

Assessment of the Adherence to ESPGHAN 2018 Guidelines in the Neonatal Intensive Care Unit of the Ghent University Hospital: A Retrospective Study
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Patient Population, and Data Collection
2.2. Nutrition Protocol
2.3. Variables and Data Management
first day of PN)/time of PN (in weeks)
2.4. Bias and Study Size
2.5. Statistical Methods
3. Results
3.1. Patient Demographics
3.2. Reason for PN Initiation
3.3. Weekly Changes in Z-Scores
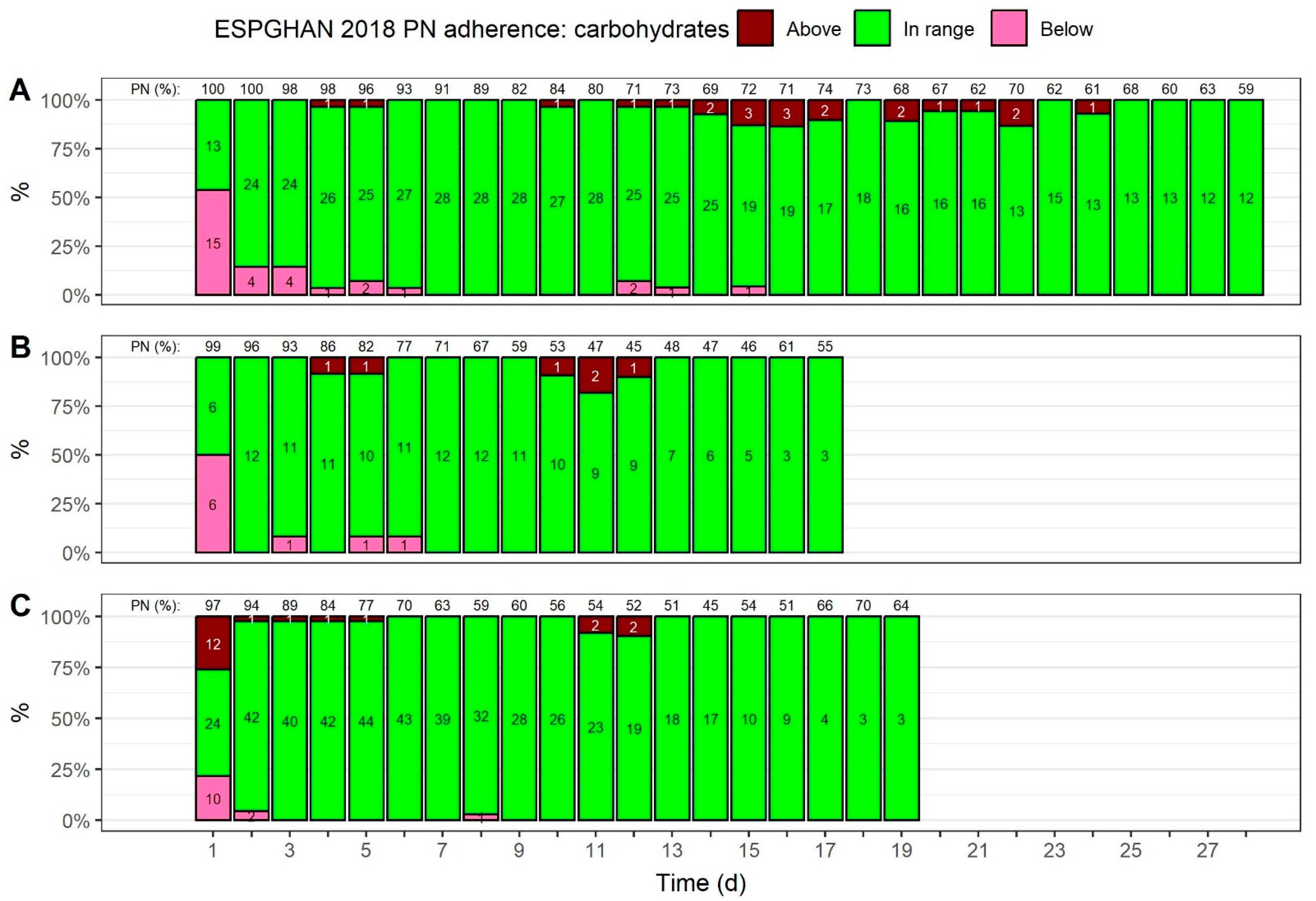
3.4. Carbohydrate Provision
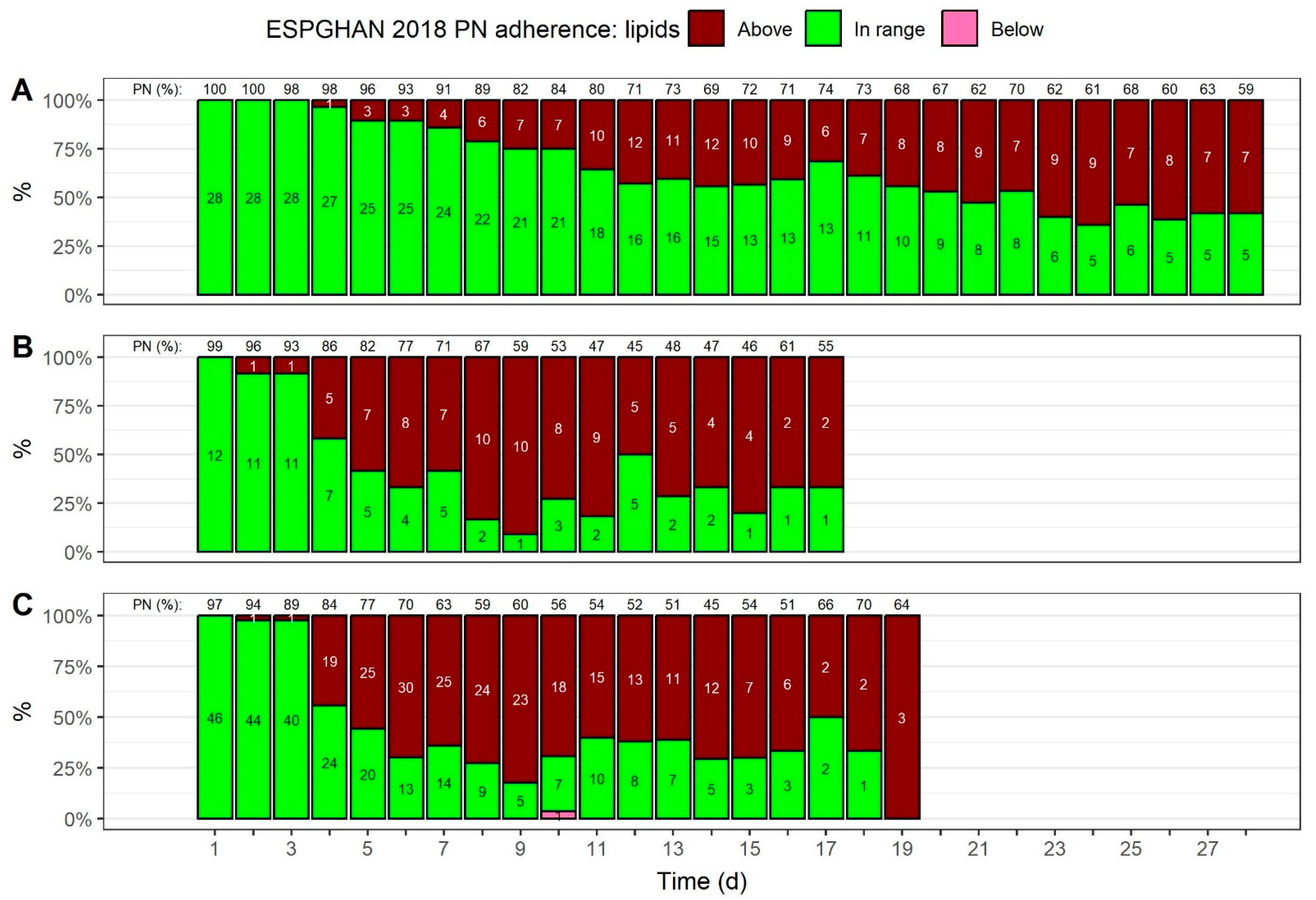
3.5. Lipid Provision
3.6. Amino Acid Provision
3.7. Energy Provision
3.8. Volume Percentage of PN Regarding Nutrient Provisions over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; van Look, P.F.A. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef]
- Zeitlin, J.; Szamotulska, K.; Drewniak, N.; Mohangoo, A.D.; Chalmers, J.; Sakkeus, L.; Irgens, L.; Gatt, M.; Gissler, M.; Blondel, B. Preterm birth time trends in Europe: A study of 19 countries. BJOG 2013, 120, 1356–1365. [Google Scholar] [CrossRef]
- dit Trolli, S.E.; Kermorvant-Duchemin, E.; Huon, C.; Bremond-Gignac, D.; Lapillonne, A. Early lipid supply and neurological development at one year in very low birth weight (VLBW) preterm infants. Early Hum. Dev. 2012, 88 (Suppl. S1), S25–S29. [Google Scholar] [CrossRef]
- Cleminson, J.S.; Zalewski, S.P.; Embleton, N.D. Nutrition in the preterm infant: What’s new? Curr. Opin. Clin Nutr. Metab. Care 2016, 19, 220–225. [Google Scholar]
- Al-Jebawi, Y.; Agarwal, N.; Groh Wargo, S.; Shekhawat, P.; Mhanna, M.J. Low caloric intake and high fluid intake during the first week of life are associated with the severity of bronchopulmonary dysplasia in extremely low birth weight infants. J. Neonatal. Perinat. Med. 2020, 13, 207–214. [Google Scholar] [CrossRef]
- Lapillonne, A.; Carnielli, V.P.; Embleton, N.D.; Mihatsch, W. Quality of newborn care: Adherence to guidelines for parenteral nutrition in preterm infants in four European countries. BMJ Open 2013, 3, e003478. [Google Scholar] [CrossRef]
- Klevebro, S.; Westin, V.; Stoltz Sjöström, E.; Norman, M.; Domellöf, M.; Edstedt Bonamy, A.-K.; Hallberg, B. Early energy and protein intakes and associations with growth, BPD, and ROP in extremely preterm infants. Clin. Nutr. 2019, 38, 1289–1295. [Google Scholar] [CrossRef]
- Ng, D.V.Y.; Unger, S.; Asbury, M.; Kiss, A.; Bishara, R.; Bando, N.; Tomlinson, C.; Gibbins, S.; O’Connor, D.L. Neonatal Morbidity Count Is Associated with a Reduced Likelihood of Achieving Recommendations for Protein, Lipid, and Energy in Very Low Birth Weight Infants: A Prospective Cohort Study. J. Parenter. Enter. Nutr. 2018, 42, 623–632. [Google Scholar] [CrossRef]
- Martínez-Jiménez, M.D.; Gómez-García, F.J.; Gil-Campos, M.; Pérez-Navero, J.L. Comorbidities in childhood associated with extrauterine growth restriction in preterm infants: A scoping review. Eur. J. Pediatr. 2020, 179, 1255–1265. [Google Scholar] [CrossRef]
- Puntis, J.; Hojsak, I.; Ksiazyk, J. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Organisational aspects. Clin. Nutr. 2018, 37, 2392–2400. [Google Scholar] [CrossRef]
- Colomb, V. Commercially premixed 3-chamber bags for pediatric parenteral nutrition are available for hospitalized children. J. Nutr. 2013, 143, 2071S–2076S. [Google Scholar] [CrossRef]
- Embleton, N.D.; Simmer, K. Practice of parenteral nutrition in VLBW and ELBW infants. World Rev. Nutr. Diet. 2014, 110, 177–189. [Google Scholar] [CrossRef]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef]
- Mesotten, D.; Joosten, K.; van Kempen, A.; Verbruggen, S. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Carbohydrates. Clin. Nutr. 2018, 37, 2337–2343. [Google Scholar] [CrossRef]
- Lapillonne, A.; Fidler Mis, N.; Goulet, O.; van den Akker, C.H.P.; Wu, J.; Koletzko, B. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clin. Nutr. 2018, 37, 2324–2336. [Google Scholar] [CrossRef]
- van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; Sainz de Pipaon, M. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef]
- Johnson, M.J.; Lapillonne, A.; Bronsky, J.; Domellof, M.; Embleton, N.; Iacobelli, S.; Jochum, F.; Joosten, K.; Kolacek, S.; Mihatsch, W.A.; et al. Research priorities in pediatric parenteral nutrition: A consensus and perspective from ESPGHAN/ESPEN/ESPR/CSPEN. Pediatr. Res. 2022, 92, 61–70. [Google Scholar] [CrossRef]
- Embleton, N.D.; Moltu, S.J.; Lapillonne, A.; van den Akker, C.H.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and invited experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef]
- Iacobelli, S.; Viaud, M.; Lapillonne, A.; Robillard, P.-Y.; Gouyon, J.-B.; Bonsante, F. Nutrition practice, compliance to guidelines and postnatal growth in moderately premature babies: The NUTRIQUAL French survey. BMC Pediatr. 2015, 15, 110. [Google Scholar] [CrossRef]
- Xiang, Y.; Tang, Q.; Wang, Y.; Cai, W. Nutrition profile of very low birth weight infants with extrauterine growth restriction in NICU. Clin. Nutr. ESPEN 2021, 42, 252–257. [Google Scholar] [CrossRef]
- Moltu, S.J.; Bronsky, J.; Embleton, N.; Gerasimidis, K.; Indrio, F.; Köglmeier, J.; de Koning, B.; Lapillonne, A.; Norsa, L.; Verduci, E.; et al. Nutritional Management of the Critically Ill Neonate: A Position Paper of the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2021, 73, 274–289. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, V.; Capozza, M.; Panza, R.; Laforgia, N.; Baldassarre, M.E. Macronutrients and Micronutrients in Parenteral Nutrition for Preterm Newborns: A Narrative Review. Nutrients 2022, 14, 1530. [Google Scholar] [CrossRef] [PubMed]
- Riskin, A.; Picaud, J.-C.; Shamir, R. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Standard versus individualized parenteral nutrition. Clin. Nutr. 2018, 37, 2409–2417. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R. 1. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 41 (Suppl. S2), S1–S87. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Chou, J.H.; Roumiantsev, S.; Singh, R. PediTools Electronic Growth Chart Calculators: Applications in Clinical Care, Research, and Quality Improvement. J. Med. Internet Res. 2020, 22, e16204. [Google Scholar] [CrossRef]
- Boscarino, G.; Conti, M.G.; Gasparini, C.; Onestà, E.; Faccioli, F.; Dito, L.; Regoli, D.; Spalice, A.; Parisi, P.; Terrin, G. Neonatal Hyperglycemia Related to Parenteral Nutrition Affects Long-Term Neurodevelopment in Preterm Newborn: A Prospective Cohort Study. Nutrients 2021, 13, 1930. [Google Scholar] [CrossRef]
- Izquierdo Renau, M.; Aldecoa-Bilbao, V.; Balcells Esponera, C.; Del Rey Hurtado de Mendoza, B.; Iriondo Sanz, M.; Iglesias-Platas, I. Applying Methods for Postnatal Growth Assessment in the Clinical Setting: Evaluation in a Longitudinal Cohort of Very Preterm Infants. Nutrients 2019, 11, 2772. [Google Scholar] [CrossRef]
- Westin, V.; Klevebro, S.; Domellöf, M.; Vanpée, M.; Hallberg, B.; Stoltz Sjöström, E. Improved nutrition for extremely preterm infants—A population based observational study. Clin. Nutr. ESPEN 2018, 23, 245–251. [Google Scholar] [CrossRef]
- Khan, Z.; Morris, N.; Unterrainer, H.; Haiden, N.; Holasek, S.J.; Urlesberger, B. Effect of standardized feeding protocol on nutrient supply and postnatal growth of preterm infants: A prospective study. J. Neonatal Perinat. Med. 2018, 11, 11–19. [Google Scholar] [CrossRef]
- Embleton, N.E.; Pang, N.; Cooke, R.J. Postnatal malnutrition and growth retardation: An inevitable consequence of current recommendations in preterm infants? Pediatrics 2001, 107, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Asbury, M.R.; Unger, S.; Kiss, A.; Ng, D.V.Y.; Luk, Y.; Bando, N.; Bishara, R.; Tomlinson, C.; O’Connor, D.L. Optimizing the growth of very-low-birth-weight infants requires targeting both nutritional and nonnutritional modifiable factors specific to stage of hospitalization. Am. J. Clin. Nutr. 2019, 110, 1384–1394. [Google Scholar] [CrossRef] [PubMed]
- Giretti, I.; D’Ascenzo, R.; Correani, A.; Antognoli, L.; Monachesi, C.; Biagetti, C.; Pompilio, A.; Marinelli, L.; Burattini, I.; Cogo, P.; et al. Hypertriglyceridemia and lipid tolerance in preterm infants with a birth weight of less than 1250 g on routine parenteral nutrition. Clin. Nutr. 2021, 40, 4444–4448. [Google Scholar] [CrossRef] [PubMed]
- Kilicbay, F.; Keskin, A.; Gunlemez, A. Effects of Fish Oil (SMOFlipid®) and Olive Oil Lipid (ClinOleic®) on Neonatal Morbidities in Preterm Infants. Medeni. Med. J. 2022, 37, 240–247. [Google Scholar] [CrossRef]
- Peila, C.; Spada, E.; Giuliani, F.; Maiocco, G.; Raia, M.; Cresi, F.; Bertino, E.; Coscia, A. Extrauterine Growth Restriction: Definitions and Predictability of Outcomes in a Cohort of Very Low Birth Weight Infants or Preterm Neonates. Nutrients 2020, 12, 1224. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Shen, W.; Wu, F.; Mao, J.; Liu, L.; Chang, Y.-M.; Zhang, R.; Ye, X.-Z.; Qiu, Y.-P.; Ma, L.; et al. Factors influencing extrauterine growth retardation in singleton-non-small for gestational age infants in China: A prospective multicenter study. Pediatr. Neonatol. 2022, 63, 590–598. [Google Scholar] [CrossRef]
- Cao, W.; Zhang, Y.-H.; Zhao, D.-Y.; Xia, H.-P.; Zhu, T.-W.; Xie, L.-J. Risk factors for extrauterine growth restriction in preterm infants with gestational age less than 34 weeks. Zhongguo Dang Dai Er Ke Za Zhi 2015, 17, 453–458. [Google Scholar]
- Radmacher, P.G.; Looney, S.W.; Rafail, S.T.; Adamkin, D.H. Prediction of extrauterine growth retardation (EUGR) in VVLBW infants. J. Perinatol. 2003, 23, 392–395. [Google Scholar] [CrossRef]
- Stevens, T.P.; Shields, E.; Campbell, D.; Combs, A.; Horgan, M.; La Gamma, E.F.; Xiong, K.; Kacica, M. Variation in Enteral Feeding Practices and Growth Outcomes among Very Premature Infants: A Report from the New York State Perinatal Quality Collaborative. Am. J. Perinatol. 2016, 33, 9–19. [Google Scholar] [CrossRef]
- Immeli, L.; Sankilampi, U.; Mäkelä, P.M.; Leskinen, M.; Sund, R.; Andersson, S.; Luukkainen, P. Length of Nutritional Transition Associates Negatively with Postnatal Growth in Very Low Birthweight Infants. Nutrients 2021, 13, 3961. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gestational Age | Nutrient | Minimum Day 1 | Maximum Day 1 | Minimum Day 2+ | Maximum Day 2+ |
|---|---|---|---|---|---|
| <37 weeks | Carbohydrates (g/kg/d) | 5.8 | 11.5 | 5.8 | 17.3 |
| Lipids (g/kg/d) | - | - | 1.0 | 4 | |
| Amino acids (g/kg/d) | 1.5 | 2.5 | 2.5 | 3.5 | |
| Non-protein energy (kcal/kg/d) | - | - | >65 | >65 | |
| Energy (kcal/kg/d) | 45.0 | 55.0 | 90.0 | 120 | |
| ≥37 weeks | Carbohydrates (g/kg/d) | 3.6 | 7.2 | 3.6 | 17.3 |
| Lipids (g/kg/d) | - | - | 1.0 | 4 | |
| Amino acids (g/kg/d) | 1.5 | 3.0 | 1.5 | 3.0 | |
| Energy (kcal/kg/d) | 45.0 | 50.0 | 75 | 85 |
| Parameter | Overall | BW < 1000 g | BW of 1000 to <1500 g | BW ≥ 1500 g |
|---|---|---|---|---|
| Patients, n (%) | 86 (100) | 28 (32.6) | 12 (16.3) | 46 (51.2) |
| Sex male, n (%) | 48 (55.8) | 18 (64.3) | 4 (33.3) | 26 (56.5) |
| Gestational age < 37 weeks, n (%) | 75 (87.2) | 28 (100) | 12 (100) | 35 (76.1) |
| Multiple birth yes, n (%) | 32 (37.2) | 9 (32.1) | 6 (50) | 17 (37.0) |
| Duration of PN, d, mean ± SD | 17.1 ± 11.4 | 27.4 ± 13.8 | 14.9 ± 5.6 | 11.4 ± 4.7 |
| Weight at start of PN, g, mean ± SD | 1655 ± 873.4 | 792.8 ± 107.4 | 1287.7 ± 161.2 | 2275.7 ± 731.5 |
| Weight at end of PN, g, mean ± SD | 1769.5 ± 872.3 | 973.4 ± 163.5 | 1345.7 ± 183.2 | 2364.6 ± 780.2 |
| Length at start of PN, cm, mean ± SD | 40.6 ± 6.1 | 33.8 ± 2 | 38.6 ± 1.2 | 45.3 ± 3.8 |
| Length at end of PN, cm, mean ± SD | 42.1 ± 5.9 | 35.7 ± 2.1 | 40 ± 1.3 | 46.6 ± 3.9 |
| Head circumference at start of PN, cm, mean ± SD | 28.1 ± 4.1 | 23.6 ± 1.6 | 27 ± 1.1 | 31.1 ± 2.7 |
| Head circumference at end of PN, cm, mean ± SD | 29.1 ± 3.8 | 25.2 ± 1.6 | 27.7 ± 1.6 | 31.9 ± 2.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Cloet, J.; Simal, I.; Benoot, K.; Goossens, L. Assessment of the Adherence to ESPGHAN 2018 Guidelines in the Neonatal Intensive Care Unit of the Ghent University Hospital: A Retrospective Study. Nutrients 2023, 15, 2324. https://doi.org/10.3390/nu15102324
De Cloet J, Simal I, Benoot K, Goossens L. Assessment of the Adherence to ESPGHAN 2018 Guidelines in the Neonatal Intensive Care Unit of the Ghent University Hospital: A Retrospective Study. Nutrients. 2023; 15(10):2324. https://doi.org/10.3390/nu15102324
Chicago/Turabian StyleDe Cloet, Joeri, Ine Simal, Karel Benoot, and Linde Goossens. 2023. "Assessment of the Adherence to ESPGHAN 2018 Guidelines in the Neonatal Intensive Care Unit of the Ghent University Hospital: A Retrospective Study" Nutrients 15, no. 10: 2324. https://doi.org/10.3390/nu15102324
APA StyleDe Cloet, J., Simal, I., Benoot, K., & Goossens, L. (2023). Assessment of the Adherence to ESPGHAN 2018 Guidelines in the Neonatal Intensive Care Unit of the Ghent University Hospital: A Retrospective Study. Nutrients, 15(10), 2324. https://doi.org/10.3390/nu15102324