
Nuclear Magnetic Resonance-Measured Ionized Magnesium Is Inversely Associated with Type 2 Diabetes in the Insulin Resistance Atherosclerosis Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Optimization of an NMR-Based Ionized or Free Magnesium Assay
2.2. Evaluation of Assay Performance
2.3. Reference Interval Determination
2.4. Method Comparison Study
2.5. Insulin Resistance Atherosclerosis Study (IRAS)
2.6. Statistical Analyses
3. Results
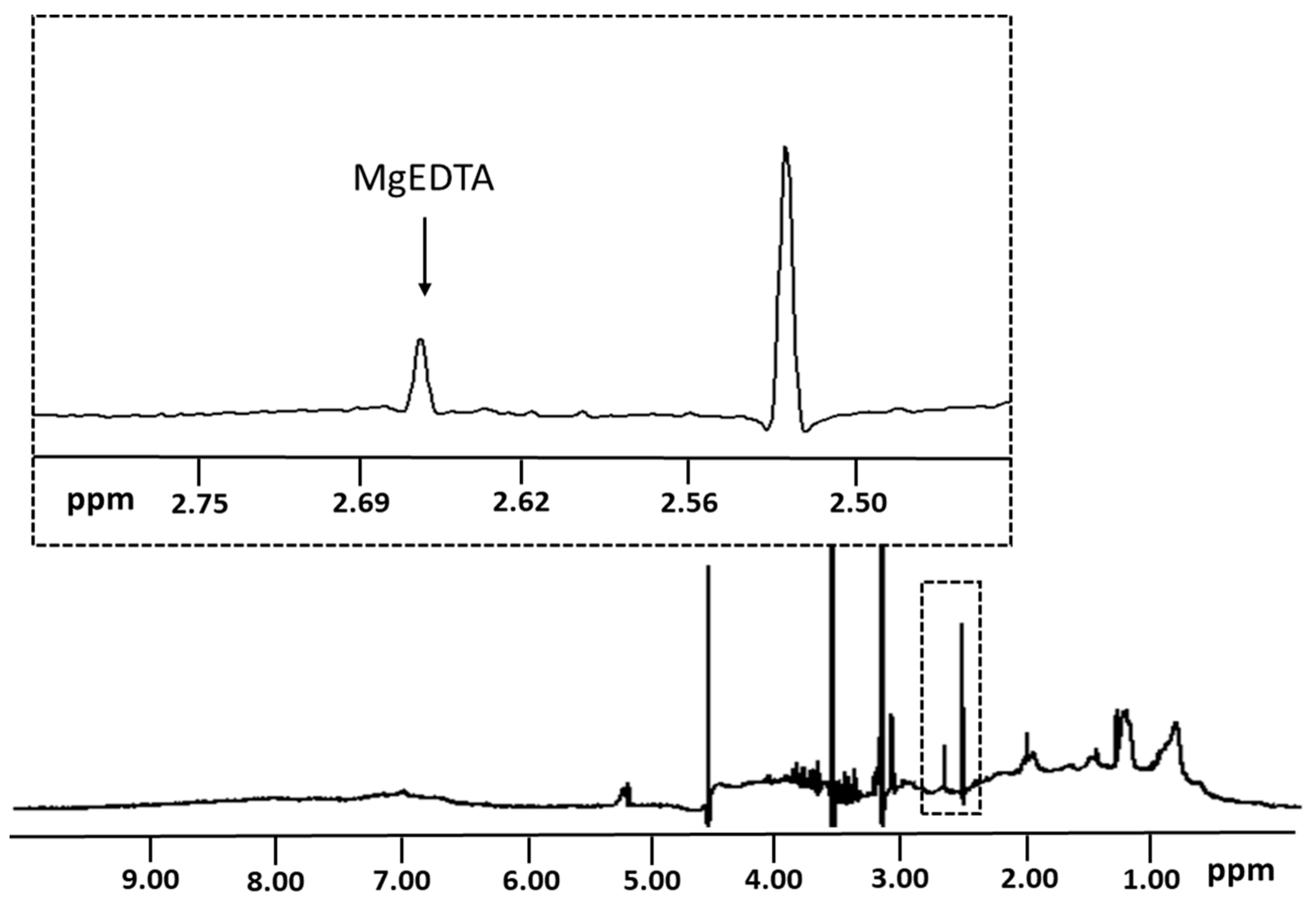
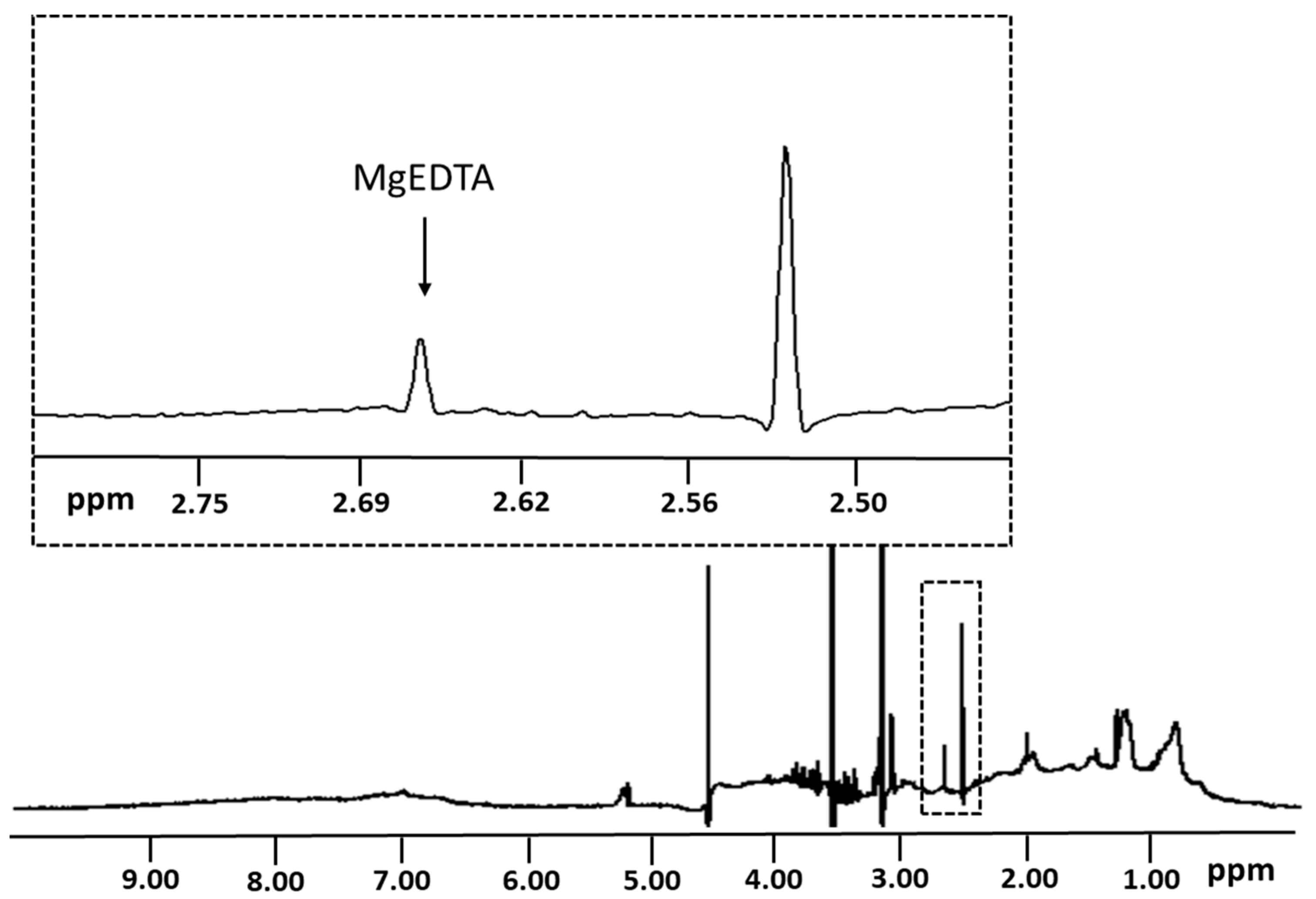
3.1. Quantification of Ionized Magnesium Using an NMR-Based Deconvolution Algorithm
3.2. Assay Characteristics and Stability of Magnesium in Plasma
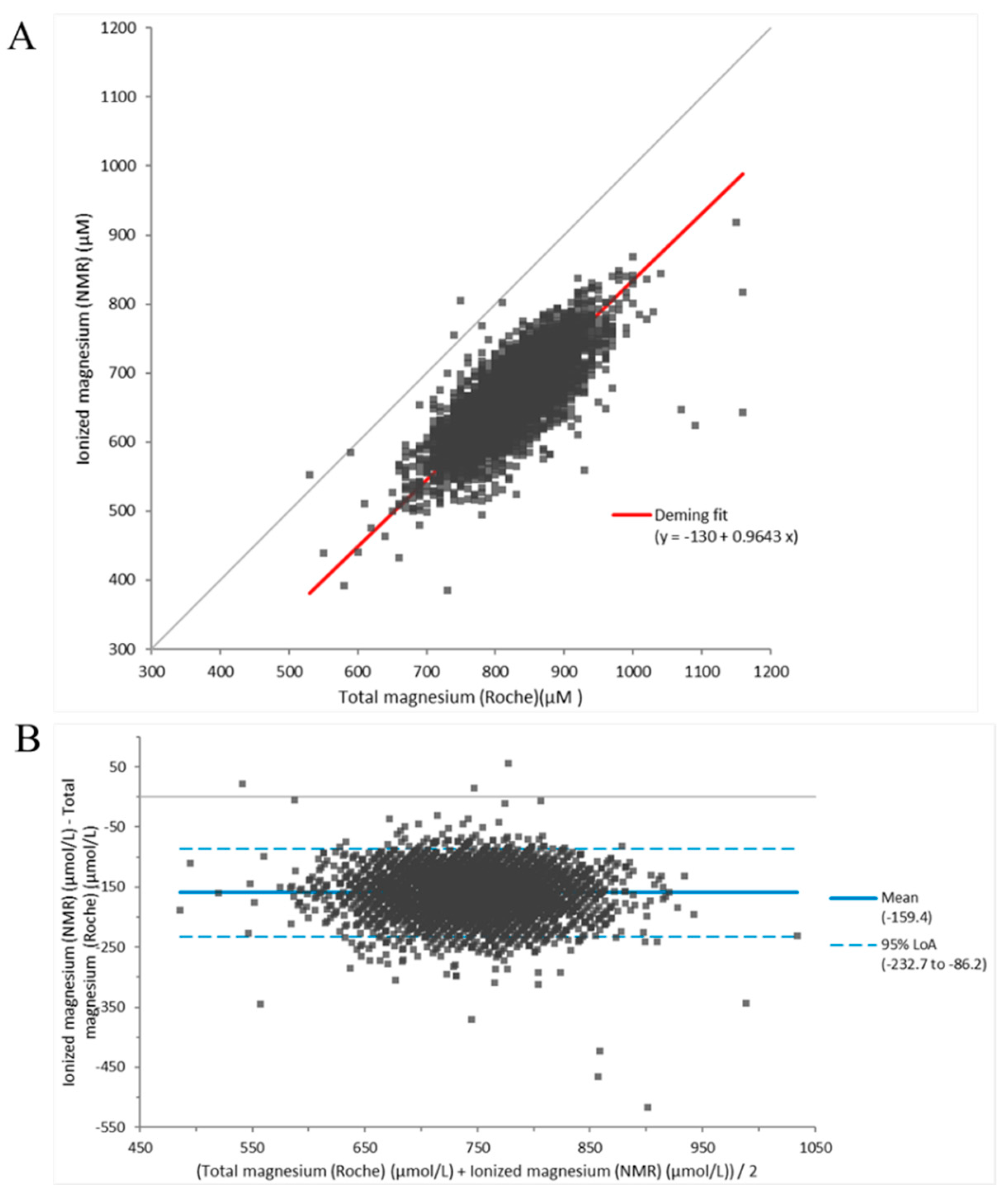
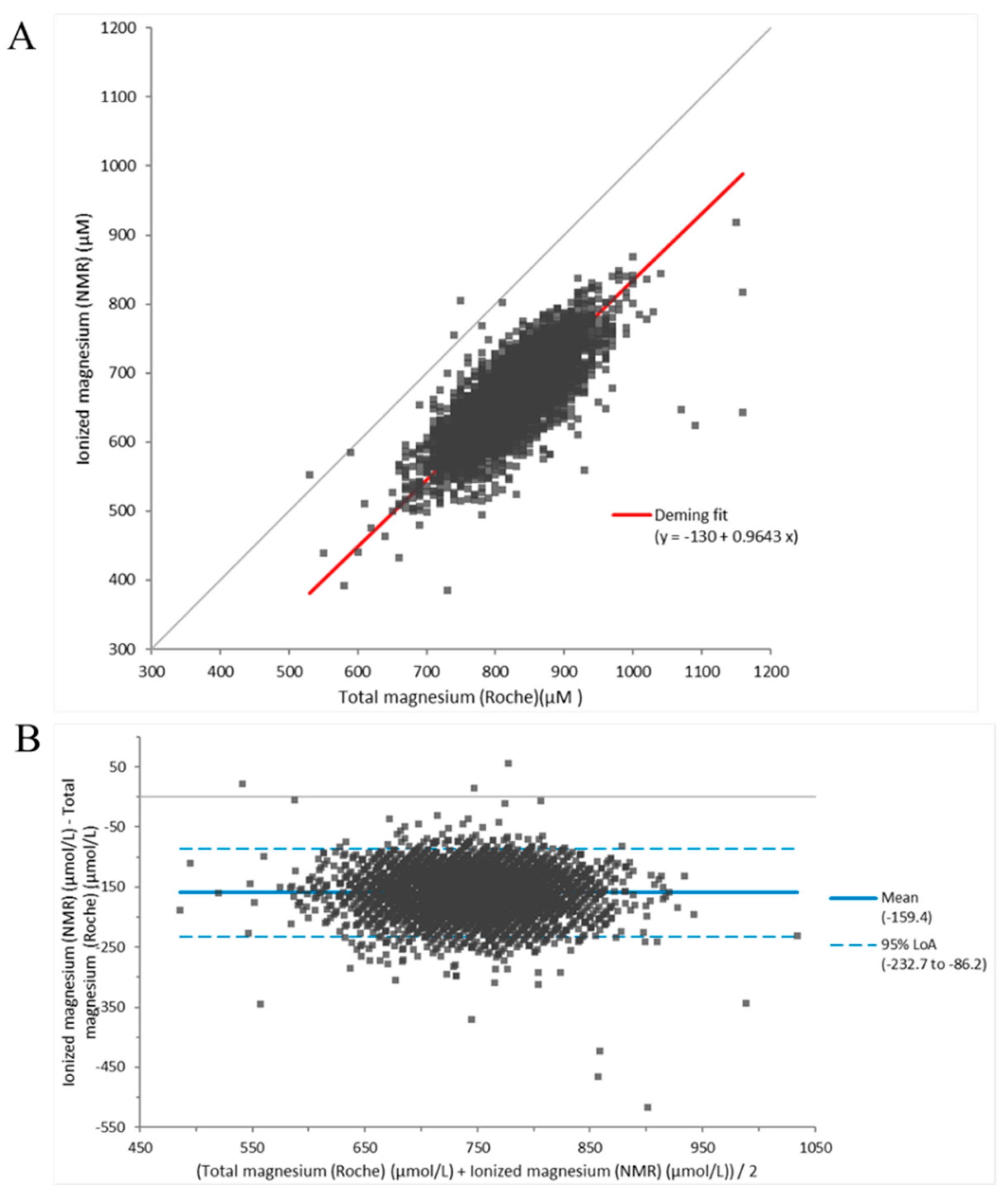
3.3. Comparison between Results Generated by the NMR-Based Ionized Magnesium Assay in EDTA Plasma and Roche Total Magnesium Assay in Serum
3.4. Association of Ionized Magnesium with T2D in a Fairly High-Risk Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saris, N.E.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium. An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Barbagallo, M.; Dominguez, L.J. Magnesium metabolism in type 2 diabetes mellitus, metabolic syndrome and insulin resistance. Arch. Biochem. Biophys. 2007, 458, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Grober, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorentini, D.; Cappadone, C.; Farruggia, G.; Prata, C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients 2021, 13, 1136. [Google Scholar] [CrossRef] [PubMed]
- De Baaij, J.H.; Hoenderop, J.G.; Bindels, R.J. Magnesium in man: Implications for health and disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef] [PubMed]
- Bairoch, A. The ENZYME database in 2000. Nucleic Acids Res. 2000, 28, 304–305. [Google Scholar] [CrossRef] [Green Version]
- Caspi, R.; Altman, T.; Dreher, K.; Fulcher, C.A.; Subhraveti, P.; Keseler, I.M.; Kothari, A.; Krummenacker, M.; Latendresse, M.; Mueller, L.A.; et al. The MetaCyc database of metabolic pathways and enzymes and the BioCyc collection of pathway/genome databases. Nucleic Acids Res. 2012, 40, D742–D753. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.C. Combating COVID-19 and Building Immune Resilience: A Potential Role for Magnesium Nutrition? J. Am. Coll. Nutr. 2020, 39, 685–693. [Google Scholar] [CrossRef]
- Elin, R.J. Assessment of magnesium status. Clin. Chem. 1987, 33, 1965–1970. [Google Scholar] [CrossRef]
- Lowenstein, F.W.; Stanton, M.F. Serum magnesium levels in the United States, 1971–1974. J. Am. Coll. Nutr. 1986, 5, 399–414. [Google Scholar] [CrossRef]
- Schutten, J.C.; Gomes-Neto, A.W.; Navis, G.; Gansevoort, R.T.; Dullaart, R.P.F.; Kootstra-Ros, J.E.; Danel, R.M.; Goorman, F.; Gans, R.O.B.; Borst, M.H.; et al. Lower Plasma Magnesium, Measured by Nuclear Magnetic Resonance Spectroscopy, is Associated with Increased Risk of Developing Type 2 Diabetes Mellitus in Women: Results from a Dutch Prospective Cohort Study. J. Clin. Med. 2019, 8, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dijk, P.R.; Schutten, J.C.; Jeyarajah, E.J.; Kootstra-Ros, J.E.; Connelly, M.A.; Bakker, S.J.L.; Dullaart, R.P.F. Blood Mg(2+) is more closely associated with hyperglycaemia than with hypertriacylglycerolaemia: The PREVEND study. Diabetologia 2019, 62, 1732–1734. [Google Scholar] [CrossRef] [PubMed]
- Waanders, F.; Dullaart, R.P.F.; Vos, M.J.; Hendriks, S.H.; van Goor, H.; Bilo, H.J.G.; van Dijk, P.R. Hypomagnesaemia and its determinants in a contemporary primary care cohort of persons with type 2 diabetes. Endocrine 2020, 67, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Piuri, G.; Zocchi, M.; Della Porta, M.; Ficara, V.; Manoni, M.; Zuccotti, G.V.; Pinotti, L.; Maier, J.A.; Cazzola, R. Magnesium in Obesity, Metabolic Syndrome, and Type 2 Diabetes. Nutrients 2021, 13, 320. [Google Scholar] [CrossRef] [PubMed]
- Altura, B.M.; Altura, B.T. Role of magnesium in patho-physiological processes and the clinical utility of magnesium ion selective electrodes. Scand. J. Clin. Lab. Investig. Suppl. 1996, 224, 211–234. [Google Scholar] [CrossRef]
- Shalaurova, I.; Connelly, M.A.; Garvey, W.T.; Otvos, J.D. Lipoprotein insulin resistance index: A lipoprotein particle-derived measure of insulin resistance. Metab. Syndr. Relat. Disord. 2014, 12, 422–429. [Google Scholar] [CrossRef]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Jeyarajah, E.J.; Shalaurova, I.; Xu, Y.; Warner, S.M.; Clement, T.S.; Connelly, M.A.; Fischer, T.J. NMR measurement of LDL particle number using the Vantera Clinical Analyzer. Clin. Biochem. 2014, 47, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Matyus, S.P.; Braun, P.J.; Wolak-Dinsmore, J.; Saenger, A.K.; Jeyarajah, E.J.; Shalaurova, I.; Warner, S.M.; Fischer, T.J.; Connelly, M.A. HDL particle number measured on the Vantera(R), the first clinical NMR analyzer. Clin. Biochem. 2015, 48, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Otvos, J.D.; Shalaurova, I.; Wolak-Dinsmore, J.; Connelly, M.A.; Mackey, R.H.; Stein, J.H.; Tracy, R.P. GlycA: A Composite Nuclear Magnetic Resonance Biomarker of Systemic Inflammation. Clin. Chem. 2015, 61, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Wolak-Dinsmore, J.; Gruppen, E.G.; Shalaurova, I.; Matyus, S.P.; Grant, R.P.; Gegen, R.; Bakker, S.J.L.; Otvos, J.D.; Connelly, M.A.; Dullaart, R.P.F. A novel NMR-based assay to measure circulating concentrations of branched-chain amino acids: Elevation in subjects with type 2 diabetes mellitus and association with carotid intima media thickness. Clin. Biochem. 2018, 54, 92–99. [Google Scholar] [CrossRef]
- Garcia, E.; Shalaurova, I.; Matyus, S.P.; Oskardmay, D.N.; Otvos, J.D.; Dullaart, R.P.F.; Connelly, M.A. Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index. J. Clin. Med. 2020, 9, 321. [Google Scholar] [CrossRef] [Green Version]
- Garcia, E.; Bennett, D.W.; Connelly, M.A.; Jeyarajah, E.J.; Warf, F.C.; Shalaurova, I.; Matyus, S.P.; Wolak-Dinsmore, J.; Oskardmay, D.N.; Young, R.M.; et al. The extended lipid panel assay: A clinically-deployed high-throughput nuclear magnetic resonance method for the simultaneous measurement of lipids and Apolipoprotein B. Lipids Health Dis. 2020, 19, 247. [Google Scholar] [CrossRef] [PubMed]
- Flores-Guerrero, J.L.; Gruppen, E.G.; Connelly, M.A.; Shalaurova, I.; Otvos, J.D.; Garcia, E.; Bakker, S.J.L.; Dullaart, R.P.F. A Newly Developed Diabetes Risk Index, Based on Lipoprotein Subfractions and Branched Chain Amino Acids, is Associated with Incident Type 2 Diabetes Mellitus in the PREVEND Cohort. J. Clin. Med. 2020, 9, 2781. [Google Scholar] [CrossRef] [PubMed]
- Garcia, E.; Connelly, M.A.; Matyus, S.P.; Otvos, J.D.; Shalaurova, I. High-throughput nuclear magnetic resonance measurement of citrate in serum and plasma in the clinical laboratory. Pract. Lab. Med. 2021, 25, e00213. [Google Scholar] [CrossRef] [PubMed]
- Connelly, M.A.; Gruppen, E.G.; Wolak-Dinsmore, J.; Matyus, S.P.; Riphagen, I.J.; Shalaurova, I.; Bakker, S.J.; Otvos, J.D.; Dullaart, R.P. GlycA, a marker of acute phase glycoproteins, and the risk of incident type 2 diabetes mellitus: PREVEND study. Clin. Chim. Acta 2016, 452, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Connelly, M.A.; Otvos, J.D.; Shalaurova, I.; Playford, M.P.; Mehta, N.N. GlycA, a novel biomarker of systemic inflammation and cardiovascular disease risk. J. Transl. Med. 2017, 15, 219. [Google Scholar] [CrossRef]
- Mehta, N.N.; Dey, A.K.; Maddineni, R.; Kraus, W.E.; Huffman, K.M. GlycA measured by NMR spectroscopy is associated with disease activity and cardiovascular disease risk in chronic inflammatory diseases. Am. J. Prev. Cardiol. 2020, 4, 100120. [Google Scholar] [CrossRef]
- Flores-Guerrero, J.L.; Connelly, M.A.; Shalaurova, I.; Gruppen, E.G.; Kieneker, L.M.; Dullaart, R.P.F.; Bakker, S.J.L. Lipoprotein insulin resistance index, a high-throughput measure of insulin resistance, is associated with incident type II diabetes mellitus in the Prevention of Renal and Vascular End-Stage Disease study. J. Clin. Lipidol. 2019, 13, 129–137.e1. [Google Scholar] [CrossRef] [Green Version]
- CLSI Document EP17-A; Protocols for Determination of Limits of Detection and Limits of Quantitation. Approved Guideline; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2004.
- CLSI Document EP5-A2; Evaluation of Precision Performance of Quantitative Measurements Methods; Approved Guideline-Second Edition. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2004.
- Wagenknecht, L.E.; Mayer, E.J.; Rewers, M.; Haffner, S.; Selby, J.; Borok, G.M.; Henkin, L.; Howard, G.; Savage, P.J.; Saad, M.F.; et al. The insulin resistance atherosclerosis study (IRAS) objectives, design, and recruitment results. Ann. Epidemiol. 1995, 5, 464–472. [Google Scholar] [CrossRef]
- Lorenzo, C.; Hartnett, S.; Hanley, A.J.; Rewers, M.J.; Wagenknecht, L.E.; Karter, A.J.; Haffner, S.M. Impaired fasting glucose and impaired glucose tolerance have distinct lipoprotein and apolipoprotein changes: The insulin resistance atherosclerosis study. J. Clin. Endocrinol. Metab. 2013, 98, 1622–1630. [Google Scholar] [CrossRef] [Green Version]
- Palaniappan, L.; Carnethon, M.R.; Wang, Y.; Hanley, A.J.; Fortmann, S.P.; Haffner, S.M.; Wagenknecht, L.; Insulin Resistance Atherosclerosis Study. Predictors of the incident metabolic syndrome in adults: The Insulin Resistance Atherosclerosis Study. Diabetes Care 2004, 27, 788–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Festa, A.; Williams, K.; Hanley, A.J.; Otvos, J.D.; Goff, D.C.; Wagenknecht, L.E.; Haffner, S.M. Nuclear magnetic resonance lipoprotein abnormalities in prediabetic subjects in the Insulin Resistance Atherosclerosis Study. Circulation 2005, 111, 3465–3472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, W.H.; Folsom, A.R.; Nieto, F.J.; Mo, J.P.; Watson, R.L.; Brancati, F.L. Serum and dietary magnesium and the risk for type 2 diabetes mellitus: The Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 1999, 159, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Everett, C.J.; King, D.E. Serum magnesium and the development of diabetes. Nutrition 2006, 22, 679. [Google Scholar] [CrossRef]
- Kieboom, B.C.T.; Licher, S.; Wolters, F.J.; Ikram, M.K.; Hoorn, E.J.; Zietse, R.; Stricker, B.H.; Ikram, M.A. Serum magnesium is associated with the risk of dementia. Neurology 2017, 89, 1716–1722. [Google Scholar] [CrossRef]
- Kieboom, B.C.T.; Ligthart, S.; Dehghan, A.; Kurstjens, S.; de Baaij, J.H.F.; Franco, O.H.; Hofman, A.; Zietse, R.; Stricker, B.H.; Hoorn, E.J. Serum magnesium and the risk of prediabetes: A population-based cohort study. Diabetologia 2017, 60, 843–853. [Google Scholar] [CrossRef] [Green Version]
- Greenway, D.C.; Hindmarsh, J.T.; Wang, J.; Khodadeen, J.A.; Hebert, P.C. Reference interval for whole blood ionized magnesium in a healthy population and the stability of ionized magnesium under varied laboratory conditions. Clin. Biochem. 1996, 29, 515–520. [Google Scholar] [CrossRef]
- Rooney, M.R.; Rudser, K.D.; Alonso, A.; Harnack, L.; Saenger, A.K.; Lutsey, P.L. Circulating Ionized Magnesium: Comparisons with Circulating Total Magnesium and the Response to Magnesium Supplementation in a Randomized Controlled Trial. Nutrients 2020, 12, 263. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Sample # | Spiked (µM) | Measured a (µM) | Recovered (µM) | % Recovery |
|---|---|---|---|---|
| 1 | 0 | 589.9 ± 12.8 b | -- | -- |
| 2 | 105.1 | 688.5 ± 12.6 | 98.6 | 93.8 |
| 3 | 304.9 | 883.0 ± 9.5 | 293.1 | 96.1 |
| 4 | 609.8 | 1156.4 ± 5.2 | 566.5 | 92.9 |
| 5 | 809.5 | 1330.0 ± 12.0 | 740.1 | 91.4 |
| 6 | 1009.3 | 1544.1 ± 9.8 | 954.2 | 94.5 |
| 7 | 1503.4 | 2003.6 ± 41.8 | 1413.8 | 94.0 |
| 8 | 2008.1 | 2479.1 ± 36.9 | 1889.3 | 94.1 |
| Magnesium (µM) | |||
|---|---|---|---|
| Low | Intermediate | High | |
| Within-Runa | |||
| Mean | 561 | 799 | 1222 |
| SD | 8 | 6 | 11 |
| %CV | 1.5 | 0.7 | 0.9 |
| Within-Laboratoryb | |||
| Mean | 567 | 762 | 1179 |
| SD | 25 | 36 | 50 |
| %CV | 4.5 | 4.7 | 4.2 |
| Percentile | Value (µM) |
|---|---|
| Min | 433 |
| 0.5th | 480 |
| 2.5th | 513 |
| 10th | 555 |
| 25th | 598 |
| 50th | 644 |
| 75th | 681 |
| 90th | 717 |
| 97.5th | 762 |
| 99.5th | 796 |
| Max | 843 |
| Mean | 640 |
| SD | 62.1 |
| 95% Reference Interval | 513–762 |
| No Diabetes (n = 614) | Prediabetes (n = 301) | Type 2 Diabetes (n = 427) | p-Value | |
|---|---|---|---|---|
| Age (years) | 54 ± 9 a,b | 57 ± 8 | 57 ± 8 | <0.0001 |
| Sex, men (%) | 52 d | 41 f | 54 | 0.0015 |
| Race | ||||
| Non-Hispanic white (%) | 41 | 39 | 34 | 0.096 |
| Hispanic (%) | 33 | 34 | 32 | 0.79 |
| African American (%) | 26 e | 27 | 34 | 0.015 |
| BMI (kg/m2) | 27.4 ± 4.9 a,b | 30.3 ± 6.2 | 31.3 ± 5.6 | <0.0001 |
| Fasting glucose (mg/dL) | 96 ± 10 d,b | 105 ± 11 c | 175 ± 59 | <0.0001 |
| Fasting insulin (mIU/L) | 13.8 ± 9.5 a,b | 19.7 ± 21.4 c | 23.3 ± 16.5 | <0.0001 |
| Fasting FFA (mmol/L) | 0.43 ± 0.17 a,b | 0.55 ± 0.19 f | 0.59 ± 0.23 | <0.0001 |
| Total cholesterol (mg/dL) | 208 ± 44 d | 216 ± 39 | 212 ± 43 | 0.033 |
| Triglycerides (mg/dL) | 125 ± 83 d,b | 159 ± 96 f | 189 ± 165 | <0.0001 |
| HDL-C (mg/dL) | 47.2 ± 15.4 b | 45.0 ± 14.5 c | 40.0 ± 11.5 | <0.0001 |
| GlycA (µmol/L) | 350 ± 64 a,b | 379 ± 76 | 381 ± 70 | <0.0001 |
| HOMA-IR | 3.3 ± 2.4 a,b | 5.1 ± 5.9 c | 9.9 ± 7.9 | <0.0001 |
| LP-IR score (0–100) | 41 ± 21 a,b | 49 ± 20 c | 56 ± 19 | <0.0001 |
| Ionized magnesium (µM) | 644 ± 119 d,b | 612 ±123 c | 572 ± 135 | <0.0001 |
| Total Participants (n = 1342) | Wald χ2 | p-Value | Women (n = 669) | Wald χ2 | p-Value | Men (n = 673) | Wald χ2 | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Prevalent T2D, n (%) | 427 (31.8) | - | - | 196 (29.3) | - | - | 231 (34.3) | - | - |
| Model 1 | 0.592 (0.523–0.671) | 67.4084 | <0.0001 | 0.479 (0.396–0.579) | 57.5952 | <0.0001 | 0.711 (0.602–0.841) | 15.8831 | <0.0001 |
| Model 2 | 0.644 (0.562–0.738) | 40.3684 | <0.0001 | 0.537 (0.438–0.657) | 36.0651 | <0.0001 | 0.749 (0.623–0.901) | 9.3833 | 0.0022 |
| Model 3 | 0.638 (0.557–0.731) | 41.7936 | <0.0001 | 0.535 (0.437–0.656) | 36.3385 | <0.0001 | 0.737 (0.612–0.888) | 10.3900 | 0.0013 |
| Model 4 | 0.689 (0.599–0.792) | 27.4432 | <0.0001 | 0.606 (0.491–0.748) | 21.8372 | <0.0001 | 0.768 (0.636–0.927) | 7.5675 | 0.0059 |
| Model 5 | 0.771 (0.608–0.978) | 4.6083 | 0.032 | 0.540 (0.369–0.789) | 10.1375 | 0.0015 | 0.981 (0.714–1.349) | 0.0139 | 0.90 |
| Total Participants (n = 833) | Wald χ2 | p-Value | Women (n = 473) | Wald χ2 | p-Value | Men (n = 360) | Wald χ2 | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Events, n (%) | 131 (15.7) | - | - | 79 (16.7) | - | - | 52 (14.4) | - | - |
| Model 1 | 0.817 (0.677–0.986) | 4.4439 | 0.035 | 0.851 (0.666–1.087) | 1.6731 | 0.20 | 0.772 (0.576–1.036) | 2.9707 | 0.085 |
| Model 2 | 0.814 (0.669–0.991) | 4.1968 | 0.041 | 0.857 (0.662–1.110) | 1.3614 | 0.24 | 0.739 (0.543–1.007) | 3.6630 | 0.056 |
| Model 3 | 0.808 (0.664–0.985) | 4.4657 | 0.035 | 0.845 (0.651–1.097) | 1.5988 | 0.21 | 0.739 (0.542–1.006) | 3.6832 | 0.055 |
| Model 4 | 0.802 (0.655–0.983) | 4.5351 | 0.033 | 0.835 (0.637–1.093) | 1.7252 | 0.19 | 0.734 (0.536–1.005) | 3.7231 | 0.054 |
| Model 5 | 0.881 (0.719–1.080) | 1.4908 | 0.22 | 1.005 (0.760–1.329) | 0.0010 | 0.97 | 0.745 (0.545–1.018) | 3.4160 | 0.065 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, E.; Shalaurova, I.; Matyus, S.P.; Schutten, J.C.; Bakker, S.J.L.; Dullaart, R.P.F.; Connelly, M.A. Nuclear Magnetic Resonance-Measured Ionized Magnesium Is Inversely Associated with Type 2 Diabetes in the Insulin Resistance Atherosclerosis Study. Nutrients 2022, 14, 1792. https://doi.org/10.3390/nu14091792
Garcia E, Shalaurova I, Matyus SP, Schutten JC, Bakker SJL, Dullaart RPF, Connelly MA. Nuclear Magnetic Resonance-Measured Ionized Magnesium Is Inversely Associated with Type 2 Diabetes in the Insulin Resistance Atherosclerosis Study. Nutrients. 2022; 14(9):1792. https://doi.org/10.3390/nu14091792
Chicago/Turabian StyleGarcia, Erwin, Irina Shalaurova, Steven P. Matyus, Joelle C. Schutten, Stephan J. L. Bakker, Robin P. F. Dullaart, and Margery A. Connelly. 2022. "Nuclear Magnetic Resonance-Measured Ionized Magnesium Is Inversely Associated with Type 2 Diabetes in the Insulin Resistance Atherosclerosis Study" Nutrients 14, no. 9: 1792. https://doi.org/10.3390/nu14091792
APA StyleGarcia, E., Shalaurova, I., Matyus, S. P., Schutten, J. C., Bakker, S. J. L., Dullaart, R. P. F., & Connelly, M. A. (2022). Nuclear Magnetic Resonance-Measured Ionized Magnesium Is Inversely Associated with Type 2 Diabetes in the Insulin Resistance Atherosclerosis Study. Nutrients, 14(9), 1792. https://doi.org/10.3390/nu14091792