
Positive Effects of a Lecithin-Based Delivery Form of Boswellia serrata Extract in Acute Diarrhea of Adult Subjects

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
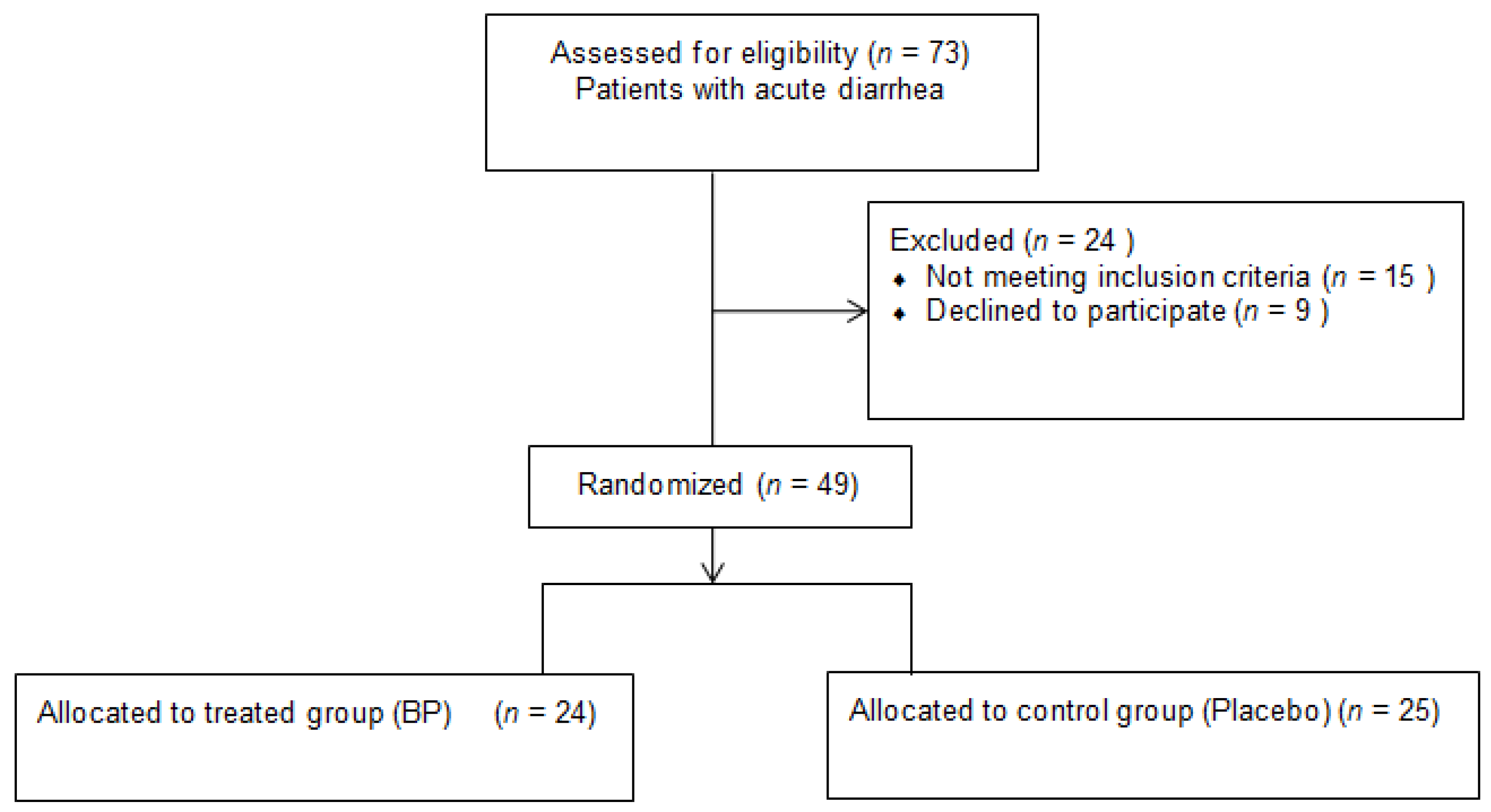
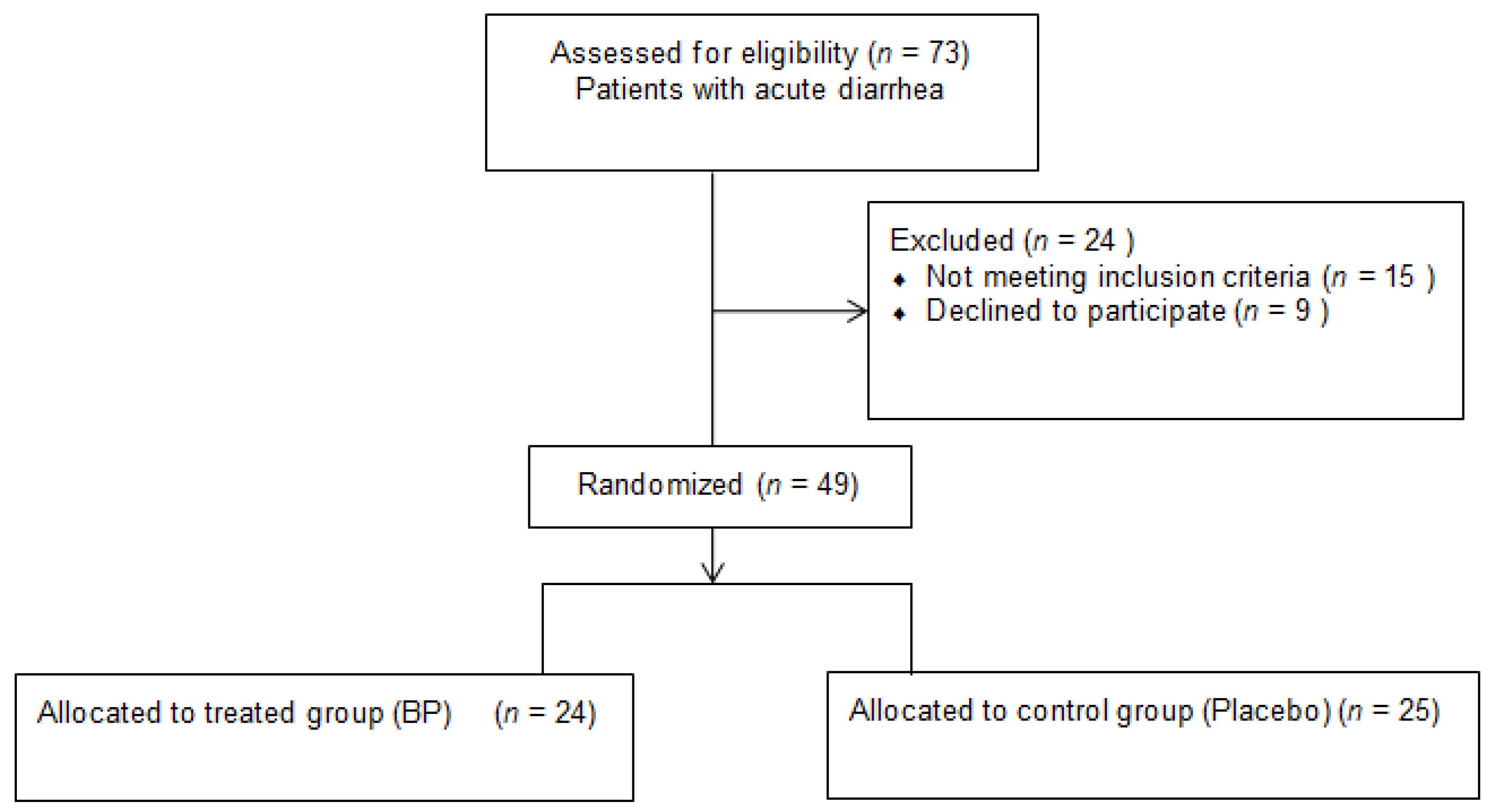
2.1. Study Design
2.2. Population
2.3. Treatment and Concomitant Medications
2.4. Clinical Evaluation
2.5. Supplement Description
2.6. Study Endpoints
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shane, A.L.; Mody, R.K.; Crump, J.A.; Tarr, P.I.; Steiner, T.S.; Kotloff, K.; Langley, J.M.; Wanke, C.; Warren, C.A.; Cheng, A.C.; et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin. Infect. Dis. 2017, 65, 1963–1973. [Google Scholar] [CrossRef]
- Kosek, M.; Bern, C.; Guerrant, R.L. The Global Burden of Diarrhoeal Disease, as Estimated from Studies Published between 1992 and 2000. Bull. World Health Organ. 2003, 81, 197–204. [Google Scholar] [CrossRef]
- Scallan, E.; Hoekstra, R.M.; Angulo, F.J.; Tauxe, R.V.; Widdowson, M.A.; Roy, S.L.; Jones, J.L.; Griffin, P.M. Foodborne Illness Acquired in the United States—Major Pathogens. Emerg. Infect. Dis. 2011, 17, 7–15. [Google Scholar] [CrossRef]
- Scallan, E.; Griffin, P.M.; Angulo, F.J.; Tauxe, R.V.; Hoekstra, R.M. Foodborne Illness Acquired in the United States—Unspecified Agents. Emerg. Infect. Dis. 2011, 17, 16–22. [Google Scholar] [CrossRef]
- DuPont, H.L. Diarrheal Diseases in the Developing World. Infect. Dis. Clin. N. Am. 1995, 9, 313–324. [Google Scholar] [CrossRef]
- Hedberg, C.W.; MacDonald, K.L.; Osterholm, M.T. Changing Epidemiology of Food-Borne Disease: A Minnesota Perspective. Clin. Infect. Dis. 1994, 18, 671–680. Available online: https://www.jstor.org/stable/4457788 (accessed on 20 August 2016). [CrossRef]
- Barr, W.; Smith, A. Acute Diarrhoea in Adults. Am. Fam. Physician 2014, 89, 180–189. [Google Scholar] [CrossRef]
- Bauer, T.M.; Lalvani, A.; Fehrenbach, J.; Steffen, I.; Aponte, J.J.; Segovia, R.; Vila, J.; Philippczik, G.; Steinbrückner, B.; Frei, R.; et al. Derivation and Validation of Guidelines for Stool Cultures for Enteropathogenic Bacteria Other than Clostridium Difficile in Hospitalized Adults. J. Am. Med. Assoc. 2001, 285, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Manatsathit, S.; Dupont, H.L.; Farthing, M. Guideline for the Management of Acute Diarrhea in Adults. J. Gastroenterol. Hepatol. 2002, 17, 54–71. [Google Scholar] [CrossRef] [Green Version]
- Rohner, P.; Pittet, D.; Pepey, B.; Nije-Kinge, T.; Auckenthaler, R. Etiological Agents of Infectious Diarrhea: Implications for Requests for Microbial Culture. J. Clin. Microbiol. 1997, 35, 1427–1432. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention Vital Signs: Preventing Clostridium Difficile Infections. MMWR. Morb. Mortal. Wkly. Rep. 2012, 61, 157–162. [CrossRef]
- Drancourt, M. Acute Diarrhea. Infect. Dis. 2017, 335–340.e2. [Google Scholar] [CrossRef]
- Belcaro, G.; Gizzi, G.; Pellegrini, L.; Corsi, M.; Dugall, M.; Cacchio, M.; Feragalli, B.; Togni, S.; Riva, A.; Eggenhoffner, R.; et al. Supplementation with a Lecithin-Based Delivery Form of Boswellia Serrata Extract (Casperome®) Controls Symptoms of Mild Irritable Bowel Syndrome. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2249–2254. [Google Scholar] [PubMed]
- Riva, A.; Giacomelli, L.; Totogni, S.; Franceschi, F.; Eggenhoffner, R.; Zuccarini, M.C.; Belcaro, G. Oral Administration of a Lecithin-Based Delivery Form of Boswellic Acids (Casperome®) for the Prevention of Symptoms of Irritable Bowel Syndrome: A Randomized Clinical Study. Minerva Gastroenterol. Dietol. 2019, 65, 30–35. [Google Scholar] [CrossRef]
- Likert, R. A Technique for the Measurement of Attitudes. Arch. Psychol. 1932, 22, 55. [Google Scholar]
- El Sherif, F.A.; Othman, A.H.; Abd El-Rahman, A.M.; Taha, O. Effect of Adding Intrathecal Morphine to a Multimodal Analgesic Regimen for Postoperative Pain Management after Laparoscopic Bariatric Surgery: A Prospective, Double-Blind, Randomized Controlled Trial. Br. J. Pain 2016, 10, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Brodribb, A.J.M. Treatment of Symptomatic Diverticular Disease with a High-Fibre Diet. Lancet 1977, 1, 664–666. [Google Scholar] [CrossRef]
- Kruis, W.; Meier, E.; Schumacher, M.; Mickisch, O.; Greinwald, R.; Mueller, R. Randomised Clinical Trial: Mesalazine (Salofalk Granules) for Uncomplicated Diverticular Disease of the Colon—A Placebo-Controlled Study. Aliment. Pharmacol. Ther. 2013, 37, 680–690. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2017. [Google Scholar]
- Taylor, D.N.; Sanchez, J.L.; Candler, W.; Thornton, S.; McQueen, C.; Echeverria, P. Treatment of Travelers’ Diarrhea: Ciprofloxacin plus Loperamide Compared with Ciprofloxacin Alone: A Placebo-Controlled, Randomized Trial. Ann. Intern. Med. 1991, 114, 731–734. [Google Scholar] [CrossRef]
- Riddle, M.S.; Arnold, S.; Tribble, D.R. Effect of Adjunctive Loperamide in Combination with Antibiotics on Treatment Outcomes in Traveler’s Diarrhea: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2008, 47, 1007–1014. [Google Scholar] [CrossRef]
- Matheson, A.J.; Noble, S. Racecadotril. Drugs 2000, 59, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Guarner, F.; Khan, A.G.; Garisch, J.; Eliakim, R.; Gangl, A.; Thomson, A.; Krabshuis, J.; Mair, T.L.; Kaufmann, P.; De Paula, J.A.; et al. World Gastroenterology Organisation Practice Guideline: Probiotics and Prebiotics—May 2008. S. Afr. Gastroenterol. Rev. 2008, 6, 14–25. [Google Scholar]
- Halloran, K.; Underwood, M.A. Probiotic Mechanisms of Action. Early Hum. Dev. 2019, 135, 58–65. [Google Scholar] [CrossRef]
- Nair, M.S.; Amalaradjou, M.; Venkitanarayanan, K. Antivirulence Properties of Probiotics in Combating Microbial Pathogenesis. Adv. Appl. Microbiol. 2017, 98, 1–29. [Google Scholar]
- Wilkins, T.; Sequoia, J. Probiotics for Gastrointestinal Conditions: A Summary of the Evidence. Am. Fam. Physician 2017, 96, 170–178. [Google Scholar]
- Liu, Y.; Tran, D.Q.; Rhoads, J.M. Probiotics in Disease Prevention and Treatment. J. Clin. Pharmacol. 2018, 58, S164–S179. [Google Scholar] [CrossRef]
- Collinson, S.; Deans, A.; Padua-Zamora, A.; Gregorio, G.V.; Li, C.; Dans, L.F.; Allen, S.J. Probiotics for Treating Acute Infectious Diarrhoea. Cochrane Database Syst. Rev. 2020, 2020, CD003048. [Google Scholar] [CrossRef]
- Siddiqui, M.Z. Boswellia Serrata, a Potential Antiinflammatory Agent: An Overview. Indian J. Pharm. Sci. 2011, 73, 255–261. [Google Scholar] [CrossRef]
- Raja, A.F.; Ali, F.; Khan, I.A.; Shawl, A.S.; Arora, D.S.; Shah, B.A.; Taneja, S.C. Antistaphylococcal and Biofilm Inhibitory Activities of Acetyl-11-Keto-β-Boswellic Acid from Boswellia Serrata. BMC Microbiol. 2011, 11, 54. [Google Scholar] [CrossRef] [Green Version]
- Maraghehpour, B.; Khayamzadeh, M.; Najafi, S.; Kharazifard, M. Traditionally Used Herbal Medicines with Antibacterial Effect on Aggegatibacter Actinomycetemcomitans: Boswellia Serrata and Nigella Sativa. J. Indian Soc. Periodontol. 2016, 20, 603–607. [Google Scholar] [CrossRef]
- Abdel-Tawab, M.; Werz, O.; Schubert-Zsilavecz, M. Boswellia Serrata: An Overall Assessment of in Vitro, Preclinical, Pharmacokinetic and Clinical Data. Clin. Pharmacokinet. 2011, 50, 349–369. [Google Scholar] [CrossRef] [PubMed]
- Poeckel, D.; Werz, O. Boswellic Acids: Biological Actions and Molecular Targets. Curr. Med. Chem. 2006, 13, 3359–3369. [Google Scholar] [CrossRef] [PubMed]
- Anthoni, C.; Laukoetter, M.G.; Rijcken, E.; Vowinkel, T.; Mennigen, R.; Müller, S.; Senninger, N.; Russell, J.; Jauch, J.; Bergmann, J.; et al. Mechanisms Underlying the Anti-Inflammatory Actions of Boswellic Acid Derivatives in Experimental Colitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, 1131–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammon, H.P.T. Modulation of the Immune System by Boswellia Serrata Extracts and Boswellic Acids. Phytomedicine 2010, 17, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Ammon, H.P.; Mack, T.; Singh, G.B.; Safayhi, H. Inhibition of Leukotriene B4 Formation in Rat Peritoneal Neutrophils by an Ethanolic Extract of the Gum Resin Exudate of Boswellia Serrata. Planta Med. 1991, 57, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Sana, H.; Sabitha Rani, A. Determination of Antioxidant Potential in Spilanthes Acmella Using DPPH Assay. Int. J. Curr. Microbiol. Appl. Sci. 2014, 3, 219–223. [Google Scholar]
- Catanzaro, D.; Rancan, S.; Orso, G.; Dall’Acqua, S.; Brun, P.; Giron, M.C.; Carrara, M.; Castagliuolo, I.; Ragazzi, E.; Caparrotta, L.; et al. Boswellia Serrata Preserves Intestinal Epithelial Barrier from Oxidative and Inflammatory Damage. PLoS ONE 2015, 10, e0125375. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, L.; Milano, E.; Franceschi, F.; Belcaro, G.; Gizzi, G.; Feragalli, G.; Dugall, M.; Luzzi, R.; Togni, S.; Eggenhoffner, R.; et al. Managing Ulcerative Colitis in Remission Phase: Usefulness of Casperome®, an Innovative Lecithin-Based Delivery System of Boswellia Serrata Extract. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2695–2700. [Google Scholar]
- Borrelli, F.; Capasso, F.; Capasso, R.; Ascione, V.; Aviello, G.; Longo, R.; Izzo, A.A. Effect of Boswellia Serrata on Intestinal Motility in Rodents: Inhibition of Diarrhoea without Constipation. Br. J. Pharmacol. 2006, 148, 553–560. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Treated Group (n = 24) Mean (SD) | Control Group (n = 25) Mean (SD) | p-Value a | |
|---|---|---|---|
| Age (years) | 50.37 (16.31) | 49.84 (14.77) | 0.90 |
| Number of stools at baseline | 5.37 (1.99) | 5.16 (1.82) | 0.70 |
| n (%) | n (%) | ||
| Sex | |||
| Female Male | 13 (54.17) 11 (45.83) | 14 (56.00) 11 (44.00) | 1 |
| Supplemented Group (n = 24) | Placebo Group (n = 25) | p-Value | |
|---|---|---|---|
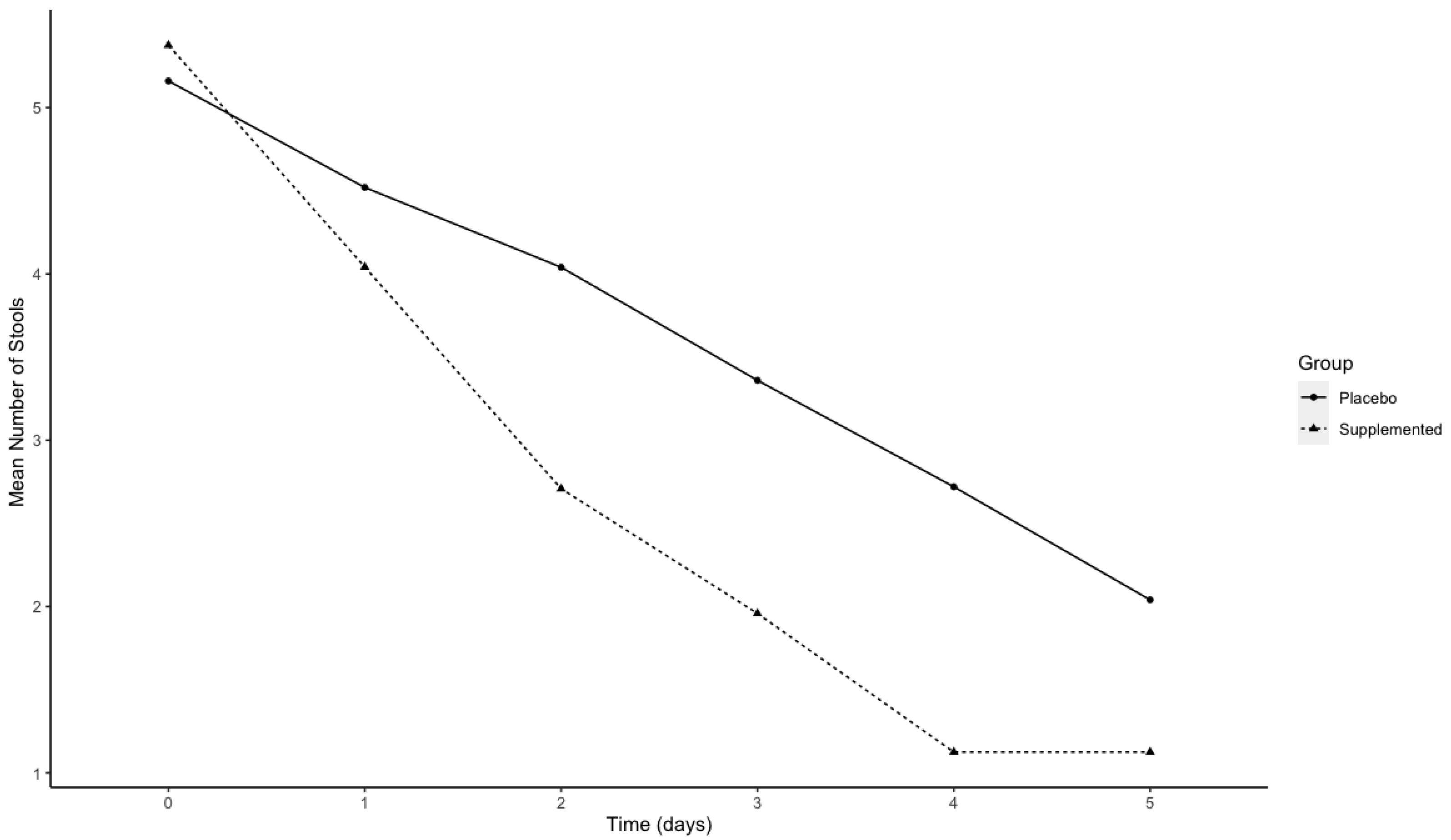
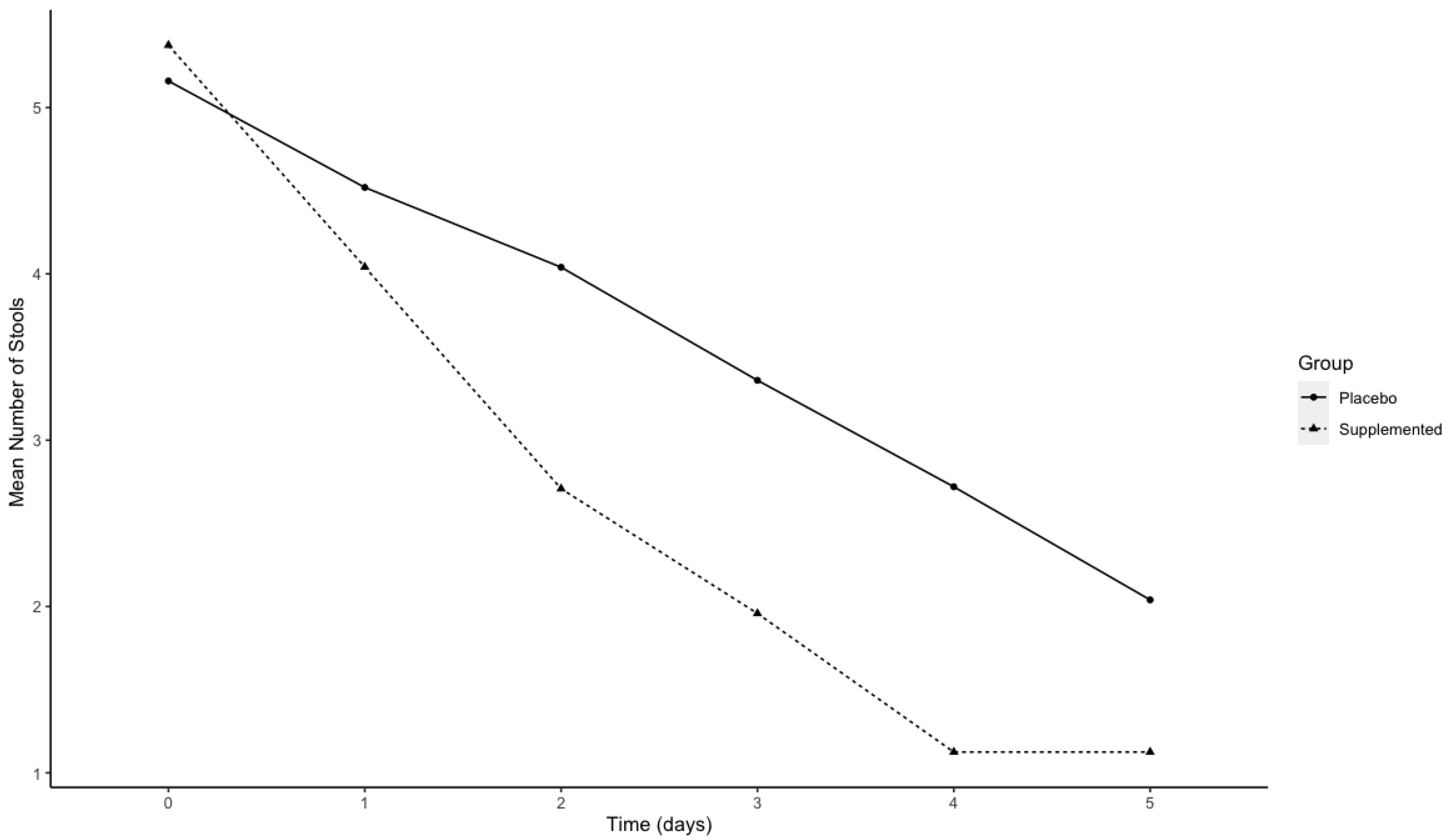
| Mean number of stool reported on day 0 | 5.37 (2.00) | 5.16 (1.82) | 0.85 |
| Mean number of stool reported on day 1 | 4.04 (1.63) | 4.52 (1.64) | 0.34 |
| Mean number of stool reported on day 2 | 2.71 (1.57) | 4.04 (1.37) | 0.02 |
| Mean number of stool reported on day 3 | 1.96 (1.12) | 3.36 (1.44) | 0.002 |
| Mean number of stool reported on day 4 | 1.12 (0.80) | 2.72 (1.81) | 0.002 |
| Mean number of stool reported on day 5 | 1.12 (0.61) | 2.04 (1.79) | 0.045 |
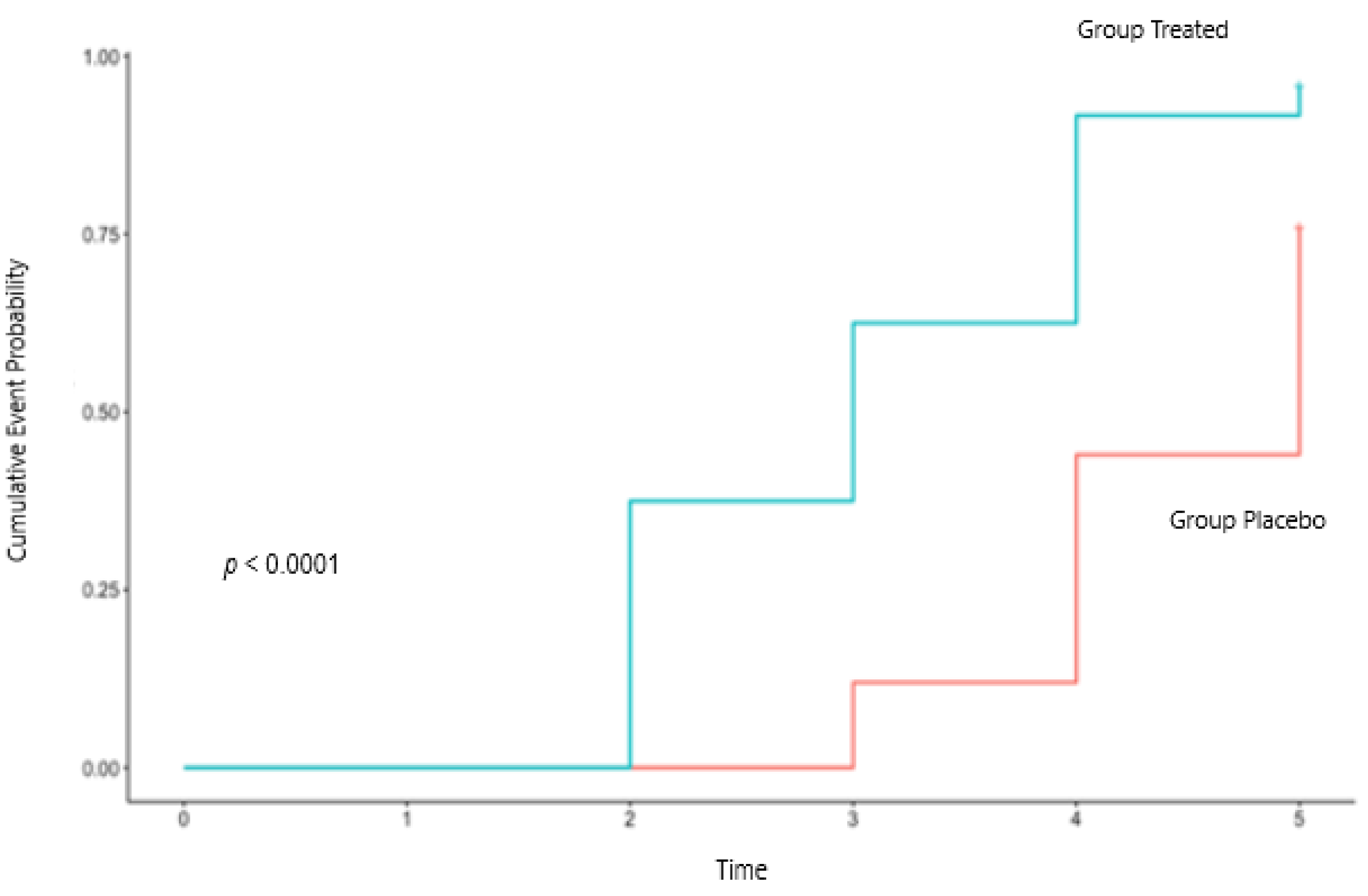
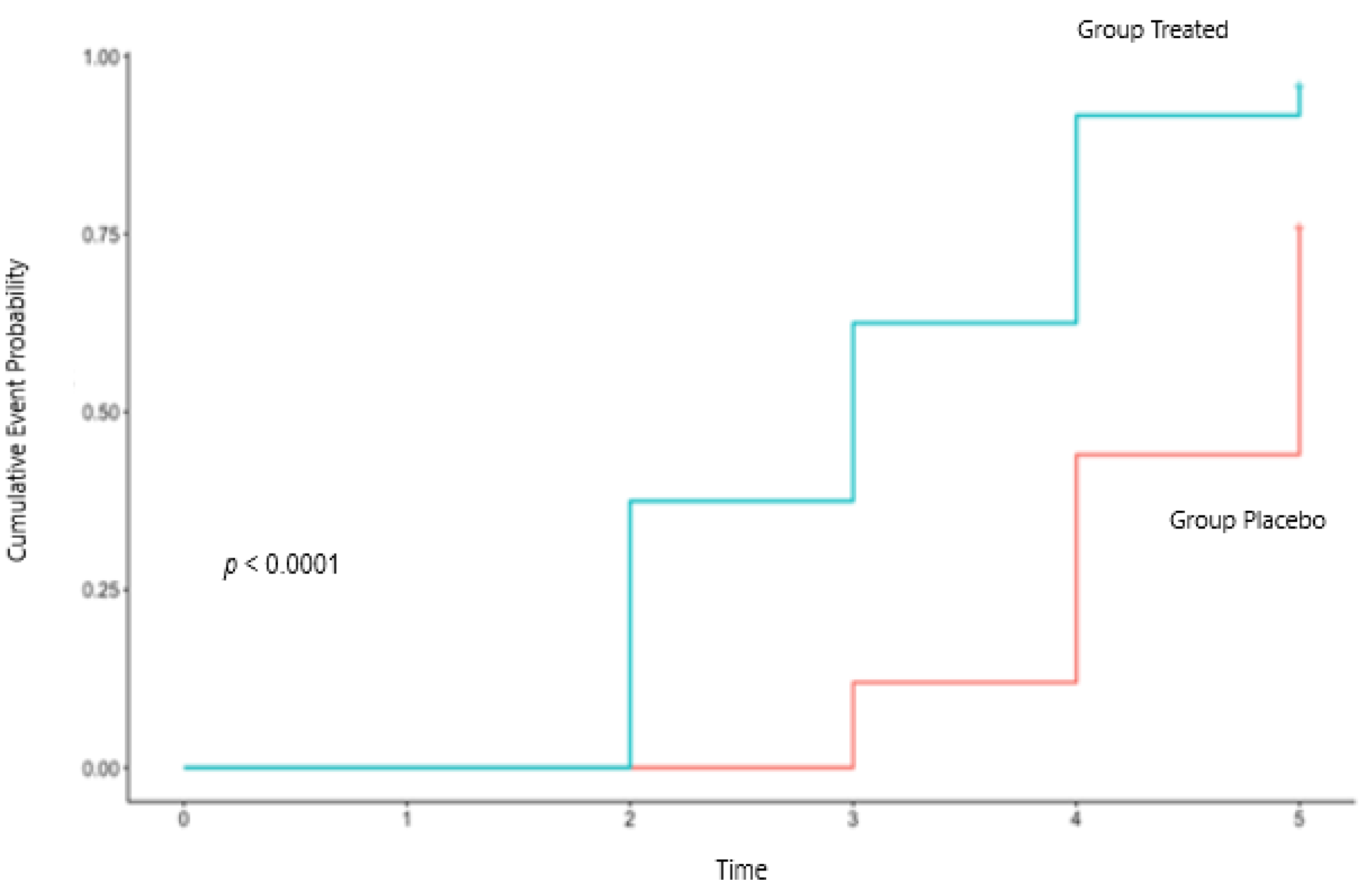
| Duration of diarrhea (days) | 3.08 (1.02) | 4.44 (0.71) | <0.0001 |
| Treated Group (n = 24) n (%) | Placebo Group (n = 25) n (%) | p-Value | |
|---|---|---|---|
| GAE | |||
| 1 2 3 4 | 1 (4.17) 2 (8.33) 10 (41.67) 11 (45.83) | 6 (24.00) 11 (44.00) 7 (28.00) 1 (4.00) | 0.0002 |
| Vomiting | |||
| 0 1 2 | 23 (95.83) 1 (4.17) 0 (0) | 22 (88.00) 2 (8.00) 2 (4.00) | 1 |
| Nausea | |||
| 0 1 2 | 19 (79.17) 5 (20.83) 0 (0) | 11 (44.00) 10 (40.00) 4 (16.00) | 0.02 |
| Abdominal Pain | |||
| 0 3 6 10 | 16 (66.67) 5 (20.83) 3 (12.50) 0 (0) | 8 (32.00) 4 (16.00) 8 (32.00) 5 (20.00) | 0.02 |
| Abdominal Distension | |||
| 0 1 2 3 | 9 (37.5) 8 (33.33) 6 (25.00) 1 (4.17) | 7 (28.00) 6 (24.00) 10 (40.00) 2 (8.00) | 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacosa, A.; Riva, A.; Petrangolini, G.; Allegrini, P.; Fazia, T.; Bernardinelli, L.; Peroni, G.; Rondanelli, M. Positive Effects of a Lecithin-Based Delivery Form of Boswellia serrata Extract in Acute Diarrhea of Adult Subjects. Nutrients 2022, 14, 1858. https://doi.org/10.3390/nu14091858
Giacosa A, Riva A, Petrangolini G, Allegrini P, Fazia T, Bernardinelli L, Peroni G, Rondanelli M. Positive Effects of a Lecithin-Based Delivery Form of Boswellia serrata Extract in Acute Diarrhea of Adult Subjects. Nutrients. 2022; 14(9):1858. https://doi.org/10.3390/nu14091858
Chicago/Turabian StyleGiacosa, Attilio, Antonella Riva, Giovanna Petrangolini, Pietro Allegrini, Teresa Fazia, Luisa Bernardinelli, Gabriella Peroni, and Mariangela Rondanelli. 2022. "Positive Effects of a Lecithin-Based Delivery Form of Boswellia serrata Extract in Acute Diarrhea of Adult Subjects" Nutrients 14, no. 9: 1858. https://doi.org/10.3390/nu14091858
APA StyleGiacosa, A., Riva, A., Petrangolini, G., Allegrini, P., Fazia, T., Bernardinelli, L., Peroni, G., & Rondanelli, M. (2022). Positive Effects of a Lecithin-Based Delivery Form of Boswellia serrata Extract in Acute Diarrhea of Adult Subjects. Nutrients, 14(9), 1858. https://doi.org/10.3390/nu14091858