
Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome





Abstract
:1. Introduction
2. Methods
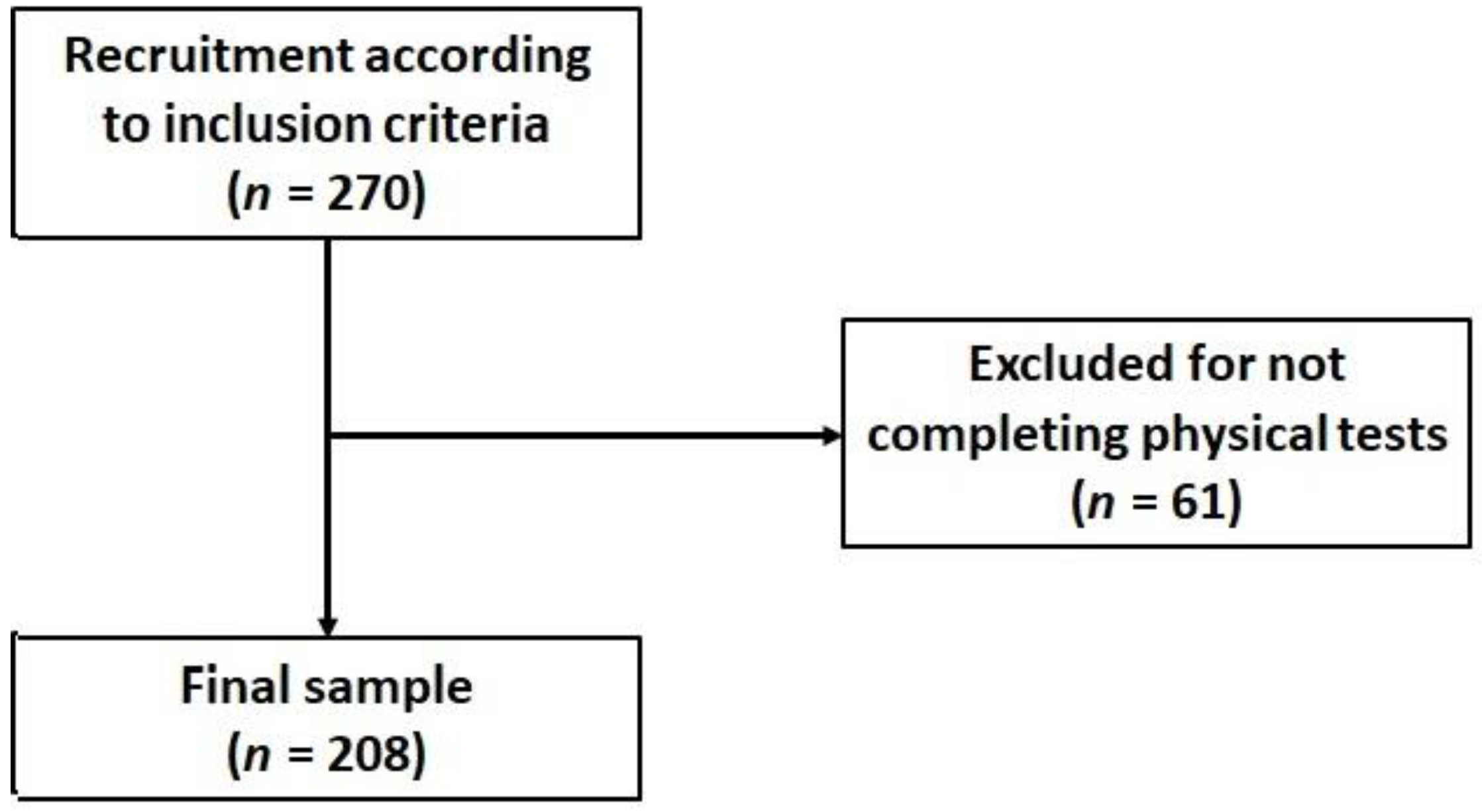
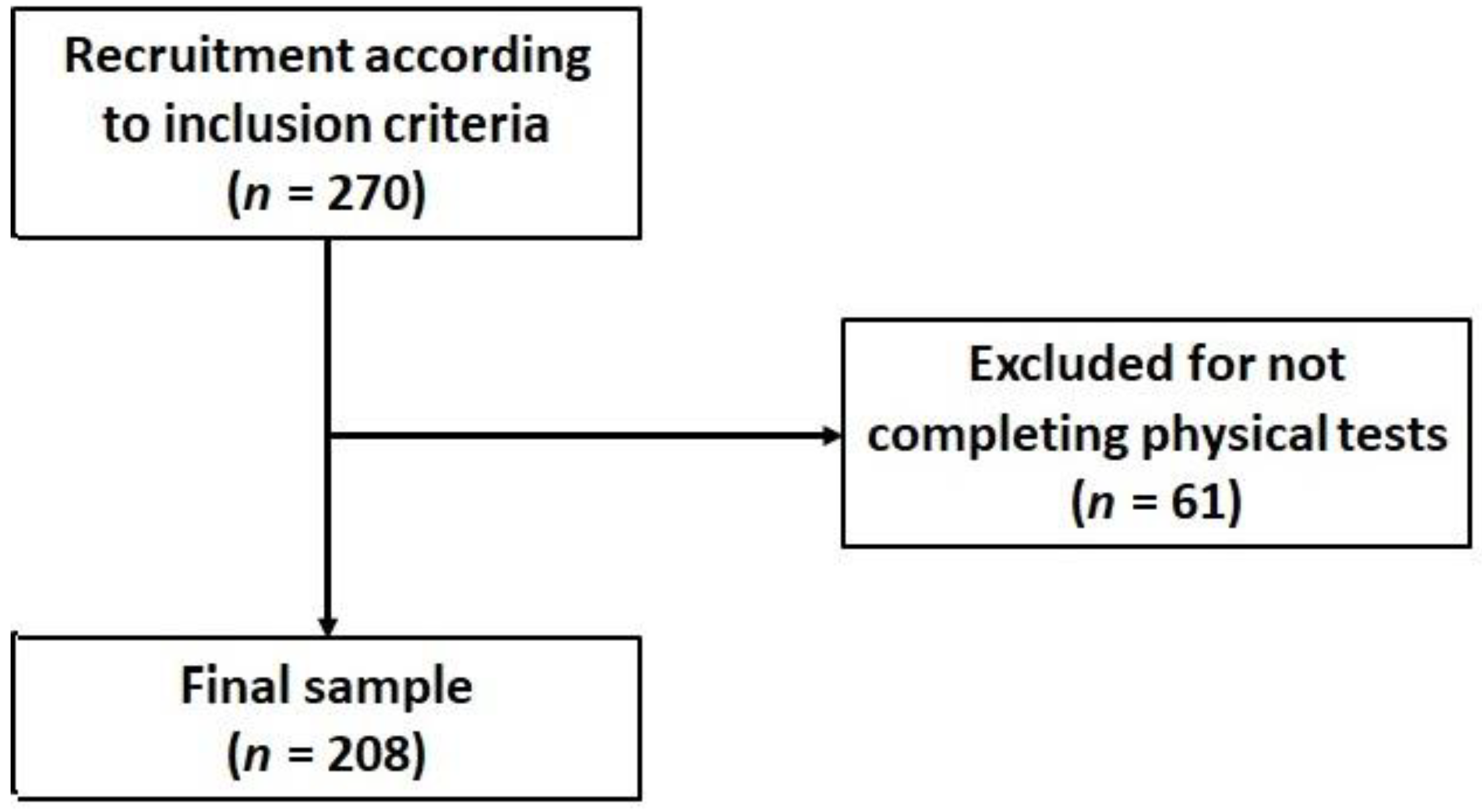
2.1. Design and Subjects
2.2. Sociodemographic and Lifestyle Determinants
2.3. Physical Activity
2.4. Anthropometrics, Blood Pressure, and Blood Analytical
2.5. Metabolic Syndrome Assessment
2.6. Functional Fitness Test Battery
2.7. Health-Related Quality of Life
2.8. Adherence to the Mediterranean Dietary Pattern
2.9. Statistics
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mateos, D.; Ugarriza, L.; Tur, J.A. Leisure-time physical activity and metabolic syndrome in older adults. Int. J. Environ. Res. Public Health 2019, 16, 3358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Capó, X.; Bouzas, C.; Mateos, D.; Pons, A.; Tur, J.A.; Sureda, A. Metabolic syndrome is associated with oxidative stress and proinflammatory state. Antioxidants 2020, 9, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engin, A. The definition and prevalence of obesity and metabolic syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar]
- Dziegielewska-Gesiak, S. Metabolic syndrome in an aging society—Role of oxidant-antioxidant imbalance and inflammation markers in disentangling atherosclerosis. Clin. Interv. Aging 2021, 16, 1057–1070. [Google Scholar] [CrossRef] [PubMed]
- Pucci, G.; Alcidi, R.; Tap, L.; Battista, F.; Mattace-Raso, F.; Schillaci, G. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: A review of the literature. Pharmacol. Res. 2017, 120, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Bergés, D.; de León, A.C.; Sanz, H.; Elosua, R.; Guembe, M.J.; Alzamora, M.; Vega-Alonso, T.; Félix-Redondo, F.J.; Ortiz-Marrón, H.; Rigo, F.; et al. Metabolic Syndrome in Spain: Prevalence and Coronary Risk Associated with Harmonized Definition and WHO Proposal. DARIOS Study. Rev. Española Cardiol. 2012, 65, 241–248. [Google Scholar] [CrossRef]
- Foscolou, A.; Magriplis, E.; Tyrovolas, S.; Soulis, G.; Bountziouka, V.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Anastasiou, F.; Gotsis, E.; et al. Lifestyle determinants of healthy ageing in a Mediterranean population: The multinational MEDIS study. Exp. Gerontol. 2018, 110, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Bowden, D.K.A.; Pickles, S.; Sprung, V.S.; Kemp, G.J.; Alam, U.; Moore, D.R.; Tahrani, A.A.; Cuthbertson, D.J. Reduced physical activity in young and older adults: Metabolic and musculoskeletal implications. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819888824. [Google Scholar]
- Carroll, S.; Dudfield, M. What is the relationship between exercise and metabolic abnormalities? A review of the metabolic syndrome. Sport Med. 2004, 34, 371–418. [Google Scholar] [CrossRef]
- Joseph, M.S.; Tincopa, M.A.; Walden, P.; Jackson, E.; Conte, M.L.; Rubenfire, M. The impact of structured exercise programs on metabolic syndrome and its components: A systematic review. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2395–2404. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrano-Sánchez, J.A.; Fernández-Rodríguez, M.J.; Sanchis-Moysi, J.; del Cristo Rodríguez-Pérez, M.; Marcelino-Rodríguez, I.; de León, A.C. Domain and intensity of physical activity are associated with metabolic syndrome: A population-based study. PLoS ONE 2019, 14, e0219798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, P.K.; Zhao, Y.; Liu, J.D.; Quach, B. A canonical correlation analysis on the relationship between functional fitness and health-related quality of life in older adults. Arch. Gerontol. Geriatr. 2017, 68, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef]
- Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Gillison, F.B.; Skevington, S.M.; Sato, A.; Standage, M.; Evangelidou, S. The effects of exercise interventions on quality of life in clinical and healthy populations; a meta-analysis. Soc. Sci. Med. 2009, 68, 1700–1710. [Google Scholar] [CrossRef] [Green Version]
- Medrano-Ureña, M.D.R.; Ortega-Ruiz, R.; de Benítez-Sillero, J.D. Physical fitness, exercise self-efficacy, and quality of life in adulthood: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6343. [Google Scholar] [CrossRef] [PubMed]
- Knapik, A.; Brzęk, A.; Famuła-Wąż, A.; Gallert-Kopyto, W.; Szydłak, D.; Marcisz, C.; Plinta, R. The relationship between physical fitness and health self-assessment in elderly. Medicine 2019, 98, e15984. [Google Scholar] [CrossRef]
- Nawrocka, A.; Polechoński, J.; Garbaciak, W.; Mynarski, W. Functional fitness and quality of life among women over 60 years of age depending on their level of objectively measured physical activity. Int. J. Environ. Res. Public Health 2019, 16, 972. [Google Scholar] [CrossRef] [Green Version]
- Sunde, S.; Hesseberg, K.; Skelton, D.A.; Ranhoff, A.H.; Pripp, A.H.; Aarønæs, M.; Brovold, T. Associations between health-related quality of life and physical function in older adults with or at risk of mobility disability after discharge from the hospital. Eur. Geriatr. Med. 2021, 12, 1247–1256. [Google Scholar] [CrossRef]
- Ostman, C.; Jewiss, D.; Smart, N.A. The Effect of Exercise Training Intensity on Quality of Life in Heart Failure Patients: A Systematic Review and Meta-Analysis. Cardiology 2017, 136, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Vega-López, S.; Chavez, A.; Farr, K.J.; Ainsworth, B.E. Validity and reliability of two brief physical activity questionnaires among Spanish-speaking individuals of Mexican descent. BMC Res. Notes 2014, 7, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, A.; Brugnera, A.; Adorni, R.; D’Addario, M.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Maloberti, A.; Zanatta, F.; Steca, P. Protein intake and physical activity in newly diagnosed patients with acute coronary syndrome: A 5-year longitudinal study. Nutrients 2021, 13, 634. [Google Scholar] [CrossRef] [PubMed]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.B. The Rapid Assessment of Physical Activity (RAPA) Among Older Adults. Prev. Chronic Dis. 2006, 3, A118. [Google Scholar]
- Daimiel, L.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Schröder, H.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; Lopez-Miranda, J.; et al. Physical fitness and physical activity association with cognitive function and quality of life: Baseline cross-sectional analysis of the PREDIMED-Plus trial. Sci. Rep. 2020, 10, 3472. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.Y.; Yang, C.Y.; Shih, S.R.; Hsieh, H.J.; Hung, C.S.; Chiu, F.C.; Lin, M.-S.; Liu, P.-H.; Hua, C.-H.; Hsein, Y.-C.; et al. Measurement of waist circumference: Midabdominal or iliac crest? Diabetes Care 2013, 36, 1660–1666. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community—Residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Chien, M.Y.; Kuo, H.K.; Wu, Y.T. Sarcopenia, cardiopulmonary fitness, and physical disability in community-dwelling elderly people. Phys. Ther. 2010, 90, 1277–1287. [Google Scholar] [CrossRef]
- Jiménez-García, J.D.; Martínez-Amat, A.; De La Torre-Cruz, M.J.; Fábrega-Cuadros, R.; Cruz-Díaz, D.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension Training HIIT Improves Gait Speed, Strength and Quality of Life in Older Adults. Int. J. Sports Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Nawrocka, A.; Mynarski, W.; Cholewa, J. Adherence to physical activity guidelines and functional fitness of elderly women, using objective measurement. Ann. Agric. Environ. Med. 2017, 24, 632–635. [Google Scholar] [CrossRef]
- Vargas, d.O.B.L.; Albuquerque, M.N.G.; Moraes, H.; Fonseca, S.E.R.; Camaz, D.A. Relationship between level of independence in activities of daily living and estimated cardiovascular capacity in elderly women. Arch. Gerontol. Geriatr. 2014, 59, 367–371. [Google Scholar]
- Hsiao, M.Y.; Li, C.M.; Lu, I.S.; Lin, Y.H.; Wang, T.G.; Han, D.S. An investigation of the use of the Kinect system as a measure of dynamic balance and forward reach in the elderly. Clin. Rehabil. 2018, 32, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, R.; Tomohiro, O. A novel exercise for improving lower-extremity functional fitness in the elderly. Aging Clin. Exp. Res. 2005, 18, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.M.; Thomas, S.G.; Burr, J. Evidence-based risk assessment and recommendations for exercise testing and physical activity clearance in apparently healthy individuals. Appl. Physiol. Nutr. Metab. 2011, 36 (Suppl. 1), 14–32. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Prieto, L.; Anto, J.M. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Bergland, A. Effect of a resistance and balance exercise programme for women with osteoporosis and vertebral fracture: Study protocol for a randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 100. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Moreiras, O.; Carbajal, A.; Cabrera, L. Tablas de Composición de Alimentos, 17th ed.; Piramide: Madrid, Spain, 2015. [Google Scholar]
- Sureda, A.; Del Mar Bibiloni, M.; Julibert, A.; Bouzas, C.; Argelich, E.; Llompart, I.; Pons, A.; Tur, J.A. Adherence to the mediterranean diet and inflammatory markers. Nutrients 2018, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 34826348, 2599–2608. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Villegas, A.; Martínez, J.A.; De Irala, J.; Martínez-González, M.A. Determinants of the adherence to an “a priori” defined Mediterranean dietary pattern. Eur. J. Nutr. 2002, 41, 249–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switerzerland, 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/325147/WHO-NMH-PND-2019.4-eng.pdf?sequence=1&isAllowed=y%0Ahttp://www.who.int/iris/handle/10665/311664%0Ahttps://apps.who.int/iris/handle/10665/325147 (accessed on 25 March 2022).
- Van Den Bogaard, L.; Henkens, K.; Kalmijn, M. Retirement as a relief? The role of physical job demands and psychological job stress for effects of retirement on self-rated health. Eur. Soc. Rev. 2016, 32, 295–306. [Google Scholar] [CrossRef] [Green Version]
- Rijk, L.; Kortlever, J.T.; Bandell, D.L.; Zhang, J.; Gallagher, S.M.; Bozic, K.J.; Ring, D. The impact of socioeconomic status and social deprivation on musculoskeletal limitations. J. Orthop. 2020, 22, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Rosique-Esteban, N.; Babio, N.; Díaz-López, A.; Romaguera, D.; Martinez, J.A.; Martin-Sanchez, V.; Schröder, H.; Estruch, R.; Vidal, J.; Buil-Cosiales, P.; et al. Leisure-time physical activity at moderate and high intensity is associated with parameters of body composition, muscle strength and sarcopenia in aged adults with obesity and metabolic syndrome from the PREDIMED-Plus study. Clin. Nutr. 2019, 38, 1324–1331. [Google Scholar] [CrossRef]
- Koster, A.; Patel, K.V.; Visser, M.; van Eijk, J.T.M.; Kanaya, A.M.; de Rekeneire, N.; Newman, A.B.; Tylavsky, F.A.; Kritchevsky, S.B.; Harris, T.B.; et al. Joint effects of adiposity and physical activity on incident mobility limitation in older adults. J. Am. Geriatr. Soc. 2008, 56, 636–643. [Google Scholar] [CrossRef]
- Meadows, R.; Bower, J.K. Associations of anthropometric measures of obesity with physical limitations in older adults. Disabil. Rehabil. 2020, 42, 1101–1106. [Google Scholar] [CrossRef]
- Stokes, A.C.; Xie, W.; Lundberg, D.J.; Hempstead, K.; Zajacova, A.; Zimmer, Z.; Glei, D.A.; Meara, E.; Preston, S.H. Increases in BMI and chronic pain for US adults in midlife, 1992 to 2016. SSM Popul. Health 2020, 12, 100644. [Google Scholar] [CrossRef]

{kind=link}
| Men | Women | p | |
|---|---|---|---|
| Sample (n; %) | 121 (57.8) | 88 (42.2) | 0.022 * |
| Age (years; mean and SD) | 63.3 (5.6) | 65.6 (4.2) | 0.001 * |
| Height (cm; mean and SD) | 169.3 (6.1) | 155.1 (5.7) | 0.001 * |
| Weight (kg; mean and SD) | 93.3 (13.3) | 79.5 (10.7) | 0.001 * |
| BMI (kg/m2; mean and SD) | 32.4 (3.5) | 33.03 (3.8) | 0.261 * |
| Waist circumference (cm; mean and SD) | 113.9 (9.5) | 106.6 (9.4) | 0.001 * |
| Obesity (n; %) | 121 (57.8) | 88 (42.2) | 0.022 # |
| Metabolic pathologies (n; %) | |||
| 3 | 57 (47.1) | 48 (54.5) | 0.440 # |
| 4 | 42 (34.7) | 29 (33.0) | |
| 5 | 22 (18.2) | 11 (12.5) | |
| Physical activity (n; %) | |||
| Low | 77 (63.6) | 57 (64.8) | 0.972 # |
| Medium | 25 (20.7) | 17 (19.3) | |
| High | 19 (15.7) | 14 (15.9) | |
| Adherence to MedDiet (n; %) | |||
| Low (<p25) | 54 (45.4) | 19 (21.6) | 0.001 # |
| Medium (p25–p75) | 45 (37.8) | 43 (48.9) | |
| High (>p75) | 20 (16.8) | 26 (29.5) | |
| Smoking (n; %) | |||
| Smoker | 19 (15.7) | 10 (11.5) | 0.001 # |
| Ex-smoker | 72 (59.5) | 30 (34.5) | |
| Nonsmoker | 30 (24.8) | 47 (54.0) | |
| Civil status (n; %) | |||
| Married | 98 (81.0) | 63 (71.6) | 0.001 # |
| Divorced | 15 (12.4) | 1 (1.1) | |
| Single | 4 (3.3) | 9 (10.2) | |
| Widow | 4 (3.3) | 15 (17.0) | |
| Educational level (n; %) | |||
| Primary | 45 (37.2) | 55 (62.5) | 0.001 # |
| Secondary | 44 (36.4) | 20 (22.7) | |
| University | 32 (26.4) | 13 (14.8) | |
| Employment status (n; %) | |||
| Retired | 63 (52.5) | 54 (61.4) | 0.261 # |
| Active | 57 (47.5) | 34 (38.6) | |
| Physical and health tests (mean; SD) | |||
| Functional fitness score | 3.89 (2.2) | 3.78 (2.3) | 0.726 * |
| Physical health component | 48.14 (7.5) | 44.37 (9.4) | 0.008 * |
| Mental health component | 52.05 (10.4) | 46.79 (12.2) | 0.001 * |
| Variable | Lower-Body Strength | Endurance | One-Leg Balance | Standing Handgrip | Sitting Handgrip | Agility | Upper-Body Flexibility | Lower-Body Flexibility | Physical Role | Physical Function | Body Pain | General Health | Social Functioning | Emotional Health | Mental Health | Vitality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Endurance | 0.58 ** | |||||||||||||||
| (0.48, 0.67) | ||||||||||||||||
| One-leg balance | 0.30 ** | 0.34 ** | ||||||||||||||
| (0.17, 0.42) | (0.21, 0.46) | |||||||||||||||
| Standing handgrip | 0.28 ** | 0.33 ** | 0.35 ** | |||||||||||||
| (0.15, 0.40) | (0.20, 0.45) | (0.22, 0.46) | ||||||||||||||
| Sitting handgrip | 0.28 ** | 0.32 ** | 0.34 ** | 0.97 ** | ||||||||||||
| (0.15, 0.40) | (0.19, 0.44) | (0.21, 0.46) | (0.96, 0.98) | |||||||||||||
| Agility | 0.16 * | 0.13 | 0.11 | 0.02 | 0.01 | |||||||||||
| (0.02, 0.29) | (−0.01, 0.27) | (−0.03, 0.24) | (−0.12, 0.16) | (−0.13, 0.14) | ||||||||||||
| Upper-body flexibility | 0.13 | 0.14 | 0.09 | −0.08 | −0.08 | 0.24 ** | ||||||||||
| (−0.01, 0.26) | (−0.00, 0.27) | (−0.04, 0.23) | (−0.21, 0.06) | (−0.21, 0.06) | (0.11, 0.37) | |||||||||||
| Lower-body flexibility | −0.51 ** | −0.48 ** | −0.53 ** | −0.39 ** | −0.37 ** | −0.12 | −0.17 * | |||||||||
| (−0.60, −0.40) | (−0.58, −0.36) | (−0.62, −0.43) | (−0.50, −0.26) | (−0.48, −0.24) | (−0.25, 0.01) | (−0.30, −0.04) | ||||||||||
| Physical role | 0.17 * | 0.27 ** | 0.12 | 0.11 | 0.11 | −0.06 | 0.03 | −0.21 ** | ||||||||
| (0.03, 0.30) | (0.13, 0.40) | (−0.02, 0.25) | (−0.02, 0.25) | (−0.03, 0.24) | (−0.20, 0.07) | (−0.10, 0.17) | (−0.33, −0.07) | |||||||||
| Physical function | 0.36 ** | 0.43 ** | 0.41 ** | 0.40 ** | 0.39 ** | 0.12 | 0.01 | −0.51 ** | 0.40 ** | |||||||
| (0.23, 0.47) | (0.31, 0.54) | (0.29, 0.52) | (0.27, 0.50) | (0.27, 0.50) | (−0.01, 0.26) | (−0.12, 0.15) | (−0.61, −0.40) | (0.28, 0.51) | ||||||||
| Body pain | 0.19 ** | 0.23 ** | 0.15 * | 0.25 ** | 0.23 ** | 0.00 | −0.07 | −0.19 ** | 0.44 ** | 0.55 ** | ||||||
| (0.05, 0.31) | (0.09, 0.36) | (0.01, 0.28) | (0.12, 0.37) | (0.10, 0.36) | (−0.13, 0.14) | (−0.21, 0.06) | (−0.32, −0.05) | (0.32, 0.54) | (0.45, 0.64) | |||||||
| General health | 0.10 | 0.17 * | 0.26 ** | 0.18 ** | 0.17 * | 0.12 | 0.14 * | −0.23 ** | 0.22 ** | 0.43 ** | 0.28 ** | |||||
| (−0.03, 0.24) | (0.03, 0.30) | (0.13, 0.39) | (0.05, 0.31) | (0.03, 0.30) | (−0.01, 0.25) | (0.01, 0.27) | (−0.36, −0.10) | (0.08, 0.34) | (0.32, 0.54) | (0.14, 0.40) | ||||||
| Social functioning | −0.01 | 0.12 | 0.09 | 0.14 * | 0.14 | −0.07 | 0.01 | −0.07 | 0.39 ** | 0.24 ** | 0.15 * | 0.16 * | ||||
| (−0.14, 0.13) | (−0.02, 0.26) | (−0.05, 0.22) | (0.01, 0.27) | (−0.00, 0.27) | (−0.21, 0.07) | (−0.13, 0.14) | (−0.20, 0.07) | (0.26, 0.50) | (0.10, 0.36) | (0.01, 0.28) | (0.02, 0.29) | |||||
| Emotional role | −0.06 | 0.02 | 0.03 | 0.06 | 0.07 | −0.13 | −0.04 | −0.09 | 0.32 ** | 0.21 ** | 0.18 ** | 0.17* | 0.59 ** | |||
| (−0.20, 0.07) | (−0.12, 0.16) | (−0.10, 0.17) | (−0.07, 0.20) | (−0.07, 0.20) | (−0.26, 0.01) | (−0.17, 0.10) | (−0.22, 0.04) | (0.20, 0.44) | (0.08, 0.34) | (0.05, 0.31) | (0.03, 0.29) | (0.49, 0.67) | ||||
| Mental health | 0.10 | 0.18 * | 0.07 | 0.23 ** | 0.23 ** | 0.02 | 0.00 | −0.18 ** | 0.36 ** | 0.34 ** | 0.31 ** | 0.34 ** | 0.38 ** | 0.51 ** | ||
| (−0.04, 0.23) | (0.04, 0.31) | (−0.07, 0.20) | (0.09, 0.35) | (0.09, 0.35) | (−0.11, 0.16) | (−0.13, 0.14) | (−0.31, −0.04) | (0.24, 0.48) | (0.22, 0.46) | (0.18, 0.42) | (0.21, 0.45) | (0.26, 0.49) | (0.40, 0.60) | |||
| Vitality | 0.16 * (0.03, 0.29) | 0.23 ** (0.09, 0.36) | 0.16 * (0.02, 0.29) | 0.19 ** (0.06, 0.32) | 0.17 * (0.04, 0.30) | 0.19 ** (0.06, 0.32) | 0.02 (−0.12, 0.16) | −0.23 ** (−0.36, −0.10) | 0.38 ** (0.25, 0.49) | 0.52 ** (0.41, 0.61) | 0.43 ** (0.31, 0.54) | 0.43 ** (0.31, 0.53) | 0.35 ** (0.22, 0.46) | 0.33 ** (0.20, 0.44) | 0.58 ** (0.49, 0.67) | |
| MDA | −0.07 (−0.20, 0.07) | −0.06 (−0.20, 0.08) | 0.01 (−0.12, 0.15) | −0.23 (0.35, −0.09) | −0.22 (−0.35, 0.09) | 0.26 * (0.12, 0.38) | 0.05 (−0.09, 0.19) | 0.08 (−0.05, 0.22) | 0.08 (−0.05, 0.22) | −0.07 (−0.21, 0.06) | 0.00 (−0.13, 0.14) | 0.03 −0.11, 0.16) | 0.03 (−0.10, 0.17) | 0.09 (−0.04, 0.23) | 0.03 (−0.11, 0.16) | 0.08 (−0.06, 0.21) |
| Functional Fitness | Physical Component > MeP | Mental Component > MeP | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Crude Values | Adjusted Values | Crude Values | Adjusted Values | Crude Values | Adjusted Values | |||||||||||||
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Model 1: health factors | ||||||||||||||||||
| Functional fitness score | ||||||||||||||||||
| High vs. low | - | - | - | - | - | - | 2.14 | 1.15–4.00 | 0.012 | 1.89 | 1.02–3.53 | 0.044 | 0.50 | 0.27–0.89 | 0.019 | 0.49 | 0.26–0.91 | 0.025 |
| MetS criteria | ||||||||||||||||||
| 4 vs. 3 | 0.85 | 0.45–1.59 | 0.623 | 0.89 | 0.46–1.72 | 0.737 | 1.09 | 0.59–2.00 | 0.777 | 1.16 | 0.61–2.18 | 0.651 | 0.93 | 0.50–1.71 | 0.822 | 0.95 | 0.51–2.70 | 0.891 |
| 5 vs. 4 | 0.19 | 0.05–0.54 | 0.004 | 0.19 | 0.05–0.56 | 0.005 | 0.67 | 0.29–1.50 | 0.346 | 0.88 | 0.35–2.14 | 0.794 | 1.25 | 0.56–2.82 | 0.588 | 1.10 | 0.46–2.70 | 0.833 |
| Body mass index | ||||||||||||||||||
| Obesity I vs. preobesity | 0.65 | 0.33–1.29 | 0.223 | 0.61 | 0.30–1.24 | 0.179 | 0.65 | 0.33, 1.27 | 0.203 | 0.70 | 0.35–1.40 | 0.318 | 1.25 | 0.637–2.44 | 0.520 | 1.20 | 0.59–2.41 | 0.609 |
| Obesity II or III vs. preobesity | 0.19 | 0.07–0.44 | 0.001 | 0.18 | 0.07–0.44 | 0.001 | 0.44 | 0.20, 0.935 | 0.034 | 0.56 | 0.25–1.26 | 0.162 | 1.18 | 0.561–2.48 | 0.664 | 0.92 | 0.41–2.06 | 0.856 |
| Model 2: lifestyle factors | ||||||||||||||||||
| Physical activity level | ||||||||||||||||||
| High vs. low | 8.09 | 3.45–20.8 | 0.001 | 10.3 | 4.19–28.2 | 0.001 | 3.25 | 1.48–7.50 | 0.003 | 3.25 | 1.44–7.72 | 0.005 | 0.74 | 0.34–1.59 | 0.440 | 0.71 | 0.32–1.57 | 0.404 |
| Medium vs. low | 1.94 | 0.93–4.02 | 0.074 | 1.83 | 0.83–3.97 | 0.126 | 1.63 | 0.80–7.50 | 0.171 | 2.21 | 1.01–4.51 | 0.046 | 1.16 | 0.57–2.37 | 0.685 | 1.13 | 0.54–2.40 | 0.736 |
| Adherence to MedDiet | ||||||||||||||||||
| Medium vs. low | 1.40 | 0.72–2.76 | 0.320 | 1.93 | 0.75–4.32 | 0.090 | 0.68 | 0.36–1.29 | 0.246 | 0.77 | 0.39–1.50 | 0.446 | 1.57 | 0.84–2.95 | 0.159 | 1.46 | 0.77–2.78 | 0.242 |
| High vs. low | 1.54 | 0.71–3.33 | 0.271 | 1.80 | 0.75–4.32 | 0.186 | 1.63 | 0.77–3.47 | 0.199 | 1.60 | 0.73–3.54 | 0.237 | 1.69 | 0.80–3.61 | 0.170 | 1.78 | 0.83–3.88 | 0.143 |
| Smoking | ||||||||||||||||||
| Ex-smoker vs. smoker | 0.66 | 0.28–1.57 | 0.354 | 0.41 | 0.15–1.08 | 0.073 | 0.70 | 0.30–1.63 | 0.404 | 0.58 | 0.24–1.42 | 0.233 | 1.31 | 0.564–3.02 | 0.523 | 1.37 | 0.57–3.25 | 0.467 |
| Nonsmoker vs. smoker | 0.39 | 0.15–0.96 | 0.042 | 0.23 | 0.08–0.63 | 0.004 | 1.56 | 0.66–3.72 | 0.313 | 1.38 | 0.56–3.42 | 0.481 | 0.75 | 0.315–1.77 | 0.514 | 0.77 | 0.31–1.86 | 0.561 |
| Model 3: sociodemographic factors | ||||||||||||||||||
| Sex | ||||||||||||||||||
| Women vs. men | 1.09 | 0.60–1.94 | 0.778 | 1.47 | 0.74–2.96 | 0270 | 1.31 | 0.75–2.28 | 0.355 | 1.32 | 0.71–2.46 | 0.378 | 0.86 | 0.497–1.50 | 0.604 | 0.89 | 0.45–1.69 | 0.722 |
| Employment level | ||||||||||||||||||
| Active vs. retired | 2.22 | 1.47–3.41 | 0.001 | 2.17 | 1.39–3.43 | 0.001 | 1.02 | 0.68–1.50 | 0.930 | 1.02 | 0.67–1.55 | 0913 | 0.592 | 0.39–0.87 | 0.009 | 0.62 | 0.40–0.95 | 0.030 |
| Civil status | ||||||||||||||||||
| Divorced | 0.91 | 0.26–2.77 | 0.871 | 0.84 | 0.23–2.76 | 0.787 | 0.52 | 0.15–1.50 | 0.246 | 0.57 | 0.17–1.71 | 0.339 | 0.39 | 0.12–1.12 | 0.086 | 0.42 | 0.13–1.26 | 0.129 |
| Single | 1.91 | 0.60–6.20 | 0.264 | 1.62 | 0.23–2.76 | 0.451 | 0.51 | 0.13–1.63 | 0.278 | 0.43 | 0.11–1.45 | 0.197 | 1.06 | 0.33–3.63 | 0.927 | 1.34 | 0.40–4.88 | 0.633 |
| Widow | 1.15 | 0.39–3.15 | 0.792 | 0.90 | 0.45–5.83 | 0.850 | 0.48 | 0.48–3.37 | 0.618 | 1.17 | 0.43–3.20 | 0.759 | 0.23 | 0.07–0.65 | 0.008 | 0.23 | 0.06–0.67 | 0.010 |
| Educational level | ||||||||||||||||||
| Primary vs. university | 0.33 | 0.15–0.70 | 0.004 | 0.41 | 0.18–0.93 | 0.034 | 0.89 | 0.43–1.81 | 0.747 | 0.78 | 0.36–1.69 | 0.538 | 1.59 | 0.78–3.26 | 0.198 | 1.37 | 0.62–2.99 | 0.429 |
| Secondary vs. university | 0.72 | 0.33–1.55 | 0.404 | 1.04 | 0.45–2.41 | 0.925 | 0.71 | 0.33–1.54 | 0.393 | 0.67 | 0.29–1.50 | 0.331 | 0.80 | 0.96–4.58 | 0.063 | 1.89 | 0.82–4.38 | 0.132 |
| Physical Abilities | 3 Mean (SD) | 4 Mean (SD) | 5 Mean (SD) | p | Size Effect | |
|---|---|---|---|---|---|---|
| eta2 | 95% CI | |||||
| Functional fitness score | ||||||
| All | 4.13 (2.31) | 3.90 (2.08) | 2.58 (1.87) | 0.002 | 0.05 | (0.01–0.10) |
| Men | 4.18 (1.91) | 3.74 (1.77) | 2.91 (1.44) | 0.032 | 0.06 | (0.01–0.14) |
| Women | 3.77 (1.77) | 3.93 (1.65) | 3.09 (1.76) | 0.322 | 0.00 | (0.00–0.06) |
| Endurance | ||||||
| All | 13.16 (3.66) | 13.15 (3.45) | 11.27 (2.76) | 0.027 | 0.04 | (0.00–0.09) |
| Men | 14.11 (4.07) | 13.55 (3.86) | 11.18 (2.59) | 0.032 | 0.06 | (0.01–0.15) |
| Women | 12.04 (2.77) | 12.59 (2.69) | 11.45 (3.21) | 0.322 | 0.00 | (0.00–0.02) |
| Lower body strength | ||||||
| All | 69.40 (18.68) | 68.48 (21.77) | 58.90 (15.81) | 0.027 | 0.04 | (0.00–0.08) |
| Men | 74.59 (18.81) | 73.24 (22.19) | 59.81 (16.24) | 0.006 | 0.06 | (0.01–0.14) |
| Women | 62.65 (16.38) | 61.78 (19.64) | 56.78 (15.47) | 0.554 | 0.00 | (0.00–0.07) |
| Sitting handgrip | ||||||
| All | 29.00 (11.57) | 30.15 (10.83) | 30.15 (9.88) | 0.780 | 0.00 | (0.00–0.02) |
| Men | 37.77 (7.46) | 37.44 (6.22) | 34.60 (9.13) | 0.143 | 0.02 | (0.00–0.08) |
| Women | 18.60 (5.13) | 19.61 (6.44) | 21.25 (2.63) | 0.267 | 0.03 | (0.00–0.10) |
| Standing handgrip | ||||||
| All | 28.50 (11.76) | 30.32 (10.40) | 30.52 (10.02) | 0.432 | 0.00 | (0.00–0.03) |
| Men | 36.95 (8.71) | 37.36 (5.93) | 34.83 (9.49) | 0.192 | 0.00 | (0.00–0.05) |
| Women | 18.46 (5.09) | 20.13 (6.10) | 21.90 (3.07) | 0.087 | 0.05 | (0.00–0.14) |
| One-leg balance | ||||||
| All | 32.22 (20.51) | 31.53 (19.68) | 21.01 (17.81) | 0.008 | 0.04 | (0.00–0.09) |
| Men | 36.27 (20.58) | 36.37 (18.75) | 25.17 (18.40) | 0.037 | 0.03 | (0.00–0.10) |
| Women | 27.41 (19.57) | 24.51 (19.17) | 12.70 (13.80) | 0.026 | 0.05 | (0.00–0.14) |
| Agility | ||||||
| All | 6.01 (1.61) | 6.14 (1.38) | 6.70 (1.49) | 0.018 | 0.02 | (0.00–0.06) |
| Men | 5.61 (1.41) | 5.82 (1.28) | 6.39 (1.45) | 0.044 | 0.04 | (0.00–0.11) |
| Women | 6.49 (1.70) | 6.60 (1.41) | 7.33 (1.43) | 0.133 | 0.02 | (0.00–0.10) |
| Upper body flexibility | ||||||
| All | −12.13 (11.98) | −12.53 (13.38) | −18.95 (10.85) | 0.005 | 0.04 | (0.00–0.08) |
| Men | −13.77 (13.60) | −14.68 (13.50) | −18.82 (12.86) | 0.250 | 0.02 | (0.00–0.07) |
| Women | −10–20 (9.49) | −9.41 (12.77) | −19.20 (5.37) | 0.004 | 0.04 | (0.00–0.13) |
| Lower body flexibility | ||||||
| All | −2.56 (9.29) | −2.08 (9.67) | −3,42 (9.10) | 0.721 | 0.00 | (0.00–0.03) |
| Men | −3.54 (9.88) | −3.81 (10.08) | −2.11 (8.84) | 0.847 | 0.00 | (0.00–0.03) |
| Women | −1.4 (8.50) | 0.42 (8.59) | −6.02 (9.46) | 0.157 | 0.00 | (0.00–0.02) |
| SF-36 Components | Low FFS (≤p50) Mean (SD) | High FFS (>p50) Mean (SD) | p | Size Effect | |
|---|---|---|---|---|---|
| d | 95% CI | ||||
| Physical role | |||||
| All | 77.12 (36.04) | 84.09 (32.67) | 0.144 | 0.20 | (−0.09–0.49) |
| Men | 84.21 (32.62) | 83.52 (33.65) | 0.947 | 0.02 | (−0.35–0.39) |
| Women | 67.41 (38.11) | 82.03 (33.14) | 0.057 | 0.40 | (0.04–0.84) |
| Physical function | |||||
| All | 75.55 (18.35) | 84.94 (14.34) | 0.001 | 0.56 | (0.26–0.85) |
| Men | 80.46 (16.15) | 89.43 (9.29) | 0.001 | 0.64 | (0.26–1.02) |
| Women | 67.50 (20.85) | 74.69 (16.85) | 0.009 | 0.37 | (0.07–0.81) |
| Body pain | |||||
| All | 63.39 (27.98) | 66.95 (25.62) | 0.367 | −0.13 | (−0.42–0.16) |
| Men | 68.07 (26.53) | 73.20 (21.58) | 0.356 | −0.21 | (−0.58–0.17) |
| Women | 53.95 (27.85) | 62.41 (28.46) | 0.101 | −0.30 | (−0.74–0.14) |
| General health | |||||
| All | 59.24 (21.37) | 66.47 (19.04) | 0.019 | 0.35 | (0.06–0.64) |
| Men | 60.50 (19.22) | 69.34 (15.62) | 0.025 | 0.49 | (0.11–0.87) |
| Women | 55.61 (24.49) | 61.16 (22.34) | 0.293 | −0.23 | (−0.67–0.20) |
| Social function | |||||
| All | 91.53 (19.26) | 88.47 (20.25) | 0.126 | 0.16 | (−0.13–0.44) |
| Men | 95.23 (14.71) | 91.19 (17.78) | 0.103 | 0.25 | (−0.12–0.63) |
| Women | 84.60 (23.23) | 85.55 (23.14) | 0.706 | −0.04 | (−0.48–0.39) |
| Emotional health | |||||
| All | 88.42 (27.00) | 77.06 (39.09) | 0.056 | 0.35 | (0.06–0.64) |
| Men | 92.54 (21.50) | 78.03 (38.00) | 0.019 | 0.51 | (0.13–0.88) |
| Women | 78.57 (37.30) | 73.96 (41.25) | 0.706 | 0.12 | (−0.32–0.55) |
| Vitality | |||||
| All | 66.65 (23.71) | 65.00 (21.44) | 0.448 | 0.07 | (−0.21–0.36) |
| Men | 72.30 (21.22) | 66.48 (18.57) | 0.075 | 0.29 | (−0.09–0.66) |
| Women | 55.27 (25.80 | 60.31 (23.07) | 0.375 | −0.20 | (−0.64–0.23) |
| Mental health | |||||
| All | 71.63 (21.93) | 70.75 (20.54) | 0.588 | 0.04 | (−0.25–0.33) |
| Men | 78.37 (18.01) | 73.27 (19.07) | 0.165 | 0.28 | (−0.10–0.65) |
| Women | 60.36 (23.94) | 67.50 (21.62) | 0.169 | −0.31 | (−0.74–0.13) |
| Physical component | |||||
| All | 45.02 (8.66) | 49.62 (7.11) | 0.001 | 0.57 | (0.28–0.86) |
| Men | 46.31 (7.45) | 51.14 (6.63) | 0.001 | 0.67 | (0.29–1.05) |
| Women | 42.90 (10.45) | 46.95 (6.74) | 0.109 | 0.44 | (0.00–0.87) |
| Mental component | |||||
| All | 51.81 (9.92) | 47.53 (12.51) | 0.013 | 0.57 | (0.28–0.86) |
| Men | 54.31 (8.79) | 48.08 (11.87) | 0.001 | 0.62 | (0.24–1.00) |
| Women | 46.85 (11.94) | 46.70 (12.87) | 0.982 | 0.01 | (−0.42–0.45) |
| Physical Health | Mental Health | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ≤MeP Mean (SD) | >MeP Mean (SD) | p | Effect Size | ≤MeP Mean (SD) | >MeP Mean (SD) | p | Effect Size | |||
| d | 95% CI | d | 95% CI | |||||||
| Functional fitness score | ||||||||||
| All | 3.39 (2.07) | 4.32 (2.32) | 0.003 | 0.42 | (0.15–0.70) | 4.04 (2.45) | 3.62 (2.02) | 0.199 | 0.19 | (−0.08–0.46) |
| Men | 3.46 (1.59) | 4.25 (2.04) | 0.028 | 0.44 | (0.08–0.81) | 4.31 (1.93) | 3.41 (1.67) | 0.004 | 0.51 | (0.14–0.87) |
| Women | 3.49 (1.62) | 4.00 (1.81) | 0.183 | 0.30 | (−012–0.72) | 3.68 (1.92) | 3.79 (1.56) | 0.737 | −0.06 | (−0.48–0.36) |
| Endurance | ||||||||||
| All | 62.86 (18.96) | 72.68 (19.17) | 0.001 | 0.52 | (0.23–0.80) | 68.45 (20.31) | 66.67 (19.13) | 0.498 | 0.09 | (−0.19–0.37) |
| Men | 66.47 (18.33) | 77.69 (20.85) | 0.009 | 0.58 | (0.20–0.95) | 74.04 (21.46) | 64.69 (19.03) | 0.216 | 0.23 | (−0.14–0.60) |
| Women | 56.95 (18.71) | 66.30 (14.70) | 0.023 | 0.56 | (−0.11–1.00) | 60.53 (15.66) | 62.65 (18.77) | 0.748 | −0.12 | (−0.56–0.32) |
| Lower body strength | ||||||||||
| All | 12.13 (3.18) | 13.76 (3.71) | 0.001 | 0.47 | (0.20–0.75) | 13.09 (3.50) | 12.68 (3.53) | 0.210 | 0.12 | (−0.16–0.39) |
| Men | 12.41 (3.09) | 14.71 (4.48) | 0.003 | 0.61 | (0.24–0.98) | 13.92 (3.78) | 12.97 (3.95) | 0.066 | 0.25 | (−0.12–0.61) |
| Women | 11.69 (3.32) | 12.63 (2.04) | 0.103 | 0.34 | (0.08–0.76) | 12.02 (2.81) | 12.26 (2.80) | 0.793 | −0.08 | (−0.50–0.34) |
| Sitting handgrip | ||||||||||
| All | 29.33 (11.04) | 29.87 (11.08) | 0.695 | −0.05 | (−0.32–0.22) | 29.88 (11.83) | 29.33 (10.40) | 0.720 | 0.05 | (−0.22–0.32) |
| Men | 36.22 (8.03) | 38.25 (6.40) | 0.141 | 0.27 | (0.09–0.64) | 38.40 (7.90) | 36.08 (6.94) | 0.040 | 0.31 | (−0.05–0.68) |
| Women | 18.62 (4.65) | 19.93 (6.06) | 0.292 | 0.24 | (0.18–0.66) | 19.07 (5.31) | 19.42 (5.53) | 0.850 | −0.06 | (−0.48–0.35) |
| Standing handgrip | ||||||||||
| All | 29.33 (11.27) | 29.57 (10.81) | 0.757 | −0.02 | (−0.29–0.25) | 29.74 (11.98) | 29.20 (10.27) | 0.679 | 0.05 | (−0.22–0.32) |
| Men | 36.02 (8.94) | 37.65 (6.46) | 0.250 | −0.20 | (−0.56–0.16) | 38.33 (8.12) | 35.48 (7.75) | 0.019 | 0.36 | (0.00–0.72) |
| Women | 18.91 (4.60) | 20.00 (6.02) | 0.335 | −0.20 | (−0.62–0.22) | 18.84 (5.34) | 19.97 (5.34) | 0.487 | −0.21 | (−0.63–0.21) |
| One-leg balance | ||||||||||
| All | 27.36 (20.20) | 33.70 (19.62) | 0.011 | 0.32 | (0.04–0.59) | 31.24 (20.40) | 29.39 (19.98) | 0.464 | 0.09 | (−0.18–0.36) |
| Men | 31.36 (20.36) | 38.30 (18.69) | 0.035 | 0.35 | (0.01–0.72) | 38.09 (19.16) | 31.41 (20.09) | 0.049 | 0.34 | (−0.02–0.70) |
| Women | 21.15 (18.48) | 28.25 (19.51) | 0.052 | 0.37 | (0.05–0.79) | 22.56 (18.72) | 26.42 (19.66) | 0.340 | −0.20 | (−0.62–0.22) |
| Agility | ||||||||||
| All | 6.38 (1.69) | 5.90 (1.26) | 0.052 | 0.32 | (0.05–0.59) | 6.26 (1.73) | 6.09 (1.35) | 0.862 | 0.11 | (−0.16–0.39) |
| Men | 6.00 (1.47) | 5.59 (1.26) | 0.148 | 0.29 | (−0.07–0.66) | 5.72 (1.42) | 5.9 (1.37) | 0.386 | −0.13 | (−0.49–0.23) |
| Women | 6.98 (1.84) | 6.27 (1.18) | 0.090 | 0.46 | (0.04–0.88) | 6.94 (1.86) | 6.36 (1.27) | 0.233 | 0.37 | (−0.05–0.79) |
| Upper body flexibility | ||||||||||
| All | −14.34 (12.88) | −12.13 (11.96) | 0.089 | 0.18 | (0.10–0.45) | −13.07 (11.49) | −13.57 (13.28) | 0.597 | 0.04 | (−0.23–0.31) |
| Men | −16.44 (13.23) | −13.03 (13.64) | 0.106 | 0.25 | (0.11–0.62) | −13.17 (12.66) | −16.39 (13.96) | 0.080 | 0.24 | (−0.12–0.60) |
| Women | −11.06 (11.71) | −11.06 (9.65) | 0.735 | 0.00 | (−0.42–0.42) | −12.94 (9.97) | −9.43 (11.12) | 0.081 | −0.33 | (−0.75–0.09) |
| Lower body flexibility | ||||||||||
| All | −3.70 (9.18) | −1.10 (9.42) | 0.060 | 0.28 | (0.01–0.55) | −2.42 (9.51) | −2.62 (9.27) | 0.561 | 0.02 | (−0.25–0.29) |
| Men | −4.83 (9.47) | −1.37 (9.77) | 0.079 | 0.36 | (0.00–0.72) | −3.72 (9.68) | −3.11 (9.80) | 0.984 | −0.06 | (−0.42–0.30) |
| Women | −1.94 (8.5) | −0.78 (9.10) | 0.426 | 0.13 | (0.29–0.55) | −0.77 (9.14) | −1.90 (8.49) | 0.413 | 0.13 | (−0.29–0.55) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conde-Pipó, J.; Bouzas, C.; Mariscal-Arcas, M.; Tur, J.A. Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome. Nutrients 2022, 14, 1798. https://doi.org/10.3390/nu14091798
Conde-Pipó J, Bouzas C, Mariscal-Arcas M, Tur JA. Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome. Nutrients. 2022; 14(9):1798. https://doi.org/10.3390/nu14091798
Chicago/Turabian StyleConde-Pipó, Javier, Cristina Bouzas, Miguel Mariscal-Arcas, and Josep A. Tur. 2022. "Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome" Nutrients 14, no. 9: 1798. https://doi.org/10.3390/nu14091798
APA StyleConde-Pipó, J., Bouzas, C., Mariscal-Arcas, M., & Tur, J. A. (2022). Association between Functional Fitness and Health-Related Quality of Life in the Balearic Islands’ Old Adults with Metabolic Syndrome. Nutrients, 14(9), 1798. https://doi.org/10.3390/nu14091798