.0) C | 69 (26.3) |
| Physical activity | ||||
| Insufficiently active/sedentary (LSI < 14) | 214 (32.4) | 20 (36.4) C | 138 (40.1) C | 56 (21.4) |
| Moderately active (LSI = 14–23) | 129 (19.5) | 17 (30.9) C | 73 (21.2) | 39 (14.9) |
| Active (LSI ≥ 24) | 318 (48.1) | 18 (32.7) | 133 (38.7) | 167 (63.7) A,B |
| Smoking status | ||||
| Never smoker | 340 (51.4) | 17 (30.9) | 168 (48.8) A | 155 (59.2) A,B |
| Former smoker | 269 (40.7) | 25 (45.5) | 139 (40.4) | 105 (40.1) |
| Current smoker | 52 (7.9) | 13 (23.6) B,C | 37 (10.8) C | 2 (0.8) |
| Alcohol consumption | ||||
| 0 drinks/day | 239 (36.2) | 33 (60.0) B,C | 128 (37.2) | 78 (29.8) |
| 0 < drinks/day ≤ 1 | 197 (29.8) | 11 (20.0) | 101 (29.4) | 85 (32.4) |
| 1 < drinks/day ≤ 2 | 150 (22.7) | 8 (14.5) | 72 (20.9) | 70 (26.7) |
| >2 drinks/day | 75 (11.3) | 3 (5.5) | 43 (12.5) | 29 (11.1) |
| Healthy diet intake b | ||||
| More fruit, mean ± SD | 3.9 ± 1.5 | 3.3 ± 1.5 B | 3.0 ± 1.1 | 5.1 ± 0.9 A,B |
| More vegetables, mean ± SD | 4.3 ± 1.3 | 3.7 ± 1.4 B | 3.5 ± 1.0 | 5.4 ± 0.6 A,B |
| More whole grains, mean ± SD | 3.5 ± 1.4 | 3.6 ± 1.5 B | 2.8 ± 1.1 | 4.2 ± 1.4 A,B |
| Less sugar, mean ± SD | 5.4 ± 1.1 | 2.2 ± 0.8 | 5.5 ± 0.7 A | 5.8 ± 0.5 A,B |
| Less red meat, mean ± SD | 4.4 ± 1.0 | 3.7 ± 1.3 | 4.3 ± 0.8 A | 4.6 ± 1.0 A,B |
| Less processed meat, mean ± SD | 4.8 ± 0.9 | 4.1 ± 1.2 | 4.6 ± 0.9 A | 5.1 ± 0.9 A,B |
| Less fast foods, mean ± SD | 5.0 ± 0.8 | 4.5 ± 0.9 | 4.9 ± 0.8 A | 5.3 ± 0.6 A,B |
| Sun safety c | ||||
| Wearing sunscreen, mean ± SD | 3.0 ± 1.4 | 2.6 ± 1.5 | 2.8 ± 1.4 | 3.4 ± 1.3 A,B |
| Wearing shirt with sleeves covering shoulders, mean ± SD | 3.8 ± 1.2 | 3.8 ± 1.4 | 3.8 ± 1.2 | 3.8 ± 1.2 |
| Wearing a hat, mean ± SD | 3.0 ± 1.3 | 3.2 ± 1.3 | 2.8 ± 1.3 | 3.2 ± 1.3 B |
| Staying in the shade or under an umbrella, mean ± SD | 3.4 ± 1.0 | 3.2 ± 1.2 | 3.4 ± 1.0 | 3.4 ± 1.0 |
| Wearing sunglasses, mean ± SD | 3.9 ± 1.3 | 3.7 ± 1.4 | 3.7 ± 1.4 | 4.2 ± 1.1 A,B |
| Last physician visit | ||||
| <4 weeks ago | 150 (22.7) | 16 (29.1) | 75 (21.8) | 59 (22.5) |
| 1–3 months ago | 204 (30.9) | 17 (30.9) | 101 (29.4) | 86 (32.8) |
| 4–6 months ago | 176 (26.6) | 11 (20.0) | 93 (27.0) | 72 (27.5) |
| 7–12 months ago | 87 (13.2) | 4 (7.3) | 49 (14.2) | 34 (13.0) |
| >2 years ago | 44 (6.7) | 7 (12.7) C | 26 (7.6) | 11 (4.2) |
| NCCN Health Behavior Guidelines | Adherence Criteria | Overall N (%) | Health Behavior Class † | |||
|---|---|---|---|---|---|---|
| High-Risk Lifestyle A (%) | Moderate-Risk Lifestyle B (%) | Lower-Risk Lifestyle C (%) | ||||
| Latent Class Membership | 661 (100.0) | 55 (8.3) | 344 (52.0) | 262 (39.6) | ||
| BMI | Achieve and maintain a healthy body weight throughout life. | Adherent: Healthy weight (18.5–24.9 kg/m2) | 189 (28.6) | 10 (18.2%) | 87 (25.3%) | 92 (35.1%) A,B |
| Non-Adherent: Underweight (<18.5 kg/m2), Overweight (25.0–29.9 kg/m2), or Obese (≥30.0 kg/m2) | 472 (71.4) | 45 (81.8%) C | 257 (74.7%) C | 170 (64.9%) | ||
| Physical activity | Regularly exercise. Stay active. Aim for 150 min of moderate or 75 min of vigorous activity per week, spread out over the course of the week. Resistance train 2–3 times a week and stretch major muscles on at least two days of higher-intensity activity. | Adherent: Active (LSI≥24) | 318 (48.1) | 18 (32.7%) | 133 (38.7%) | 167 (63.7%) A,B |
| Non-Adherent: Insufficiently/Moderately active (LSI<24) | 343 (51.9) | 37 (67.3%) C | 211 (61.3%) C | 95 (36.3%) | ||
| Smoking status | Don’t smoke, chew, or sniff tobacco products. Attempt tobacco cessation if currently smoking or using smokeless tobacco. | Adherent: Not currently smoking | 609 (92.1) | 42 (76.4%) | 307 (89.2%) A | 260 (99.2%) A,B |
| Non-Adherent: Currently smoking | 52 (7.9) | 13 (23.6%) B,C | 37 (10.8%) C | 2 (0.8%) | ||
| Alcohol consumption | Limit or abstain from alcohol intake; limit intake to one drink/day for a woman and 2 drinks/day for a man. | Adherent: 1/day for females; 2/day for males | 504 (76.2) | 46 (83.6%) | 268 (77.9%) | 190 (72.5%) |
| Non-Adherent: >1/day for females; >2/day for males | 157 (23.8) | 9 (16.4%) | 76 (22.1%) | 72 (27.5%) | ||
| Healthy diet intake | Aim for at least half of your diet to be plant-based food. Plant-based food should be mostly vegetables, fruits, and whole grains. Half or less of your diet can be animal-based food—fish and poultry are healthy choices. Limit intake of red and processed meats. Avoid processed food. Drinks with lots of added sugars or fats should be consumed sparingly. | Adherent: Mean score >3 | 647 (97.9) | 45 (81.8%) | 340 (98.8%)A | 262 (100.0%) * |
| Non-Adherent: Mean score ≤3 | 14 (2.1) | 10 (18.2%) B | 4 (1.2%) | 0 (0.0%) * | ||
| Sun safety | Practice sun safety. Use water-resistant, UVA/UVB-protecting sunscreen with at least 30 SPF. Apply generously and reapply every 2 h or after swimming/excessive sweating. If possible, consider physical barriers (i.e., hats, shirts with sleeves, avoiding direct sun during peak hours). | Adherent: Mean score >3 | 465 (70.3) | 35 (63.6%) | 221 (64.2%) | 209 (79.8%) A,B |
| Non-Adherent: Mean score ≤3 | 196 (29.7) | 20 (36.4%)C | 123 (35.8%)C | 53 (20.2%) | ||
| Last physician visit | Follow up with primary care physician regularly. | Adherent: <4 weeks ago to 12 months ago | 617 (93.3) | 48 (87.3%) | 318 (92.4%) | 251 (95.8%)A |
| Non-Adherent: >2 years ago | 44 (6.7) | 7 (12.7%)C | 26 (7.6%) | 11 (4.2%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, A.J.; Llanos, A.A.M.; Ashrafi, A.; Zeinomar, N.; Chokshi, S.; Bandera, E.V.; Devine, K.A.; Hudson, S.V.; Qin, B.; O’Malley, D.; et al. Sociodemographic and Health Correlates of Multiple Health Behavior Adherence among Cancer Survivors: A Latent Class Analysis. Nutrients 2023, 15, 2354. https://doi.org/10.3390/nu15102354
Fong AJ, Llanos AAM, Ashrafi A, Zeinomar N, Chokshi S, Bandera EV, Devine KA, Hudson SV, Qin B, O’Malley D, et al. Sociodemographic and Health Correlates of Multiple Health Behavior Adherence among Cancer Survivors: A Latent Class Analysis. Nutrients. 2023; 15(10):2354. https://doi.org/10.3390/nu15102354
Chicago/Turabian StyleFong, Angela J., Adana A. M. Llanos, Adiba Ashrafi, Nur Zeinomar, Sagar Chokshi, Elisa V. Bandera, Katie A. Devine, Shawna V. Hudson, Bo Qin, Denalee O’Malley, and et al. 2023. "Sociodemographic and Health Correlates of Multiple Health Behavior Adherence among Cancer Survivors: A Latent Class Analysis" Nutrients 15, no. 10: 2354. https://doi.org/10.3390/nu15102354
APA StyleFong, A. J., Llanos, A. A. M., Ashrafi, A., Zeinomar, N., Chokshi, S., Bandera, E. V., Devine, K. A., Hudson, S. V., Qin, B., O’Malley, D., Paddock, L. E., Stroup, A. M., Evens, A. M., & Manne, S. L. (2023). Sociodemographic and Health Correlates of Multiple Health Behavior Adherence among Cancer Survivors: A Latent Class Analysis. Nutrients, 15(10), 2354. https://doi.org/10.3390/nu15102354